
Sunitinib’s Effect on Bilateral Optic Nerve Damage in Rats Following the Unilateral Clamping and Unclamping of the Common Carotid Artery
 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. The Rats
2.2. Drugs
2.3. Experimental Animal Groups
2.4. Surgical and Pharmacological Procedures
2.5. Biochemical Analyses
2.5.1. Specimen Preparation
2.5.2. MDA, GSH, TNF-α, IL-1β and IL-6 and Protein Determination
2.6. Histopathological Examination
2.7. Statistical Analysis
3. Results
3.1. Biochemical Results
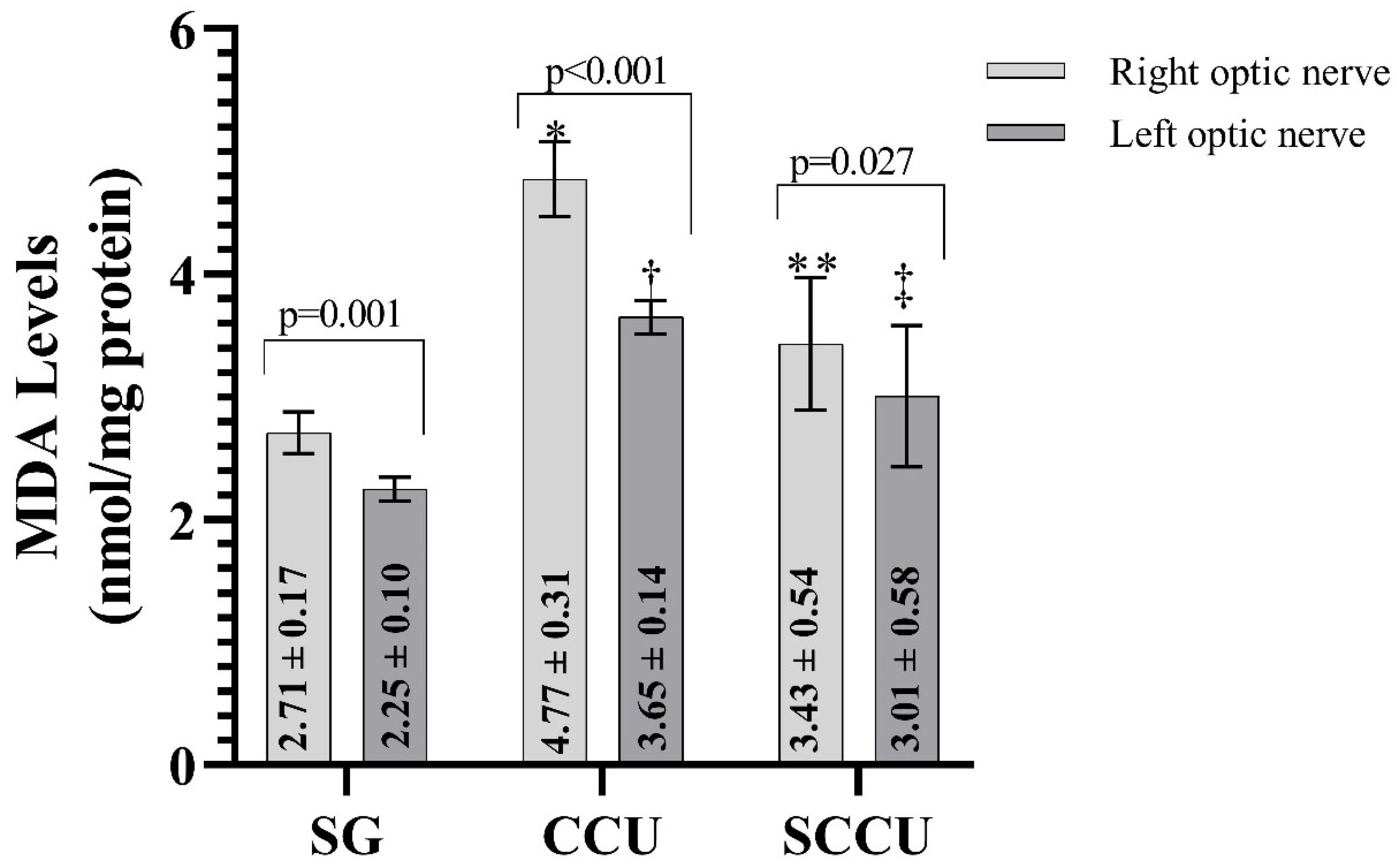
3.1.1. MDA Levels of Optic Nerve Tissues
3.1.2. tGSH Levels of Optic Nerve Tissues
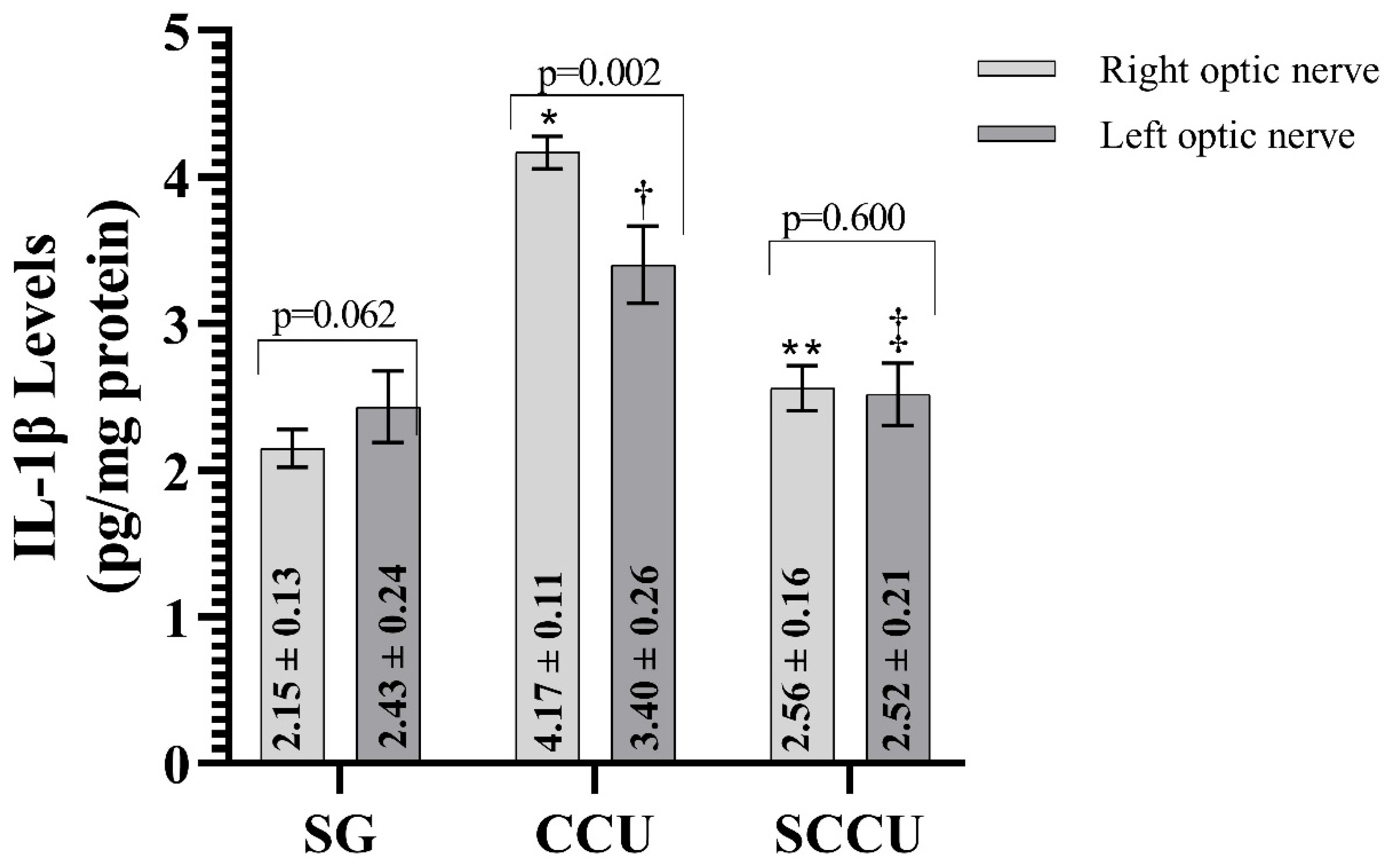
3.1.3. TNF-α, IL-1β, and IL-6 Levels of Optic Nerve Tissues
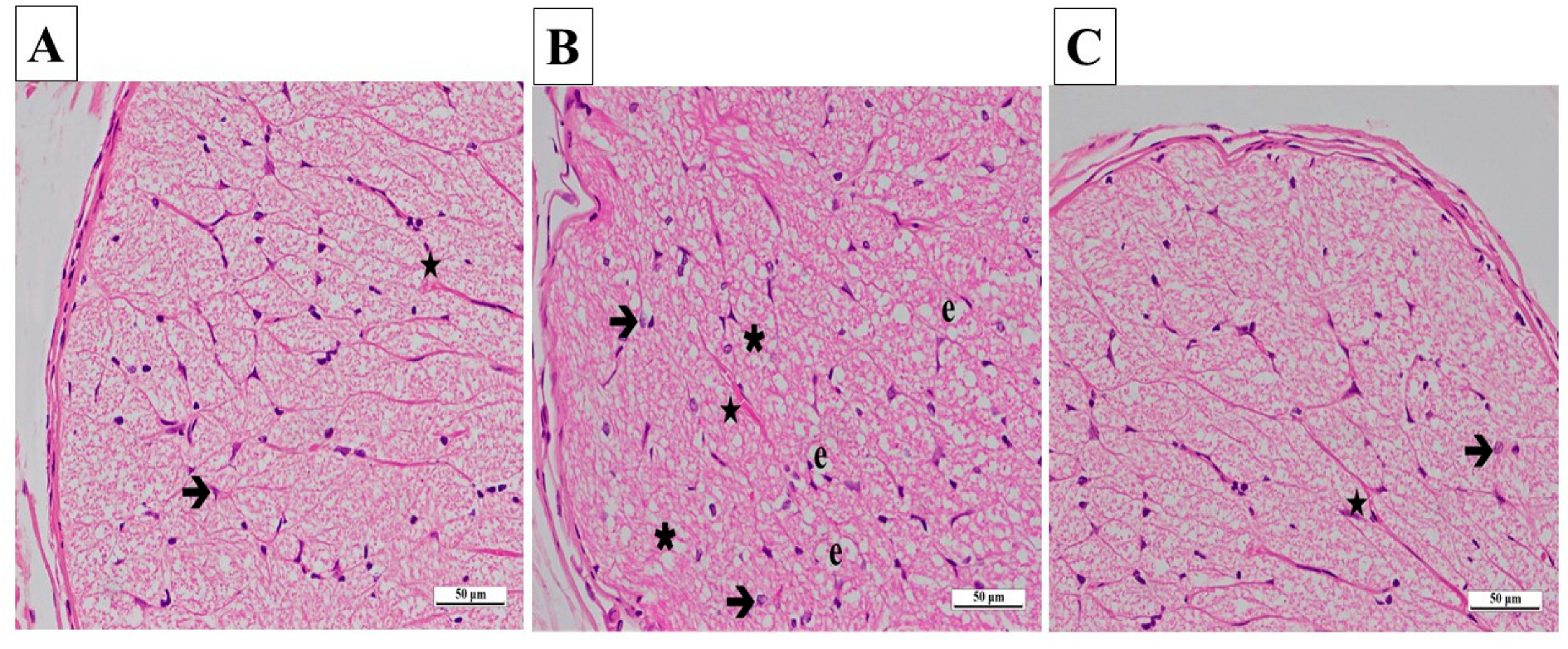
3.2. Histopathologic Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bajkó, Z.; Bălaşa, R.; Moţăţăianu, A.; Maier, S.; Chebuţ, O.C.; Szatmári, S. Common carotid artery occlusion: A case series. Int. Sch. Res. Not. 2013, 2013, 198595. [Google Scholar] [CrossRef] [PubMed]
- Cho, K.H.; Ahn, S.J.; Cho, J.H.; Jung, C.; Han, M.K.; Park, S.J.; Park, K.H.; Woo, S.J. The Characteristics of Retinal Emboli and its Association with Vascular Reperfusion in Retinal Artery Occlusion. Investig. Ophthalmol. Vis. Sci. 2016, 57, 4589–4598. [Google Scholar] [CrossRef]
- Nakajima, H.; Momose, T.; Misawa, T. Prevalence and risk factors of subclinical coronary artery disease in patients undergoing carotid endarterectomy: A retrospective cohort study. Int. Angiol. 2019, 38, 312–319. [Google Scholar] [CrossRef]
- Kniemeyer, H.W.; Aulich, A.; Schlachetzki, F.; Steinmetz, H.V.; Sandmann, W. Pseudo- and segmental occlusion of the internal carotid artery: A new classification, surgical treatment and results. Eur. J. Vasc. Endovasc. Surg. 1996, 12, 310–320. [Google Scholar] [CrossRef]
- Kels, B.D.; Grzybowski, A.; Grant-Kels, J.M. Human ocular anatomy. Clin. Dermatol. 2015, 33, 140–146.6. [Google Scholar] [CrossRef]
- Lee, D.; Tomita, Y.; Yang, L.; Negishi, K.; Kurihara, T. Ocular Ischemic Syndrome and Its Related Experimental Models. Int. J. Mol. Sci. 2022, 23, 5249. [Google Scholar] [CrossRef]
- Coviltir, V.; Burcel, M.G.; Baltă, G.; Marinescu, M.C. Interplay Between Ocular Ischemia and Glaucoma: An Update. Int. J. Mol. Sci. 2024, 25, 12400. [Google Scholar] [CrossRef]
- Kingsbury, C.; Heyck, M.; Bonsack, B.; Lee, J.Y.; Borlongan, C.V. Stroke gets in your eyes: Stroke-induced retinal ischemia and the potential of stem cell therapy. Neural. Regen. Res. 2020, 15, 1014–1018. [Google Scholar]
- Yapca, O.E.; Borekci, B.; Suleyman, H. Ischemia-reperfusion damage. Eurasian J. Med. 2013, 45, 126–127. [Google Scholar] [CrossRef]
- Turan, İ.; Cengil, O.; Büşra, O.; Altuğ, B.; Özaçmak, H.S.; Özaçmak, V.H. Çevresel Zenginleştirme Bilateral Karotid Arter Oklüzyonu ile Oluşan Retinal Oksidatif Stresi Azaltır. Batı Karadeniz Tıp Derg. 2019, 3, 101–108. [Google Scholar] [CrossRef]
- Cicek, I.; Somuncu, A.M.; Altuner, D.; Suleyman, B.; Mammadov, R.; Bulut, S.; Coban, T.A.; Bal Tastan, T.; Suleyman, H. Lacidipine, thiamine pyrophosphate and their combination on the ocular ischemic syndrome induced by bilateral common carotid artery ligation. Int. J. Ophthalmol. 2024, 17, 815–821. [Google Scholar] [CrossRef] [PubMed]
- Ojo, O.B.; Olagunju, G.B.; Olajide, A.O.; Jegede, M.E.; Fakorede, A.S.; Crown, O.O.; Olaleye, M.T.; Akinmoladun, A.C. Spondias mombin leaf extract ameliorates cerebral ischemia/reperfusion-induced cardiohepatorenal oxidative stress in rats. Phytomedicine Plus 2022, 2, 100196. [Google Scholar] [CrossRef]
- Heng, D.Y.; Kollmannsberger, C. Sunitinib. Recent Results Cancer Res. 2010, 184, 71–82. [Google Scholar] [PubMed]
- Kassem, M.G.; Motiur Rahman, A.F.; Korashy, H.M. Sunitinib malate. Profiles Drug Subst. Excip. Relat. Methodol. 2012, 37, 363–388. [Google Scholar]
- Sharma, S.M.; Wu-chen, W.Y.; Yang, Z.; Vilson, F.L.; Guo, Y.; Miller, N.R.; Donald, Z.J.; Bernstein, S.L. Sunitinib Malate Preserves Retinal Ganglion Cells in Rodent NAION. Investig. Ophthalmol. Vis. Sci. 2011, 52, 6614. [Google Scholar]
- Hsueh, H.T.; Kim, Y.-C.; Pitha, I.; Shin, M.D.; Berlinicke, C.A.; Chou, R.T.; Kimball, E.; Schaub, J.; Quillen, S.; Leo, K.T.; et al. Ion-complex microcrystal formulation provides sustained delivery of a multimodal kinase inhibitor from the subconjunctival space for the protection of retinal ganglion cells. Pharmaceutics 2021, 13, 647. [Google Scholar] [CrossRef]
- Bilici, S.; Yazici, G.N.; Altuner, D.; Aggul, A.G.; Suleyman, H. Effect of Sunitinib on Liver Oxidative and Proinflammatory Damage Induced by Ischemia-Reperfusion in Rats. Transplant. Proc. 2021, 53, 2140–2146. [Google Scholar] [CrossRef]
- Suddek, G.M. Sunitinib improves chemotherapeutic efficacy and ameliorates cisplatin-induced nephrotoxicity in experimental animals. Cancer Chemother. Pharmacol. 2022, 67, 1035–1044. [Google Scholar] [CrossRef]
- Nair, A.B.; Jacob, S. A simple practice guide for dose conversion between animals and human. J. Basic Clin. Pharm. 2016, 7, 27–31. [Google Scholar] [CrossRef]
- İnce, S.; Özer, M.; Göktuğ Kadıoğlu, B.; Kuzucu, M.; Gündoğdu, B.; Gürsul, C.; Süleyman, Z.; Suleyman, H. Biochemical and Histopathological Evaluation of Sunitinib Effect on Ovarian Injuries by Ischemia-Reperfusion in Rats. Int. J. Pharmacol. 2021, 17, 65–72. [Google Scholar] [CrossRef]
- Keskin, E.; Erdogan, A.; Suleyman, H.; Yazici, G.N.; Sunar, M.; Gul, M.A. Effect of sunitinib on testicular oxidative and proinflammatory damage induced by ischemia-reperfusion in rats. Rev. Int. Androl. 2022, 20 (Suppl. 1), S17–S23. [Google Scholar] [CrossRef] [PubMed]
- Kurt, A.; Isaoglu, U.; Yilmaz, M.; Calik, M.; Polat, B.; Hakan, H.; Ingec, M.; Suleyman, H. Biochemical and histological investigation of famotidine effect on postischemic reperfusion injury in the rat ovary. J. Pediatr. Surg. 2011, 46, 1817–1823. [Google Scholar] [CrossRef] [PubMed]
- Emir, I.; Suleyman, Z.; Suleyman, H. Effect of thiamine pyrophosphate on oxidative damage in the brain and heart of rats with experimentally induced occlusion of the common carotid artery. Investig. Clín. 2024, 65, 220–229. [Google Scholar] [CrossRef]
- Bradford, M.M. A rapid and sensitive method for the quantitation of microgram quantities of protein utilizing the principle of protein-dye binding. Anal. Biochem. 1976, 72, 248–254. [Google Scholar] [CrossRef]
- Lucas-Ruiz, F.; Galindo-Romero, C.; Albaladejo-García, V.; Vidal-Sanz, M.; Agudo-Barriuso, M. Mechanisms implicated in the contralateral effect in the central nervous system after unilateral injury: Focus on the visual system. Neural Regen. Res. 2021, 16, 2125–2131. [Google Scholar] [CrossRef]
- Machalińska, A.; Kowalska-Budek, A.; Kawa, M.P.; Kazimierczak, A.; Safranow, K.; Kirkiewicz, M.; Wilk, G.; Lubiński, W.; Gutowski, P.; Machaliński, B. Association between asymptomatic unilateral internal carotid artery stenosis and electrophysiological function of the retina and optic nerve. J. Ophthalmol. 2017, 2017, 4089262. [Google Scholar] [CrossRef]
- Guan, Z.H.; Yang, D.; Wang, Y.; Ma, J.B.; Wang, G.N. Ectodysplasin-A2 receptor (EDA2R) knockdown alleviates myocardial ischemia/reperfusion injury through inhibiting the activation of the NF-κB signaling pathway. Exp. Anim. 2024, 73, 376–389. [Google Scholar] [CrossRef]
- Zhang, M.; Liu, Q.; Meng, H.; Duan, H.; Liu, X.; Wu, J.; Gao, F.; Wang, S.; Tan, R.; Yuan, J. Ischemia-reperfusion injury: Molecular mechanisms and therapeutic targets. Signal Transduct. Target Ther. 2024, 9, 12. [Google Scholar] [CrossRef]
- Soares, R.O.S.; Losada, D.M.; Jordani, M.C.; Évora, P.; Castro, E.S.O. Ischemia/Reperfusion Injury Revisited: An Overview of the Latest Pharmacological Strategies. Int. J. Mol. Sci. 2019, 20, 5034. [Google Scholar] [CrossRef]
- Kalogeris, T.; Baines, C.P.; Krenz, M.; Korthuis, R.J. Cell biology of ischemia/reperfusion injury. Int. Rev. Cell. Mol. Biol. 2012, 298, 229–317. [Google Scholar]
- Güler, M.C.; Tanyeli, A.; Ekinci Akdemir, F.N.; Eraslan, E.; Özbek Şebin, S.; Güzel Erdoğan, D.; Nacar, T. An Overview of Ischemia-Reperfusion Injury: Review on Oxidative Stress and Inflammatory Response. Eurasian J. Med. 2022, 54 (Suppl. 1), 62–65. [Google Scholar] [CrossRef] [PubMed]
- Chazelas, P.; Steichen, C.; Favreau, F.; Trouillas, P.; Hannaert, P.; Thuillier, R.; Giraud, S.; Hauet, T.; Guillard, J. Oxidative Stress Evaluation in Ischemia Reperfusion Models: Characteristics, Limits and Perspectives. Int. J. Mol. Sci. 2021, 22, 2366. [Google Scholar] [CrossRef] [PubMed]
- Ayala, A.; Muñoz, M.F.; Argüelles, S. Lipid peroxidation: Production, metabolism, and signaling mechanisms of malondialdehyde and 4-hydroxy-2-nonenal. Oxid. Med. Cell. Longev. 2014, 2014, 360438. [Google Scholar] [CrossRef]
- Cherian, D.A.; Peter, T.; Narayanan, A.; Madhavan, S.S.; Achammada, S.; Vynat, G.P. Malondialdehyde as a Marker of Oxidative Stress in Periodontitis Patients. J. Pharm. Bioallied. Sci. 2019, 11 (Suppl. 2), S297–S300. [Google Scholar] [CrossRef]
- Gumustekin, K.; Taysi, S.; Alp, H.H.; Aktas, O.; Oztasan, N.; Akcay, F.; Suleyman, H.; Akar, S.; Dane, S.; Gul, M. Vitamin E and Hippophea rhamnoides L. extract reduce nicotine-induced oxidative stress in rat heart. Cell Biochem. Funct. 2010, 28, 329–333. [Google Scholar] [CrossRef]
- Chen, B.; Tang, L. Protective effects of catalase on retinal ischemia/reperfusion injury in rats. Exp. Eye Res. 2011, 93, 599–606. [Google Scholar] [CrossRef]
- Chen, L.; Qi, Y.; Yang, X. Neuroprotective effects of crocin against oxidative stress induced by ischemia/reperfusion injury in rat retina. Ophthalmic Res. 2015, 54, 157–168. [Google Scholar] [CrossRef]
- Yan, H.; Peng, Y.; Huang, W.; Gong, L.; Li, L. The Protective Effects of αB-Crystallin on Ischemia-Reperfusion Injury in the Rat Retina. J. Ophthalmol. 2017, 2017, 7205408. [Google Scholar] [CrossRef]
- Ighodaro, O.; Akinloye, O. First line defence antioxidants-superoxide dismutase (SOD), catalase (CAT) and glutathione peroxidase (GPX): Their fundamental role in the entire antioxidant defence grid. Alex. J. Med. 2018, 54, 287–293. [Google Scholar] [CrossRef]
- Ren, X.; Léveillard, T. Modulating antioxidant systems as a therapeutic approach to retinal degeneration. Redox Biol. 2022, 57, 102510. [Google Scholar] [CrossRef]
- Sreekumar, P.G.; Ferrington, D.A.; Kannan, R. Glutathione Metabolism and the Novel Role of Mitochondrial GSH in Retinal Degeneration. Antioxidants 2021, 10, 661. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Huang, Y.; Han, X.; Wang, Y.; Zhang, L.; Chen, L. Evaluating the Protective Effects of Mitochondrial Glutathione on Cerebral Ischemia/Reperfusion Injury via Near-Infrared Fluorescence Imaging. Anal. Chem. 2019, 91, 14728–14736. [Google Scholar] [CrossRef] [PubMed]
- Aliyeva, D.; Amanvermez, R.; Karabulut, K.; Gün, S. The effects of silymarin plus glutathione on the prevention of liver ischemia-reperfusion injury. Braz. J. Pharm. Sci. 2022, 58, e20561. [Google Scholar] [CrossRef]
- Bertero, E.; Maack, C. Ins and Outs of Glutathione in Cardiac Ischemia/Reperfusion Injury. Circ. Res. 2023, 133, 877–879. [Google Scholar] [CrossRef]
- Eltzschig, H.K.; Eckle, T. Ischemia and reperfusion—From mechanism to translation. Nat. Med. 2011, 17, 1391–1401. [Google Scholar] [CrossRef]
- Kvietys, P.R.; Granger, D.N. Role of reactive oxygen and nitrogen species in the vascular responses to inflammation. Free Radic. Biol. Med. 2012, 52, 556–592. [Google Scholar] [CrossRef]
- Guler, M.; Tanyeli, A.; Eraslan, E.; Ekinci Akdemir, F.; Nacar, T.; Topdagı, O. Higenamine decreased oxidative kidney damage induced by ischemia reperfusion in rats. Kafkas Univ. Vet. Fak. Derg. 2020, 26, 365–370. [Google Scholar]
- Topdagi, O.; Tanyeli, A.; Akdemir, F.N.E.; Erdogan, D.G.; Eraslan, E.; Guler, M.C.; Polat, E. Casticin mitigates renal damage injured by ischemia reperfusion: A biochemical study. Int. J. Acad. Med. Pharm. 2021, 3, 245–248. [Google Scholar] [CrossRef]
- Wang, N.; Yang, Y.; Liu, Y.; Huang, L.; Gu, M.; Wu, Y.; Xu, L.; Sun, H.; Guo, W. Magnolol limits NFκB-dependent inflammation by targeting PPARγ relieving retinal ischemia/reperfusion injury. Int. Immunopharmacol. 2022, 112, 109242. [Google Scholar] [CrossRef]
- Yang, Y.; Wang, N.; Xu, L.; Liu, Y.; Huang, L.; Gu, M.; Wu, Y.; Guo, W.; Sun, H. Aryl hydrocarbon receptor dependent anti-inflammation and neuroprotective effects of tryptophan metabolites on retinal ischemia/reperfusion injury. Cell. Death. Dis. 2023, 14, 92. [Google Scholar] [CrossRef]
- Breder, C.D.; Tsujimoto, M.; Terano, Y.; Scott, D.W.; Saper, C.B. Distribution and characterization of tumor necrosis factor-alpha-like immunoreactivity in the murine central nervous system. J. Comp. Neurol. 1993, 337, 543–567. [Google Scholar] [CrossRef] [PubMed]
- Church, L.D.; Cook, G.P.; McDermott, F. Primer: Inflammasomes and interleukin 1beta in inflammatory disorders. Nat. Clin. Pract. Rheumatol. 2008, 4, 34–42. [Google Scholar] [CrossRef]
- Dembic, Z. Chapter 6-cytokines of the immune system: Interleukins. In The Cytokines of the Immune System; Elsevier: Amsterdam, The Netherlands, 2015; pp. 143–239. [Google Scholar]
- Jang, D.I.; Lee, A.H.; Shin, H.Y.; Song, H.R.; Park, J.H.; Kang, T.B.; Lee, S.R.; Yang, S.H. The Role of Tumor Necrosis Factor Alpha (TNF-α) in Autoimmune Disease and Current TNF-α Inhibitors in Therapeutics. Int. J. Mol. Sci. 2021, 22, 2719. [Google Scholar] [CrossRef]
- Lin, W.N.; Kapupara, K.; Wen, Y.T.; Chen, Y.H.; Pan, I.H.; Tsai, R.K. Haematococcus pluvialis-derived astaxanthin is a potential neuroprotective agent against optic nerve ischemia. Mar. Drugs 2020, 18, 85. [Google Scholar] [CrossRef]
- Santonocito, M.; Zappulla, C.; Viola, S.; La Rosa, L.R.; Solfato, E.; Abbate, I.; Tarallo, V.; Apicella, I.; Platania, C.B.M.; Maugeri, G.; et al. Assessment of a new nanostructured microemulsion system for ocular delivery of sorafenib to posterior segment of the eye. Int. J. Mol. Sci. 2021, 22, 4404. [Google Scholar] [CrossRef]
- Jaganjac, M.; Milkovic, L.; Zarkovic, N.; Zarkovic, K. Oxidative stress and regeneration. Free Radic. Biol. Med. 2022, 181, 154–165. [Google Scholar] [CrossRef]
- Musayeva, A.; Unkrig, J.C.; Zhutdieva, M.B.; Manicam, C.; Ruan, Y.; Laspas, P.; Chronopoulos, P.; Göbel, M.L.; Pfeiffer, N.; Brochhausen, C.; et al. Betulinic Acid Protects from Ischemia-Reperfusion Injury in the Mouse Retina. Cells 2021, 10, 2440. [Google Scholar] [CrossRef]
- Renner, M.; Stute, G.; Alzureiqi, M.; Reinhard, J.; Wiemann, S.; Schmid, H.; Faissner, A.; Dick, H.B.; Joachim, S.C. Optic Nerve Degeneration after Retinal Ischemia/Reperfusion in a Rodent Model. Front. Cell. Neurosci. 2017, 11, 254. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Histopathological Parameters | Optic Nerves | SG | CCU | SCCU |
|---|---|---|---|---|
| Median (Quartile 1–Quartile 3) X ± SD | ||||
| Destruction | Right | 0 (0–0) 0 ± 0 | 3 (2–3) * 2.5 ± 0.56 | 0 (0–1) ** 0.42 ± 0.55 |
| Left | 0 (0–0) 0 ± 0 | 3 (2–3) † 2.53 ± 0.56 | 0 (0–1) ‡ 0.42 ± 0.55 | |
| Polymorphonuclear Cell Infiltration | Right | 0 (0–0) 0 ± 0 | 1 (0–1) * 0.83 ± 0.70 | 0 (0–0) ** 0 ± 0 |
| Left | 0 (0–0) 0 ± 0 | 0 (0–0) † 0.11 ± 0.32 | 0 (0–0) ‡ 0 ± 0 | |
| Increase In Connective Tissue Thickness | Right | 0 (0–0) 0 ± 0 | 2 (2–3) * 2.28 ± 0.66 | 0 (0–1) ** 0.44 ± 0.56 |
| Left | 0 (0–0) 0 ± 0 | 1 (1–1) † 0.94 ± 0.63 | 0 (0–0) ‡ 0.17 ± 0.38 | |
| Increase In Astrocyte Cell Population | Right | 0 (0–0) 0 ± 0 | 2 (1–2) * 1.61 ± 0.60 | 0 (0–1) ** 0.42 ± 0.50 |
| Left | 0 (0–0) 0 ± 0 | 2 (1–2) † 1.67 ± 0.68 | 0 (0–1) ‡ 0.42 ± 0.50 | |
| Edema/Vacuolization | Right | 0 (0–0) 0 ± 0 | 3 (2–3) * 2.58 ± 0.50 | 0 (0–1) ** 0.42 ± 0.50 |
| Left | 0 (0–0) 0 ± 0 | 3 (2–3) † 2.31 ± 0.62 | 0 (0–0.75) ‡ 0.25 ± 0.44 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cicek, I.; Esenulku, C.M.; Somuncu, A.M.; Bulut, S.; Yucel, N.; Bal Tastan, T.; Coban, T.A.; Suleyman, H. Sunitinib’s Effect on Bilateral Optic Nerve Damage in Rats Following the Unilateral Clamping and Unclamping of the Common Carotid Artery. Biomedicines 2025, 13, 620. https://doi.org/10.3390/biomedicines13030620
Cicek I, Esenulku CM, Somuncu AM, Bulut S, Yucel N, Bal Tastan T, Coban TA, Suleyman H. Sunitinib’s Effect on Bilateral Optic Nerve Damage in Rats Following the Unilateral Clamping and Unclamping of the Common Carotid Artery. Biomedicines. 2025; 13(3):620. https://doi.org/10.3390/biomedicines13030620
Chicago/Turabian StyleCicek, Ibrahim, Cenap Mahmut Esenulku, Ahmet Mehmet Somuncu, Seval Bulut, Nurinisa Yucel, Tugba Bal Tastan, Taha Abdulkadir Coban, and Halis Suleyman. 2025. "Sunitinib’s Effect on Bilateral Optic Nerve Damage in Rats Following the Unilateral Clamping and Unclamping of the Common Carotid Artery" Biomedicines 13, no. 3: 620. https://doi.org/10.3390/biomedicines13030620
APA StyleCicek, I., Esenulku, C. M., Somuncu, A. M., Bulut, S., Yucel, N., Bal Tastan, T., Coban, T. A., & Suleyman, H. (2025). Sunitinib’s Effect on Bilateral Optic Nerve Damage in Rats Following the Unilateral Clamping and Unclamping of the Common Carotid Artery. Biomedicines, 13(3), 620. https://doi.org/10.3390/biomedicines13030620