

Impact of Tumor Size on Prolactinoma Characteristics and Treatment Outcomes: A Study of a Tunisian Cohort

 , , and
, , and
Abstract
1. Introduction
2. Methods
2.1. Study Design and Population
2.2. Main Steps of the Study
- A descriptive overview of the clinical, hormonal, and radiological features of prolactinomas and their comparison between the three groups.
- An evaluation of treatment strategies and outcomes across the three groups.
- An analytical study to identify predictive factors of prolactinoma remission.
2.3. Data Collection
2.3.1. Clinical Parameters
2.3.2. Biological Parameters
2.3.3. Imaging Parameters
2.4. Treatment and Evaluation of Outcomes
2.5. Definitions of Treatment Outcomes
2.6. Statistical Analysis
3. Results
3.1. Epidemiological Data
3.2. Anthropometric Data
3.3. Biological Data
3.3.1. Metabolic Parameters
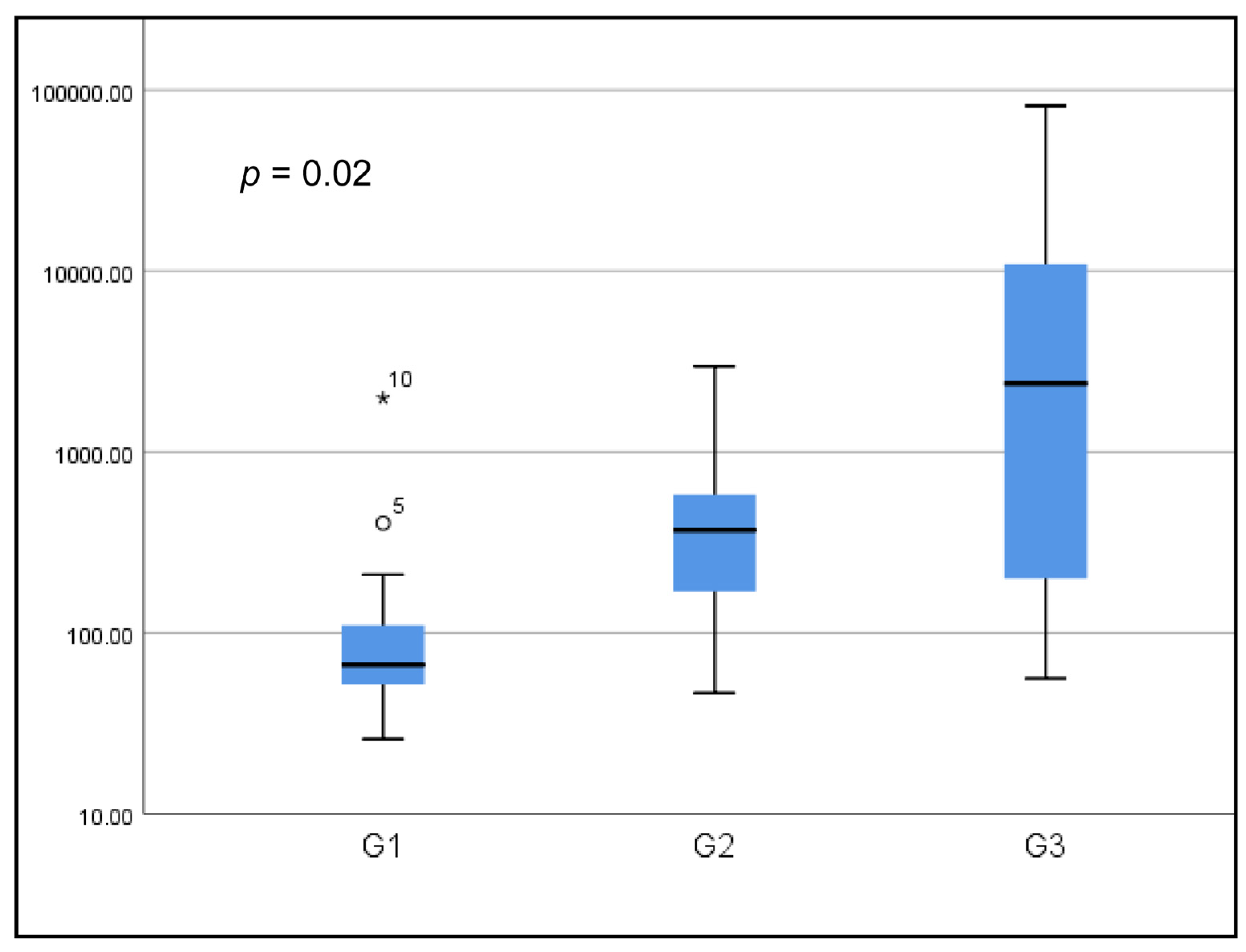
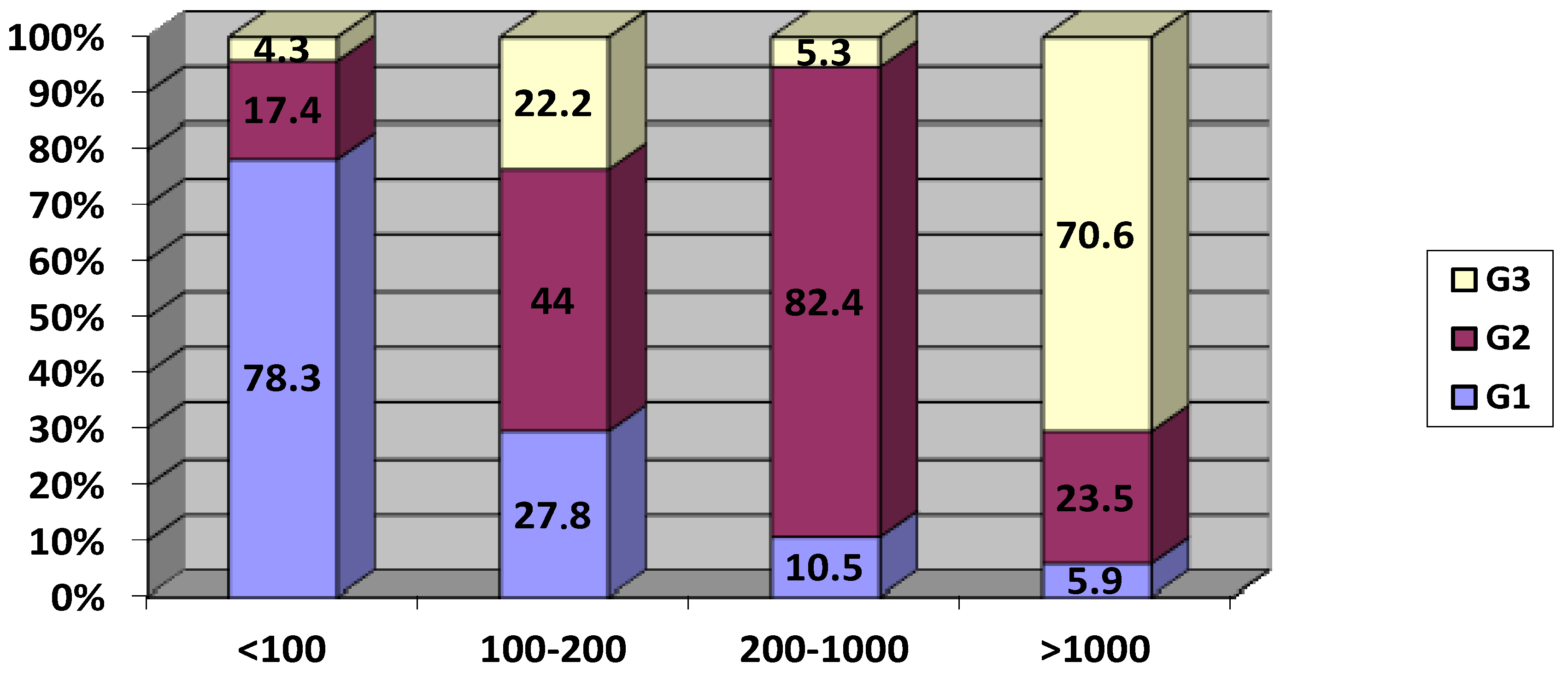
3.3.2. Prolactinemia
3.3.3. Other Hormonal Dosages
3.4. Treatment
3.5. Follow-Up Data
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Glezer, A.; Bronstein, M.D. Prolactinoma. Arq. Bras. Endocrinol. Metabol. 2014, 58, 118–123. [Google Scholar] [CrossRef] [PubMed]
- Gruppetta, M.; Vassallo, J. Epidemiology and radiological geometric assessment of pituitary macroadenomas: Population-based study. Clin. Endocrinol. 2016, 85, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Bonneville, J.-F. Magnetic Resonance Imaging of Pituitary Tumors. Front. Horm. Res. 2016, 45, 97–120. [Google Scholar] [PubMed]
- Hu, J.; Zheng, X.; Zhang, W.; Yang, H. Current drug withdrawal strategy in prolactinoma patients treated with cabergoline: A systematic review and meta-analysis. Pituitary 2015, 18, 745–751. [Google Scholar] [CrossRef] [PubMed]
- Sala, E.; Bellaviti Buttoni, P.; Malchiodi, E.; Verrua, E.; Carosi, G.; Profka, E.; Rodari, G.; Filopanti, M.; Ferrante, E.; Spada, A.; et al. Recurrence of hyperprolactinemia following dopamine agonist withdrawal and possible predictive factors of recurrence in prolactinomas. J. Endocrinol. Investig. 2016, 39, 1377–1382. [Google Scholar] [CrossRef] [PubMed]
- Melmed, S.; Casanueva, F.F.; Hoffman, A.R.; Kleinberg, D.L.; Montori, V.M.; Schlechte, J.A.; Wass, J.A.H. Diagnosis and treatment of hyperprolactinemia: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 273–288. [Google Scholar] [CrossRef] [PubMed]
- Agustsson, T.T.; Baldvinsdottir, T.; Jonasson, J.G.; Olafsdottir, E.; Steinthorsdottir, V.; Sigurdsson, G.; Thorsson, A.V.; Carroll, P.V.; Korbonits, M.; Benediktsson, R. The epidemiology of pituitary adenomas in Iceland, 1955–2012: A nationwide population-based study. Eur. J. Endocrinol. 2015, 173, 655–664. [Google Scholar] [CrossRef]
- Larouche, V.; Correa, J.A.; Cassidy, P.; Beauregard, C.; Garfield, N.; Rivera, J. Prevalence of autoimmune disease in patients with prolactinomas and non-functioning pituitary adenomas. Pituitary 2016, 19, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Delgrange, E.; Trouillas, J.; Maiter, D.; Donckier, J.; Tourniaire, J. Sex-related difference in the growth of prolactinomas: A clinical and proliferation marker study. J. Clin. Endocrinol. Metab. 1997, 82, 2102–2107. [Google Scholar] [CrossRef] [PubMed]
- Delemer, B. Adénomes à prolactine: Diagnostic et prise en charge. Presse Médicale 2009, 38, 117–124. [Google Scholar] [CrossRef]
- Recouvreux, M.V.; Faraoni, E.Y.; Camilletti, M.A.; Ratner, L.; Abeledo-Machado, A.; Rulli, S.B.; Díaz-Torga, G. Sex differences in the pituitary TGFβ1 system: The role of TGFβ1 in prolactinoma development. Front. Neuroendocrinol. 2018, 50, 118–122. [Google Scholar] [CrossRef]
- Kuroda, S.; Yonekawa, Y.; Kawano, T. Pituitary prolactinoma associated with polycystic ovary—case report. Neurol. Med. Chir. 1991, 31, 736–739. [Google Scholar] [CrossRef]
- De, A.; Morgan, T.E.; Speth, R.C.; Boyadjieva, N.; Sarkar, D.K. Pituitary lactotrope expresses transforming growth factor beta (TGF beta) type II receptor mRNA and protein and contains 125I-TGF beta 1 binding sites. J. Endocrinol. 1996, 149, 19–27. [Google Scholar] [CrossRef]
- Vilar, L.; Abucham, J.; Albuquerque, J.L.; Araujo, L.A.; Azevedo, M.F.; Boguszewski, C.L.; Casulari, L.A.; Cunha, M.B.C.; Czepielewski, M.A.; Duarte, F.H.G. Controversial issues in the management of hyperprolactinemia and prolactinomas—An overview by the Neuroendocrinology Department of the Brazilian Society of Endocrinology and Metabolism. Arch. Endocrinol. Metab. 2018, 62, 236–263. [Google Scholar] [CrossRef] [PubMed]
- Casanueva, F.F.; Molitch, M.E.; Schlechte, J.A.; Abs, R.; Bonert, V.; Bronstein, M.D.; Brue, T.; Cappabianca, P.; Colao, A.; Fahlbusch, R. Guidelines of the Pituitary Society for the diagnosis and management of prolactinomas. Clin. Endocrinol. 2006, 65, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Chambeh, W. les Prolactinomes Modalités de Diagnostic, de Suivi et de Prise en Charge: À Propos de 37 Cas; Faculté de Medecine de Sousse: Sousse, Tunisia, 2009. [Google Scholar]
- Espinosa, E.; Sosa, E.; Mendoza, V.; Ramírez, C.; Melgar, V.; Mercado, M. Giant prolactinomas: Are they really different from ordinary macroprolactinomas? Endocrine 2016, 52, 652–659. [Google Scholar] [CrossRef] [PubMed]
- Maiter, D.; Delgrange, E. Therapy of endocrine disease: The challenges in managing giant prolactinomas. Eur. J. Endocrinol. 2014, 170, R213–R227. [Google Scholar] [CrossRef] [PubMed]
- Shimon, I.; Sosa, E.; Mendoza, V.; Greenman, Y.; Tirosh, A.; Espinosa, E.; Popovic, V.; Glezer, A.; Bronstein, M.D.; Mercado, M. Giant prolactinomas larger than 60 mm in size: A cohort of massive and aggressive prolactin-secreting pituitary adenomas. Pituitary 2016, 19, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Arafah, B.M.; Nasrallah, M.P. Pituitary tumors: Pathophysiology, clinical manifestations and management. Endocr. Relat. Cancer 2001, 8, 287–305. [Google Scholar] [CrossRef] [PubMed]
- Sibal, L.; Ugwu, P.; Kendall-Taylor, P.; Ball, S.G.; James, R.A.; Pearce, S.H.S.; Hall, K.; Quinton, R. Medical therapy of macroprolactinomas in males:, I. Prevalence of hypopituitarism at diagnosis. II. Proportion of cases exhibiting recovery of pituitary function. Pituitary 2002, 5, 243–246. [Google Scholar] [CrossRef]
- Tirosh, A.; Benbassat, C.; Lifshitz, A.; Shimon, I. Hypopituitarism patterns and prevalence among men with macroprolactinomas. Pituitary 2015, 18, 108–115. [Google Scholar] [CrossRef]
- Behan, L.A.; Moyles, P.; Cuesta, M.; Rogers, B.; Crowley, R.K.; Ryan, J.; Brennan, P.; Smith, D.; Tormey, W.; Sherlock, M.; et al. The incidence of anterior pituitary hormone deficiencies in patients with microprolactinoma and idiopathic hyperprolactinaemia. Clin. Endocrinol. 2017, 87, 257–263. [Google Scholar] [CrossRef]
- Mychka, V.B.; Chazova, I.E.; Dmitriev, V.V.; Masenko, V.P. Role of hypothalamo-hypophyseal-adrenal axis in the pathogenesis of arterial hypertension in patients with prolactinoma of the anterior lobe of the hypophysis. Ter. Arkh. 2000, 72, 10–13. [Google Scholar] [PubMed]
- Arafah, B.M.; Prunty, D.; Ybarra, J.; Hlavin, M.L.; Selman, W.R. The dominant role of increased intrasellar pressure in the pathogenesis of hypopituitarism, hyperprolactinemia, and headaches in patients with pituitary adenomas. J. Clin. Endocrinol. Metab. 2000, 85, 1789–1793. [Google Scholar]
- Berinder, K.; Nyström, T.; Höybye, C.; Hall, K.; Hulting, A.-L. Insulin sensitivity and lipid profile in prolactinoma patients before and after normalization of prolactin by dopamine agonist therapy. Pituitary 2011, 14, 199–207. [Google Scholar] [CrossRef]
- dos Santos Silva, C.M.; Barbosa, F.R.P.; Lima, G.A.B.; Warszawski, L.; Fontes, R.; Domingues, R.C.; Gadelha, M.R. BMI and metabolic profile in patients with prolactinoma before and after treatment with dopamine agonists. Obesity 2011, 19, 800–805. [Google Scholar] [CrossRef] [PubMed]
- Araújo, C.; Marques, O.; Almeida, R.; Santos, M.J. Macroprolactinomas: Longitudinal assessment of biochemical and imaging therapeutic responses. Endocrine 2018, 62, 470–476. [Google Scholar] [CrossRef]
- Jethwa, P.R.; Patel, T.D.; Hajart, A.F.; Eloy, J.A.; Couldwell, W.T.; Liu, J.K. Cost-Effectiveness Analysis of Microscopic and Endoscopic Transsphenoidal Surgery Versus Medical Therapy in the Management of Microprolactinoma in the United States. World Neurosurg. 2016, 87, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Iglesias, P.; Rodríguez Berrocal, V.; Díez, J.J. Giant pituitary adenoma: Histological types, clinical features and therapeutic approaches. Endocrine 2018, 61, 407–421. [Google Scholar] [CrossRef] [PubMed]
- Buchfelder, M.; Schlaffer, S. Surgical treatment of pituitary tumours. Best Pract. Res. Clin. Endocrinol. Metab. 2009, 23, 677–692. [Google Scholar] [CrossRef]
- Ikeda, H.; Watanabe, K.; Tominaga, T.; Yoshimoto, T. Transsphenoidal microsurgical results of female patients with prolactinomas. Clin. Neurol. Neurosurg. 2013, 115, 1621–1625. [Google Scholar] [CrossRef]
- Colao, A.; Vitale, G.; Cappabianca, P.; Briganti, F.; Ciccarelli, A.; De Rosa, M.; Zarrilli, S.; Lombardi, G. Outcome of cabergoline treatment in men with prolactinoma: Effects of a 24-month treatment on prolactin levels, tumor mass, recovery of pituitary function, and semen analysis. J. Clin. Endocrinol. Metab. 2004, 89, 1704–1711. [Google Scholar] [CrossRef] [PubMed]
- Rastogi, A.; Bhansali, A.; Dutta, P.; Singh, P.; Vijaivergiya, R.; Gupta, V.; Sachdeva, N.; Bhadada, S.K.; Walia, R. A comparison between intensive and conventional cabergoline treatment of newly diagnosed patients with macroprolactinoma. Clin. Endocrinol. 2013, 79, 409–415. [Google Scholar] [CrossRef]
- Vroonen, L.; Jaffrain-Rea, M.-L.; Petrossians, P.; Tamagno, G.; Chanson, P.; Vilar, L.; Borson-Chazot, F.; Naves, L.A.; Brue, T.; Gatta, B.; et al. Prolactinomas resistant to standard doses of cabergoline: A multicenter study of 92 patients. Eur. J. Endocrinol. 2012, 167, 651–662. [Google Scholar] [CrossRef]
- Wu, Z.B.; Yu, C.J.; Su, Z.P.; Zhuge, Q.C.; Wu, J.S.; Zheng, W.M. Bromocriptine treatment of invasive giant prolactinomas involving the cavernous sinus: Results of a long-term follow up. J. Neurosurg. 2006, 104, 54–61. [Google Scholar] [CrossRef] [PubMed]
- de Castro, L.F.; Magalhães Gonzaga, M.d.F.; Naves, L.A.; Luiz Mendonça, J.; Oton de Lima, B.; Casulari, L.A. Beneficial Effects of High Doses of Cabergoline in the Treatment of Giant Prolactinoma Resistant to Dopamine Agonists: A Case Report with a 21-Year Follow-Up. Horm. Res. Paediatr. 2018, 89, 63–70. [Google Scholar] [CrossRef]
- Berwaerts, J.; Verhelst, J.; Abs, R.; Appel, B.; Mahler, C. A giant prolactinoma presenting with unilateral exophthalmos: Effect of cabergoline and review of the literature. J. Endocrinol. Investig. 2000, 23, 393–398. [Google Scholar] [CrossRef]
- Davis, J.R.; Sheppard, M.C.; Heath, D.A. Giant invasive prolactinoma: A case report and review of nine further cases. QJM Int. J. Med. 1990, 74, 227–238. [Google Scholar]
- Andujar-Plata, P.; Villar-Taibo, R.; Ballesteros-Pomar, M.D.; Vidal-Casariego, A.; Pérez-Corral, B.; Cabezas-Agrícola, J.M.; Álvarez-Vázquez, P.; Serramito, R.; Bernabeu, I. Long-term outcome of multimodal therapy for giant prolactinomas. Endocrine 2017, 55, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Dekkers, O.M.; Lagro, J.; Burman, P.; Jørgensen, J.O.; Romijn, J.A.; Pereira, A.M. Recurrence of Hyperprolactinemia after Withdrawal of Dopamine Agonists: Systematic Review and Meta-Analysis. J. Clin. Endocrinol. Metab. 2010, 95, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Delgrange, E.; Daems, T.; Verhelst, J.; Abs, R.; Maiter, D. Characterization of resistance to the prolactin-lowering effects of cabergoline in macroprolactinomas: A study in 122 patients. Eur. J. Endocrinol. 2009, 160, 747–752. [Google Scholar] [CrossRef] [PubMed]
- Kukstas, L.A.; Domec, C.; Bascles, L.; Bonnet, J.; Verrier, D.; Israel, J.M.; Vincent, J.-D. Different expression of the two dopaminergic D2 receptors, D2415 and D2444, in two types of lactotroph each characterised by their response to dopamine, and modification of expression by sex steroids. Endocrinology 1991, 129, 1101–1103. [Google Scholar] [CrossRef]
- Kovacs, K.; Stefaneanu, L.; Horvath, E.; Buchfelder, M.; Fahlbusch, R.; Becker, W. Prolactin-producing pituitary tumor: Resistance to dopamine agonist therapy. J. Neurosurg. 1995, 82, 886–890. [Google Scholar] [CrossRef] [PubMed]
- Barlier, A.; Pellegrini-Bouiller, I.; Caccavelli, L.; Gunz, G.; Morange-Ramos, I.; Jaquet, P.; Enjalbert, A. Abnormal transduction mechanisms in pituitary adenomas. Horm. Res. 1997, 47, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Prior, J.C.; Cox, T.A.; Fairholm, D.; Kostashuk, E.; Nugent, R. Testosterone-related exacerbation of a prolactin-producing macroadenoma: Possible role for estrogen. J. Clin. Endocrinol. Metab. 1987, 64, 391–394. [Google Scholar] [CrossRef]
- Hu, B.; Mao, Z.; Jiang, X.; He, D.; Wang, Z.; Wang, X.; Zhu, Y.; Wang, H. Role of TGF-β1/Smad3-mediated fibrosis in drug resistance mechanism of prolactinoma. Brain Res. 2018, 1698, 204–212. [Google Scholar] [CrossRef]
- Dogansen, S.C.; Selcukbiricik, O.S.; Tanrikulu, S.; Yarman, S. Withdrawal of dopamine agonist therapy in prolactinomas: In which patients and when? Pituitary 2016, 19, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, M.; Souteiro, P.; Carvalho, D. Prolactinoma management: Predictors of remission and recurrence after dopamine agonists withdrawal. Pituitary 2017, 20, 464–470. [Google Scholar] [CrossRef]
- Colao, A.; Di Sarno, A.; Guerra, E.; Pivonello, R.; Cappabianca, P.; Caranci, F.; Elefante, A.; Cavallo, L.M.; Briganti, F.; Cirillo, S.; et al. Predictors of remission of hyperprolactinaemia after long-term withdrawal of cabergoline therapy. Clin. Endocrinol. 2007, 67, 426–433. [Google Scholar] [CrossRef]
- Romijn, J.A. Hyperprolactinemia and prolactinoma. Handb. Clin. Neurol. 2014, 124, 185–195. [Google Scholar] [PubMed]
- Colao, A.; Lombardi, G.; Annunziato, L. Cabergoline. Expert. Opin. Pharmacother. 2000, 1, 555–574. [Google Scholar] [CrossRef]
- Webster, J.; Piscitelli, G.; Polli, A.; Ferrari, C.I.; Ismail, I.; Scanlon, M.F. A comparison of cabergoline and bromocriptine in the treatment of hyperprolactinemic amenorrhea. Cabergoline Comparative Study Group. N. Engl. J. Med. 1994, 331, 904–909. [Google Scholar] [CrossRef]
- Rutkowski, M.J.; Aghi, M.K. Medical versus surgical treatment of prolactinomas: An analysis of treatment outcomes. Expert. Rev. Endocrinol. Metab. 2018, 13, 25–33. [Google Scholar] [CrossRef]
- Hofstetter, C.P.; Shin, B.J.; Mubita, L.; Huang, C.; Anand, V.K.; Boockvar, J.A.; Schwartz, T.H. Endoscopic endonasal transsphenoidal surgery for functional pituitary adenomas. Neurosurg. Focus. 2011, 30, E10. [Google Scholar] [CrossRef] [PubMed]
- Amar, A.P.; Couldwell, W.T.; Chen, J.C.T.; Weiss, M.H. Predictive value of serum prolactin levels measured immediately after transsphenoidal surgery. J. Neurosurg. 2002, 97, 307–314. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| G1 | G2 | G3 | Total | p | |
|---|---|---|---|---|---|
| Overweight and/or obese | 19 (70.3%) | 19 (59.3%) | 17 (94.4%) | 55 (71.4%) | 0.029 |
| Mean waist size in women (cm) | 87.3 | 95.6 | 113 | 93.8 | 0.006 |
| Mean waist size in men (cm) | 106 | 96.4 | 98.5 | 98.4 | 0.051 |
| G1 | G2 | G3 | Total | p | |
|---|---|---|---|---|---|
| Dyslipidemia | 14 (51.8%) | 16 (50%) | 12 (70.5%) | 42 (54.5%) | 0.454 |
| FHG/ICH | 0% | 4 (12.5%) | 5 (29.4%) | 9 (11.6%) | 0.042 |
| Metabolic syndrome | 6 (22.2%) | 12 (37.5%) | 10 (58.8%) | 28 (36.3%) | 0.042 |
| Mean | G1 | G2 | G3 | p |
|---|---|---|---|---|
| FSH (IU/mL) | 11.4 | 4.1 | 2.9 | 0.049 |
| LH (IU/mL) | 9.5 | 2.9 | 1.1 | 0.004 |
| Testosterone (ng/mL) | 1.4 | 1.9 | 0.9 | 0.266 |
| G1 | G2 | G3 | p | |
|---|---|---|---|---|
| Hypogonadotropic hypogonadism | 14 (26%) | 22 (42.3%) | 17 (32.7%) | 0.008 |
| Central hypothyroidism | 2 (14.3%) | 5 (35.7%) | 7 (50%) | 0.028 |
| Corticotroph deficiency | 3 (9.4%) | 14 (43.8%) | 15 (46.9%) | 0.000 |
| Three-axis deficit | 1 (9%) | 4 (36.3%) | 6 (54.5%) | 0.002 |
| Medical Treatment Only | Surgical Treatment | |
|---|---|---|
| G1 | 25 (92.5%) | 2 (7.4%) |
| G2 | 20 (62.5%) | 12 (37.5%) |
| G3 | 11 (61.1%) | 7 (38.8%) |
| p | 0.082 | 0.024 |
| G1 | G2 | G3 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Dosage Timing | N | M | % | N | M | % | N | M | % | p |
| Pre-therapeutic | 26 | 164.1 | 0 | 32 | 523.4 | 0 | 18 | 10,569.1 | 0 | 0.000 |
| After 1 month | 10 | 71.8 | 33.3% | 11 | 689.7 | 33.3% | 9 | 4594.9 | 33.3% | 0.989 |
| After 6 months | 20 | 41.5 | 30% | 23 | 97.8 | 50% | 13 | 726.7 | 20% | 0.598 |
| After 1 year | 18 | 56.1 | 50% | 21 | 136 | 38.5% | 5 | 1315 | 11.5% | 0.283 |
| Remission (N = 10) | Resistance (N = 10) | |
|---|---|---|
| Men | 4 (40%) | 4 (40%) |
| Women | 6 (60%) | 6 (60%) |
| Under cabergoline | 5 (50%) | 0% |
| Under bromocriptine | 0% | 10 (100%) |
| Mean treatment duration before remission | 6.2 ± 2.6 years | N/A |
| G1 | 4 (40%) | 0% |
| G2 | 4 (40%) | 7(70%) |
| G3 | 2 (20%) | 3 (30%) |
| Prolactin Normalization During Follow-Up | >50% Diameter Reduction | |||
|---|---|---|---|---|
| No = 32 (41.5%) | Yes = 45 (58.4%) | No = 42 (53.3%) | Yes = 35 (46.7%) | |
| G1 | 8 (29.6%) | 19 (70.3%) | 17 (63%) | 10 (37.3%) |
| G2 | 13 (40.6%) | 19 (59.3%) | 10 (31.2%) | 22 (68.7%) |
| G3 | 11 (6.1%) | 7 (38.8%) | 15 (83.3%) | 3 (16.6%) |
| p | 0.076 | 0.001 | ||
| Mean maximal dose of BC (mg) | 7.72 | 6.71 | 7.07 | 7.4 |
| p | 0.39 | 0.49 | ||
| Mean maximal dose of CB (mg) | 0.91 | 0.68 | 0.78 | 0.79 |
| p | 0.16 | 0.780 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elleuch, M.; Frikha, H.; Loukil, F.; Boujelben, K.; Ben Salah, D.; Rekik, N.M. Impact of Tumor Size on Prolactinoma Characteristics and Treatment Outcomes: A Study of a Tunisian Cohort. Biomedicines 2025, 13, 1125. https://doi.org/10.3390/biomedicines13051125
Elleuch M, Frikha H, Loukil F, Boujelben K, Ben Salah D, Rekik NM. Impact of Tumor Size on Prolactinoma Characteristics and Treatment Outcomes: A Study of a Tunisian Cohort. Biomedicines. 2025; 13(5):1125. https://doi.org/10.3390/biomedicines13051125
Chicago/Turabian StyleElleuch, Mouna, Hamdi Frikha, Fatma Loukil, Khouloud Boujelben, Dhouha Ben Salah, and Nabila Mejdoub Rekik. 2025. "Impact of Tumor Size on Prolactinoma Characteristics and Treatment Outcomes: A Study of a Tunisian Cohort" Biomedicines 13, no. 5: 1125. https://doi.org/10.3390/biomedicines13051125
APA StyleElleuch, M., Frikha, H., Loukil, F., Boujelben, K., Ben Salah, D., & Rekik, N. M. (2025). Impact of Tumor Size on Prolactinoma Characteristics and Treatment Outcomes: A Study of a Tunisian Cohort. Biomedicines, 13(5), 1125. https://doi.org/10.3390/biomedicines13051125