
Fragmented QRS in Lateral Leads on Electrocardiography Is Associated with Cardiac Dysfunction and Left Ventricular Dilation in Duchenne Muscular Dystrophy

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Recruitment
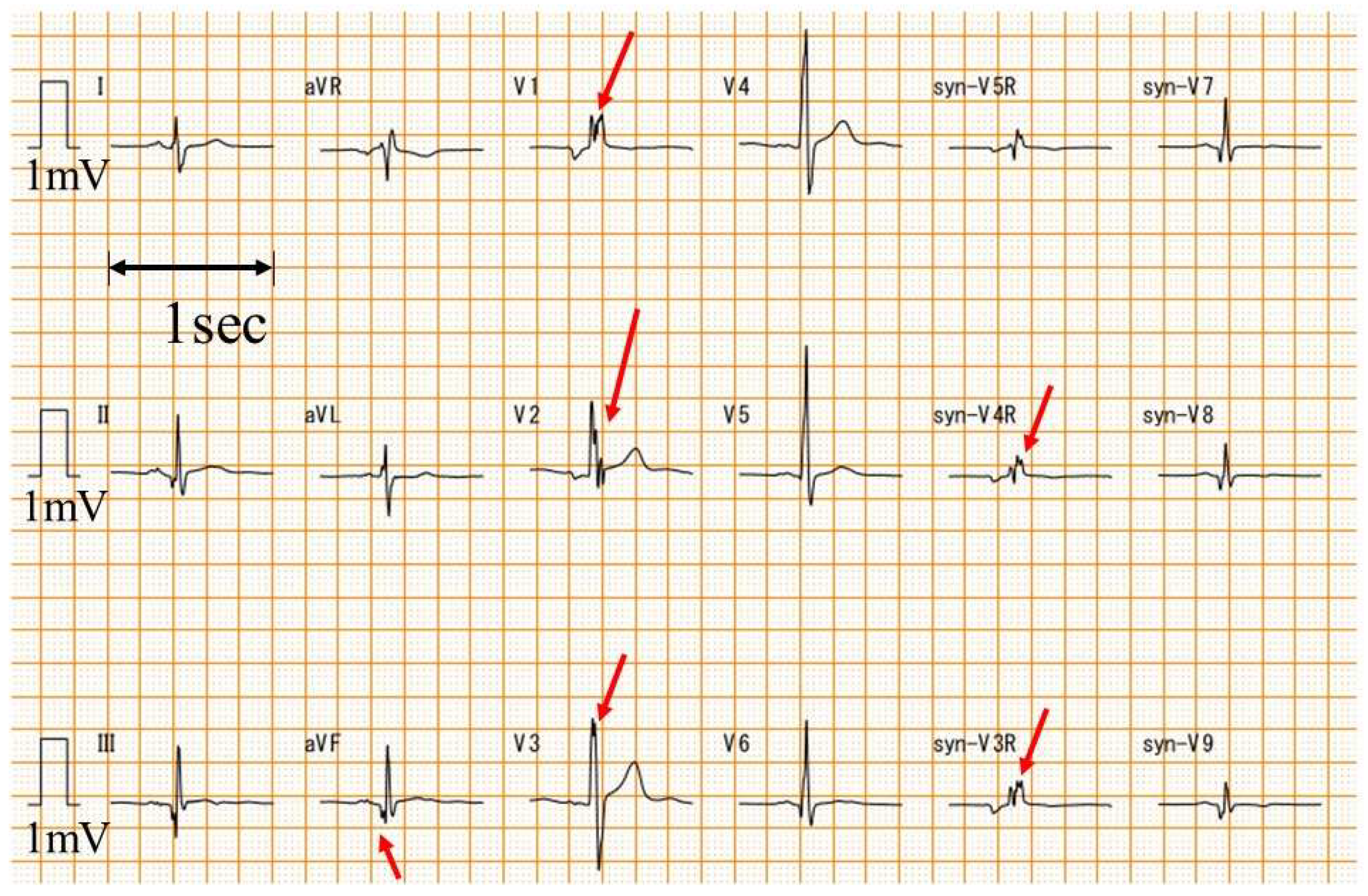
2.2. Electrocardiography
2.3. Echocardiography
2.4. Statistical Analysis
2.5. Ethics
3. Results
3.1. Patients
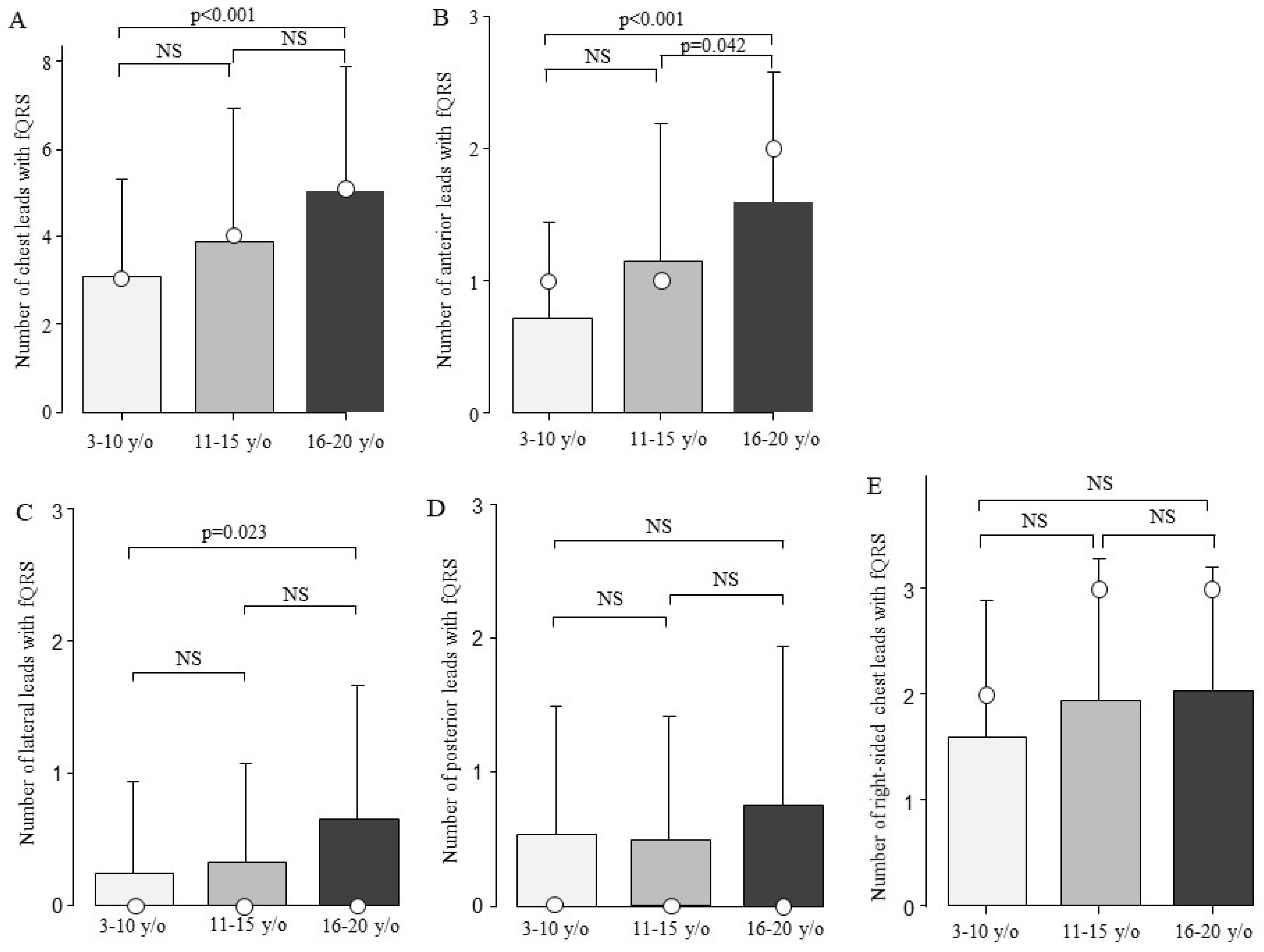
3.2. Number of fQRSs
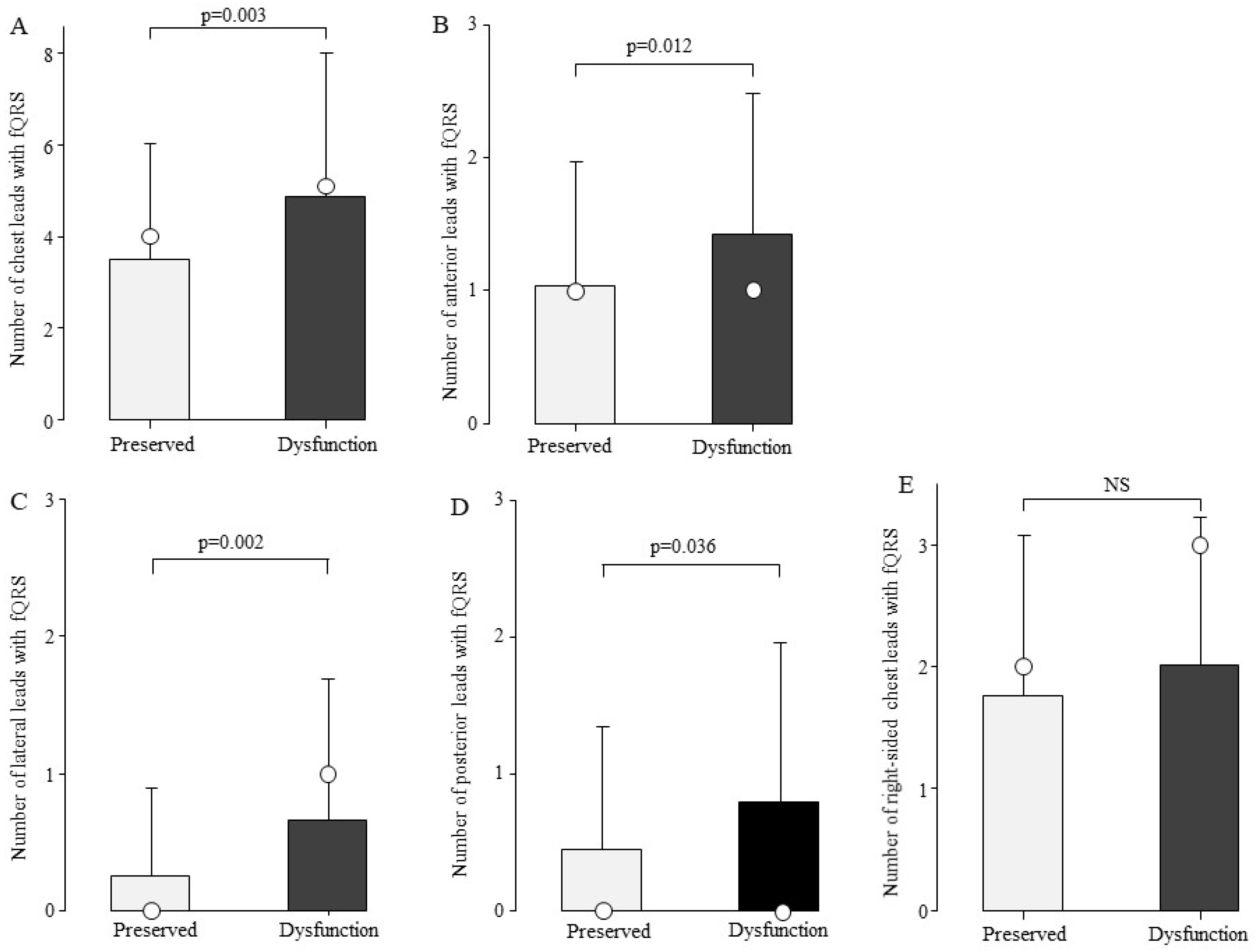
3.3. Relationship Between the Number of fQRS and Cardiac Function
3.4. Relationship Between the Number of fQRS and LV Dilation
3.5. Independent Determinants Related to Cardiac Dysfunction and LV Dilation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BPM | Beats Per Minute |
| CK | Creatine Kinase |
| DMD | Duchenne Muscular Dystrophy |
| ECG | Electrocardiography |
| fQRS | Fragmented QRS |
| HR | Heart Rate |
| IU/L | International Units per Liter |
| LV | Left Ventricle |
| LVEF | Left Ventricular Ejection Fraction |
| MRI | Magnetic Resonance Imaging |
| SD | Standard Deviation |
References
- Norwood, F.L.; Harling, C.; Chinnery, P.F.; Eagle, M.; Bushby, K.; Straub, V. Prevalence of genetic muscle disease in Northern England: In-depth analysis of a muscle clinic population. Brain 2009, 132, 3175–3186. [Google Scholar] [CrossRef] [PubMed]
- Passamano, L.; Taglia, A.; Palladino, A.; Viggiano, E.; D’Ambrosio, P.; Scutifero, M.; Rosaria Cecio, M.; Torre, V.; Luca, F.D.E.; Picillo, E.; et al. Improvement of survival in Duchenne Muscular Dystrophy: Retrospective analysis of 835 patients. Acta Myol. Myopathies Cardiomyopathies Off. J. Mediterr. Soc. Myol. 2012, 31, 121–125. [Google Scholar]
- Rall, S.; Grimm, T. Survival in Duchenne muscular dystrophy. Acta Myol. Myopathies Cardiomyopathies Off. J. Mediterr. Soc. Myol. 2012, 31, 117–120. [Google Scholar]
- Ishikawa, Y.; Miura, T.; Ishikawa, Y.; Aoyagi, T.; Ogata, H.; Hamada, S.; Minami, R. Duchenne muscular dystrophy: Survival by cardio-respiratory interventions. Neuromuscul. Disord. NMD 2011, 21, 47–51. [Google Scholar] [CrossRef] [PubMed]
- Birnkrant, D.J.; Bushby, K.; Bann, C.M.; Alman, B.A.; Apkon, S.D.; Blackwell, A.; Case, L.E.; Cripe, L.; Hadjiyannakis, S.; Olson, A.K.; et al. Diagnosis and management of Duchenne muscular dystrophy, part 2: Respiratory, cardiac, bone health, and orthopaedic management. Lancet Neurol. 2018, 17, 347–361. [Google Scholar] [CrossRef] [PubMed]
- Wahlgren, L.; Kroksmark, A.K.; Tulinius, M.; Sofou, K. One in five patients with Duchenne muscular dystrophy dies from other causes than cardiac or respiratory failure. Eur. J. Epidemiol. 2022, 37, 147–156. [Google Scholar] [CrossRef]
- Silva, M.C.; Meira, Z.M.; Gurgel Giannetti, J.; da Silva, M.M.; Campos, A.F.; Barbosa Mde, M.; Starling Filho, G.M.; Ferreira Rde, A.; Zatz, M.; Rochitte, C.E. Myocardial delayed enhancement by magnetic resonance imaging in patients with muscular dystrophy. J. Am. Coll. Cardiol. 2007, 49, 1874–1879. [Google Scholar] [CrossRef]
- Puchalski, M.D.; Williams, R.V.; Askovich, B.; Sower, C.T.; Hor, K.H.; Su, J.T.; Pack, N.; Dibella, E.; Gottliebson, W.M. Late gadolinium enhancement: Precursor to cardiomyopathy in Duchenne muscular dystrophy? Int. J. Cardiovasc. Imaging 2009, 25, 57–63. [Google Scholar] [CrossRef]
- Verhaert, D.; Richards, K.; Rafael-Fortney, J.A.; Raman, S.V. Cardiac involvement in patients with muscular dystrophies: Magnetic resonance imaging phenotype and genotypic considerations. Circ. Cardiovasc. Imaging 2011, 4, 67–76. [Google Scholar] [CrossRef]
- Hor, K.N.; Taylor, M.D.; Al-Khalidi, H.R.; Cripe, L.H.; Raman, S.V.; Jefferies, J.L.; O’Donnell, R.; Benson, D.W.; Mazur, W. Prevalence and distribution of late gadolinium enhancement in a large population of patients with Duchenne muscular dystrophy: Effect of age and left ventricular systolic function. J. Cardiovasc. Magn. Reson. 2013, 15, 107. [Google Scholar] [CrossRef]
- Tandon, A.; Villa, C.R.; Hor, K.N.; Jefferies, J.L.; Gao, Z.; Towbin, J.A.; Wong, B.L.; Mazur, W.; Fleck, R.J.; Sticka, J.J.; et al. Myocardial fibrosis burden predicts left ventricular ejection fraction and is associated with age and steroid treatment duration in duchenne muscular dystrophy. J. Am. Heart Assoc. 2015, 4, e001338. [Google Scholar] [CrossRef]
- Bilchick, K.C.; Salerno, M.; Plitt, D.; Dori, Y.; Crawford, T.O.; Drachman, D.; Thompson, W.R. Prevalence and distribution of regional scar in dysfunctional myocardial segments in Duchenne muscular dystrophy. J. Cardiovasc. Magn. Reson. 2011, 13, 20. [Google Scholar] [CrossRef]
- Flowers, N.C.; Horan, L.G.; Thomas, J.R.; Tolleson, W.J. The anatomic basis for high-frequency components in the electrocardiogram. Circulation 1969, 39, 531–539. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.D.; Buerkel, D.M.; Corbett, J.R.; Gurm, H.S. Fragmented QRS complex has poor sensitivity in detecting myocardial scar. Ann. Noninvasive Electrocardiol. Off. J. Int. Soc. Holter Noninvasive Electrocardiol. 2010, 15, 308–314. [Google Scholar] [CrossRef]
- Carey, M.G.; Luisi, A.J., Jr.; Baldwa, S.; Al-Zaiti, S.; Veneziano, M.J.; deKemp, R.A.; Canty, J.M., Jr.; Fallavollita, J.A. The Selvester QRS Score is more accurate than Q waves and fragmented QRS complexes using the Mason-Likar configuration in estimating infarct volume in patients with ischemic cardiomyopathy. J. Electrocardiol. 2010, 43, 318–325. [Google Scholar] [CrossRef] [PubMed]
- Canpolat, U.; Kabakçi, G.; Aytemir, K.; Dural, M.; Sahiner, L.; Yorgun, H.; Sunman, H.; Bariş Kaya, E.; Tokgözoğlu, L.; Oto, A. Fragmented QRS complex predicts the arrhythmic events in patients with arrhythmogenic right ventricular cardiomyopathy/dysplasia. J. Cardiovasc. Electrophysiol. 2013, 24, 1260–1266. [Google Scholar] [CrossRef]
- Bae, M.H.; Jang, S.Y.; Choi, W.S.; Kim, K.H.; Park, S.H.; Lee, J.H.; Kim, H.K.; Yang, D.H.; Huh, S.; Park, H.S.; et al. A new revised cardiac risk index incorporating fragmented QRS complex as a prognostic marker in patients undergoing noncardiac vascular surgery. Am. J. Cardiol. 2013, 112, 122–127. [Google Scholar] [CrossRef]
- Timonen, P.; Magga, J.; Risteli, J.; Punnonen, K.; Vanninen, E.; Turpeinen, A.; Tuomainen, P.; Kuusisto, J.; Vuolteenaho, O.; Peuhkurinen, K. Cytokines, interstitial collagen and ventricular remodelling in dilated cardiomyopathy. Int. J. Cardiol. 2008, 124, 293–300. [Google Scholar] [CrossRef]
- Kawano, H.; Tsuneto, A.; Koide, Y.; Tasaki, H.; Sueyoshi, E.; Sakamoto, I.; Hayashi, T. Magnetic resonance imaging in a patient with peripartum cardiomyopathy. Intern. Med. 2008, 47, 97–102. [Google Scholar] [CrossRef]
- Marijianowski, M.M.; Teeling, P.; Mann, J.; Becker, A.E. Dilated cardiomyopathy is associated with an increase in the type I/type III collagen ratio: A quantitative assessment. J. Am. Coll. Cardiol. 1995, 25, 1263–1272. [Google Scholar] [CrossRef]
- Gunja-Smith, Z.; Morales, A.R.; Romanelli, R.; Woessner, J.F., Jr. Remodeling of human myocardial collagen in idiopathic dilated cardiomyopathy. Role of metalloproteinases and pyridinoline cross-links. Am. J. Pathol. 1996, 148, 1639–1648. [Google Scholar] [PubMed]
- Daming, W. Derived electrocardiograms on the posterior leads from 12-lead system: Method and evaluation. In Proceedings of the 25th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (IEEE Cat. No. 03CH37439), Cancun, Mexico, 17–21 September 2003; Volume 71, pp. 74–77. [Google Scholar]
- Takeshima, Y.; Yagi, M.; Okizuka, Y.; Awano, H.; Zhang, Z.; Yamauchi, Y.; Nishio, H.; Matsuo, M. Mutation spectrum of the dystrophin gene in 442 Duchenne/Becker muscular dystrophy cases from one Japanese referral center. J. Hum. Genet. 2010, 55, 379–388. [Google Scholar] [CrossRef]
- Cho, H.J.; Kim, N.; Kim, H.J.; Park, B.E.; Kim, H.N.; Jang, S.Y.; Bae, M.H.; Lee, J.H.; Yang, D.H.; Park, H.S.; et al. Effectiveness of a new cardiac risk scoring model reclassified by QRS fragmentation as a predictor of postoperative cardiac event in patients with severe renal dysfunction. BMC Cardiovasc. Disord. 2021, 21, 359. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef]
- Kampmann, C.; Wiethoff, C.M.; Wenzel, A.; Stolz, G.; Betancor, M.; Wippermann, C.-F.; Huth, R.-G.; Habermehl, P.; Knuf, M.; Emschermann, T.; et al. Normal values of M mode echocardiographic measurements of more than 2000 healthy infants and children in central Europe. Heart 2000, 83, 667–672. [Google Scholar] [CrossRef] [PubMed]
- Cho, M.J.; Lee, J.W.; Lee, J.; Shin, Y.B.; Lee, H.D. Relationship Between Fragmented QRS Complexes and Cardiac Status in Duchenne Muscular Dystrophy: Multimodal Validation Using Echocardiography, Magnetic Resonance Imaging, and Holter Monitoring. Pediatr. Cardiol. 2017, 38, 1042–1048. [Google Scholar] [CrossRef] [PubMed]
- Silva, R.; Monteze, N.M.; Giannetti, J.G.; Meira, Z.M.A. Electrocardiographic and Autonomic Nervous System Changes after Changes in the Posture of Children and Adolescents with Duchenne Muscular Dystrophy. Arq. Bras. Cardiol. 2024, 121, e20230483. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, C.; Pieters, Z.H.; Lao, K.; Tonnis, R.; Jacobs, H.; Gunsaulus, M.; Buddhavarapu, A.; Hayes, E.; Wood, P.; Lee, M.; et al. QRS Fragmentation in duchenne muscular dystrophy correlates with delayed enhancement and cardiac dysfunction on CMR. J. Cardiovasc. Magn. Reson. 2025, 27, 101370. [Google Scholar] [CrossRef]
- Ho, S.Y. Anatomy and myoarchitecture of the left ventricular wall in normal and in disease. Eur. J. Echocardiogr. J. Work. Group Echocardiogr. Eur. Soc. Cardiol. 2009, 10, iii3–iii7. [Google Scholar] [CrossRef]
- Marcus, F.I.; Fontaine, G.H.; Guiraudon, G.; Frank, R.; Laurenceau, J.L.; Malergue, C.; Grosgogeat, Y. Right ventricular dysplasia: A report of 24 adult cases. Circulation 1982, 65, 384–398. [Google Scholar] [CrossRef]
- Gemayel, C.; Pelliccia, A.; Thompson, P.D. Arrhythmogenic right ventricular cardiomyopathy. J. Am. Coll. Cardiol. 2001, 38, 1773–1781. [Google Scholar] [CrossRef] [PubMed]
- Nasir, K.; Bomma, C.; Tandri, H.; Roguin, A.; Dalal, D.; Prakasa, K.; Tichnell, C.; James, C.; Spevak, P.J.; Marcus, F.; et al. Electrocardiographic features of arrhythmogenic right ventricular dysplasia/cardiomyopathy according to disease severity: A need to broaden diagnostic criteria. Circulation 2004, 110, 1527–1534. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Tanaka, H.; Matsumoto, K.; Lee, T.; Awano, H.; Yagi, M.; Imanishi, T.; Hayashi, N.; Takeshima, Y.; Kawai, H.; et al. Utility of transmural myocardial strain profile for prediction of early left ventricular dysfunction in patients with Duchenne muscular dystrophy. Am. J. Cardiol. 2013, 111, 902–907. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Tanaka, H.; Takeshima, Y.; Hayashi, N.; Hirata, K.; Kawano, S. Combining passive leg-lifting with transmural myocardial strain profile for enhanced predictive capability for subclinical left ventricular dysfunction in Duchenne muscular dystrophy. J. Cardiol. 2015, 66, 212–217. [Google Scholar] [CrossRef]
- Ogata, H.; Nakatani, S.; Ishikawa, Y.; Negishi, A.; Kobayashi, M.; Ishikawa, Y.; Minami, R. Myocardial strain changes in Duchenne muscular dystrophy without overt cardiomyopathy. Int. J. Cardiol. 2007, 115, 190–195. [Google Scholar] [CrossRef]
- Mori, K.; Hayabuchi, Y.; Inoue, M.; Suzuki, M.; Sakata, M.; Nakagawa, R.; Kagami, S.; Tatara, K.; Hirayama, Y.; Abe, Y. Myocardial strain imaging for early detection of cardiac involvement in patients with Duchenne’s progressive muscular dystrophy. Echocardiography 2007, 24, 598–608. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| With fQRS | Without fQRS | p Value | ||
|---|---|---|---|---|
| Number of patients | 167 | 17 | ||
| Age (years) | 14.3 ± 4.6 | 10.6 ± 4.1 | 0.003 | |
| Creatine kinase (IU/L) | 3791.5 ± 3974.2 | 8486.6 ± 13,346 | 0.21 | |
| Brain natriuretic peptide (pg/mL) | 21.5 ± 40.6 | 11.6 ± 11.3 | 0.036 | |
| Echocardiographic parameters | ||||
| Left ventricular end-diastolic dimension (mm) | 42.8 ± 8.9 | 38.3 ± 3.7 | <0.001 | |
| Left ventricular end-systolic dimension (mm) | 32.2 ± 10.8 | 25.9 ± 4.8 | <0.001 | |
| Left ventricular ejection fraction (%) | 51.8 ± 12.3 | 60.4 ± 8.4 | 0.001 | |
| Electrocardiographic parameters | ||||
| Heart rate (BPM) | 85.7 ± 14.4 | 91.9 ± 14 | 0.11 | |
| QRS duration (msec) | 92.8 ± 12.7 | 86.3 ± 11.9 | 0.052 | |
| QRS axial (degree) | 74.4 ± 39.7 | 75.8 ± 17.2 | 0.80 | |
| Mutation type | ||||
| Deletion | 106 | 1 | ||
| Nonsense mutation | 36 | 2 | ||
| Duplication | 17 | 1 | ||
| Small insertion/deletion | 16 | 0 | ||
| Splice site mutation | 4 | 0 | ||
| Deep intron mutation | 1 | 0 | 0.30 | |
| Position | Variable | Odds Ratio | 95% Confidence Interval | p Value |
|---|---|---|---|---|
| Anterior | Age | 1.14 | 1.06–1.23 | <0.001 |
| Dysfunction | 0.816 | 0.329–2.02 | 0.66 | |
| Lateral | Age | 1.06 | 0.961–1.17 | 0.24 |
| Dysfunction | 2.71 | 1.37–5.39 | 0.004 | |
| Posterior | Dysfunction | 1.85 | 0.979–3.51 | 0.058 |
| Variable | Odds Ratio | 95% Confidence Interval | p Value |
|---|---|---|---|
| Lateral | 2.00 | 1.35–2.95 | <0.001 |
| Posterior | 1.15 | 0.725–1.82 | 0.55 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamamoto, T.; Ogawa, S.; Ide, Y.; Miyazaki, K.; Sunami, A.; Nambu, Y.; Bo, R.; Matsuo, M.; Awano, H. Fragmented QRS in Lateral Leads on Electrocardiography Is Associated with Cardiac Dysfunction and Left Ventricular Dilation in Duchenne Muscular Dystrophy. Biomedicines 2025, 13, 804. https://doi.org/10.3390/biomedicines13040804
Yamamoto T, Ogawa S, Ide Y, Miyazaki K, Sunami A, Nambu Y, Bo R, Matsuo M, Awano H. Fragmented QRS in Lateral Leads on Electrocardiography Is Associated with Cardiac Dysfunction and Left Ventricular Dilation in Duchenne Muscular Dystrophy. Biomedicines. 2025; 13(4):804. https://doi.org/10.3390/biomedicines13040804
Chicago/Turabian StyleYamamoto, Tetsushi, Shuichiro Ogawa, Yusuke Ide, Kokoro Miyazaki, Aiko Sunami, Yoshinori Nambu, Ryosuke Bo, Masafumi Matsuo, and Hiroyuki Awano. 2025. "Fragmented QRS in Lateral Leads on Electrocardiography Is Associated with Cardiac Dysfunction and Left Ventricular Dilation in Duchenne Muscular Dystrophy" Biomedicines 13, no. 4: 804. https://doi.org/10.3390/biomedicines13040804
APA StyleYamamoto, T., Ogawa, S., Ide, Y., Miyazaki, K., Sunami, A., Nambu, Y., Bo, R., Matsuo, M., & Awano, H. (2025). Fragmented QRS in Lateral Leads on Electrocardiography Is Associated with Cardiac Dysfunction and Left Ventricular Dilation in Duchenne Muscular Dystrophy. Biomedicines, 13(4), 804. https://doi.org/10.3390/biomedicines13040804