
Transimpedance Matrix Measurement (TIM) Parameters Evaluation for the Assessment of Cochlear Implant Electrode Placement and Modiolar Proximity in Children

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Establishing Normative Values for the TIM Measurement
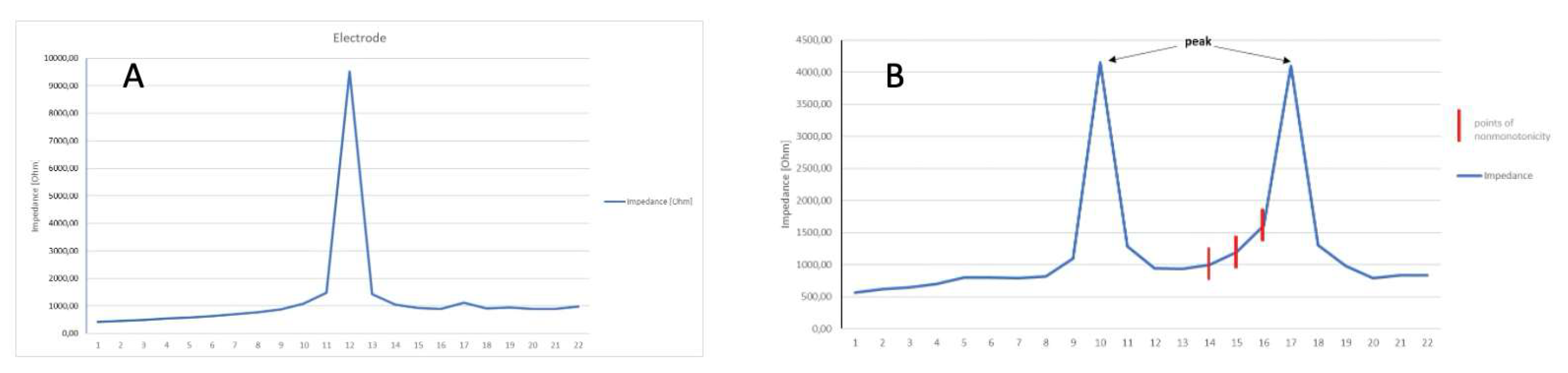
- Mean number of points of non-monotonicity;
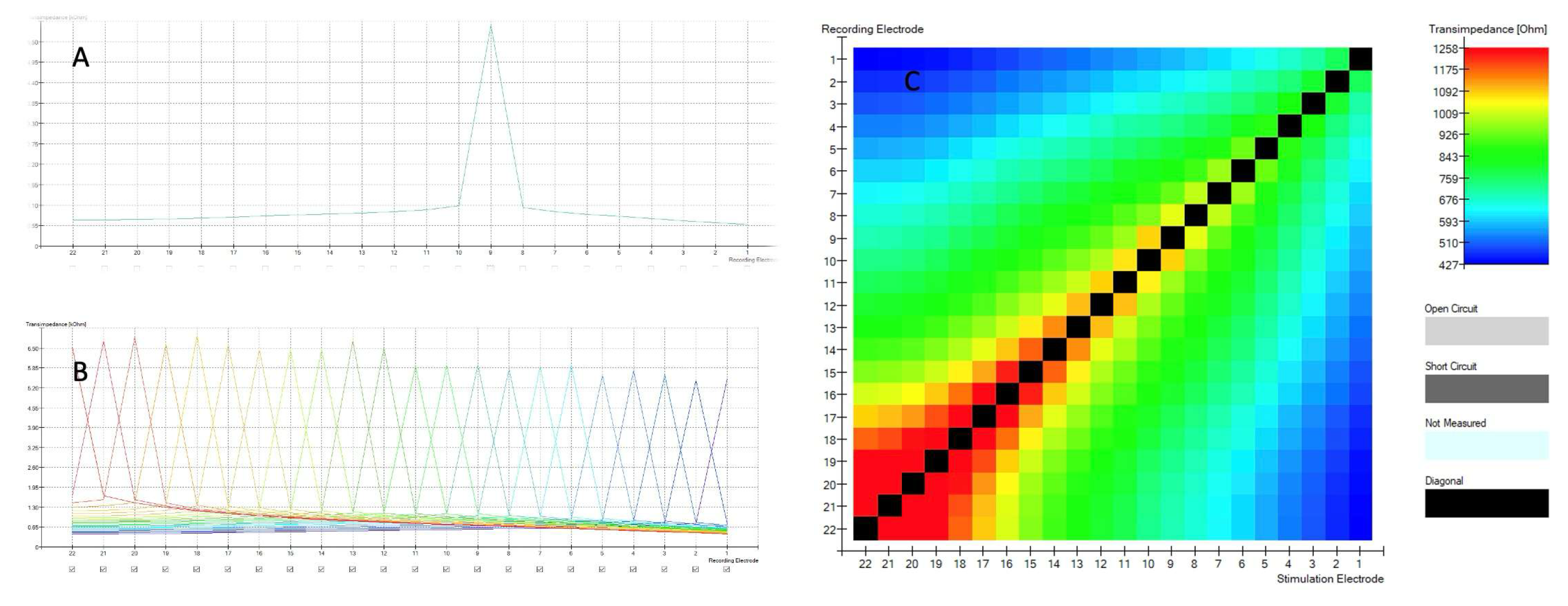
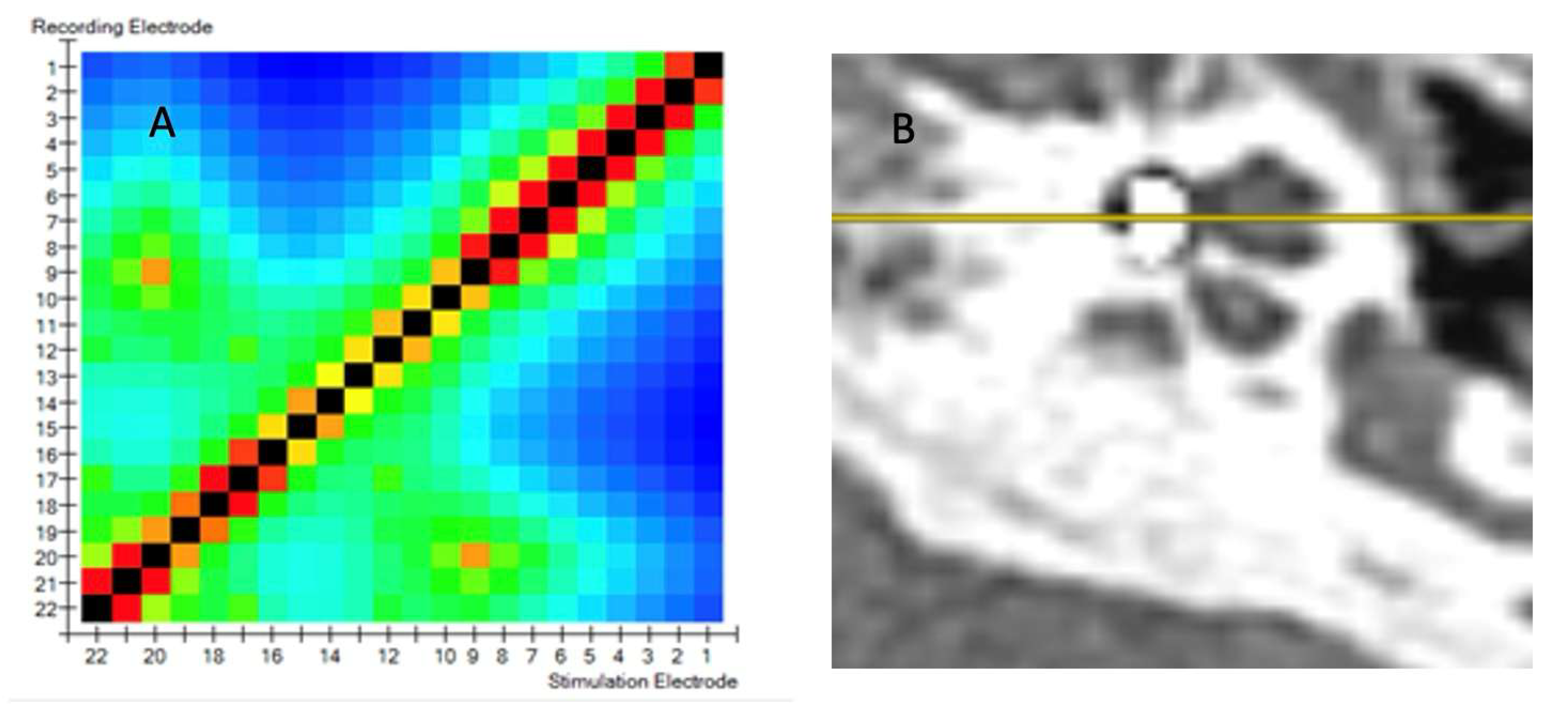
- Mean number of peaks in the matrix;
- Maximum number of points of non-monotonicity;
- Maximum number of peaks in the matrix.
- 5.
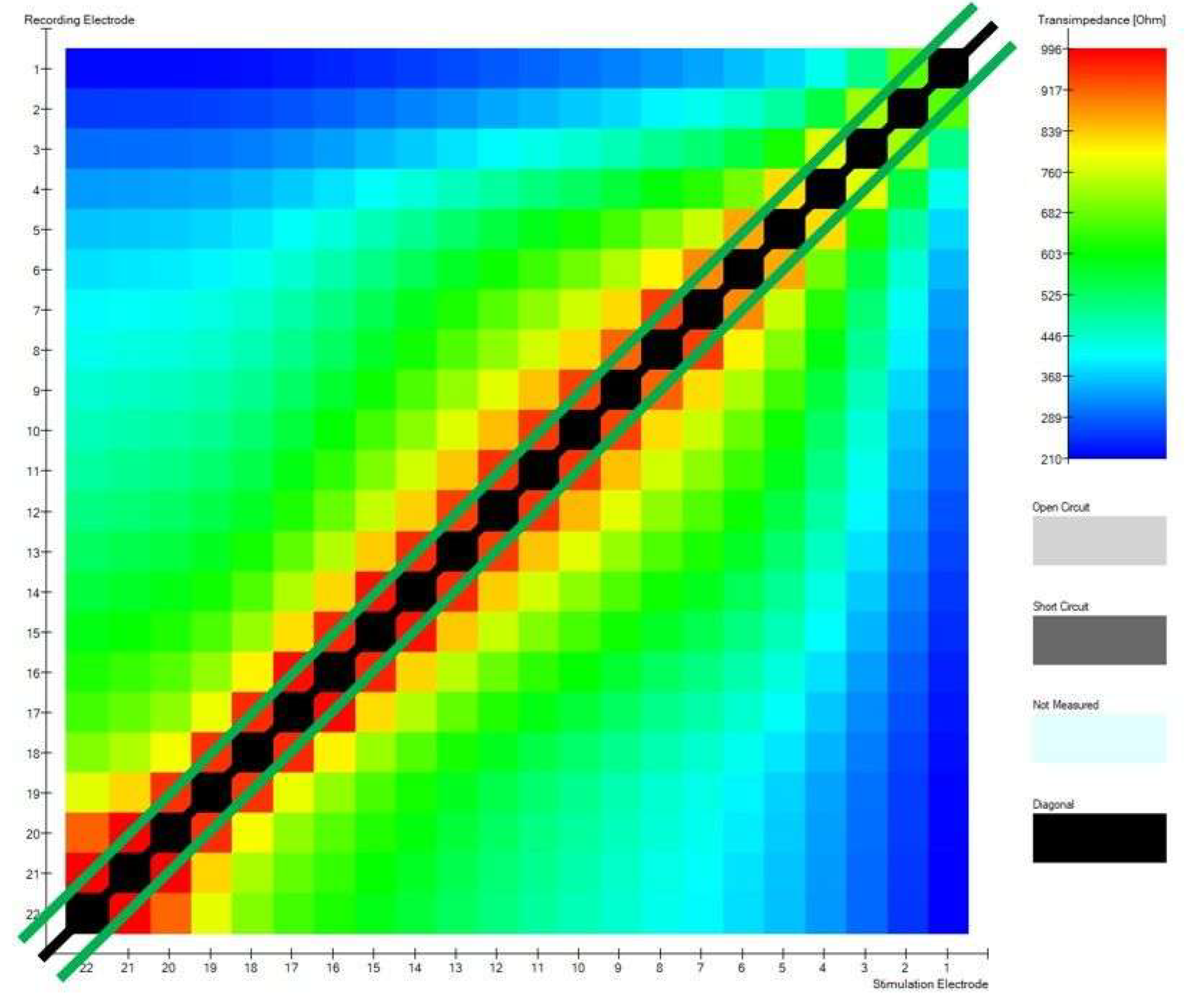
- Correct construction of the diagonal;
- 6.
- Minimalities on the sub-diagonals.
2.2. Statistical Analysis
3. Results
Comparison of Implant Electrode Array Models
4. Discussion
4.1. Electrode Tip Fold-Over (TFO)
4.2. Perimodiolar Electrode Position and Intraoperative Measurements
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients Without TFO | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean Number of Points of Non-Monotonicity | Maximum Number of Points of Non-Monotonicity | Mean Number of Peaks in the Matrix | Maximum Number of Peaks in the Matrix | |||||||
| Mean | SD | M | SD | M | SD | M | SD | |||
| Normal anatomy | 0.064 | 0.266 | 0.109 | 0.379 | 1.04 | 0.197 | 1.04 | 0.206 | ||
| Congenital malformation | 0.355 | 0.368 | 1.73 | 1.56 | 1.07 | 0.143 | 1.64 | 1.29 | ||
| Mean | Standard deviation | Sub-diagonal | Diagonal | AutoNRT | ||||||
| M | SD | M | SD | M | SD | M | SD | M | SD | |
| Normal anatomy | 684 | 191 | 550 | 153 | 31.8 | 4.21 | 0.935 | 0.250 | 2.09 | 4.37 |
| Congenital malformation | 980 | 416 | 1039 | 412 | 31.9 | 8.72 | 1 | 0 | 7 | 8.22 |
| All patients | ||||||||||
| Mean number of points of non-monotonicity | Maximum number of points of non-monotonicity | Mean number of peaks in the matrix | Maximum number of peaks in the matrix | |||||||
| Mean | SD | M | SD | M | SD | M | SD | |||
| Normal anatomy | 0.303 | 0.876 | 0.52 | 1.47 | 1.10 | 0.275 | 1.18 | 0.560 | ||
| Congenital malformation | 0.639 | 1.05 | 2.17 | 2.12 | 1.23 | 0.560 | 1.92 | 1.56 | ||
| Mean value | Standard deviation | Sub-diagonal | Diagonal | AutoNRT | ||||||
| M | SD | M | SD | M | SD | M | SD | M | SD | |
| Normal anatomy | 700 | 216 | 578 | 270 | 31.8 | 4.57 | 0.920 | 0.274 | 2.10 | 4.22 |
| Congenital malformation | 1009 | 409 | 1126 | 495 | 31.6 | 8.39 | 0.917 | 0.289 | 7.83 | 8.35 |
References
- Perenyi, A.; Toth, F.; Dimak, B.; Nagy, R.; Schoerg, P.; Jori, J.; Kiss, J.G.; Sprinzl, G.; Csanady, M.; Rovo, L. Electrophysiological measurements with electrode types of different perimodiolar properties and the same cochlear implant electronics—A retrospective comparison study. J. Otolaryngol. Head Neck Surg. 2019, 48, 46. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Aschendorff, A.; Briggs, R.; Brademann, G.; Helbig, S.; Hornung, J.; Lenarz, T.; Marx, M.; Ramos, A.; Stöver, T.; Escudé, B.; et al. Clinical investigation of the Nucleus Slim Modiolar Electrode. Audiol. Neurootol. 2017, 22, 169–179. [Google Scholar] [CrossRef] [PubMed]
- Haber, K.; Neagu, A.; Konopka, W.; Amernik, K.; Gheorghe, D.C.; Drela, M.; Wrukowska-Niemczewska, I.; Mierzwiński, J. The influence of Slim Modiolar electrode on residual hearing in pediatric patients. Eur. Arch. Otorhinolaryngol. 2021, 278, 2723–2732. [Google Scholar] [CrossRef] [PubMed]
- Gabrielpillai, J.; Burck, I.; Baumann, U.; Stöver, T.; Helbig, S. Incidence for Tip Foldover During Cochlear Implantation. Otol. Neurotol. 2018, 39, 1115–1121. [Google Scholar] [CrossRef] [PubMed]
- Zuniga, M.G.; Rivas, A.; Hedley-Williams, A.; Gifford, R.H.; Dwyer, R.; Dawant, B.M.; Sunderhaus, L.W.; Hovis, K.L.; Wanna, G.B.; Noble, J.H.; et al. Tip Fold-over in Cochlear Implantation: Case Series. Otol. Neurotol. 2017, 38, 199–206. [Google Scholar] [CrossRef]
- Fishman, A.J.; Roland, J.T., Jr.; Alexiades, G.; Mierzwinski, J.; Cohen, N.L. Fluoroscopically assisted cochlear implantation. Otol. Neurotol. 2003, 24, 882–886. [Google Scholar] [CrossRef]
- Perényi, Á.; Nagy, R.; Dimák, B.; Csanády, M.; Jóri, J.; Kiss, J.G.; Rovó, L. Cochlearis implantátumok különböző, előre görbített elektródasorainak elhelyezkedése a cochlea tengelyéhez viszonyítva. Radiológiai vizsgálat a perimodiolaritás mértékének megállapítására. [The distance from the modiolus of perimodiolar electrode arrays of cochlear implants. A radiological study to evaluate the difference in perimodiolar properties]. Orv. Hetil. 2019, 160, 1216–1222. (In Hungarian) [Google Scholar] [CrossRef] [PubMed]
- Grolman, W.; Maat, A.; Verdam, F.; Simis, Y.; Carelsen, B.; Freling, N.; Tange, R.A. Spread of excitation measurements for the detection of electrode array foldovers: A prospective study comparing 3-dimensional rotational x-ray and intraoperative spread of excitation measurements. Otol. Neurotol. 2009, 30, 27–33. [Google Scholar] [CrossRef]
- Vanpoucke, F.J.; Boermans, P.P.; Frijns, J.H. Assessing the placement of a cochlear electrode array by multidimensional scaling. IEEE Trans. Biomed. Eng. 2012, 59, 307–310. [Google Scholar] [CrossRef]
- Hoppe, U.; Brademann, G.; Stöver, T.; Ramos de Miguel, A.; Cowan, R.; Manrique, M.; Falcón-González, J.C.; Hey, M.; Baumann, U.; Huarte, A.; et al. Evaluation of a Transimpedance Matrix Algorithm to Detect Anomalous Cochlear Implant Electrode Position. Audiol. Neurootol. 2022, 27, 347–355. [Google Scholar] [CrossRef]
- Leblans, M.; Zarowski, A.; Molisz, A.; van Dinther, J.; Dedeyne, J.; Lerut, B.; Kuhweide, R.; Offeciers, E. Cochlear implant electrode array tip-foldover detection by electrode voltage telemetry. Cochlear Implant. Int. 2023, 24, 95–106. [Google Scholar] [CrossRef] [PubMed]
- Mierzwiński, J.; Van Den Heuvel, E.; Fishman, A.J.; Rivera, A.L.; Haber, K.; Skrivan, J. Application of “banana cochleostomy” and looped electrode insertion for cochlear implantation in children with common cavity malformation and cystic forms of cochlear hypoplasia. Int. J. Pediatr. Otorhinolaryngol. 2018, 112, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Naples, J.G.; Ruckenstein, M.J. Cochlear Implant. Otolaryngol. Clin. N. Am. 2020, 53, 87–102. [Google Scholar] [CrossRef] [PubMed]
- Holden, L.K.; Finley, C.C.; Firszt, J.B.; Holden, T.A.; Brenner, C.; Potts, L.G.; Gotter, B.D.; Vanderhoof, S.S.; Mispagel, K.; Heydebrand, G.; et al. Factors affecting open-set word recognition in adults with cochlear implants. Ear. Hear. 2013, 34, 342–360. [Google Scholar] [CrossRef]
- Varghese, J.J.; Walia, A.; Lefler, S.M.; Ortmann, A.J.; Shew, M.A.; Durakovic, N.; Wick, C.C.; Herzog, J.A.; Buchman, C.A. Identifying Slim Modiolar Electrode Tip Fold-Over with Intracochlear Electrocochleography. Otolaryngol. Head Neck Surg. 2024, 170, 1124–1132. [Google Scholar] [CrossRef]
- Harris, M.S.; Riggs, W.J.; Giardina, C.K.; O’Connell, B.P.; Holder, J.T.; Dwyer, R.T.; Koka, K.; Labadie, R.F.; Fitzpatrick, D.C.; Adunka, O.F. Patterns Seen During Electrode Insertion Using Intracochlear Electrocochleography Obtained Directly Through a Cochlear Implant. Otol. Neurotol. 2017, 38, 1415–1420. [Google Scholar] [CrossRef]
- Gawęcki, W.; Balcerowiak, A.; Podlawska, P.; Borowska, P.; Gibasiewicz, R.; Szyfter, W.; Wierzbicka, M. Robot-Assisted Electrode Insertion in Cochlear Implantation Controlled by Intraoperative Electrocochleography-A Pilot Study. J. Clin. Med. 2022, 11, 7045. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jwair, S.; Prins, A.; Wegner, I.; Stokroos, R.J.; Versnel, H.; Thomeer, H.G.X.M. Scalar Translocation Comparison Between Lateral Wall and Perimodiolar Cochlear Implant Arrays—A Meta-Analysis. Laryngoscope 2021, 131, 1358–1368. [Google Scholar] [CrossRef]
- Klabbers, T.M.; Huinck, W.J.; Heutink, F.; Verbist, B.M.; Mylanus, E.A.M. Transimpedance Matrix (TIM) Measurement for the Detection of Intraoperative Electrode Tip Foldover Using the Slim Modiolar Electrode: A Proof of Concept Study. Otol. Neurotol. 2021, 42, e124–e129. [Google Scholar] [CrossRef]
- Ramos-Macias, A.; De Miguel, A.R.; Falcon-González, J.C. Mechanisms of electrode fold-over in cochlear implant surgery when using a flexible and slim perimodiolar electrode array. Acta Otolaryngol. 2017, 137, 1129–1135. [Google Scholar] [CrossRef]
- Salkim, E.; Zamani, M.; Jiang, D.; Saeed, S.R.; Demosthenous, A. Insertion Guidance Based on Impedance Measurements of a Cochlear Electrode Array. Front. Comput. Neurosci. 2022, 16, 862126. [Google Scholar] [CrossRef] [PubMed]
- Gottfried, T.M.; Galeazzi, P.; Föger, A.; Dejaco, D.; Tröger, A.; Fischer, N.; Innerhofer, V.; Di Trapani, F.; Weiss, N.; Seebacher, J.; et al. Evaluation of an impedance-based method to monitor the insertion of the electrode array during cochlear implantation. Eur. Arch. Otorhinolaryngol. 2024, 281, 4121–4131. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-Y.; Kim, Y.S.; Jo, H.D.; Kim, Y.; Carandang, M.; Huh, G.; Choi, B.Y. Effects of in vivo repositioning of slim modiolar electrodes on electrical thresholds and speech perception. Sci. Rep. 2021, 11, 15135. [Google Scholar] [CrossRef]
- Riojas, K.E.; Bruns, T.L.; Granna, J.; Webster, R.J., III; Labadie, R.F. Robotic pullback technique of a precurved cochlear-implant electrode array using real-time impedance sensing feedback. Int. J. Comput. Assist. Radiol. Surg. 2023, 18, 413–421. [Google Scholar] [CrossRef]
- Riojas, K.E.; Bruns, T.L.; Granna, J.; Smetak, M.R.; Labadie, R.F.; Webster, R.J., III. Towards inferring positioning of straight cochlear-implant electrode arrays during insertion using real-time impedance sensing. Int. J. Med. Robot. Comput. Assist. Surg. 2024, 20, e2609. [Google Scholar] [CrossRef]
- Pile, J.; Sweeney, A.D.; Kumar, S.; Simaan, N.; Wanna, G.B. Detection of modiolar proximity through bipolar impedance measurements. Laryngoscope 2017, 127, 1413–1419. [Google Scholar] [CrossRef] [PubMed]

| Measure | Mean Value—in Fold-Over Cases | Mean Value—Proper Insertion Cases | T Test | df | p |
|---|---|---|---|---|---|
| 3.045 | 0.064 | −7.882 | 3.066 | 0.004 |
| 1.727 | 1.041 | −4.877 | 3.272 | 0.013 |
| 5.250 | 0.109 | −10.667 | 3.082 | 0.002 |
| 2.750 | 1.043 | −3.558 | 3.024 | 0.037 |
| 0.750 | 0.935 | 0.731 | 3.131 | 0.516 |
| 32.250 | 31.783 | −0.107 | 3.124 | 0.921 |
| Measure | Mean Value in CA Electrode | Mean Value in SM Electrode | T Test | df | p-Value |
|---|---|---|---|---|---|
| 0 | 0.098 | −1.655 | 29 | 0.109 |
| 1 | 1.063 | −1.437 | 29 | 0.161 |
| 0 | 0.167 | −1.980 | 29 | 0.057 |
| 1 | 1.067 | −1.439 | 29 | 0.161 |
| 1 | 0.900 | 1.795 | 29 | 0.083 |
| 29.750 | 32.867 | −2.258 | 29 | 0.034 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Radomska, K.; Talar, M.; Haber, K.; Mierzwińska-Dolny, P.; Fishman, A.J.; Mierzwiński, J. Transimpedance Matrix Measurement (TIM) Parameters Evaluation for the Assessment of Cochlear Implant Electrode Placement and Modiolar Proximity in Children. Biomedicines 2025, 13, 319. https://doi.org/10.3390/biomedicines13020319
Radomska K, Talar M, Haber K, Mierzwińska-Dolny P, Fishman AJ, Mierzwiński J. Transimpedance Matrix Measurement (TIM) Parameters Evaluation for the Assessment of Cochlear Implant Electrode Placement and Modiolar Proximity in Children. Biomedicines. 2025; 13(2):319. https://doi.org/10.3390/biomedicines13020319
Chicago/Turabian StyleRadomska, Katarzyna, Marcin Talar, Karolina Haber, Paulina Mierzwińska-Dolny, Andrew J. Fishman, and Józef Mierzwiński. 2025. "Transimpedance Matrix Measurement (TIM) Parameters Evaluation for the Assessment of Cochlear Implant Electrode Placement and Modiolar Proximity in Children" Biomedicines 13, no. 2: 319. https://doi.org/10.3390/biomedicines13020319
APA StyleRadomska, K., Talar, M., Haber, K., Mierzwińska-Dolny, P., Fishman, A. J., & Mierzwiński, J. (2025). Transimpedance Matrix Measurement (TIM) Parameters Evaluation for the Assessment of Cochlear Implant Electrode Placement and Modiolar Proximity in Children. Biomedicines, 13(2), 319. https://doi.org/10.3390/biomedicines13020319