
Lower Plasma IL-32 Levels Linked to Better Survival in Sepsis

 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Cohort
2.2. IL-32 ELISA
2.3. Statistical Analysis
3. Results
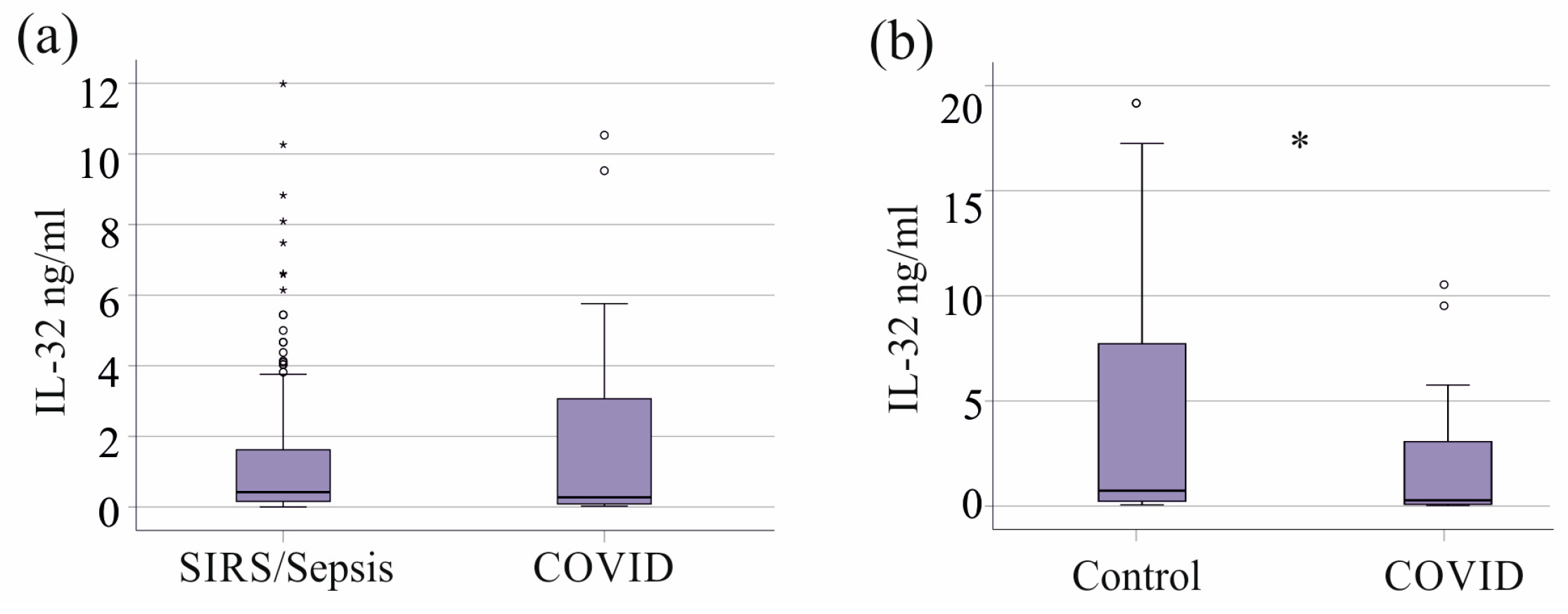
3.1. IL-32 in Plasma of Controls and SIRS/Sepsis Patients with and Without Liver Cirrhosis
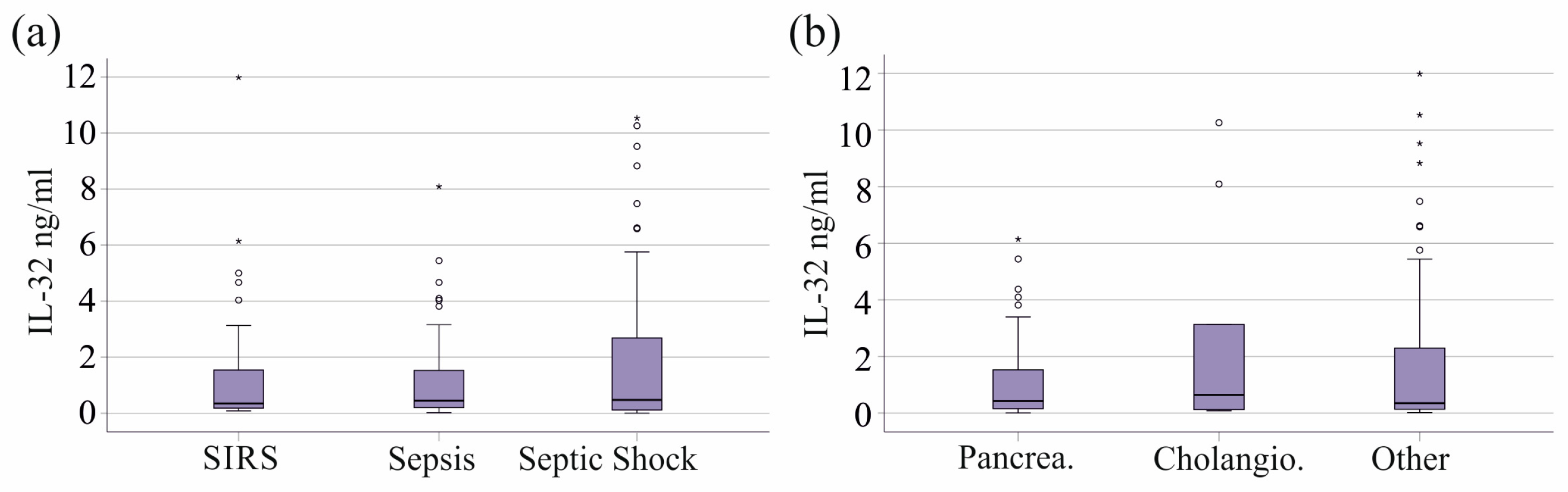
3.2. Plasma IL-32 of SIRS/Sepsis Patients Stratified for SIRS, Sepsis, and Septic Shock and Underlying Diseases
3.3. Plasma IL-32 Levels of SIRS/Sepsis Patients Stratified for Infectious Diseases, SARS-CoV-2, and Bacterial Infections
3.4. Plasma IL-32 Levels in Relation to Vasopressor Therapy and Interventions
3.5. Plasma IL-32 Levels in Relation to Biomarkers of Inflammation and Liver Function
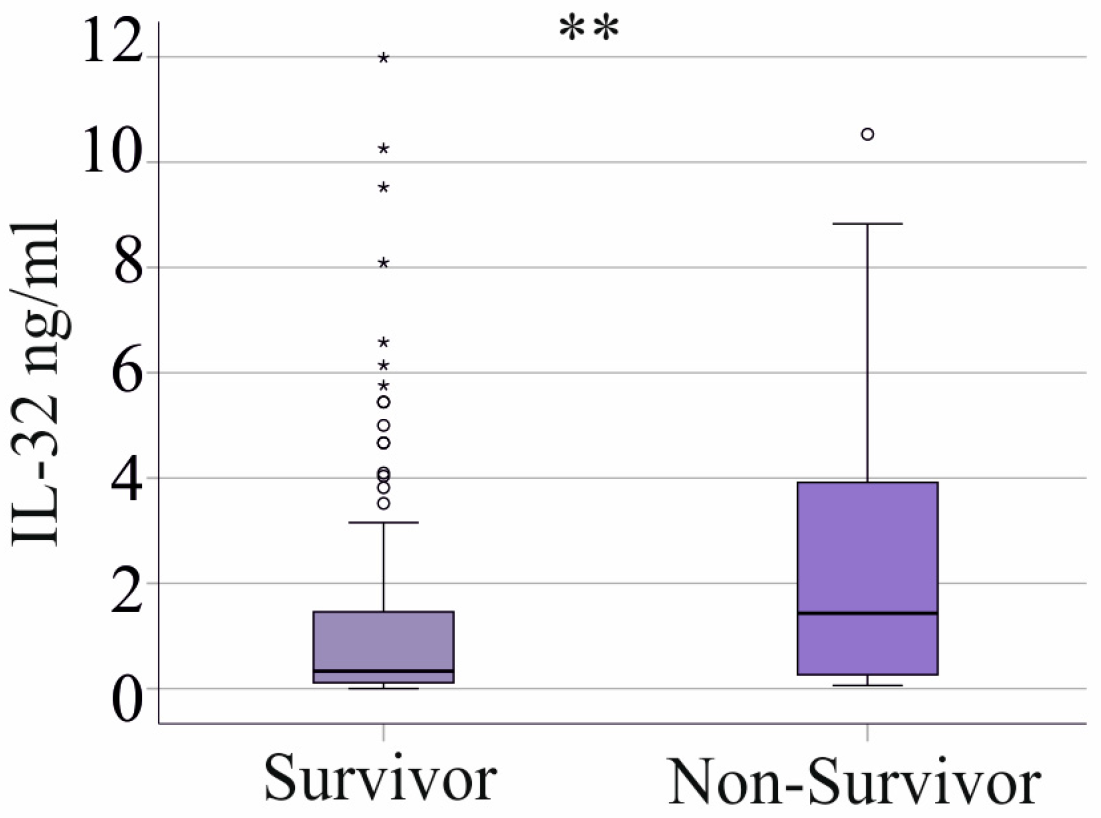
3.6. Plasma IL-32 Levels and Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ALT | Alanine aminotransferase |
| AST | Aspartate aminotransferase |
| ARDS | Acute respiratory distress syndrome |
| CRP | C-reactive protein |
| GGT | Gamma-glutamyl transferase |
| HIV | Human immunodeficiency virus |
| IL | Interleukin |
| NK | Natural killer |
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
References
- Gyawali, B.; Ramakrishna, K.; Dhamoon, A.S. Sepsis: The evolution in definition, pathophysiology, and management. SAGE Open Med. 2019, 7, 2050312119835043. [Google Scholar] [CrossRef] [PubMed]
- Jarczak, D.; Kluge, S.; Nierhaus, A. Sepsis-Pathophysiology and Therapeutic Concepts. Front. Med. 2021, 8, 628302. [Google Scholar] [CrossRef] [PubMed]
- Barichello, T.; Generoso, J.S.; Singer, M.; Dal-Pizzol, F. Biomarkers for sepsis: More than just fever and leukocytosis-a narrative review. Crit. Care 2022, 26, 14. [Google Scholar] [CrossRef] [PubMed]
- Nedeva, C.; Menassa, J.; Puthalakath, H. Sepsis: Inflammation Is a Necessary Evil. Front. Cell Dev. Biol. 2019, 7, 108. [Google Scholar] [CrossRef]
- Hong, J.T.; Son, D.J.; Lee, C.K.; Yoon, D.Y.; Lee, D.H.; Park, M.H. Interleukin 32, inflammation and cancer. Pharmacol. Ther. 2017, 174, 127–137. [Google Scholar] [CrossRef]
- Jensen, I.J.; Sjaastad, F.V.; Griffith, T.S.; Badovinac, V.P. Sepsis-Induced T Cell Immunoparalysis: The Ins and Outs of Impaired T Cell Immunity. J. Immunol. 2018, 200, 1543–1553. [Google Scholar] [CrossRef]
- Wang, F.; Cui, Y.; He, D.; Gong, L.; Liang, H. Natural killer cells in sepsis: Friends or foes? Front. Immunol. 2023, 14, 1101918. [Google Scholar] [CrossRef]
- Giamarellos-Bourboulis, E.J.; Tsaganos, T.; Spyridaki, E.; Mouktaroudi, M.; Plachouras, D.; Vaki, I.; Karagianni, V.; Antonopoulou, A.; Veloni, V.; Giamarellou, H. Early changes of CD4-positive lymphocytes and NK cells in patients with severe Gram-negative sepsis. Crit. Care 2006, 10, R166. [Google Scholar] [CrossRef]
- Boomer, J.S.; Shuherk-Shaffer, J.; Hotchkiss, R.S.; Green, J.M. A prospective analysis of lymphocyte phenotype and function over the course of acute sepsis. Crit. Care 2012, 16, R112. [Google Scholar] [CrossRef]
- Qu, P.; Wuest, T.; Min, Y.; Alevizos, I.; Young, H.A.; Lin, P.C. Natural Killer Cell Transcript 4 promotes the development of Sjögren’s syndrome via activation of Rap1 on B cells. J. Autoimmun. 2021, 116, 102559. [Google Scholar] [CrossRef]
- Rong, B.; Fu, T.; Rong, C.; Liu, W.; Li, K.; Liu, H. Correlation between serum IL-32 concentration and clinical parameters of stable COPD: A retrospective clinical analysis. Sci. Rep. 2020, 10, 12092. [Google Scholar] [CrossRef] [PubMed]
- Moschen, A.R.; Fritz, T.; Clouston, A.D.; Rebhan, I.; Bauhofer, O.; Barrie, H.D.; Powell, E.E.; Kim, S.H.; Dinarello, C.A.; Bartenschlager, R.; et al. Interleukin-32: A new proinflammatory cytokine involved in hepatitis C virus-related liver inflammation and fibrosis. Hepatology 2011, 53, 1819–1829. [Google Scholar] [CrossRef] [PubMed]
- Xu, Q.; Pan, X.; Shu, X.; Cao, H.; Li, X.; Zhang, K.; Lu, J.; Zou, Y.; Li, X.; Liu, H.; et al. Increased interleukin-32 expression in chronic hepatitis B virus-infected liver. J. Infect. 2012, 65, 336–342. [Google Scholar] [CrossRef] [PubMed]
- Schilcher, K.; Dayoub, R.; Kubitza, M.; Riepl, J.; Klein, K.; Buechler, C.; Melter, M.; Weiss, T.S. Saturated Fat-Mediated Upregulation of IL-32 and CCL20 in Hepatocytes Contributes to Higher Expression of These Fibrosis-Driving Molecules in MASLD. Int. J. Mol. Sci. 2023, 24, 13222. [Google Scholar] [CrossRef]
- Bai, X.; Ovrutsky, A.R.; Kartalija, M.; Chmura, K.; Kamali, A.; Honda, J.R.; Oberley-Deegan, R.E.; Dinarello, C.A.; Crapo, J.D.; Chang, L.Y.; et al. IL-32 expression in the airway epithelial cells of patients with Mycobacterium avium complex lung disease. Int. Immunol. 2011, 23, 679–691. [Google Scholar] [CrossRef]
- Ribeiro-Dias, F.; Saar Gomes, R.; de Lima Silva, L.L.; Dos Santos, J.C.; Joosten, L.A. Interleukin 32: A novel player in the control of infectious diseases. J. Leukoc. Biol. 2017, 101, 39–52. [Google Scholar] [CrossRef]
- Zhou, Y.; Zhu, Y. Important Role of the IL-32 Inflammatory Network in the Host Response against Viral Infection. Viruses 2015, 7, 3116–3129. [Google Scholar] [CrossRef]
- Bergantini, L.; d’Alessandro, M.; Cameli, P.; Otranto, A.; Luzzi, S.; Bianchi, F.; Bargagli, E. Cytokine profiles in the detection of severe lung involvement in hospitalized patients with COVID-19: The IL-8/IL-32 axis. Cytokine 2022, 151, 155804. [Google Scholar] [CrossRef]
- Bergantini, L.; d’Alessandro, M.; Gangi, S.; Bianchi, F.; Cameli, P.; Perea, B.; Meocci, M.; Fabbri, G.; Marrucci, S.; Ederbali, M.; et al. Predictive Role of Cytokine and Adipokine Panel in Hospitalized COVID-19 Patients: Evaluation of Disease Severity, Survival and Lung Sequelae. Int. J. Mol. Sci. 2023, 24, 12994. [Google Scholar] [CrossRef]
- Kaufmann, C.C.; Ahmed, A.; Muthspiel, M.; Rostocki, I.; Pogran, E.; Zweiker, D.; Burger, A.L.; Jager, B.; Aicher, G.; Spiel, A.O.; et al. Association of Interleukin-32 and Interleukin-34 with Cardiovascular Disease and Short-Term Mortality in COVID-19. J. Clin. Med. 2023, 12, 975. [Google Scholar] [CrossRef]
- Zamani, B.; Najafizadeh, M.; Motedayyen, H.; Arefnezhad, R. Predicting roles of IL-27 and IL-32 in determining the severity and outcome of COVID-19. Int. J. Immunopathol. Pharmacol. 2022, 36, 3946320221145827. [Google Scholar] [CrossRef] [PubMed]
- Grewal, T.; Buechler, C. Adipokines as Diagnostic and Prognostic Markers for the Severity of COVID-19. Biomedicines 2023, 11, 1302. [Google Scholar] [CrossRef] [PubMed]
- Coomes, E.A.; Haghbayan, H. Interleukin-6 in Covid-19: A systematic review and meta-analysis. Rev. Med. Virol. 2020, 30, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Elahi, R.; Hozhabri, S.; Moradi, A.; Siahmansouri, A.; Jahani Maleki, A.; Esmaeilzadeh, A. Targeting the cGAS-STING pathway as an inflammatory crossroad in coronavirus disease 2019 (COVID-19). Immunopharmacol. Immunotoxicol. 2023, 45, 639–649. [Google Scholar] [CrossRef]
- Georgieva, E.; Ananiev, J.; Yovchev, Y.; Arabadzhiev, G.; Abrashev, H.; Abrasheva, D.; Atanasov, V.; Kostandieva, R.; Mitev, M.; Petkova-Parlapanska, K.; et al. COVID-19 Complications: Oxidative Stress, Inflammation, and Mitochondrial and Endothelial Dysfunction. Int. J. Mol. Sci. 2023, 24, 14876. [Google Scholar] [CrossRef]
- Mazzoni, A.; Salvati, L.; Maggi, L.; Annunziato, F.; Cosmi, L. Hallmarks of immune response in COVID-19: Exploring dysregulation and exhaustion. Semin. Immunol. 2021, 55, 101508. [Google Scholar] [CrossRef]
- Tang, J.; Luo, J.; Huang, Z.; Xu, J.; Liao, J.; Zhan, H.; Xiong, Y.; Luo, H.; Jiang, Y.; Zeng, Q. Admission IL-32 concentration predicts severity and mortality of severe community-acquired pneumonia independently of etiology. Clin. Chim. Acta 2020, 510, 647–653. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Bone, R.C. Sepsis, sepsis syndrome, and the systemic inflammatory response syndrome (SIRS). Gulliver in Laputa. JAMA 1995, 273, 155–156. [Google Scholar] [CrossRef]
- Brun-Buisson, C. The epidemiology of the systemic inflammatory response. Intensive Care Med. 2000, 26 (Suppl. S1), S64–S74. [Google Scholar] [CrossRef]
- Shappell, C.N.; Klompas, M.; Kanjilal, S.; Chan, C.; Rhee, C. Prevalence, Clinical Characteristics, and Outcomes of Sepsis Caused by Severe Acute Respiratory Syndrome Coronavirus 2 Versus Other Pathogens in Hospitalized Patients with COVID-19. Crit. Care Explor. 2022, 4, e0703. [Google Scholar] [CrossRef] [PubMed]
- Sieurin, J.; Branden, G.; Magnusson, C.; Hergens, M.P.; Kosidou, K. A population-based cohort study of sex and risk of severe outcomes in COVID-19. Eur. J. Epidemiol. 2022, 37, 1159–1169. [Google Scholar] [CrossRef]
- Hammed, M.M. Review of interleukin-32 and liver disease. Int. J. Health Sci. 2022, 6, 14–20. [Google Scholar] [CrossRef]
- Li, Y.; Xie, J.; Xu, X.; Liu, L.; Wan, Y.; Liu, Y.; Zhu, C.; Zhu, Y. Inducible interleukin 32 (IL-32) exerts extensive antiviral function via selective stimulation of interferon lambda1 (IFN-lambda1). J. Biol. Chem. 2013, 288, 20927–20941. [Google Scholar] [CrossRef]
- Sasidharan, K.; Caddeo, A.; Jamialahmadi, O.; Noto, F.R.; Tomasi, M.; Malvestiti, F.; Ciociola, E.; Tavaglione, F.; Mancina, R.M.; Cherubini, A.; et al. IL32 downregulation lowers triglycerides and type I collagen in di-lineage human primary liver organoids. Cell Rep. Med. 2024, 5, 101352. [Google Scholar] [CrossRef]
- Nesseler, N.; Launey, Y.; Aninat, C.; Morel, F.; Malledant, Y.; Seguin, P. Clinical review: The liver in sepsis. Crit. Care 2012, 16, 235. [Google Scholar] [CrossRef]
- Woznica, E.A.; Inglot, M.; Woznica, R.K.; Lysenko, L. Liver dysfunction in sepsis. Adv. Clin. Exp. Med. 2018, 27, 547–551. [Google Scholar] [CrossRef]
- Foreman, M.G.; Mannino, D.M.; Moss, M. Cirrhosis as a risk factor for sepsis and death: Analysis of the National Hospital Discharge Survey. Chest 2003, 124, 1016–1020. [Google Scholar] [CrossRef]
- Li, W.; Yang, F.; Liu, Y.; Gong, R.; Liu, L.; Feng, Y.; Hu, P.; Sun, W.; Hao, Q.; Kang, L.; et al. Negative feedback regulation of IL-32 production by iNOS activation in response to dsRNA or influenza virus infection. Eur. J. Immunol. 2009, 39, 1019–1024. [Google Scholar] [CrossRef]
- Rasool, S.T.; Tang, H.; Wu, J.; Li, W.; Mukhtar, M.M.; Zhang, J.; Mu, Y.; Xing, H.X.; Wu, J.; Zhu, Y. Increased level of IL-32 during human immunodeficiency virus infection suppresses HIV replication. Immunol. Lett. 2008, 117, 161–167. [Google Scholar] [CrossRef]
- Dahl, C.A.; Schall, R.P.; He, H.L.; Cairns, J.S. Identification of a novel gene expressed in activated natural killer cells and T cells. J. Immunol. 1992, 148, 597–603. [Google Scholar] [CrossRef] [PubMed]
- Finfer, S.; Venkatesh, B.; Hotchkiss, R.S.; Sasson, S.C. Lymphopenia in sepsis-an acquired immunodeficiency? Immunol. Cell Biol. 2023, 101, 535–544. [Google Scholar] [CrossRef] [PubMed]
- Catalan, V.; Gomez-Ambrosi, J.; Rodriguez, A.; Ramirez, B.; Valenti, V.; Moncada, R.; Landecho, M.F.; Silva, C.; Salvador, J.; Fruhbeck, G. Increased Interleukin-32 Levels in Obesity Promote Adipose Tissue Inflammation and Extracellular Matrix Remodeling: Effect of Weight Loss. Diabetes 2016, 65, 3636–3648. [Google Scholar] [CrossRef] [PubMed]
- Martinez Perez, L.A.; Becerra-Ruiz, J.S.; Garcia-Avina, J.E.; Gonzalez-Sanchez, G.D.; Martinez-Esquivias, F.; Vazquez-Jimenez, S.I.; Ramirez-De Los Santos, S.; Lopez-Pulido, E.I.; Guzman-Flores, J.M. Relation of serum IL-32 levels and gene polymorphism rs45499297 with obesity in Mexican patients: A laboratory and in silico analysis. Nutr. Hosp. 2022, 39, 313–319. [Google Scholar] [CrossRef]
- Sloot, Y.J.E.; Smit, J.W.; Joosten, L.A.B.; Netea-Maier, R.T. Insights into the role of IL-32 in cancer. Semin. Immunol. 2018, 38, 24–32. [Google Scholar] [CrossRef]
- Shim, S.; Lee, S.; Hisham, Y.; Kim, S.; Nguyen, T.T.; Taitt, A.S.; Hwang, J.; Jhun, H.; Park, H.Y.; Lee, Y.; et al. Comparison of the Seven Interleukin-32 Isoforms’ Biological Activities: IL-32theta Possesses the Most Dominant Biological Activity. Front. Immunol. 2022, 13, 837588. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | SIRS/Sepsis | Controls |
|---|---|---|
| Males/Females | 110/42 | 19/21 ** |
| Age, years | 60 (21–93) | 54 (21–63) *** |
| Body mass index, kg/m2 | 26.7 (15.4–55.6) 148 | not defined |
| SIRS/Sepsis/Septic shock | 39/37/76 | not defined |
| C-reactive protein, mg/L | 178 (4–697) | not defined |
| Procalcitonin, ng/mL | 1.48 (0.05–270.00) 148 | not defined |
| Leukocytes, n/nL | 10.40 (0.06–246.94) | not defined |
| Neutrophils, n/nL | 7.94 (0–70.20) 146 | not defined |
| Basophils, n/nL | 0.04 (0–0.90) 147 | not defined |
| Eosinophils, n/nL | 0.09 (0–8.80) 147 | not defined |
| Monocytes, n/nL | 0.76 (0–45.00) 147 | not defined |
| Lymphocytes, n/nL | 0.96 (0.08–28.60) 147 | not defined |
| Immature granulocytes, n/nL | 0.15 (0–7.25) 147 | not defined |
| Total bilirubin, mg/dL | 0.80 (0.10–23.90) 144 | not defined |
| Albumin, g/L | 24.1 (6.0–42.0) 141 | not defined |
| Aspartate aminotransferase, U/L | 43 (6–3252) 139 | not defined |
| Alanine aminotransferase, U/L | 32 (5–889) 139 | not defined |
| Gamma-glutamyl transferase, U/L | 137 (11–1266) 125 | not defined |
| Intervention/Drug | ||
|---|---|---|
| Number | p-Value | |
| Dialysis | 51 | 0.532 |
| Ventilation | 91 | 0.348 |
| Vasopressor therapy | 96 | 0.733 |
| Biomarker of Inflammation | SIRS/Sepsis Without Liver Cirrhosis |
|---|---|
| Procalcitonin | 0.095 |
| C-reactive protein | −0.045 |
| IL-6 | 0.140 |
| Leukocytes | 0.098 |
| Neutrophils | 0.075 |
| Basophils | 0.038 |
| Eosinophils | −0.011 |
| Monocytes | 0.011 |
| Lymphocytes | −0.049 |
| Immature granulocytes | 0.138 |
| Biomarker of Liver Disease | SIRS/Sepsis Without Liver Cirrhosis |
| Total bilirubin, mg/dL | 0.324 *** |
| Albumin, g/L | 0.025 |
| Aspartate aminotransferase, U/L | 0.265 ** |
| Alanine aminotransferase, U/L | 0.189 * |
| Gamma-glutamyl transferase, U/L | 0.245 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mester, P.; Utrata, A.; Schmidtner, N.; Birner, C.; Schmid, S.; Müller, M.; Pavel, V.; Buechler, C. Lower Plasma IL-32 Levels Linked to Better Survival in Sepsis. Biomedicines 2025, 13, 750. https://doi.org/10.3390/biomedicines13030750
Mester P, Utrata A, Schmidtner N, Birner C, Schmid S, Müller M, Pavel V, Buechler C. Lower Plasma IL-32 Levels Linked to Better Survival in Sepsis. Biomedicines. 2025; 13(3):750. https://doi.org/10.3390/biomedicines13030750
Chicago/Turabian StyleMester, Patricia, Alexander Utrata, Niklas Schmidtner, Charlotte Birner, Stephan Schmid, Martina Müller, Vlad Pavel, and Christa Buechler. 2025. "Lower Plasma IL-32 Levels Linked to Better Survival in Sepsis" Biomedicines 13, no. 3: 750. https://doi.org/10.3390/biomedicines13030750
APA StyleMester, P., Utrata, A., Schmidtner, N., Birner, C., Schmid, S., Müller, M., Pavel, V., & Buechler, C. (2025). Lower Plasma IL-32 Levels Linked to Better Survival in Sepsis. Biomedicines, 13(3), 750. https://doi.org/10.3390/biomedicines13030750