
Relationship Between Radiological Features of Primary Empty or Primary Partial Empty Sella and Pituitary Hormone Levels
 , , , ,
, , , ,
Abstract
1. Introduction
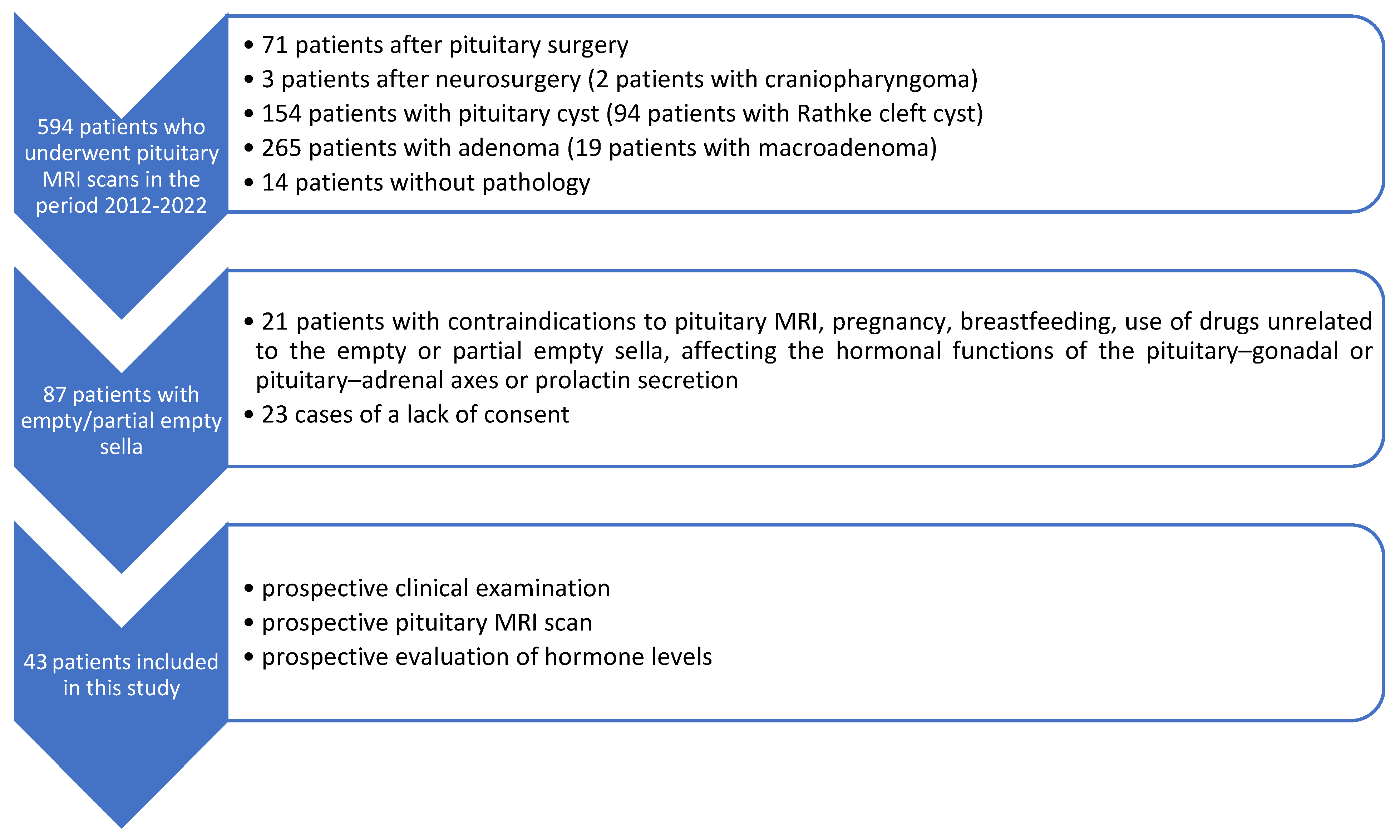
2. Material and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Iskra, T.; Stachera, B.; Możdżeń, K.; Murawska, A.; Ostrowski, P.; Bonczar, M.; Gregorczyk-Maga, I.; Walocha, J.; Koziej, M.; Wysiadecki, G.; et al. Morphology of the Sella Turcica: A Meta-Analysis Based on the Results of 18,364 Patients. Brain Sci. 2023, 13, 1208. [Google Scholar] [CrossRef] [PubMed]
- Jankowski, T.; Jedliński, M.; Grocholewicz, K.; Janiszewska-Olszowska, J. Sella Turcica Morphology on Cephalometric Radiographs and Dental Abnormalities-Is There Any Association?—Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 4456. [Google Scholar] [CrossRef] [PubMed]
- Bonczar, M.; Wysiadecki, G.; Ostrowski, P.; Michalczak, M.; Plutecki, D.; Wilk, J.; Michalik, W.; Walocha, J.; Balawender, K.; Iskra, T.; et al. The Morphology of the Pituitary Gland: A Meta-Analysis with Implications for Diagnostic Imaging. Brain Sci. 2023, 13, 89. [Google Scholar] [CrossRef]
- Rice-Canetto, T.E.; Carroll, P.; Reier, L.; Siddiqi, J. Asymptomatic Empty Sella: A Literature Review and Suggestions for Evaluation in Clinical Practice. Cureus 2024, 16, e75965. [Google Scholar] [CrossRef]
- Önal, V.; Evren, A.; Chatzioglou, G.O.N.; Tellioğlu, A.M. Anatomical features of sella turcica with comprehensive literature review. Rev. Assoc. Med. Bras. (1992) 2023, 69, e20230402. [Google Scholar] [CrossRef] [PubMed]
- Chiloiro, S.; Giampietro, A.; Bianchi, A.; Tartaglione, T.; Capobianco, A.; Anile, C.; De Marinis, L. Diagnosis of endocrine disease: Primary empty sella: A comprehensive review. Eur. J. Endocrinol. 2017, 177, 275–285. [Google Scholar] [CrossRef]
- Auer, M.K.; Stieg, M.R.; Crispin, A.; Sievers, C.; Stalla, G.K.; Kopczak, A. Primary Empty Sella Syndrome and the Prevalence of Hormonal Dysregulation. Dtsch. Arztebl. Int. 2018, 115, 99–105. [Google Scholar] [CrossRef]
- Guitelman, M.; Garcia Basavilbaso, N.; Vitale, M.; Chervin, A.; Katz, D.; Miragaya, K.; Herrera, J.; Cornalo, D.; Servidio, M.; Boero, L.; et al. Primary empty sella (PES): A review of 175 cases. Pituitary 2013, 16, 270–274. [Google Scholar] [CrossRef]
- Zuhur, S.S.; Kuzu, I.; Ozturk, F.Y.; Uysal, E.; Altuntas, Y. Anterior pituitary hormone deficiency in subjects with total and partial primary empty sella: Do all cases need endocrinological evaluation? Turk. Neurosurg. 2014, 24, 374–379. [Google Scholar] [CrossRef]
- Padovano Sorrentino, F.; Chiloiro, S.; Giampietro, A.; Bianchi, A.; Pontecorvi, A.; De Marinis, L. Empty sella syndrome: An update. Pituitary 2024, 28, 13. [Google Scholar] [CrossRef]
- Foresti, M.; Guidali, A.; Susanna, P. Primary empty sella. Incidence in 500 asymptomatic subjects examined with magnetic resonance. Radiol. Med. 1991, 81, 803–807. [Google Scholar] [PubMed]
- Gallardo, E.; Schächter, D.; Cáceres, E.; Becker, P.; Colin, E.; Martínez, C.; Henríquez, C. The empty sella: Results of treatment in 76 successive cases and high frequency of endocrine and neurological disturbances. Clin. Endocrinol. 1992, 37, 529–533. [Google Scholar] [CrossRef]
- Lupi, I.; Manetti, L.; Raffaelli, V.; Grasso, L.; Sardella, C.; Cosottini, M.; Iannelli, A.; Gasperi, M.; Bogazzi, F.; Caturegli, P.; et al. Pituitary autoimmunity is associated with hypopituitarism in patients with primary empty sella. J. Endocrinol. Investig. 2011, 34, 240–244. [Google Scholar]
- Cannavò, S.; Curtò, L.; Venturino, M.; Squadrito, S.; Almoto, B.; Narbone, M.C.; Rao, R.; Trimarchi, F. Abnormalities of hypothalamic-pituitary-thyroid axis in patients with primary empty sella. J. Endocrinol. Investig. 2002, 25, 236–239. [Google Scholar] [CrossRef] [PubMed]
- Colao, A.; Cotta, O.R.; Ferone, D.; Torre, M.L.; Ferraù, F.; Di Somma, C.; Boschetti, M.; Teti, C.; Maria CSavanelli Alibrandi, A.; Trimarchi, F.; et al. Role of pituitary dysfunction on cardiovascular risk in primary empty sella patients. Clin. Endocrinol. 2013, 79, 211–216. [Google Scholar] [CrossRef]
- Chiloiro, S.; Giampietro, A.; Bianchi, A.; De Marinis, L. Empty sella syndrome: Multiple endocrine disorders. Handb. Clin. Neurol. 2021, 181, 29–40. [Google Scholar]
- Prabhat, N.; Kaur, K.; Takkar, A.; Ahuja, C.; Katoch, D.; Goyal, M.; Dutta, P.; Bhansali, A.; Lal, V. Pituitary Dysfunction in Idiopathic Intracranial Hypertension: An Analysis of 80 Patients. Can. J. Neurol. Sci. 2024, 51, 265–271. [Google Scholar] [CrossRef]
- Fleseriu, M.; Hashim, I.A.; Karavitaki, N.; Melmed, S.; Murad, H.M.; Salvatori, R.; Samuels, M.H. Hormonal Replacement in Hypopituitarism in Adults: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2016, 101, 3888–3921. [Google Scholar] [CrossRef] [PubMed]
- Xu, P.; He, H.; Chen, Y.; Wang, C.; Zhu, Y.; Ye, X. Osteoporotic fractures and persistent non-fusion of the hand epiphyses caused by empty sella syndrome in an adult: A case report. J. Int. Med. Res. 2013, 41, 1768–1772. [Google Scholar] [CrossRef]
- Carosi, G.; Brunetti, A.; Mangone, A.; Baldelli, R.; Tresoldi, A.; Del Sindaco, G.; Lavezzi, E.; Sala, E.; Mungari, R.; Fatti, L.M.; et al. A multicenter Cohort Study in Patients with Primary Empty Sella: Hormonal and Neuroradiological Features Over a Long Follow-Up. Front. Endocrinol. 2022, 13, 925378. [Google Scholar] [CrossRef]
- Yuh, W.T.; Zhu, M.; Taoka, T.; Quets, J.P.; Maley, J.E.; Muhonen, M.G.; Schuster, M.E.; Kardon, R.H. MR imaging of pituitary morphology in idiopathic intracranial hypertension. J. Magn. Reson. Imaging JMRI 2000, 12, 808–813. [Google Scholar] [CrossRef] [PubMed]
- Barkatullah, A.F.; Leishangthem, L.; Moss, H.E. MRI findings as markers of idiopathic intracranial hypertension. Curr. Opin. Neurol. 2021, 34, 75–83. [Google Scholar] [CrossRef]
- Weber, K.T.; Singh, K.D.; Hey, J.C. Idiopathic intracranial hypertension with primary aldosteronism: Report of 2 cases. Am. J. Med. Sci. 2002, 324, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.U.; Khalid, H.; Salpietro, V.; Weber, K.T. Idiopathic intracranial hypertension associated with either primary or secondary aldosteronism. Am. J. Med. Sci. 2013, 346, 194–198. [Google Scholar] [CrossRef]
- Thaller, M.; Homer, V.; Sassani, M.; Mollan, S.P.; Sinclair, A.J. Longitudinal prospective cohort study evaluating prognosis in idiopathic intracranial hypertension patients with and without comorbid polycystic ovarian syndrome. Eye 2023, 37, 3621–3628. [Google Scholar] [CrossRef] [PubMed]
- Rzewuska, N.; Kunicki, J.; Pieniak, K.; Laskus, P.; Zabielska, B.; Smolarczyk, R.; Kunicki, M. A systematic review on idiopathic intracranial hypertension comorbid with polycystic ovarian syndrome and its consequences. Eur. J. Obstet. Gynecol. Reprod. Biol. 2024, 292, 1–7. [Google Scholar] [CrossRef]
- Thaller M, Mytton J, Wakerley BR, Mollan SP, Sinclair AJ. Idiopathic intracranial hypertension: Evaluation of births and fertility through the Hospital Episode Statistics dataset. BJOG 2022, 129, 2019–2027. [CrossRef] [PubMed] [PubMed Central]
- Leca, B.M.; Mytilinaiou, M.; Tsoli, M.; Epure, A.; Aylwin, S.J.B.; Kaltsas, G.; Randeva, H.S.; Dimitriadis, G.K. Identification of an optimal prolactin threshold to determine prolactinma size using receiver perating characteristic analysis. Sci. Rep. 2021, 11, 9801. [Google Scholar] [CrossRef]
- Alyami, N.; Alhenaki, G.; Al Atwah, S.; Alhenaki, N.; Smaisem, F.; Alotaibi, A.; Abu Risheh j Smaisem, M.; Alhenaki, A.; Alanazi, S.; Alshammeri, M.; et al. Correlation between MRI findings of pituitary gland and prolactin level among hyperprolactinemia adult female Saudi patients in rural areas: A retrospective multicentric study. Medicine 2025, 104, e40686. [Google Scholar] [CrossRef]
- Chen, H.C.; Sung, C.C. A young man with secondary adrenal insufficiency due to empty sella syndrome. BMC Nephrol. 2022, 23, 81. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Del Monte, P.; Foppiani, L.; Cafferata, C.; Marugo, A.; Bernasconi, D. Primary “empty sella” in adults: Endocrine findings. Endocr. J. 2006, 53, 803–809. [Google Scholar] [CrossRef] [PubMed]
- Terano, T.; Seya, A.; Tamura, Y.; Yoshida, S.; Hirayama, T. Characteristic of the pituitary gland in elderly subjects from magnetic resonance images: Relationship to pituitary hormone secretion. Clin. Endocrinol. 1996, 45, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Akkus, G.; Sözütok, S.; Odabaş, F.; Onan, B.; Evran, M.; Karagun, B.; Sert, M.; Tetiker, T. Pituitary Volume in Patients with Primary Empty Sella and Clinical Relevance to Pituitary Hormone Secretion: A Retrospective Single Center Study. Curr. Med. Imaging 2021, 17, 1018–1024. [Google Scholar] [CrossRef]
- Kaess, M.; Simmons, J.G.; Whittle, S.; Jovev, M.; Chanen, A.M.; Yücel, M.; Pantelis Ch Allen, N.B. Sex-specific prediction of hypothalamic-pituitary-adrenal axis activity by pituitary volume during adolescence: A longitudinal study from 12 to 17 years of age. Psychoneuroendocrinolog 2013, 38, 2694–2704. [Google Scholar] [CrossRef]
- Ertekin, T.; Acer, N.; Turgut, A.T.; Aycan, K.; Ozçelik, O.; Turgut, M. Comparison of three methods for the estimation of the pituitary gland volume using magnetic resonance imaging: A stereological study. Pituitary 2011, 14, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Tsunoda, A.; Okuda, O.; Sato, K. MR Height of the Pituitary Gland as a Function of Age and Sex: Especially Physiological Hypertrophy in Adolescence and in Climacterium. AJNR Am. J. Neuroradiol. 1997, 18, 551–554. [Google Scholar] [PubMed]
- Destrieux, C.; Kakou, M.K.; Velut, S.; Lefrancq, T.; Jan, M. Microanatomy of the hypophyseal fossa boundaries. J. Neurosurg. 1998, 88, 743–752. [Google Scholar] [CrossRef]
- Peker, S.; Kurtkaya-Yapicier, O.; Kiliç, T.; Pamir, M.N. Microsurgical anatomy of the lateral walls of the pituitary fossa. Acta Neurochir. 2005, 147, 641–648. [Google Scholar] [CrossRef]
- Yasuda, A.; Campero, A.; Martins, C.; Rhoton, A.L.; Ribas, G.C. The medial wall of the cavernous sinus: Microsurgical anatomy. Neurosurgery 2004, 55, 179–189. [Google Scholar] [CrossRef]
- Dos Santos Silva, J.; Schreiner, C.A.; de Lima, L.; Brigido, C.E.P.L.; Wilson, C.D.; McVeigh, L.; Acchiardo, J.; Landeiro, J.A.; Acioly, M.A.; Cohen-Gadol, A. Volumetric measurement of intracranial meningiomas: A comparison between linear, planimetric, and machine learning with multiparametric voxel-based morphometry methods. J. Neurooncol. 2023, 161, 235–243. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Patients Without Hormonal Disorders n = 37 | Patients with Hormonal Disorders n = 6 | p-Value |
|---|---|---|---|
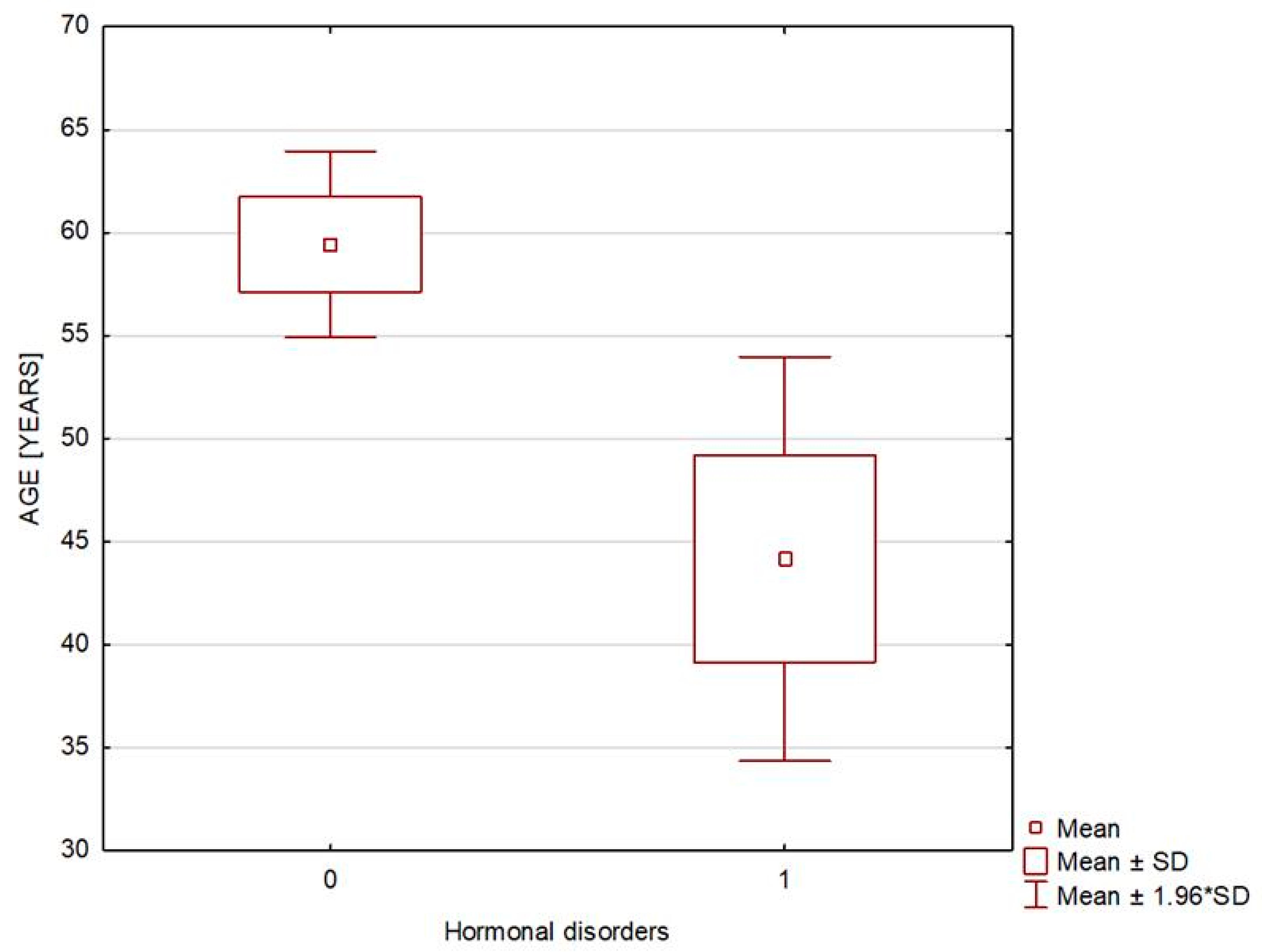
| Age [years] | 59.432 ± 14.041 | 44.167 ± 12.254 | 0.021 |
| Sex [M] | 9 (2.324%) | 0 (0%) | 0.187 |
| Body weight [kg] | 79.697 ± 13.462 | 67.583 ± 10.414 | 0.034 |
| BMI [kg/m2] | 28.096 ± 4.567 | 25.45 ± 3.169 | 0.045 |
| Overweight and obesity | 27 (72.973%) | 3 (50%) | 0.271 |
| Waist circumference [cm] | 95.125 ± 11.284 | 79.833 ± 15.943 | 0.022 |
| Arterial hypertension | 16 (43.243%) | 1 (16.667%) | 0.16 |
| Variable | Patients Without Hormonal Disorders n = 37 | Patients with Hormonal Disorders n = 6 | p-Value | ||
|---|---|---|---|---|---|
| Median (Min–Max) | Mean ± SD | Median (Min–Max) | Mean ± SD | ||
| Specific gravity of urine [g/mL] | 1.016 (1.007–1.04) | 1.017 ± 0.007 | 1.013 (1.006–1.028) | 1.016 ± 0.009 | 0.663 |
| Serum sodium [mmol/L] | 142 (128–145) | 141 ± 3.04 | 137.50 (136–141) | 138 ± 1.79 | 0.005 |
| Serum potassium [mmol/L] | 4.55 (3.78–5.39) | 4.54 ± 0.39 | 4.13 (3.69–4.49) | 4.12 ± 0.29 | 0.016 |
| Serum osmolality [mOsm/kg] | 291 (278–313) | 290.87 ± 6.79 | 287 (282–293) | 287.33 ± 3.67 | 0.171 |
| Urine osmolality [mOsm/kg] | 539.50 (251–956) | 571.75 ± 203.21 | 440.5 (258–957) | 558.33 ± 304.79 | 0.787 |
| TSH [µIU/mL] | 1.95 (0.27–4.08) | 1.959 ± 0.97 | 2.02 (0.95–2.82) | 1.90 ± 0.74 | 0.899 |
| fT3 [pg/mL] | 3.06 (2.16–3.82) | 3.10 ± 0.39 | 2.75 (2.34–3.58) | 2.83 ± 0.43 | 0.109 |
| fT4 [ng/dL] | 1.26 (1.02–1.70) | 1.27 ± 0.162 | 1.10 (0.90–1.33) | 1.11 ± 0.168 | 0.081 |
| Prolactin [ng/mL] | 11.00 (4.9–20.8) | 11.86 ± 5.21 | 15.15 (3.20–52.60) | 22.08 ± 18.69 | 0.326 |
| Cortisol at 8 a.m. [µg/dL] | 14.30 (6.1–24.5) | 13.68 ± 3.63 | 11.6 (8.90–24.30) | 14.73 ± 6.56 | 0.746 |
| ACTH at 8 a.m. [pg/mL] | 22.5 (7.3–87.2) | 25.82 ± 16.29 | 15.8 (2.30–28.90) | 16.08 ± 9.04 | 0.136 |
| Growth hormone [ng/mL] | 0.44 (0.05–17.10) | 1.32 ± 2.99 | 0.45 (0.17–8.96) | 2.17 ± 3.47 | 0.472 |
| IGF-1 [ng/mL] | 135.50 (61.33–253.50) | 140.84 ± 46.41 | 188.70 (82.65–350.80) | 195.09 ± 94.43 | 0.166 |
| Variable | Mean | SD | Median | Minimum | Maximum |
|---|---|---|---|---|---|
| ACTH [pg/mL] (n = 6) | 16.067 | 9.041 | 15.800 | 2.300 | 28.900 |
| ACTH [pg/mL] in patients with secondary adrenocortical insufficiency on glucocorticoid replacement with Hydrocortisonum (n = 3) | 10.667 | 7.786 | 12.000 | 2.300 | 17.700 |
| Serum cortisol [µg/dL] | 14.733 | 6.563 | 11.600 | 8.900 | 24.300 |
| Serum cortisol [µg/dL] in patients with secondary adrenocortical insufficiency on glucocorticoid replacement with Hydrocortisonum (n = 3) | 18.300 | 8.24 | 21.700 | 8.900 | 24.300 |
| Serum prolactin [ng/mL] (n = 6) | 22.083 | 18.691 | 15.150 | 3.200 | 52.600 |
| Serum prolactin [ng/mL] in patients with hyperprolactinemia (n = 4) | 26.700 | 22.154 | 25.500 | 3.200 | 52.600 |
| Serum prolactin [ng/mL] in patients with hyperprolactinemia receiving dopamine receptor agonists (n = 2) | 8.800 | 7.919 | 8.800 | 3.200 | 14.400 |
| Serum prolactin [ng/mL] in patients with hyperprolactinemia receiving no dopamine receptor agonists (n = 2) | 44.600 | 11.314 | 44.600 | 36.600 | 52.600 |
| TSH [µIU/mL] | 1.904 | 0.741 | 2.020 | 0.952 | 2.820 |
| fT3 [pg/mL] | 2.833 | 0.426 | 2.745 | 2.340 | 3.580 |
| fT4 [ng/dL] | 1.110 | 0.168 | 1.100 | 0.900 | 1.330 |
| Growth hormone [ng/mL] | 2.168 | 3.465 | 0.450 | 0.170 | 8.960 |
| IGF-1 [ng/mL] | 195.092 | 94.434 | 188.700 | 82.650 | 350.800 |
| Variable | Patients Without Hormonal Disorders n = 37 | Patients with Hormonal Disorders n = 6 | p-Value | ||
|---|---|---|---|---|---|
| Median (Min–Max) | Mean ± SD | Median (Min–Max) | Mean ± SD | ||
| Pituitary AP diameter [mm] | 12.00 (7.50–17.10) | 12.40 ± 2.03 | 12.00(10.00–13.30) | 12.00 ± 1.38 | 0.659 |
| Pituitary RL diameter [mm] | 16.00 (5.00–25.00) | 15.95 ± 3.27 | 16.25 (14.40–20.00) | 16.80 ± 2.39 | 0.516 |
| Pituitary CC diameter [mm] | 2.80 (0.80–5.00) | 2.97 ± 1.06 | 2.90 (1.40–4.50) | 3.05 ± 1.093 | 0.752 |
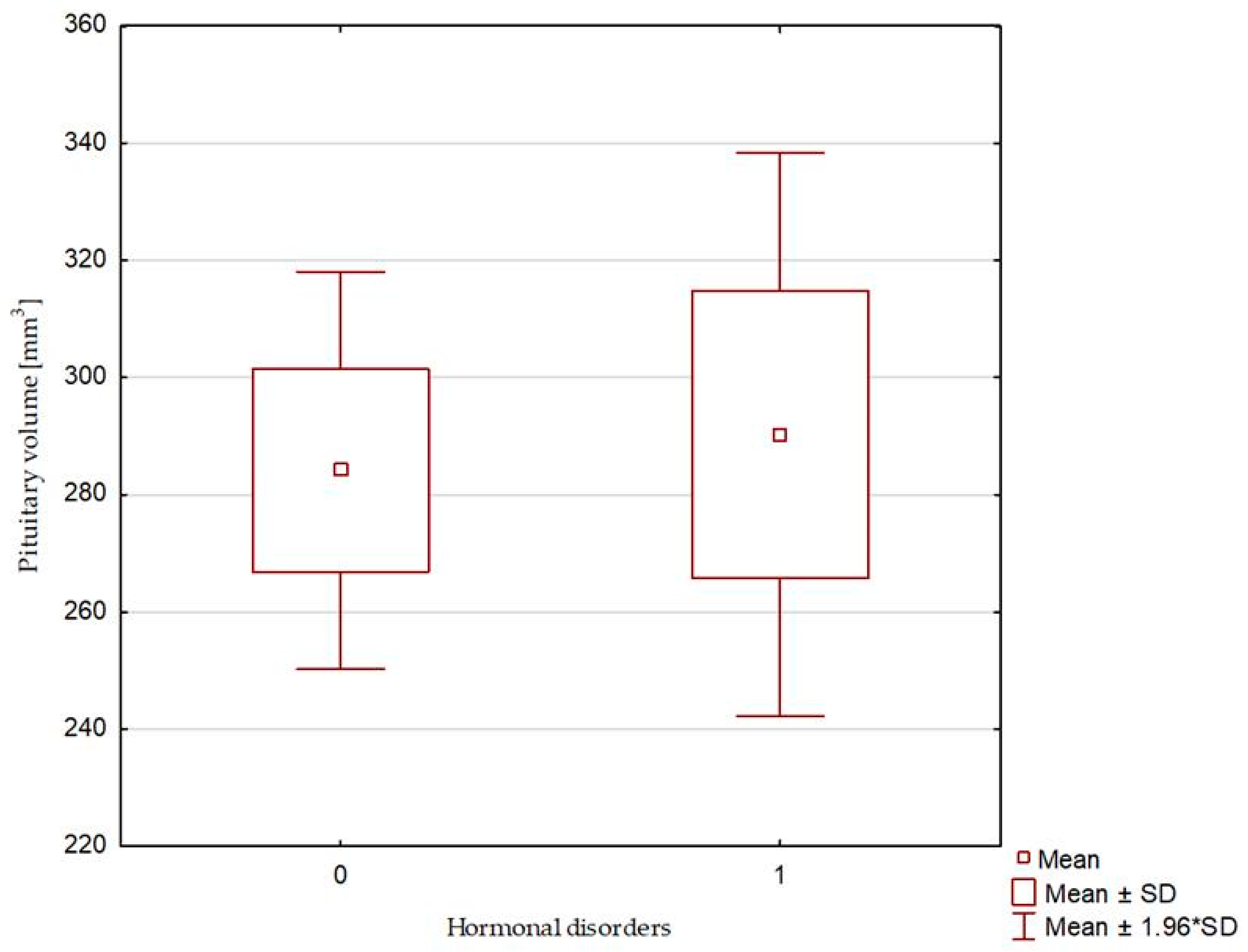
| Pituitary volume [mm3] | 276.12 (62.40–536.30) | 284.14 ± 105.12 | 299.55 (194.194–368.00) | 290.29 ± 60.05 | 0.739 |
| Sella turcica—AP diameter [mm] | 12.00 (7.50–17.10) | 12.51 ± 2.08 | 12.50 (10.00–14.30) | 12.38 ± 1.15 | 0.902 |
| Sella turcica—RL diameter [mm] | 16.00 (5.00–25.00) | 15.95 ± 3.27 | 16.25 (14.40–20.00) | 16.80 ± 2.39 | 0.516 |
| Sella turcica—bony—CC diameter [mm] | 10.40 (7.30–17.40) | 11.25 ± 2.53 | 10.40 (9.50–13.30) | 10.68 ± 1.43 | 0.833 |
| Sella turcica—diaphragma sellae—CC diameter [mm] | 7.40 (5.50–15.70) | 8.20 ± 2.46 | 7.90 (6.50–9.70) | 7.97 ± 1.26 | 0.699 |
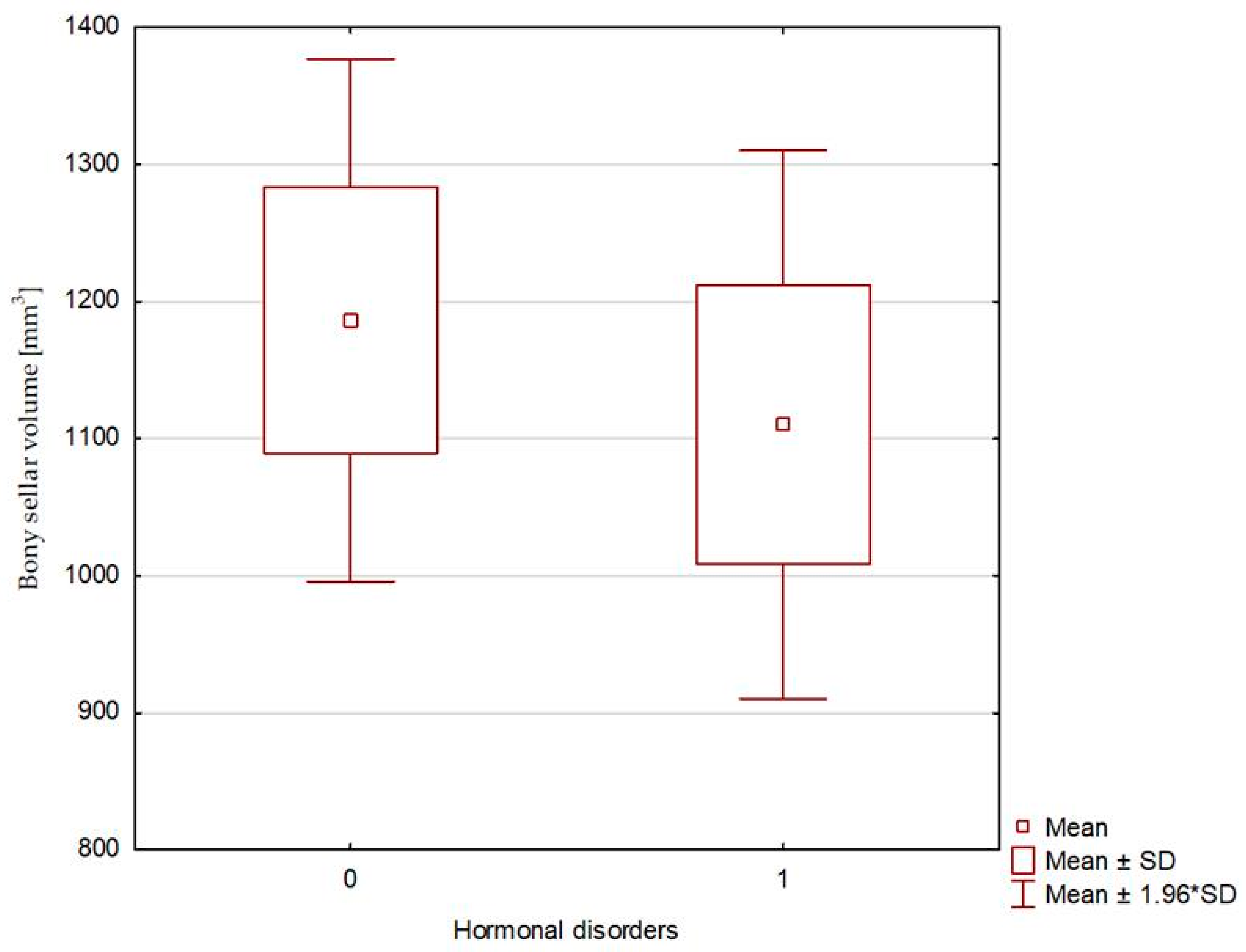
| Bony sellar volume [mm3] | 976.19 (140.63–1683.71) | 1186.41 ± 591.43 | 1099.03 (792.00–1498.07) | 1110.28 ± 249,81 | 0.661 |
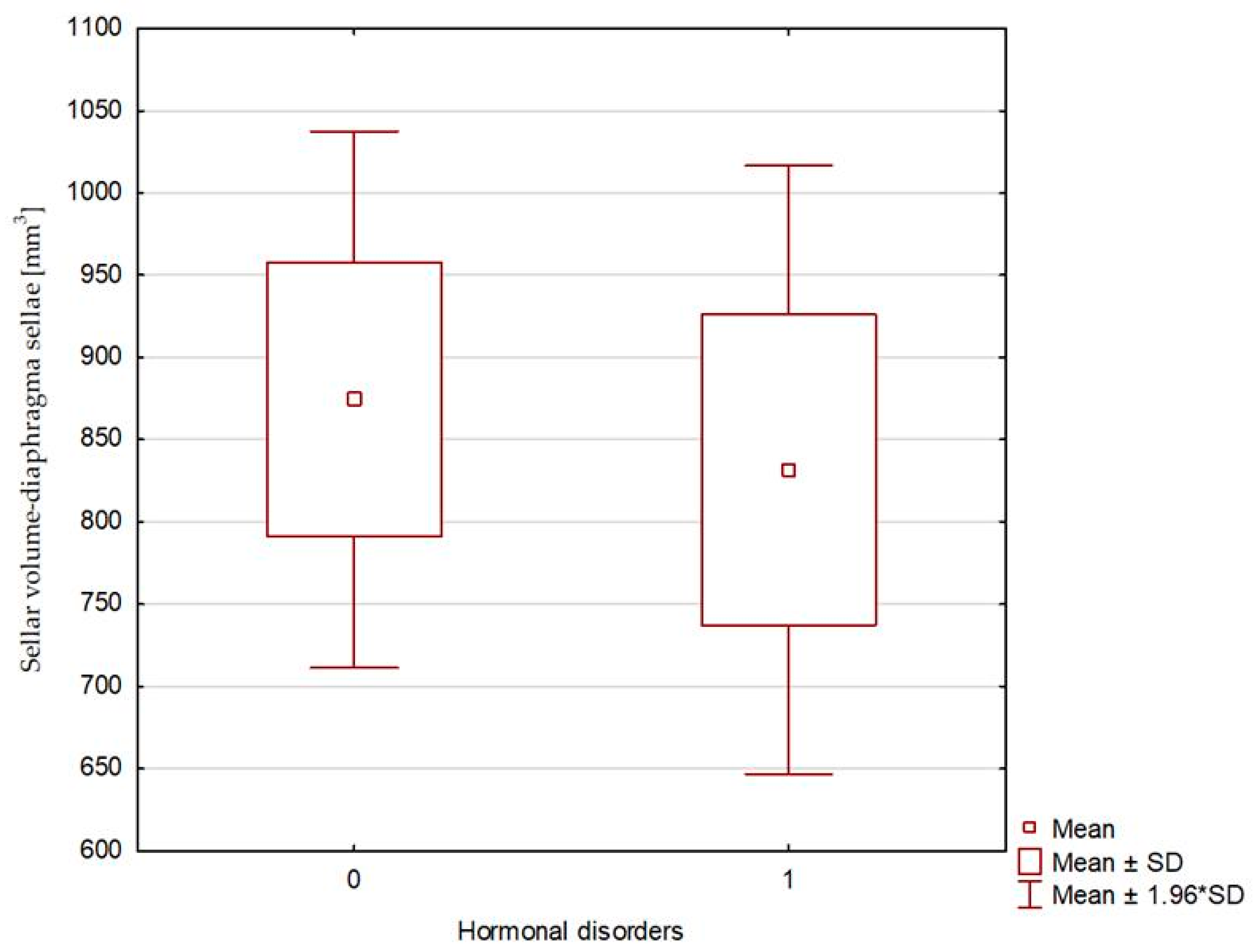
| Sellar volume—diaphragma sellae [mm3] | 665.63 (116.25–2316.99) | 874.48 ± 506.25 | 769.97 (597.60–1248.39) | 831.69 ± 231.16 | 0.451 |
| Pituitary volume expressed as a percentage of sellar volume [%] | 28.79 (6.02–66.67) | 28.15 ± 12.93 | 27.25 (12.96–40.91) | 28.14 ± 10.91 | 0.986 |
| Pituitary height expressed as a percentage of bony sella height [%] | 28.79 (6.02–66.67) | 28.35 ± 12.94 | 28.95 (12.96–40.91) | 28.93 ± 10.74 | 0.875 |
| Pituitary height expressed as a percentage of sella height—diaphragma sellae [%] | 39.79 (9.09–80.65) | 40.08 ± 19.25 | 41.43 (15.56–54.22) | 39.31 ± 14.84 | 0.986 |
| Right optic nerve sheath diameter [mm] | 4.65 (3.80–5.80) | 4.71 ± 0.44 | 4.75 (4.40–5.30) | 4.77 ± 0.33 | 0.793 |
| Left optic nerve sheath diameter [mm] | 4.60 (3.70–6.30) | 4.56 ± 0.51 | 4.5 (3.90–5.30) | 4.57 ± 0.47 | 0.930 |
| VARIABLE | N (%) | N (%) | p-value | ||
| Empty sella—with the pituitary CC diameter less than 2 mm | 8 (21.62%) | 1 (16.67%) | 0.804 | ||
| Empty sella—with the pituitary CC diameter less than 3 mm | 19 (51.35%) | 4 (66.67%) | 0.503 | ||
| Pituitary stalk displacement | 21 (56.76%) | 3 (50.00%) | 0.757 | ||
| Enlarged cerebrospinal fluid spaces | 10 (27.03%) | 1 (16.67%) | 0.589 | ||
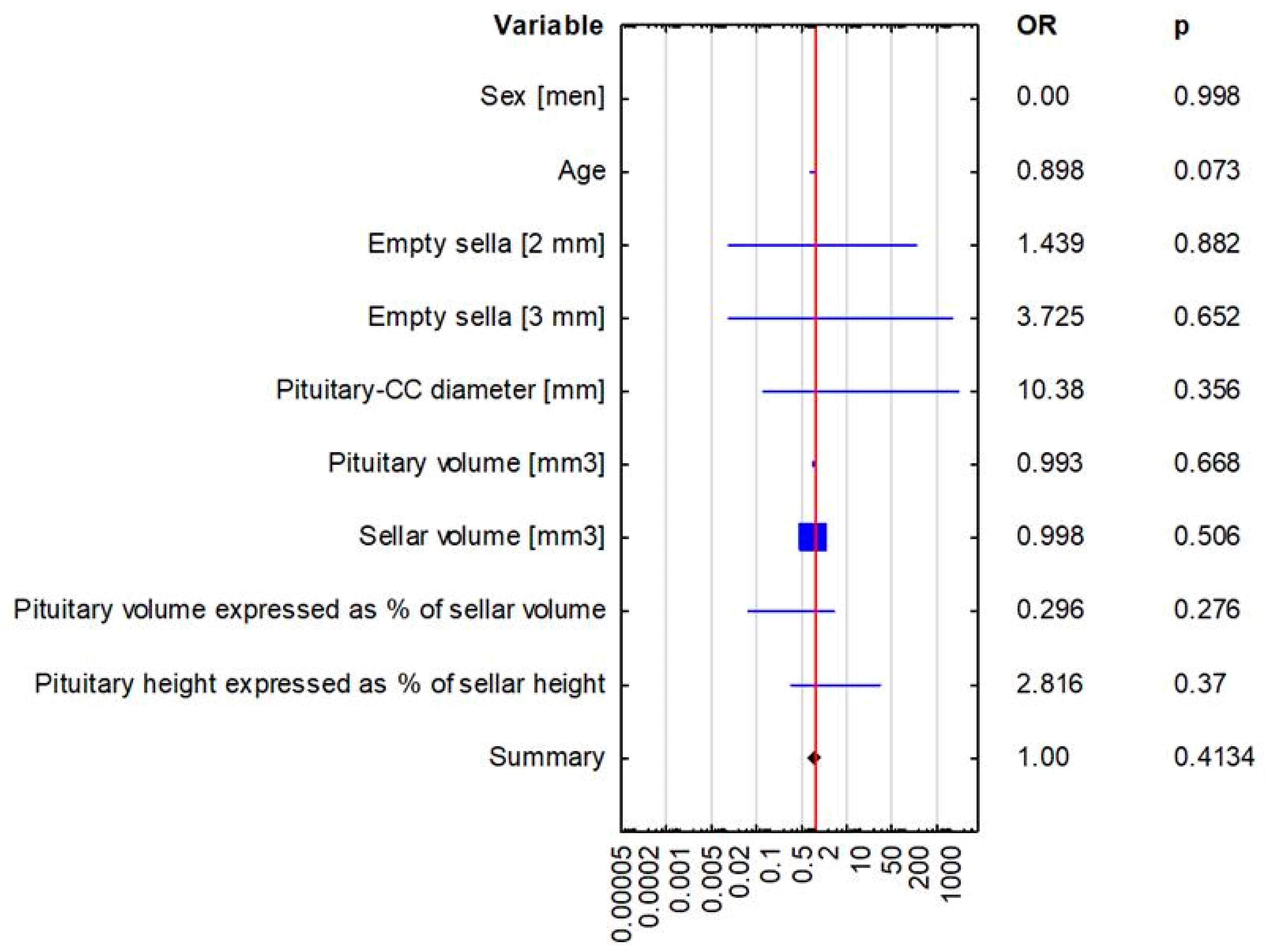
| Variable | Hormonal Disorders OR (95% CI) p-Value | |
|---|---|---|
| Multivariate Logistic Regression | Univariate Logistic Regression | |
| Sex | 0.00 (0.00–0.00), p = 0.998 | 0.00 (0.00–0.00), p = 0.997 |
| Age | 0.898 (0.798–1.01), p = 0.073 | 0.916 (0.844–0.993), p = 0.034 |
| Empty sella [2 mm] | 1.439 (0.008–297.121), p = 0.882 | 0.725 (0.074–7.126), p = 0.783 |
| Empty sella [3 mm] | 3.725 (0.012–1131.502), p = 0.652 | 1.895 (0.308–11.644), p = 0.49 |
| Pituitary—craniocaudal diameter [mm] | 10.380 (0.072–1495.711), p = 0.356 | 1.073 (0.469–2.454), p = 0.8668 |
| Pituitary volume [mm3] | 0.993 (0.964–1.024), p = 0.668 | 1.001 (0.992–1.009), p = 0.887 |
| Sellar volume [mm3] | 0.998 (0.992–1.004), p = 0.506 | 1 (0.998–1.001), p = 0.7531 |
| Pituitary volume expressed as percentage of sellar volume(bony sella) | 0.296 (0.033–2.639), p = 0.276 | 1 (0.933–1.072), p = 0.999 |
| Pituitary height expressed as percentage of sellar height (bony sella) | 2.816 (0.293–27.105), p = 0.37 | 1.004 (0.937–1.076), p = 0.916 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kałuża, B.; Furmanek, M.; Domański, J.; Żuk-Łapan, A.; Babula, E.; Poprawa, I.; Walecki, J.; Franek, E. Relationship Between Radiological Features of Primary Empty or Primary Partial Empty Sella and Pituitary Hormone Levels. Biomedicines 2025, 13, 722. https://doi.org/10.3390/biomedicines13030722
Kałuża B, Furmanek M, Domański J, Żuk-Łapan A, Babula E, Poprawa I, Walecki J, Franek E. Relationship Between Radiological Features of Primary Empty or Primary Partial Empty Sella and Pituitary Hormone Levels. Biomedicines. 2025; 13(3):722. https://doi.org/10.3390/biomedicines13030722
Chicago/Turabian StyleKałuża, Bernadetta, Mariusz Furmanek, Jan Domański, Aleksandra Żuk-Łapan, Emilia Babula, Iga Poprawa, Jerzy Walecki, and Edward Franek. 2025. "Relationship Between Radiological Features of Primary Empty or Primary Partial Empty Sella and Pituitary Hormone Levels" Biomedicines 13, no. 3: 722. https://doi.org/10.3390/biomedicines13030722
APA StyleKałuża, B., Furmanek, M., Domański, J., Żuk-Łapan, A., Babula, E., Poprawa, I., Walecki, J., & Franek, E. (2025). Relationship Between Radiological Features of Primary Empty or Primary Partial Empty Sella and Pituitary Hormone Levels. Biomedicines, 13(3), 722. https://doi.org/10.3390/biomedicines13030722