
The Role of Glycemic Control in Inflammation Markers and Clinical Outcomes in Type 2 Diabetes Patients with Severe COVID-19

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Patient Selection and Grouping
2.3. Data Collection and Variables
2.4. Statistical Analysis
3. Results
Demographics
4. Discussion
4.1. Analysis of Findings
4.2. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sarker, R.; Roknuzzaman, A.S.M.; Nazmunnahar Shahriar, M.; Hossain, M.J.; Islam, M.R. The WHO has declared the end of pandemic phase of COVID-19: Way to come back in the normal life. Health Sci. Rep. 2023, 6, e1544. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cheng, K.; Wu, C.; Gu, S.; Lu, Y.; Wu, H.; Li, C. WHO declares the end of the COVID-19 global health emergency: Lessons and recommendations from the perspective of ChatGPT/GPT-4. Int. J. Surg. 2023, 109, 2859–2862. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhang, J.J.; Dong, X.; Liu, G.H.; Gao, Y.D. Risk and Protective Factors for COVID-19 Morbidity, Severity, and Mortality. Clin. Rev. Allergy Immunol. 2023, 64, 90–107. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Atanasov, V.; Barreto, N.; Franchi, L.; Whittle, J.; Meurer, J.; Weston, B.W.; Luo, Q.E.; Yuan, A.Y.; Zhang, R.; Black, B. Evidence on COVID-19 Mortality and Disparities Using a Novel Measure, COVID excess mortality percentage: Evidence from Indiana, Wisconsin, and Illinois. PLoS ONE 2024, 19, e0295936. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Floyd, J.S.; Walker, R.L.; Kuntz, J.L.; Shortreed, S.M.; Fortmann, S.P.; Bayliss, E.A.; Harrington, L.B.; Fuller, S.; Albertson-Junkans, L.H.; Powers, J.D.; et al. Association Between Diabetes Severity and Risks of COVID-19 Infection and Outcomes. J. Gen. Intern. Med. 2023, 38, 1484–1492. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jin, S.; Hu, W. Severity of COVID-19 and Treatment Strategy for Patient With Diabetes. Front. Endocrinol. 2021, 12, 602735. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Schlesinger, S.; Lang, A.; Christodoulou, N.; Linnerz, P.; Pafili, K.; Kuss, O.; Herder, C.; Neuenschwander, M.; Barbaresko, J.; Roden, M. Risk phenotypes of diabetes and association with COVID-19 severity and death: An update of a living systematic review and meta-analysis. Diabetologia 2023, 66, 1395–1412. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wang, J.; Meng, W. COVID-19 and diabetes: The contributions of hyperglycemia. J. Mol. Cell Biol. 2020, 12, 958–962. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tsioufis, C.; Dimitriadis, K.; Tousoulis, D. The interplay of hypertension, ACE-2 and SARS-CoV-2: Emerging data as the “Ariadne’s thread” for the “labyrinth” of COVID-19. Hellenic J. Cardiol. 2020, 61, 31–33. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Seiglie, J.; Platt, J.; Cromer, S.J.; Bunda, B.; Foulkes, A.S.; Bassett, I.V.; Hsu, J.; Meigs, J.B.; Leong, A.; Putman, M.S.; et al. Diabetes as a Risk Factor for Poor Early Outcomes in Patients Hospitalized With COVID-19. Diabetes Care 2020, 43, 2938–2944. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chander, S.; Deepak, V.; Kumari, R.; Leys, L.; Wang, H.Y.; Mehta, P.; Sadarat, F. Glycemic Control in Critically Ill COVID-19 Patients: Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 2555. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Andor, M.; Man, D.E.; Nistor, D.C.; Buda, V.; Dragan, S. The Influence of COVID-19 in Glycemic Control: Predictive Value of Inflammation and Metabolic Parameters. Biomedicines 2024, 12, 2642. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Geetha, H.S.; Singh, G.; Sekar, A.; Gogtay, M.; Singh, Y.; Abraham, G.M.; Trivedi, N. Hyperglycemia in COVID-19 infection without diabetes mellitus: Association with inflammatory markers. World J. Clin. Cases 2023, 11, 1287–1298. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Beigmohammadi, M.T.; Amoozadeh, L.; Rezaei Motlagh, F.; Rahimi, M.; Maghsoudloo, M.; Jafarnejad, B.; Eslami, B.; Salehi, M.R.; Zendehdel, K. Mortality Predictive Value of APACHE II and SOFA Scores in COVID-19 Patients in the Intensive Care Unit. Can. Respir. J. 2022, 2022, 5129314. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Toker, İ.; Kılınç-Toker, A.; Turunç-Özdemir, A.; Altuntaş, M. Comparison of CURB-65 Pneumonia Severity Score, Quick COVID-19 Severity Index, and Brescia-COVID Respiratory Severity Scale in Emergently Hospitalized COVID-19 Patients with Pneumonia. Infect. Dis. Clin. Microbiol. 2022, 4, 244–251. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Leggat, P.A.; Frean, J.; Blumberg, L. COVID-19: Current Status and Future Prospects. Trop. Med. Infect. Dis. 2023, 8, 94. [Google Scholar] [CrossRef]
- Xia, W.; Tan, Y.; Hu, S.; Li, C.; Jiang, T. Predictive Value of Systemic Immune-Inflammation index and Neutrophil-to-Lymphocyte Ratio in Patients with Severe COVID-19. Clin. Appl. Thromb. Hemost. 2022, 28, 10760296221111391. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sayed, A.A. Assessing the Diagnostic Values of the Neutrophil-to-Lymphocyte Ratio (NLR) and Systematic Immunoinflammatory Index (SII) as Biomarkers in Predicting COVID-19 Severity: A Multicentre Comparative Study. Medicina 2024, 60, 602. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Girard, D.; Vandiedonck, C. How dysregulation of the immune system promotes diabetes mellitus and cardiovascular risk complications. Front. Cardiovasc. Med. 2022, 9, 991716. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Galicia-Garcia, U.; Benito-Vicente, A.; Jebari, S.; Larrea-Sebal, A.; Siddiqi, H.; Uribe, K.B.; Ostolaza, H.; Martín, C. Pathophysiology of Type 2 Diabetes Mellitus. Int. J. Mol. Sci. 2020, 21, 6275. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Feldman, E.L.; Savelieff, M.G.; Hayek, S.S.; Pennathur, S.; Kretzler, M.; Pop-Busui, R. COVID-19 and Diabetes: A Collision and Collusion of Two Diseases. Diabetes 2020, 69, 2549–2565. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Atwah, B.; Iqbal, M.S.; Kabrah, S.; Kabrah, A.; Alghamdi, S.; Tabassum, A.; Baghdadi, M.A.; Alzahrani, H. Susceptibility of Diabetic Patients to COVID-19 Infections: Clinico-Hematological and Complications Analysis. Vaccines 2023, 11, 561. [Google Scholar] [CrossRef] [PubMed]
- Nunes, J.P.L.; DeMarco, J.P. A 7.0–7.7% value for glycated haemoglobin is better than a <7% value as an appropriate target for patient-centered drug treatment of type 2 diabetes mellitus. Ann. Transl. Med. 2019, 7 (Suppl. 3), S122. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wang, P.; Huang, R.; Lu, S.; Xia, W.; Sun, H.; Sun, J.; Cai, R.; Wang, S. HbA1c below 7% as the goal of glucose control fails to maximize the cardiovascular benefits: A meta-analysis. Cardiovasc. Diabetol. 2015, 14, 124. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Prattichizzo, F.; de Candia, P.; Nicolucci, A.; Ceriello, A. Elevated HbA1c levels in pre-Covid-19 infection increases the risk of mortality: A sistematic review and meta-analysis. Diabetes Metab. Res. Rev. 2022, 38, e3476. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Yoroidaka, A.; Kurita, S.; Kita, T. HbA1c measurement may save COVID-19 inpatients from overlooked diabetes. J. Diabetes Investig. 2022, 13, 1925–1933. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Krishnasamy, S.; Sheikh, D.; Ali, T.; Clemons, V.; Furmanek, S.; Mohamed Fawzy Abdelhaleem, A.A.; Salunkhe, V.; Akbar, U.A.; Chlebowy, D.; Ramirez, J.; et al. Impact of Hyperglycemia on Cardiovascular Events and Clinical Outcomes in Patients Hospitalized With COVID-19 Pneumonia. Endocr. Pract. 2022, 28, 780–786. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tsikala Vafea, M.; Traboulsi, C.; Stefanovic-Racic, M. Lower Glycosylated Hemoglobin Is Associated With Lower In-Hospital Mortality in Patients With COVID-19: A Systematic Review of the Literature and Meta-Analysis. Endocr. Pract. 2024, 30, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Alhakak, A.; Butt, J.H.; Gerds, T.A.; Fosbøl, E.L.; Mogensen, U.M.; Krøll, J.; Pallisgaard, J.L.; Gislason, G.H.; Torp-Pedersen, C.; Køber, L.; et al. Glycated haemoglobin levels among 3295 hospitalized COVID-19 patients, with and without diabetes, and risk of severe infection, admission to an intensive care unit and all-cause mortality. Diabetes Obes. Metab. 2022, 24, 499–510. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhu, Z.; Mao, Y.; Chen, G. Predictive value of HbA1c for in-hospital adverse prognosis in COVID-19: A systematic review and meta-analysis. Prim. Care Diabetes 2021, 15, 910–917. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Barmanray, R.D.; Cheuk, N.; Fourlanos, S.; Greenberg, P.B.; Colman, P.G.; Worth, L.J. In-hospital hyperglycemia but not diabetes mellitus alone is associated with increased in-hospital mortality in community-acquired pneumonia (CAP): A systematic review and meta-analysis of observational studies prior to COVID-19. BMJ Open Diabetes Res. Care 2022, 10, e002880. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kandinata, S.G.; Soelistijo, S.A.; Pranoto, A.; Triyono, E.A. Random Blood Glucose, but Not HbA1c, Was Associated with Mortality in COVID-19 Patients with Type 2 Diabetes Mellitus-A Retrospective Study. Pathophysiology 2023, 30, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Berbudi, A.; Rahmadika, N.; Tjahjadi, A.I.; Ruslami, R. Type 2 Diabetes and its Impact on the Immune System. Curr. Diabetes Rev. 2020, 16, 442–449. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lee, J.; Yun, J.S.; Ko, S.H. Advanced Glycation End Products and Their Effect on Vascular Complications in Type 2 Diabetes Mellitus. Nutrients 2022, 14, 3086. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Steenblock, C.; Hassanein, M.; Khan, E.G.; Yaman, M.; Kamel, M.; Barbir, M.; Lorke, D.E.; Rock, J.A.; Everett, D.; Bejtullah, S.; et al. Diabetes and COVID-19: Short- and Long-Term Consequences. Horm. Metab. Res. 2022, 54, 503–509. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]

{kind=link}
{kind=link}
| Variable | Well-Controlled T2DM (n = 117) | Poorly Controlled T2DM (n = 64) | p-Value |
|---|---|---|---|
| Age (years) | 62.7 ± 10.6 | 63.9 ± 9.8 | 0.4 |
| Male (%) | 54.7% (64/117) | 59.4% (38/64) | 0.5 |
| Duration of T2DM (years) | 10.2 ± 4.8 | 10.4 ± 5.0 | 0.75 |
| BMI (kg/m2) | 28.4 ± 4.2 | 30.2 ± 3.9 | 0.006 |
| Hypertension (%) | 70.1% (82/117) | 75.0% (48/64) | 0.46 |
| CKD (%) | 16.2% (19/117) | 20.3% (13/64) | 0.46 |
| Marker | Well-Controlled (n = 117) | Poorly Controlled (n = 64) | p-Value | Mean Diff. [95% CI] |
|---|---|---|---|---|
| CRP (mg/L) | 78.6 ± 23.4 | 93.4 ± 24.7 | 0.002 | 14.8 [6.0, 23.6] |
| IL-6 (pg/mL) | 52.8 ± 15.9 | 64.2 ± 16.1 | 0.004 | 11.4 [4.0, 18.8] |
| Ferritin (µg/L) | 449.2 ± 136.5 | 524.7 ± 139.2 | 0.01 | 75.5 [15.2, 135.8] |
| Lymphocytes (×109/L) | 1.2 ± 0.4 | 1.0 ± 0.3 | 0.003 | −0.2 [−0.3, −0.1] |
| NLR | 5.7 ± 2.0 | 7.2 ± 2.3 | <0.001 | 1.5 [0.9, 2.1] |
| SII (×103) | 1039.3 ± 319.5 | 1344.7 ± 385.6 | <0.001 | 305.4 [148.2, 462.6] |
| Score | Well-Controlled (n = 117) | Poorly Controlled (n = 64) | Mean Diff. [95% CI] | Non-Diabetic COVID Control (n = 80) | p-Value (Well vs. Poor) | p-Value (All 3 Groups) |
|---|---|---|---|---|---|---|
| APACHE II | 14.1 ± 4.3 | 16.8 ± 4.8 | 2.7 [1.2, 4.2] | 13.2 ± 3.9 | 0.001 | 0.002 |
| CURB-65 | 2.1 ± 1.0 | 2.5 ± 1.1 | 0.4 [0.1, 0.7] | 1.8 ± 0.8 | 0.03 | 0.04 |
| NEWS | 6.6 ± 2.4 | 7.7 ± 2.7 | 1.1 [0.3, 1.9] | 5.9 ± 2.2 | 0.007 | 0.01 |
| Outcome | Well-Controlled (n = 117) | Poorly Controlled (n = 64) | Non-Diabetic Controls (n = 80) | Effect Size [95% CI] | p-Value (Well vs. Poor) | p-Value (All 3 Groups) |
|---|---|---|---|---|---|---|
| ICU Admission (%) | 22.2% (26/117) | 39.1% (25/64) | 15.0% (12/80) | OR 2.24 [1.15, 4.37] | 0.02 | 0.01 |
| Mechanical Ventilation (%) | 10.3% (12/117) | 18.8% (12/64) | 8.8% (7/80) | OR 2.02 [0.84, 4.89] | 0.10 | 0.12 |
| Mortality (%) | 6.0% (7/117) | 14.1% (9/64) | 4.7% (4/80) | OR 2.56 [0.97, 6.77] | 0.05 | 0.03 |
| Length of Stay (days) | 12.7 ± 4.2 | 14.4 ± 4.8 | 10.9 ± 4.0 | 1.7 [0.4, 3.0] | 0.01 | 0.01 |
| Subgroup | Well-Controlled T2DM | Poorly Controlled T2DM | Non-Diabetic Controls (n = 80) | Effect Size [95% CI] | p-Value (Well vs. Poor) | p-Value (All 3 Groups) |
|---|---|---|---|---|---|---|
| Age ≥ 65 years (%) | 46.2% (54/117) | 48.4% (31/64) | 45.0% (36/80) | OR 1.10 [0.65, 1.86] | 0.77 | 0.81 |
| ICU in Age ≥ 65 (%) | 29.6% (16/54) | 41.9% (13/31) | 25.0% (9/36) | OR 1.74 [0.69, 4.41] | 0.23 | 0.26 |
| Obesity (BMI ≥ 30 kg/m2) | 30.8% (36/117) | 48.4% (31/64) | 28.8% (23/80) | OR 2.16 [1.14, 4.10] | 0.02 | 0.03 |
| ICU in Obesity (%) | 25.0% (9/36) | 38.7% (12/31) | 17.4% (4/23) | OR 1.90 [0.62, 5.78] | 0.24 | 0.21 |
| Variable | Correlation Coefficient (r) | p-Value |
|---|---|---|
| CRP (mg/L) | 0.41 | <0.001 |
| IL-6 (pg/mL) | 0.45 | <0.001 |
| NLR | 0.38 | <0.001 |
| SII (×103) | 0.33 | 0.001 |
| APACHE II | 0.51 | <0.001 |
| CURB-65 | 0.31 | 0.001 |
| NEWS | 0.36 | <0.001 |
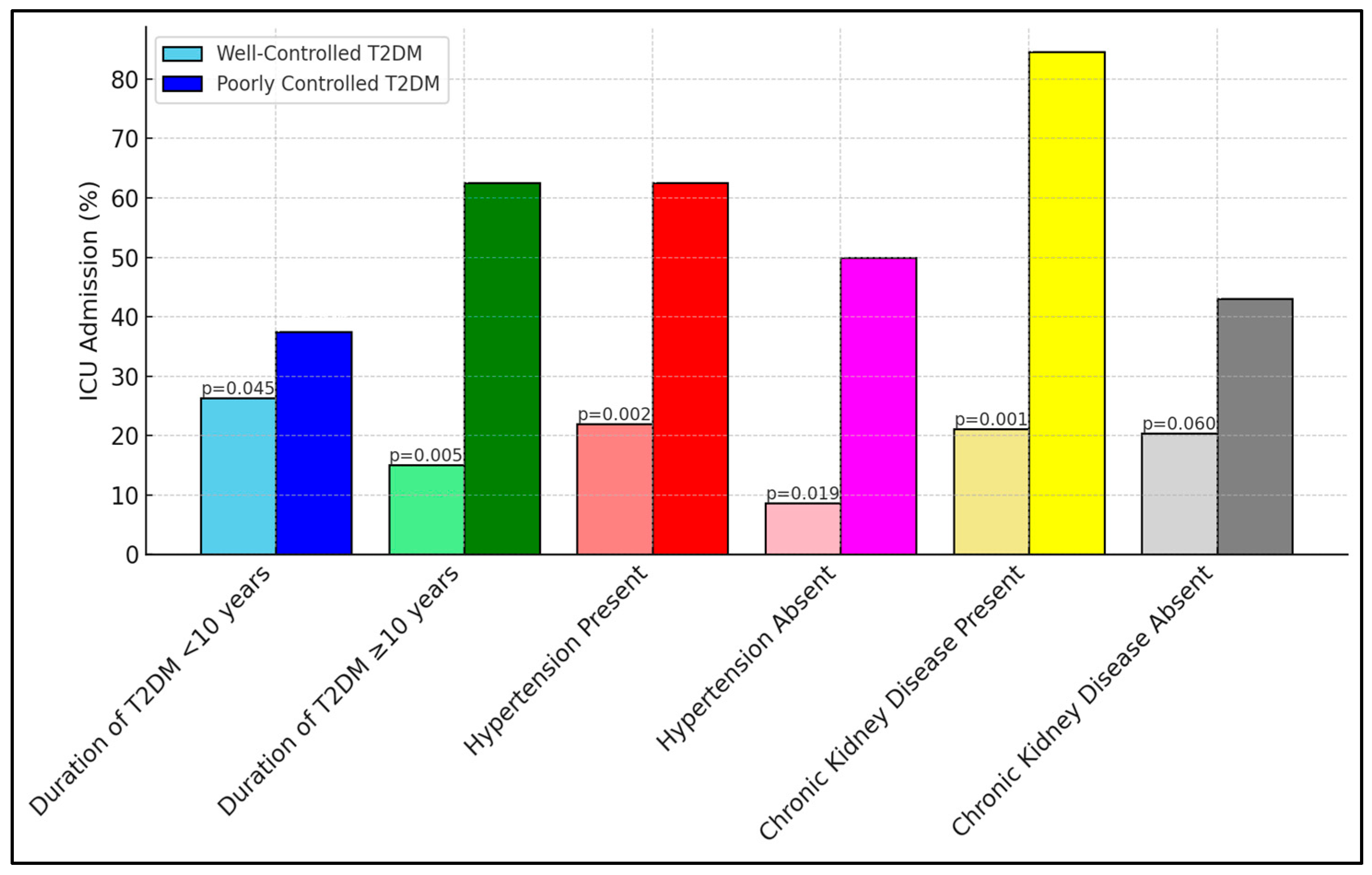
| Subgroup | Well-Controlled T2DM ICU Admission (%) | Poorly Controlled T2DM ICU Admission (%) | p-Value |
|---|---|---|---|
| Duration of T2DM <10 years | 15/57 (26.3%) | 12/32 (37.5%) | 0.045 |
| Duration of T2DM ≥ 10 years | 9/60 (15.0%) | 20/32 (62.5%) | 0.005 |
| Hypertension Present | 18/82 (22.0%) | 30/48 (62.5%) | 0.002 |
| Hypertension Absent | 3/35 (8.6%) | 8/16 (50.0%) | 0.019 |
| Chronic Kidney Disease Present | 4/19 (21.1%) | 11/13 (84.6%) | 0.001 |
| Chronic Kidney Disease Absent | 20/98 (20.4%) | 22/51 (43.1%) | 0.06 |
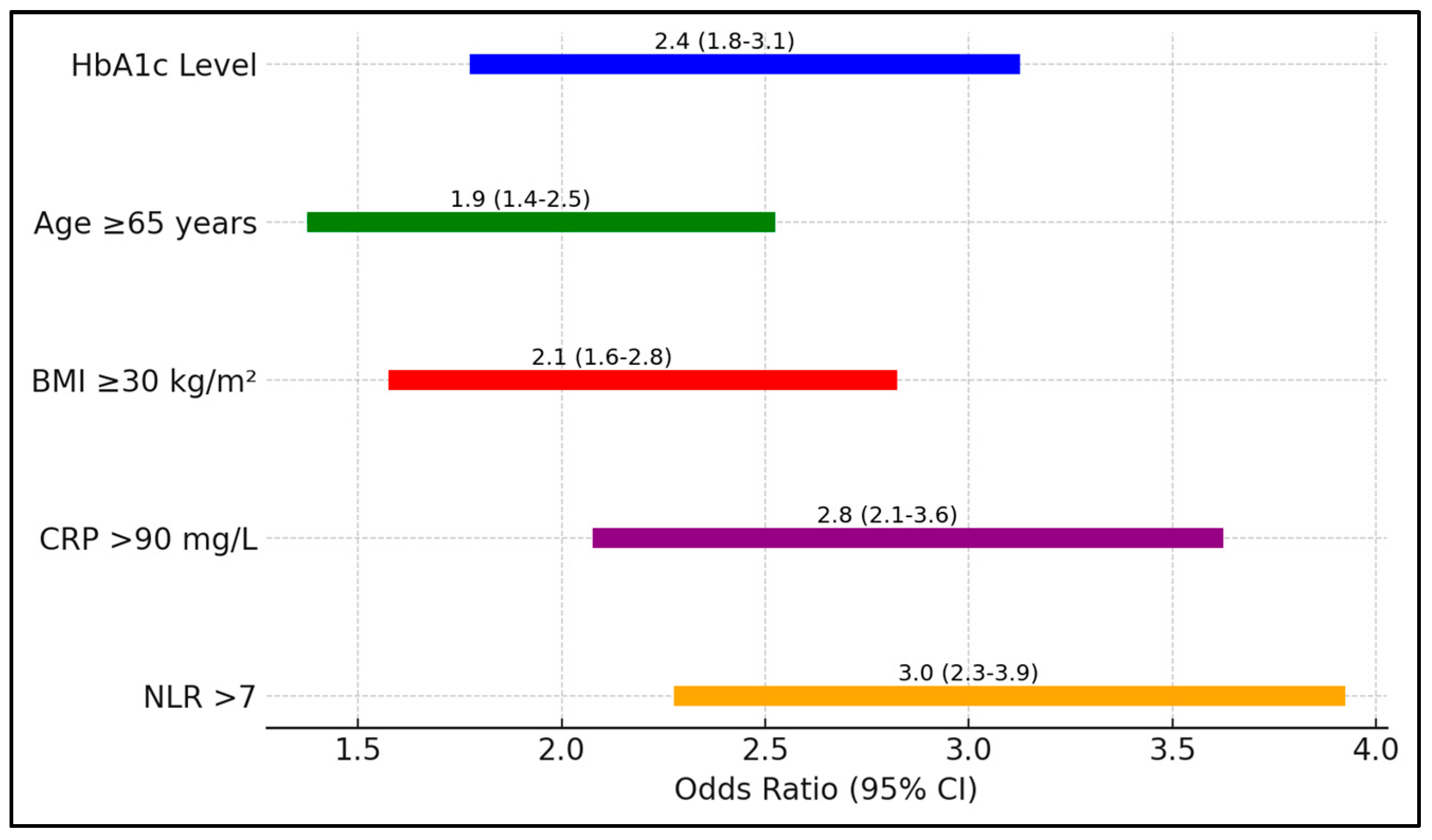
| Risk Factor | Odds Ratio (95% CI) | p-Value |
|---|---|---|
| HbA1c Level | 2.4 (1.8–3.1) | 0.001 |
| Age ≥ 65 years | 1.9 (1.4–2.5) | 0.003 |
| BMI ≥ 30 kg/m2 | 2.1 (1.6–2.8) | 0.002 |
| CRP > 90 mg/L | 2.8 (2.1–3.6) | 0.0005 |
| NLR > 7 | 3.0 (2.3–3.9) | 0.0003 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Craciun, L.; Ignuta, F.; Rayudu, U.S.; Afra, M.; Rosca, O.; Vlad, A.; Aburel, O.; Velimirovici, D.E. The Role of Glycemic Control in Inflammation Markers and Clinical Outcomes in Type 2 Diabetes Patients with Severe COVID-19. Biomedicines 2025, 13, 886. https://doi.org/10.3390/biomedicines13040886
Craciun L, Ignuta F, Rayudu US, Afra M, Rosca O, Vlad A, Aburel O, Velimirovici DE. The Role of Glycemic Control in Inflammation Markers and Clinical Outcomes in Type 2 Diabetes Patients with Severe COVID-19. Biomedicines. 2025; 13(4):886. https://doi.org/10.3390/biomedicines13040886
Chicago/Turabian StyleCraciun, Lavinia, Flavia Ignuta, Uma Shailendri Rayudu, Maliha Afra, Ovidiu Rosca, Adrian Vlad, Oana Aburel, and Dana Emilia Velimirovici. 2025. "The Role of Glycemic Control in Inflammation Markers and Clinical Outcomes in Type 2 Diabetes Patients with Severe COVID-19" Biomedicines 13, no. 4: 886. https://doi.org/10.3390/biomedicines13040886
APA StyleCraciun, L., Ignuta, F., Rayudu, U. S., Afra, M., Rosca, O., Vlad, A., Aburel, O., & Velimirovici, D. E. (2025). The Role of Glycemic Control in Inflammation Markers and Clinical Outcomes in Type 2 Diabetes Patients with Severe COVID-19. Biomedicines, 13(4), 886. https://doi.org/10.3390/biomedicines13040886