Abstract
Introduction/Objectives: Restless legs syndrome (RLS), a chronic neurological disorder related to brain iron metabolism, has been linked to immune-mediated inflammatory conditions such as psoriatic arthritis (PsA). However, the role that inflammation plays in this association and the impact of RLS on PsA outcomes remain unclear. This study aims to investigate the association between RLS and inflammatory/clinical parameters in PsA patients. Materials and Methods: In this cross-sectional study, 230 PsA patients completed the International Restless Legs Syndrome Study Group (IRLSSG) screening questionnaire, with diagnoses confirmed by a neurologist. Data collected included clinical features, disease activity, and comorbidities (obesity, anxiety, depression, insomnia, and fibromyalgia). Results: In total, forty-six patients met the IRLSSG criteria (20%). Those with RLS more frequently had polyarthritis (27% vs. 6%; p < 0.001), more swollen joints (2.0 vs. 1.4; p = 0.04), greater psoriatic involvement (5.7 vs. 3.6; p < 0.001), greater fatigue (39.0 vs. 30.5; p < 0.001), and greater disease activity (14.5 vs. 10.5; p < 0.001). They also exhibited increased disease impact (4.7 vs. 2.9; p < 0.001), poorer functioning (0.7 vs. 0.5; p = 0.01), and higher levels of anxiety (8.0 vs. 5.5; p < 0.001), depression (6.5 vs. 3.9; p < 0.001), and sleep disturbance (13.9 vs. 8.7; p < 0.001). Skin lesions and polyarthritis explained nearly 40% of RLS cases (Odds Ratio (OR) 1.4; 95% Confidence Interval (CI) 1.03–2.0; p = 0.03 and OR 1.03; 95% CI 1.00–1.9; p = 0.04). Conclusions: Psoriatic activity and inflammation may contribute to RLS in PsA. The coexistence of RLS was associated with greater disease activity, greater disease impact, and more emotional and sleep-related comorbidities.
1. Introduction
Psoriatic arthritis (PsA) is a chronic inflammatory disease that can affect the joints, entheses, the spine, and the skin. Psoriatic arthritis is a chronic, immune-mediated inflammatory arthritis associated with psoriasis. Its incidence varies geographically, influenced by genetic and environmental factors. Genetic predisposition plays a significant role, with familial aggregation and specific HLA alleles contributing to susceptibility. The pathogenesis is complex and multifactorial, involving an interplay between genetic susceptibility and environmental triggers such as infections, microbiota changes, obesity, and biomechanical stress, which activate innate and adaptive immune responses [1].
It is associated with a wide range of comorbidities, including sleep disorders [2]. These disorders are a heterogeneous group of conditions, of which sleep apnoea, insomnia, and restless legs syndrome (RLS) are the most common.
RLS is a chronic movement disorder characterised by an urge to move one’s legs, generally accompanied by uncomfortable feelings, that may interfere with sleep. Although the physiopathology of RLS is not fully understood, the most widely accepted hypotheses include (a) genetic variants; (b) abnormal iron metabolism in the central nervous system; and (c) dopaminergic dysfunction [3]. The decision to investigate the association between RLS and PsA is supported by several converging lines of evidence. First, emerging research indicates that RLS is significantly more prevalent in patients with immune-mediated inflammatory diseases, including rheumatoid arthritis (up to 30%), systemic lupus erythematosus, and axial spondyloarthritis, compared to the general population (7–10%). Second, both conditions share common pathophysiological mechanisms involving systemic inflammation and immune dysregulation. Multiple studies have demonstrated elevated inflammatory markers, particularly C-reactive protein (CRP), tumour necrosis factor-alpha (TNF-α), and interleukin-17 (IL-17), in patients with RLS. These same pro-inflammatory cytokines play central roles in PsA pathogenesis, suggesting overlapping inflammatory pathways that could mechanistically link these conditions [4,5,6,7,8]. Nonetheless, there is currently limited information on the influence of the inflammatory process on the development of RLS or the impact of RLS on clinical manifestations in PsA. Because of this, we decided to perform a study that assesses the relationship of RLS with inflammatory and clinical factors in a cohort of patients with PsA.
2. Materials and Methods
We performed a cross-sectional observational study that included adults (over 18 years of age) diagnosed with PsA according to the CASPAR criteria [9]. Participants who agreed to participate in this study and gave their written informed consent were consecutively recruited from the Rheumatology Department at Salamanca University Hospital between 1 September 2023 and 30 April 2024.
Exclusion criterion: Patients taking antidepressant or anxiolytic drugs, given their potential influence on the occurrence of RLS [10,11].
All participants completed a screening questionnaire based on the International Restless Legs Syndrome Study Group (IRLSSG) criteria [12]. This questionnaire covered four features of RLS: (1) the urge to move the legs, usually but not always accompanied by—or felt to be caused by—uncomfortable and unpleasant sensations in the legs; (2) the urge to move the legs and any accompanying unpleasant sensations that begin or worsen during periods of rest or inactivity, such as lying down or sitting; (3) the urge to move the legs and any accompanying unpleasant sensations that are partially or totally relieved by movement, such as walking or stretching, at least as long as the activity continues; and (4) the urge to move the legs and any accompanying unpleasant sensations during rest or inactivity that only occur or are worse in the evening or at night than during the day. Patients who reported showing all four of these features were assessed by an expert neurologist (LLM) who confirmed or ruled out the diagnosis of RLS. The process is summarised in the flowchart (Figure 1).
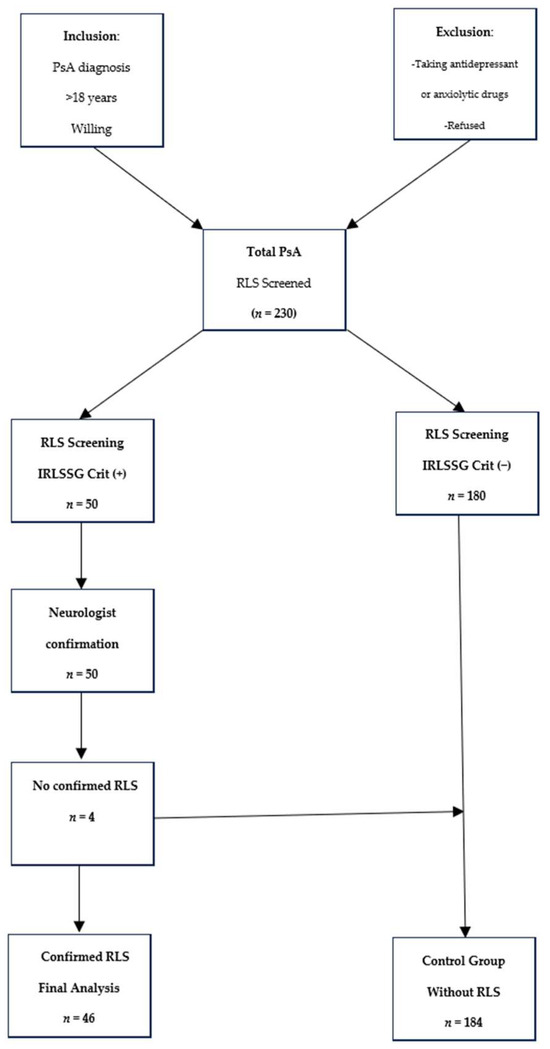
Figure 1.
Study Population Flow Diagram and Selection Process. +: Positive, −: Negetive.
2.1. Data Were Recorded on the Following Variables
2.1.1. Standard Baseline Demographic Characteristics and Routine Blood Test Results
Age, sex, time since disease onset (years), smoking status (smoker/former smoker/non-smoker; a person who had previously been a smoker but had not smoked for at least 12 months was classified as a former smoker), and the number of cigarettes smoked measured in pack-years [13]; CRP level, additional blood parameters such as iron status (iron, ferritin, transferrin saturation, total iron-binding capacity), and kidney function (creatinine level) due to their potential association with RLS.
2.1.2. Variables Related to the Treatment Received
Treatment with conventional synthetic disease-modifying antirheumatic drugs (csDMARDs), targeted synthetic disease-modifying antirheumatic drugs (tsDMARDs), and biologic disease-modifying antirheumatic drugs (bDMARDs), and also any changes in treatment due to poor response to tsDMARDs or bDMARDs.
2.1.3. Variables Related to Psoriatic Disease
Clinical form of the disease at the time of the study peripheral, mixed, or axial classifying patients with inflammatory lower back pain and radiographic damage (sacroiliitis of at least grade 2 as per New York criteria and/or the presence of syndesmophytes) as having axial involvement [14,15]; dactylitis (current or past); and the number of entheses involved as assessed using the modified Maastricht Ankylosing Spondylitis Enthesitis Score (mMASES) [16]. The original MASES [17] took into account 13 entheses (the bilateral first and seventh costochondral joints, the anterior and posterior superior iliac spine, the iliac crests, the proximal insertion of the Achilles tendons, and the fifth lumbar spinous process). That score was modified for PsA to include the plantar fascia, with scores ranging from 0 to 15 [17]. Further, the extent of psoriasis was assessed using the Psoriasis Area Severity Index (PASI) [18] and the third item of the PsA Impact of Disease (PsAID) questionnaire (skin problems, including itchiness), and fatigue was assessed using the Functional Assessment of Chronic Illness Therapy (FACIT) fatigue scale [19]. Permission to use the latter instrument was obtained from FACIT.org (Access date: 22 October 2023).
Disease activity, functioning, and disease impact: In the case of peripheral involvement, disease activity was measured using the Disease Activity in Psoriatic Arthritis (DAPSA) score [20], a composite measure designed to assess disease activity in PsA. The DAPSA score is the sum of the CRP (mg/dL), tender joint count (0–68), swollen joint count (0–66), the patient’s global assessment of disease activity score (between 0 and 10 on a numerical rating scale [NRS]), and the pain NRS score (0–10). In addition, we recorded whether patients had polyarthritis (involvement of five or more joints). In cases of axial involvement, we used the Ankylosing Spondylitis Disease Activity Score with C-reactive protein (ASDAS-CRP) [21]. We measured functional ability based on the Health Assessment Questionnaire-Disability Index (HAQ-DI) for peripheral involvement and the Bath Ankylosing Spondylitis Functional Index (BASFI) for axial involvement [22,23]. Disease impact was assessed using the PsAID-12 [24].
2.1.4. Further, Comorbidities Were Evaluated Using Validated Questionnaires
Emotional distress was assessed using the Hospital Anxiety and Depression Scale (HADS), a 14-item scale applied to identify anxiety and depression in patients with physical illnesses. Scores range from 0 to 21 for each subscale (HADS-D for depression and HADS-A for anxiety) and are classified as normal (0–7); borderline abnormal, indicating a possible clinical disorder (8–10); and abnormal, indicating a probable clinical disorder (11–21) [25].
Sleep quality was measured with the Insomnia Severity Index (ISI). The ISI is a self-administered questionnaire that includes 7 items that address the nature, severity, and impact of insomnia. Patient responses are reported on a 5-point Likert-type scale (0 to 4) for the previous month. The overall score ranges between 0 and 28 and is classified as no clinically significant insomnia (0–7), subthreshold insomnia (8–14), clinical insomnia (moderate severity) (15–21), and clinical insomnia (severe) (22–28) [26].
Obesity was measured using body mass index (BMI) [27].
Fibromyalgia: This condition was assessed using the diagnostic criteria of the Analgesic, Anaesthetic, and Addiction Clinical Trial Translations, Innovations, Opportunities, and Networks—American Pain Society Pain Taxonomy (AAPT) [28].
2.2. Statistical Analysis
Quantitative variables are reported as the mean and standard deviation (SD) if the data are normally distributed; otherwise, they are reported as the median and interquartile range (IQR), and the categorical variables are reported as numbers and percentages (N/%). The groups were compared using the t-test for normally distributed quantitative variables and the Mann–Whitney test for ordinal or non-normally distributed quantitative variables. Comparisons between more than two groups were performed using one-factor analysis of variance (normally distributed quantitative variables) and the Kruskal–Wallis test (ordinal or non-normally distributed quantitative variables). The threshold for statistical significance was set at p < 0.05.
Binary logistic regression explanatory model was employed to identify independent predictors of RLS occurrence in PsA patients. This model is appropriate for binary dependent variables (presence/absence of RLS), where the outcome is coded as 1 (RLS confirmed) or 0 (no RLS). These included both variables found to be significant in our univariate analysis and those associated with RLS in previous studies, such as fatigue [6], psoriasis severity [29], CRP [30,31], ferritin levels [32], smoking status [33,34], age [35], obesity [36], sex [12], and fibromyalgia [37].
Two approaches were used to analyse the reliability and stability of the logistic regression results in relation to the sample size of the study. First, the approach proposed by Peluzzi et al. [38] was applied, whereby the sample size for a logistic regression is calculated based on the events per variable, the number of predictor variables, and the expected proportion. The adjusted logistic model has 12 variables, a minimum of 10 events per variable, and an expected proportion of 0.5, so the required sample size would be 240. The power has also been calculated for a logistic regression model with a dichotomous variable, a significance level of 5%, an odds ratio of 2, and a proportion of 50%. Under these conditions, the power of the analysis would be 80%. The ‘powermediation’ package, version 0.3.4, in R, version 4.5.2, was used to calculate the statistical power of the models. Statistical analyses were performed using IBM SPSS Statistics for Windows, Version 23.0 (IBM Corp., Armonk, NY, USA).
2.3. Ethical Statement
2.3.1. Study Approval and Ethical Compliance
This study was conducted in accordance with the principles established in the Declaration of Helsinki and adhered to all applicable ethical guidelines for human research. The study protocol was prospectively reviewed and approved by the Institutional Review Board (Ethics Committee) of Salamanca University Hospital (Comité de Ética en Investigación Clínica—CEIC), with project number PI 2023 03 1560 (approved on 24 April 2023).
2.3.2. Informed Consent Procedures
All eligible participants were provided with detailed written information about the study objectives, procedures, data collection methods, and potential risks or benefits of participation. Prior to enrollment, written informed consent was obtained from each participant after ensuring they fully understood the study protocol and had the opportunity to ask questions. All participants had the right to withdraw from the study at any time without providing justification or incurring any consequences on their clinical care.
2.3.3. Data Protection and Confidentiality
Patient data were collected and managed in accordance with current data protection regulations. All collected information was assigned a unique identification code, and personal identifiers were removed from the database to ensure participant confidentiality and anonymity throughout the study. Data were stored securely in a password-protected database accessible only to authorised research team members.
3. Results
3.1. Baseline Variables
Out of the 230 patients recruited, 50 (21.7%) met the IRLSSG criteria for RLS [12]. After being assessed by a neurologist (LM), four patients were excluded from this study (three with a diagnosis of nocturnal cramps and one with polyneuropathy).
Among the 46 patients with confirmed RLS (20% of the sample), the majority were smokers, and this group had more discomfort associated with psoriasis and reported greater levels of fatigue. Table 1 summarises our analysis of these and other descriptive statistics.

Table 1.
General characteristics of the disease and treatment received overall and stratified by whether patients met the RLS criteria.
3.2. Disease Activity, Functioning, and Disease Impact
Patients with RLS were found to have greater disease activity clinically in terms of both swollen and tender joint counts. Moreover, they also had poorer functioning. The results are shown in Table 2.
Table 2.
Disease activity, functioning, and disease impact.
3.3. Comorbidities
Patients with RLS had higher levels of anxiety and depression and poorer sleep quality. The results are shown in Table 3.
Table 3.
Comorbidities (emotional state, sleep quality, obesity, and fibromyalgia).
In binary logistic regression explanatory model, Nagelkerke R2: 0.38, skin problems/itchiness (OR 1.4; 95% CI 1.03–2.0; p = 0.03) emerged as the only robust independent predictor of RLS. Although polyarthritis (presence/absence) (OR 1.03; 95% CI 1.00–1.9; p = 0.04) reached nominal statistical significance, the confidence interval boundary at 1.0, minimal effect size (3% odds increase), and small number of polyarthritis cases (n = 12) suggest this finding is marginally significant and warrants cautious interpretation. None of the other variables reached significance: FACIT-F (p = 0.7), PASI (p = 0.8), CRP (p = 0.1), ferritin (p = 0.2), HADS-D (p = 0.1), smoking exposure in pack-years (p = 0.2), age (p = 0.5), BMI (p = 0.1), sex (p = 0.06), or fibromyalgia (p = 0.3).
4. Discussion
RLS that occurred alongside PsA was associated with more symptomatic psoriasis (related to itching). It is possible that the polyarticular inflammatory process may increase the presence of this comorbidity.
As only a few studies within the scientific literature have examined the relationship between PsA and RLS, it is difficult to compare our results with those of previous research. Indirect evidence from a small cohort of patients with PsA was provided by Sandikci et al., who observed a higher rate of DMARD use in patients with RLS than those without RLS, suggesting that individuals with this syndrome had greater skin and joint disease activity [8].
In our study, skin problems (including itchiness) were related to the presence of RLS. To our knowledge, this association has not previously been reported, although itchiness has previously been associated with poorer sleep quality in patients with cutaneous psoriasis. In Callis Duffin et al.’s study, itchiness was a predictor of poor sleep quality (OR 1.24, 95% CI 1.11-1.39; p < 0.0001) [39]. It is possible to hypothesise that abnormalities in dopamine pathways, related to the aetiopathogenesis of RLS, may be responsible for sensory abnormalities that increase the discomfort associated with psoriasis. Previous studies have already observed a relationship between psoriasis severity and RLS. In particular, Solak et al. found an association between psoriasis severity, as measured by the PASI, and the development of RLS. The authors attributed this association to the greater levels of inflammation seen in the most severe forms of psoriasis. We did not find a relationship between PASI and RLS: this difference may be due to our patients having milder cutaneous involvement (1.8 vs. 5.4 in patients studied by Solak et al.) [29].
With the limitations related to the OR value, we found a possible relationship between the joint inflammatory process and the presence of SPI. In patients with psoriasis, Solak et al. concluded that RLS was associated with higher levels of CRP (5.0 vs. 3.0 mg/dL; p = 0.03) [29]. Their results are in line with those of Nowowiejska et al., who, in a cohort of 70 patients with psoriasis, also found that patients with RLS had higher levels of CRP (p = 0.01) [30]. In another context, in a recently published paper, Dowsett et al. compared plasma from donors who were and were not classified as RLS cases and found that those with RLS had higher CRP levels than the controls (0.74 mg/L, IQR: 0.17–1.90 vs. 0.52 mg/L, IQR: 0.14–1.39; p = 0.032) [31]. Further, when CRP plasma concentrations were grouped into high (>3 mg/L) and low (<3 mg/L) levels, a higher percentage of RLS cases compared with the controls had high CRP (p = 0.049) [31]. Nonetheless, similar studies have yielded different results [30,40], though these inconsistencies may be due to the use of different criteria to diagnose RLS. Despite this indirect evidence, the role of inflammation in the physiopathology of RLS is not yet fully understood. This role may be able to be explained given the link between inflammation and hypoxia. A proteomics study found that eight inflammation-related proteins were differentially expressed in patients with RLS, and network analysis revealed indirect links with the proteins involved in hypoxia pathways [41].
Regarding other variables potentially associated with RLS, our univariate analysis indicated that patients with RLS had higher levels of fatigue, anxiety, and depression, as well as poorer sleep quality. In the multivariate analysis, Sandikci et al. found that RLS severity was associated with fatigue and depression [8]. An association is very commonly found between fatigue and RLS. Nonetheless, as the physiopathology of these conditions is not fully understood, the reasons for such an association remain unknown, although it may be related to abnormalities in dopamine pathways [42,43].
In a recent systematic review, depression was found to be associated with RLS (OR = 1.71, 95% CI = 1.26–2.32) [35]. Although the precise mechanisms underlying this association have yet to be established, there is some indirect evidence that may help explain it. On the one hand, RLS results in poor sleep quality, which, in turn, may lead to the development of anxiety and/or depression [44]; on the other hand, lower levels of monoamine neurotransmitters, such as dopamine, may be associated with increases in anxiety and depression [45].
In our study, PsA patients with RLS had poorer functioning and greater disease impact. We have not found data with which to compare these findings due to the scarcity of studies assessing RLS in patients with PsA.
In the analysis of baseline characteristics, patients with RLS were not significantly more likely to be smokers (current or former) than never smokers, nor was a statistically significant difference reached when we considered smoking exposure in pack-years. However, a recent meta-analysis found an association between smoking and RLS (OR = 1.46; 95% CI = 1.29–1.64). The mechanism underlying this association remains unknown but may be related to complications in blood circulation in people with smoking habits [34]. We found no associations with other variables studied that have been found to be associated with RLS in previous research (sex, age, BMI, and fibromyalgia) [35,36].
The most important limitation of this study is likely its cross-sectional nature. This limitation is common in studies of RLS and is attributable to the risk factors for this syndrome not yet being well defined. Indeed, we are not able to establish causal relationships. For future studies, we are currently following up with this group of patients to detect cases of incident restless legs syndrome. Nonetheless, based on our study, motivated by previous data suggesting that inflammation is a potential trigger for RLS, we can state that our results support this hypothesis; that is, the marked inflammation seen in polyarthritis may play a role in the development of RLS. On the other hand, we could speculate that, in patients with RLS, greater levels of skin problems, related to psoriasis, may be due to an abnormal sensory response caused by an alteration in dopamine pathways [43]. Another limitation of this study was that we did not examine the severity of RLS symptoms, meaning that we could not explore potential correlations with inflammation severity, nor did we include the SPI evolution time in the data. Finally, the inclusion of a control group without PsA would allow for comparison of RLS prevalence between patients and healthy individuals, strengthening the study’s conclusions.
The main strength of this study was that the diagnosis of RLS was made based on IRLSSG criteria and subsequently confirmed by a neurologist. The symptoms associated with RLS are common to various neurological diseases; hence, the need for a definitive diagnosis by a specialist [46]. Another strength is the inclusion of several variables (smoking habits, depression, and fatigue) that had not previously been associated with RLS in patients with PsA.
5. Conclusions
This cross-sectional study provides evidence that restless legs syndrome (RLS) is a relevant comorbidity in patients with psoriatic arthritis (PsA), with a prevalence of 20% in our cohort. The main findings can be summarised as follows:
Psoriatic skin symptoms, particularly itchiness, were independently associated with RLS, suggesting that sensory abnormalities—possibly related to dopaminergic pathway dysfunction—may amplify discomfort in patients with cutaneous psoriasis.
Polyarticular joint inflammation showed a marginal association with RLS, although this finding should be interpreted cautiously due to the borderline confidence interval and small effect size. Nevertheless, these results support the hypothesis that systemic inflammation may contribute to the development of RLS in PsA.
Author Contributions
Conceptualisation, E.T., L.L.-M. and C.M.; methodology, E.T., L.L.-M. and C.M.; data curation, E.T., C.C.C., D.M., C.H., S.C. and C.M.; formal analysis, E.T., J.M.-V., C.C.C., R.D.-P., S.C. and C.M.; validation, P.S.-C. and C.M.; writing—original draft, E.T., L.L.-M. and C.M.; supervision, E.T. and C.M.; writing—review and editing, E.T. and C.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of Salamanca University Hospital (PI 2023 03 1560–TFG).
Informed Consent Statement
Informed consent was obtained from all the subjects involved in this study. Version 1, 10 April 2023.
Data Availability Statement
The data presented in this study are available upon request from the corresponding author.
Acknowledgments
The authors thank the Spanish Foundation of Rheumatology for providing medical writing/editorial assistance during the preparation of this manuscript (Grant FERBT2022).
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Perez-Chada, L.M.; Elman, S.; Villa-Ruiz, C.; Armstrong, A.W.; Gottlieb, A.B.; Merola, J.F. Psoriatic arthritis: A comprehensive review for the dermatologist part I: Epidemiology, comorbidities, pathogenesis, and diagnosis. J. Am. Acad. Dermatol. 2025, 92, 969–982. [Google Scholar] [CrossRef]
- Toledano, E.; Hidalgo, C.; Gómez-Lechón, L.; Ibáñez, M.; Chacón, C.C.; Martín-Vallejo, J.; Pastor, S.; Montilla, C. Sleep quality in patients with psoriatic arthritis and its relationship with disease activity and comorbidities: A cross-sectional study. Sci. Rep. 2023, 13, 22927. [Google Scholar] [CrossRef]
- Klingelhoefer, L.; Bhattacharya, K.; Reichmann, H. Restless legs syndrome. Clin. Med. 2016, 16, 379–382. [Google Scholar] [CrossRef]
- George, R.J.; Kumar, R.; Achenbach, S.J.; Lovering, E.; Lennon, R.J.; Davis, J.M.; Carvalho, D.Z.; Crowson, C.S.; Myasoedova, E. Sleep disorders in rheumatoid arthritis: Incidence, risk factors and association with dementia. Semin. Arthritis Rheum. 2025, 73, 152722. [Google Scholar] [CrossRef]
- Padhan, P.; Maikap, D.; Pathak, M. Restless leg syndrome in rheumatic conditions: Its prevalence and risk factors, a meta-analysis. Int. J. Rheum. Dis. 2023, 26, 1111–1119. [Google Scholar] [CrossRef]
- Falup-Pecurariu, C.; Enache, A.; Duca, L.; Fotescu, C.; Falup-Pecurariu, O.; Monescu, V.; Diaconu, Ş.; Sirbu, C.A. Restless legs syndrome in systemic lupus erythematosus: A case-control study. Exp. Ther. Med. 2021, 22, 802. [Google Scholar] [CrossRef] [PubMed]
- Tekatas, A.; Pamuk, O.N. Increased frequency of restless leg syndrome in patients with ankylosing spondylitis. Int. J. Rheum. Dis. 2015, 18, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Sandikci, S.C.; Colak, S.; Aydoğan Baykara, R.; Öktem, A.; Cüre, E.; Omma, A.; Kucuk, A. Evaluation of restless legs syndrome and sleep disorders in patients with psoriatic arthritis. Z. Rheumatol. 2019, 78, 987–995. [Google Scholar] [CrossRef]
- Taylor, W.; Gladman, D.; Helliwell, P.; Marchesoni, A.; Mease, P.; Mielants, H. Classification criteria for psoriatic arthritis: Development of new criteria from a large international study. Arthritis Rheum. 2006, 54, 2665–2673. [Google Scholar] [CrossRef]
- Cetin Erdem, H.; Kara, H.; Ozcelik, O.; Donmez, L.; Eryilmaz, M.; Ozbey, G. Frequency, risk factors, and impacts on quality of life of the restless legs syndrome and side effects among antidepressant users in a tertiary hospital: An observational cross-sectional study. Int. Clin. Psychopharmacol. 2023, 38, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Kolla, B.P.; Mansukhani, M.P.; Bostwick, J.M. The influence of antidepressants on restless legs syndrome and periodic limb movements: A systematic review. Sleep Med. Rev. 2018, 38, 131–140. [Google Scholar] [CrossRef]
- Allen, R.P.; Picchietti, D.; Hening, W.A.; Trenkwalder, C.; Walters, A.S.; Montplaisi, J. Restless legs syndrome: Diagnostic criteria, special considerations, and epidemiology. A report from the restless legs syndrome diagnosis and epidemiology workshop at the National Institutes of Health. Sleep Med. 2003, 4, 101–119. [Google Scholar] [CrossRef]
- Jiménez Ruiz, C.A.; Barrueco Ferrero, M.; Solano Reina, S.; Torrecilla García, M.; Domínguez Grandal, F.; Díaz-Maroto Muñoz, J.L.; Alonso Moreno, J.; De La Cruz Amorós, E.; Abengozar Muela, R. Guidelines for a diagnostic and therapeutic approach to smoking addiction. A consensus report. Arch. Bronconeumol. 2003, 39, 35–41. [Google Scholar] [CrossRef]
- Sieper, J.; van der Heijde, D.; Landewé, R.; Brandt, J.; Burgos-Vagas, R.; Collantes-Estevez, E.; Dijkmans, B.; Dougados, M.; Khan, M.A.; Leirisalo-Repo, M.; et al. New criteria for inflammatory back pain in patients with chronic back pain: A real patient exercise by experts from the Assessment of SpondyloArthritis International Society (ASAS). Ann. Rheum. Dis. 2009, 68, 784–788. [Google Scholar] [CrossRef]
- van der Linden, S.; Valkenburg, H.A.; Cats, A. Evaluation of diagnostic criteria for ankylosing spondylitis. A proposal for modification of the New York criteria. Arthritis Rheum. 1984, 27, 361–368. [Google Scholar] [CrossRef]
- Her, M.; Kavanaugh, A. A review of disease activity measures for psoriatic arthritis: What is the best approach? Expert Rev. Clin. Immunol. 2014, 10, 1241–1254. [Google Scholar] [CrossRef] [PubMed]
- Heuft-Dorenbosch, L.; Spoorenberg, A.; van Tubergen, A.; Landewé, R.; van ver Tempel, H.; Mielants, H.; Dougados, M.; van der Heijde, D. Assessment of enthesitis in ankylosing spondylitis. Ann. Rheum. Dis. 2003, 62, 127–132. [Google Scholar] [CrossRef]
- Fredriksson, T.; Pettersson, U. Severe psoriasis-oral therapy with a new retinoid. Dermatologica 1978, 157, 238–244. [Google Scholar] [CrossRef]
- Chandran, V.; Bhella, S.; Schentag, C.; Gladman, D.D. Functional assessment of chronic illness therapy fatigue scale is valid in patients with psoriatic arthritis. Ann. Rheum. Dis. 2007, 66, 936–939. [Google Scholar] [CrossRef] [PubMed]
- Schoels, M.M.; Aletaha, D.; Alasti, F.; Smolen, J.S. Disease activity in psoriatic arthritis (PsA): Defining remission and treatment success using the DAPSA score. Ann. Rheum. Dis. 2016, 75, 811–818. [Google Scholar] [CrossRef] [PubMed]
- Lukas, C.; Landewé, R.; Sieper, J.; Dougados, M.; Davis, J.; Braun, J.; van der Linden, S.; van der Heijde, D. Assessment of Spondyloarthritis International Society. Development of an ASAS-endorsed disease activity score (ASDAS) in patients with ankylosing spondylitis. Ann. Rheum. Dis. 2009, 68, 18–24. [Google Scholar] [CrossRef]
- Fries, J.F.; Spitz, P.; Kraines, R.G.; Holman, H.R. Measurement of patient outcome in arthritis. Arthritis Rheum. 1980, 23, 137–145. [Google Scholar] [CrossRef]
- Calin, A.; Garrett, S.; Whitelock, H.; Kennedy, L.G.; O’Hea, J.; Mallorie, P.; Jenkinson, T. A new approach to defining functional ability in ankylosing spondylitis: The development of the Bath Ankylosing Spondylitis Functional Index. J. Rheumatol. 1994, 21, 2281–2285. [Google Scholar] [PubMed]
- Gossec, L.; de Wit, M.; Kiltz, U.; Braun, J.; Kalyoncu, U.; Scrivo, R.; Maccarone, M.; Carton, L.; Otsa, K.; Sooäär, I.; et al. A patient-derived and patient-reported outcome measure for assessing psoriatic arthritis: Elaboration and preliminary validation of the Psoriatic Arthritis Impact of Disease (PsAID) questionnaire, a 13-country EULAR initiative. Ann. Rheum. Dis. 2014, 73, 1012–1019. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Bastien, C.H.; Vallières, A.; Morin, C.M. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef] [PubMed]
- Garrow, J.S.; Webster, J. Quetelet’s index (W/H2) as a measure of fatness. Int. J. Obes. 1985, 9, 147–153. [Google Scholar]
- Arnold, L.M.; Bennett, R.M.; Crofford, L.J.; Dean, L.E.; Clauw, D.J.; Goldenberg, D.L.; Fitzcharles, M.A.; Paiva, E.S.; Staud, R.; Sarzi Puttini, P.; et al. AAPT Diagnostic Criteria for Fibromyalgia. J. Pain 2019, 20, 611–628. [Google Scholar] [CrossRef] [PubMed]
- Solak, B.; Aydín, B.; Yüksekal, G.; Yaldız, M. Restless legs syndrome in patients with psoriasis: Association with inflammation and sleep quality. Int. J. Dermatol. 2023, 62, 501–507. [Google Scholar] [CrossRef]
- Nowowiejska, J.; Baran, A.; Lewoc, M.; Grabowska, P.; Kaminski, T.W.; Flisiak, I. The Assessment of Risk and Predictors of Sleep Disorders in Patients with Psoriasis--A Questionnaire-Based Cross-Sectional Analysis. J. Clin. Med. 2021, 10, 664. [Google Scholar] [CrossRef]
- Dowsett, J.; Didriksen, M.; von Stemann, J.H.; Larsen, M.H.; Thørner, L.W.; Sørensen, E.; Erikstrup, C.; Pedersen, O.B.; Hansen, M.B.; Eugen-Olsen, J.; et al. Chronic inflammation markers and cytokine-specific autoantibodies in Danish blood donors with restless legs syndrome. Sci. Rep. 2022, 12, 1672. [Google Scholar] [CrossRef]
- Benediktsdottir, B.; Janson, C.; Lindberg, E.; Arnardóttir, E.S.; Olafsson, I.; Cook, E.; Thorarinsdottir, E.H.; Gislason, T. Prevalence of restless legs syndrome among adults in Iceland and Sweden: Lung function, comorbidity, ferritin, biomarkers and quality of life. Sleep Med. 2010, 11, 1043–1048. [Google Scholar] [CrossRef]
- Song, P.; Wu, J.; Cao, J.; Sun, W.; Li, X.; Zhou, T.; Shen, Y.; Tan, X.; Ye, X.; Yuan, C.; et al. The global and regional prevalence of restless legs syndrome among adults: A systematic review and modelling analysis. J. Glob. Health 2024, 14, 04113. [Google Scholar] [CrossRef] [PubMed]
- Batool-Anwar, S.; Li, Y.; De Vito, K.; Malhotra, A.; Winkelman, J.; Gao, X. Lifestyle factors and risk of restless legs syndrome: Prospective cohort study. J. Clin. Sleep Med. 2016, 12, 187–194. [Google Scholar] [CrossRef] [PubMed]
- AlHarbi, O.R.; Bahammam, A.; Olaish, A.H.; Azzam, N.A.; Aljebreen, A.A.; Almadi, M.A.; Alsaleh, S.A. Prevalence, severity and associated factors of restless leg syndrome in inflammatory bowel disease patients. Saudi J. Gastroenterol. 2021, 27, 348–354. [Google Scholar] [CrossRef]
- Lin, S.; Zhang, H.; Gao, T.; Zhong, F.; Sun, Y.; Cai, J.; Ma, A. The association between obesity and restless legs syndrome: A systemic review and meta-analysis of observational studies. J. Affect. Disord. 2018, 235, 384–391. [Google Scholar] [CrossRef] [PubMed]
- Stehlik, R.; Ulfberg, J.; Hedner, J.; Grote, L. High prevalence of restless legs syndrome among women with multi-site pain: A population-based study in Dalarna, Sweden. Eur. J. Pain 2014, 18, 1402–1409. [Google Scholar] [CrossRef]
- Peduzzi, P.; Concato, J.; Kemper, E.; Holford, T.R.; Feinstein, A.R. A simulation study of the number of events per variable in logistic regression analysis. J. Clin. Epidemiol. 1996, 49, 1373–1379. [Google Scholar] [CrossRef]
- Callis Duffin, K.; Wong, B.; Horn, E.J.; Krueger, G.G. Psoriatic arthritis is a strong predictor of sleep interference in patients with psoriasis. J. Am. Acad. Dermatol. 2009, 60, 604–608. [Google Scholar] [CrossRef]
- Uslu, F.I.; Demir, E.; Guler, E.M.; Kocyigit, A. Circulating levels of cytokines are increased in restless legs syndrome. Sleep Breath. 2020, 25, 1581–1585. [Google Scholar] [CrossRef]
- Shin, J.-W.; Lee, J.; Kim, H.; Lee, D.-H.; Baek, K.-H.; Sunwoo, J.-S.; Byun, J.-I.; Kim, T.-J.; Jun, J.-S.; Han, D.; et al. Bioinformatic analysis of proteomic data for iron, inflammation, and hypoxic pathways in restless legs syndrome. Sleep Med. 2024, 75, 448–455. [Google Scholar] [CrossRef]
- Alves, A.C.B.; Santos, N.S.; Santos, A.P.T.; da Panatta, G.; Speck, A.E.; Cunha, R.A.; Aguiar, A.S. Adenosine A(2A) and dopamine D(2) receptor interaction controls fatigue resistance. Front. Pharmacol. 2024, 15, 1390187. [Google Scholar] [CrossRef] [PubMed]
- Clemens, S. Restless legs syndrome: Revisiting the dopamine hypothesis from the spinal cord perspective. Neurology 2006, 67, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Qi, G.; Zhang, P.; Li, T.; Li, M.; Zhang, Q.; He, F.; Zhang, L.; Cai, H.; Lv, X.; Qiao, H.; et al. NAc-VTA circuit underlies emotional stress-induced anxiety-like behavior in the three-chamber vicarious social defeat stress mouse model. Nat. Commun. 2022, 13, 577. [Google Scholar] [CrossRef] [PubMed]
- Belujon, P.; Grace, A.A. Dopamine system dysregulation in major depressive disorders. Int. J. Neuropsychopharmacol. 2017, 20, 1036–1046. [Google Scholar] [CrossRef]
- Hening, W.A.; Allen, R.P.; Washburn, M.; Lesage, S.R.; Earley, C.J. The four diagnostic criteria for Restless Legs Syndrome are unable to exclude confounding conditions (“mimics”). Sleep Med. 2009, 10, 976–981. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).