
Laboratory Puzzle of Oxidative Stress, Parameters of Hemostasis and Inflammation in Hospitalized Patients with COVID-19
 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Determination of Redox Status
2.2.1. Blood Sampling
2.2.2. Measurements of Oxidative Stress Parameters
Superoxide Anion Radical (O2−) Determination
Hydrogen Peroxide (H2O2) Determination
Nitrite (NO2−) Determination
Determination of the Index of Lipid Peroxidation
2.2.3. Measurements of Antioxidant Parameters
Determination of Superoxide Dismutase (SOD) Activity
Determination of Catalase (CAT) Activity
Determination of Reduced Glutathione (GSH) Level
2.3. Determination of Hematological and Biochemical Parameters
2.4. Statistical Analysis
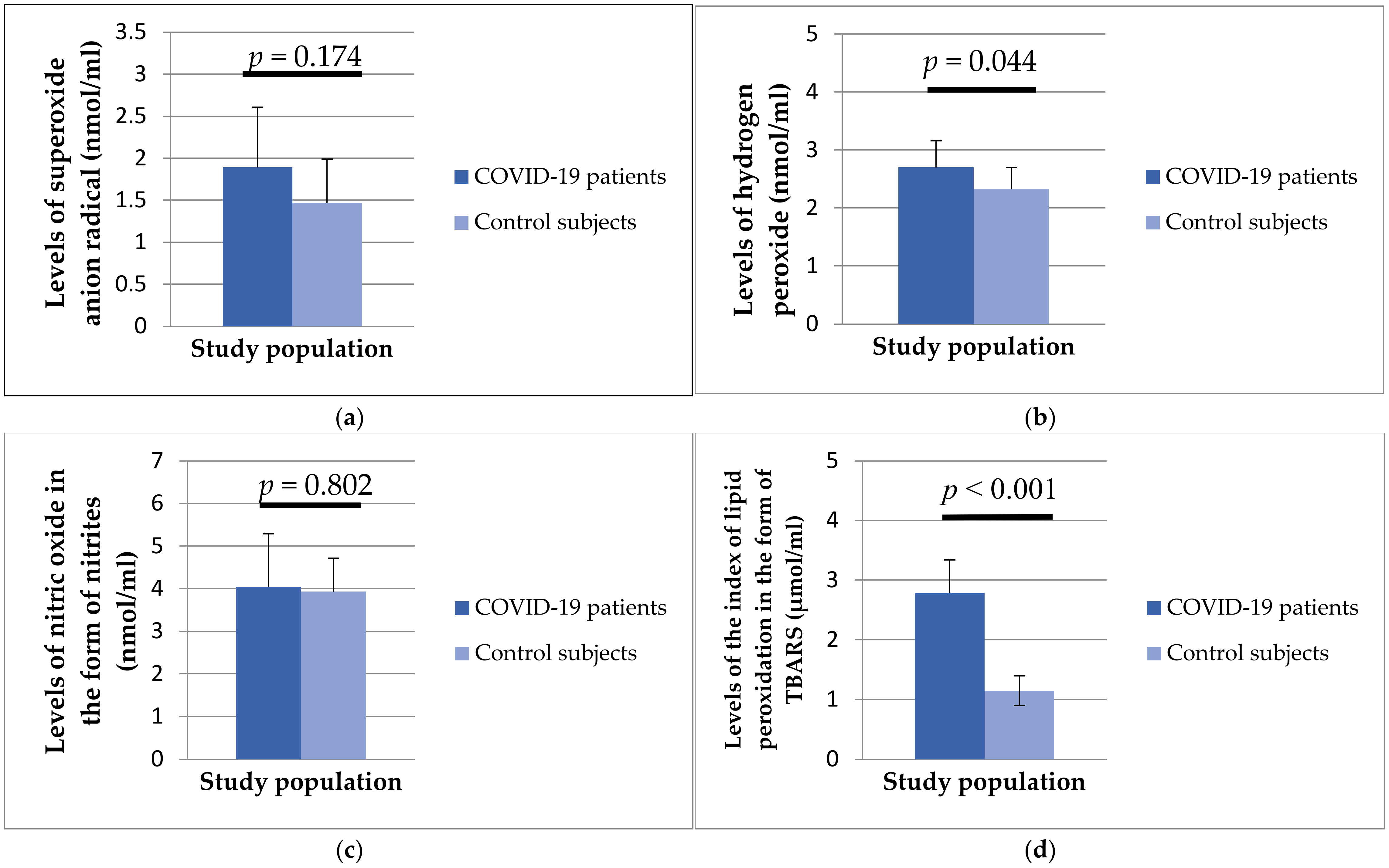
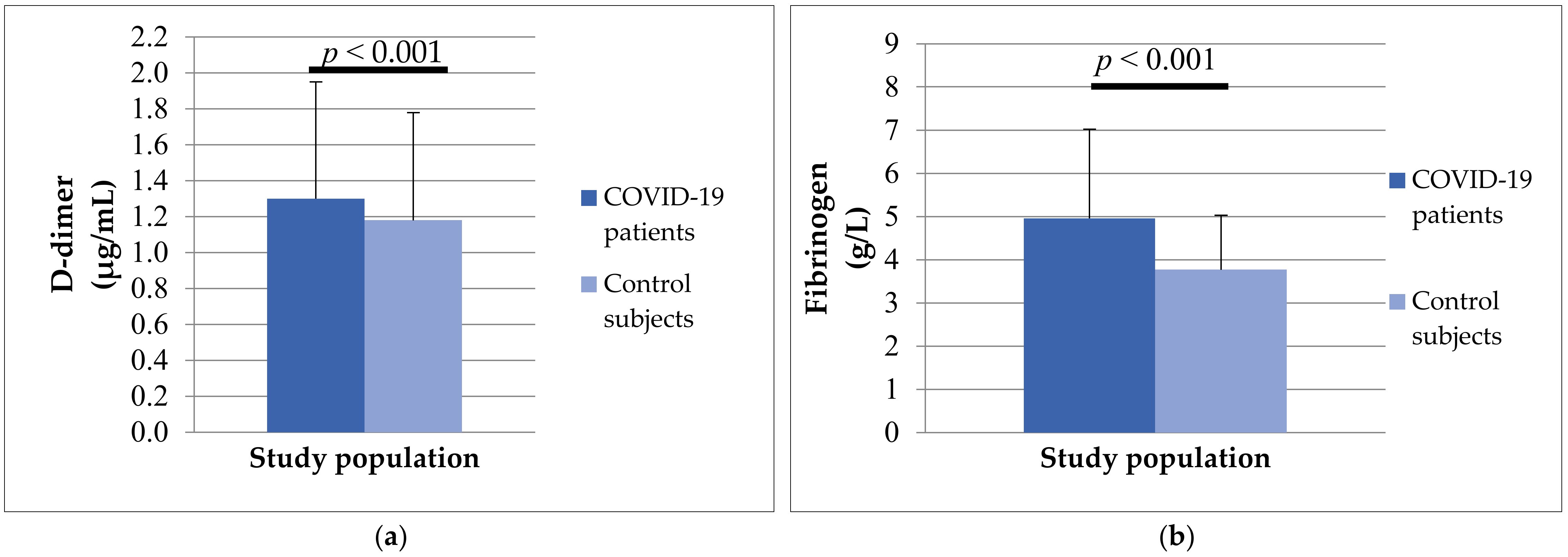
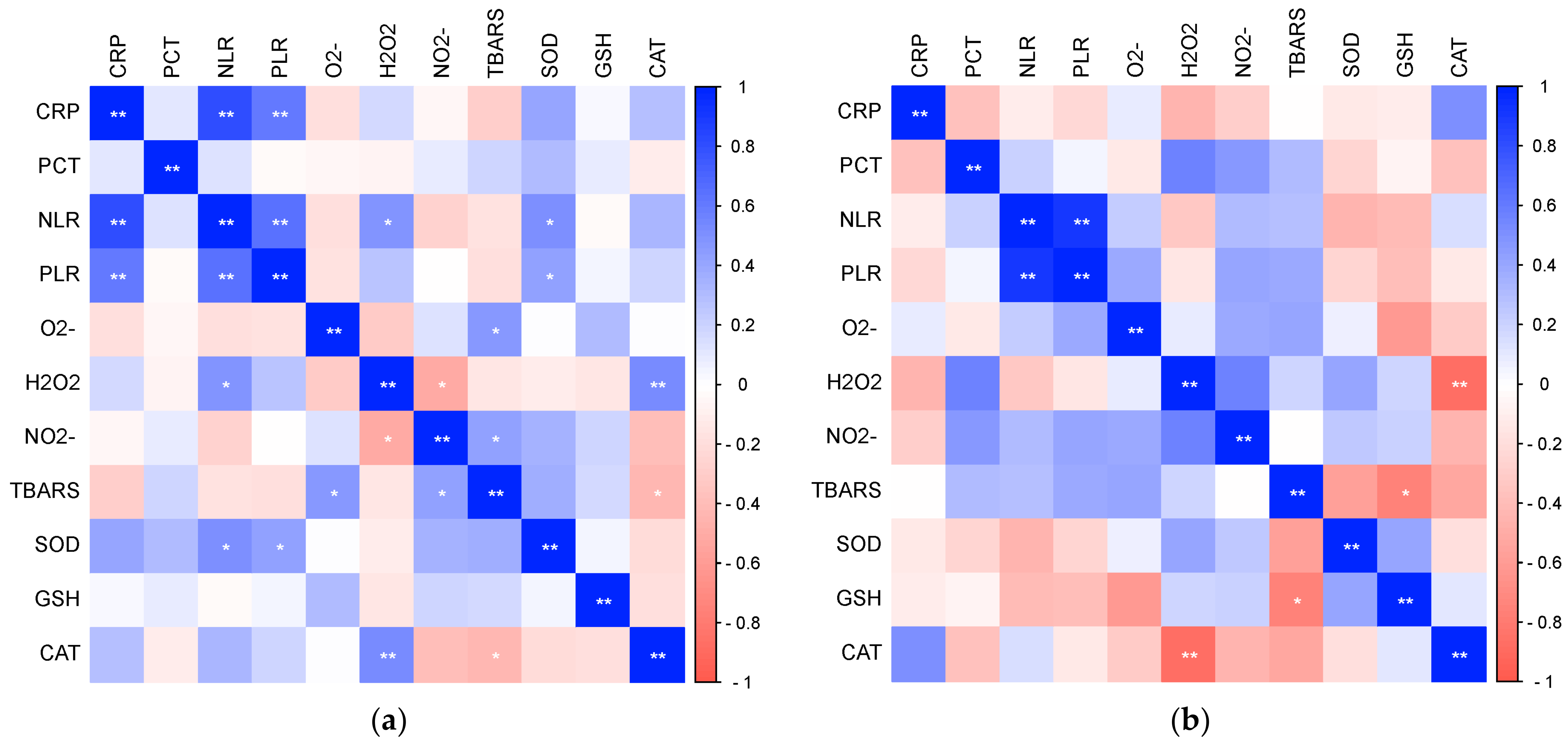
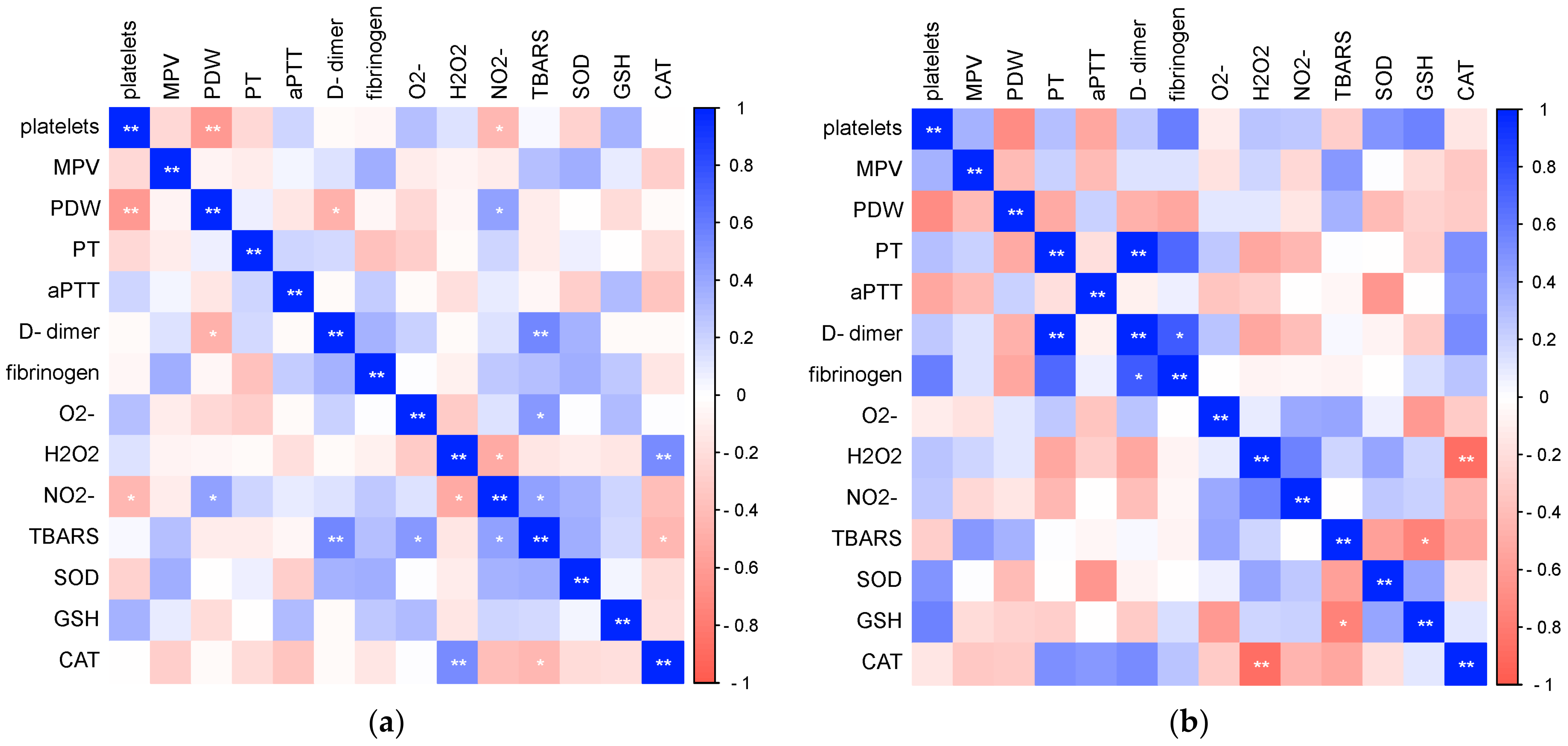
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Oh, K. Aberrant Cytokine Activity in the Host Immune Response to COVID-19 Leads to Cytokine Release Syndrome; Bio-Rad Bulletin: Philadelphia, PA, USA, 2020; p. 7335. [Google Scholar]
- WHO. Clinical Management of Severe Acute Respiratory Infection When Novel Coronavirus (2019-nCoV) Infection Is Suspected: Interim Guidance; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Yin, Y.; Wunderink, R.G. MERS, SARS and other coronaviruses as causes of pneumonia. Respirology 2018, 23, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.F.; Yuan, S.; Kok, K.H.; To, K.K.; Chu, H.; Yang, J.; Xing, F.; Liu, J.; Yip, C.C.; Poon, R.W.; et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: A study of a family cluster. Lancet 2020, 395, 514–523. [Google Scholar] [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72314 cases from the Chinese center for disease control and prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Tay, M.Z.; Poh, C.M.; Renia, L.; MacAry, P.A.; Ng, L.F.P. The trinity of COVID-19: Immunity, inflammation and intervention. Nat. Rev. Immunol. 2020, 20, 363–374. [Google Scholar] [CrossRef]
- Wu, J. Tackle the free radicals damage in COVID-19. Nitric Oxide 2020, 102, 39–41. [Google Scholar] [CrossRef]
- Nasi, A.; McArdle, S.; Gaudernack, G.; Westman, G.; Melief, C.; Rockberg, J.; Arens, R.; Kouretas, D.; Sjölin, J.; Mangsbo, S. Reactive oxygen species as an initiator of toxic innate immune responses in retort to SARS-CoV-2 in an ageing population, consider N-acetylcysteine as early therapeutic intervention. Toxicol. Rep. 2020, 7, 768–771. [Google Scholar] [CrossRef]
- Cecchini, R.; Cecchini, A.L. SARS-CoV-2 infection pathogenesis is related to oxidative stress as a response to aggression. Med. Hypotheses 2020, 143, 110102. [Google Scholar] [CrossRef]
- Beltrán-García, J.; Osca-Verdegal, R.; Pallardó, F.V.; Ferreres, J.; Rodríguez, M.; Mulet, S.; Sanchis-Gomar, F.; Carbonell, N.; García-Giménez, J.L. Oxidative Stress and Inflammation in COVID-19-Associated Sepsis: The Potential Role of Anti-Oxidant Therapy in Avoiding Disease Progression. Antioxidants 2020, 9, 936. [Google Scholar] [CrossRef]
- Iba, T.; Levy, J.H.; Levi, M.; Connors, J.M.; Thachil, J. Coagulopathy of coronavirus disease 2019. Crit. Care Med. 2020, 48, 1358–1364. [Google Scholar] [CrossRef] [PubMed]
- Manne, B.K.; Denorme, F.; Middleton, E.A.; Portier, I.; Rowley, J.W.; Stubben, C.; Petrey, A.C.; Tolley, N.D.; Guo, L.; Cody, M.; et al. Platelet gene expression and function in patients with COVID-19. Blood 2020, 136, 1317–1329. [Google Scholar] [CrossRef]
- Zaid, Y.; Puhm, F.; Allaeys, I.; Naya, A.; Oudghiri, M.; Khalki, L.; Limami, Y.; Zaid, N.; Sadki, K.; Ben El Haj, R.; et al. Platelets Can Associate with SARS-CoV-2 RNA and Are Hyperactivated in COVID-19. Circ. Res. 2020, 127, 1404–1418. [Google Scholar] [CrossRef]
- Long, H.; Nie, L.; Xiang, X.; Li, H.; Zhang, X.; Fu, X.; Ren, H.; Liu, W.; Wang, Q.; Wu, Q. D-Dimer and Prothrombin Time Are the Significant Indicators of Severe COVID-19 and Poor Prognosis. BioMed Res. Int. 2020, 2020, 6159720. [Google Scholar] [CrossRef]
- Miesbach, W.; Makris, M. COVID-19: Coagulopathy, Risk of Thrombosis, and the Rationale for Anticoagulation. Clin. Appl. Thromb. Hemost. 2020, 26, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Arachchillage, D.R.J.; Laffan, M. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J. Thromb. Haemst. 2020, 18, 1233–1234. [Google Scholar] [CrossRef] [PubMed]
- Ruan, Q.; Yang, K.; Wang, W.; Jiang, L.; Song, J. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020, 46, 846–848. [Google Scholar] [CrossRef]
- Guan, W.J.; Liang, W.H.; Zhao, Y.; Liang, H.R.; Chen, Z.S.; Li, Y.M.; Liu, X.Q.; Chen, R.C.; Tang, C.L.; Wang, T.; et al. Comorbidity and its impact on 1590 patients with COVID-19 in China: A nationwide analysis. Eur. Respir. J. 2020, 55, 2000547. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Laboratory Testing Strategy Recommendations for COVID-19: Interim Guidance; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Mihaljevic, O.; Zivancevic, S.S.; Jovanovic, D.; Drakulic, S.M.; Vukajlovic, J.T.; Markovic, A.; Pirkovic, M.S.; Srejovic, I.; Jakovljevic, V.; Milosevic, D.O. Oxidative stress and DNA damage in critically ill patients with sepsis. Mutat. Res. Genet. Toxicol. Environ. Mutagen. 2023, 889, 503655. [Google Scholar] [CrossRef]
- Alamdari, D.H.; Moghaddam, A.B.; Amini, S.; Keramati, M.R.; Zarmehri, A.M.; Alamdari, A.H.; Damsaz, M.; Banpour, H.; Yarahmadi, A.; Koliakos, G. Application of methylene blue-vitamin C-N-acetyl cysteine for treatment of critically ill COVID-19 patients, report of a phase-I clinical trial. Eur. J. Pharmacol. 2020, 885, 173494. [Google Scholar] [CrossRef]
- Suhail, S.; Zajac, J.; Fossum, C.; Lowater, H.; McCracken, C.; Severson, N.; Laatsch, B.; Narkiewicz-Jodko, A.; Johnson, B.; Liebau, J.; et al. Role of oxidative stress on SARS-CoV (SARS) and SARS-CoV-2 (COVID-19) infection: A review. Protein J. 2020, 39, 644–656. [Google Scholar] [CrossRef]
- Tsermpini, E.E.; Glamočlija, U.; Ulucan-Karnak, F.; Redenšek Trampuž, S.; Dolžan, V. Molecular Mechanisms Related to Responses to Oxidative Stress and Antioxidative Therapies in COVID-19: A Systematic Review. Antioxidants 2022, 11, 1609. [Google Scholar] [CrossRef]
- Bastin, A.; Abbasi, F.; Roustaei, N.; Abdesheikhi, J.; Karami, H.; Gholamnezhad, M.; Eftekhari, M.; Doustimotlagh, A. Severity of oxidative stress as a hallmark in COVID-19 patients. Eur. J. Med. Res. 2023, 28, 558. [Google Scholar] [CrossRef]
- Lage, S.L.; Amaral, E.P.; Hilligan, L.; Laidlaw, E.; Rupert, A.; Namasivayan, S.; Rocco, J.; Galindo, F.; Kellogg, A.; Kumar, P.; et al. Persistent Oxidative Stress and Inflammasome Activation in CD14 high CD16− Monocytes from COVID-19 Patients. Front. Immunol. 2022, 12, 799558. [Google Scholar] [CrossRef] [PubMed]
- Yaghoubi, N.; Youssefi, M.; Jabbari Azad, F.; Farzad, F.; Yavari, Z.; Zahedi Avval, F. Total antioxidant capacity as a marker of severity of COVID-19 infection: Possible prognostic and therapeutic clinical application. J. Med. Virol. 2022, 94, 1558–1565. [Google Scholar] [CrossRef] [PubMed]
- Saberi-Movahed, F.; Mohammadifard, M.; Mehrpooya, A.; Rezaei-Ravari, M.; Berahmand, K.; Rostami, M.; Karami, S.; Najafzadeh, M.; Hajinezhad, D.; Jamshidi, M.; et al. Decoding Clinical Biomarker Space of COVID-19: Exploring Matrix Factorization-based Feature Selection Methods. Comput. Biol. Med. 2022, 146, 105426. [Google Scholar] [CrossRef]
- Georgieva, E.; Ananiev, J.; Yovchev, Y.; Arabadzhiev, G.; Abrashev, H.; Abrashev, D.; Atanasov, V.; Kostandieva, R.; Mitev, M.; Petkova-Parlapanska, K.; et al. COVID-19 Complications: Oxidative Stress, Inflammation, and Mitochondrial and Endothelial Dysfunction. Int. J. Mol. Sci. 2023, 24, 14876. [Google Scholar] [CrossRef] [PubMed]
- Laforge, M.; Elbim, C.; Frère, C.; Hémadi, M.; Massaad, C.; Nuss, P.; Benoliel, J.; Becker, C. Tissue damage from neutrophil-induced oxidative stress in COVID-19. Nat. Rev. Immunol. 2020, 20, 515–516. [Google Scholar] [CrossRef]
- Aydınyılmaz, F.; Aksakal, E.; Pamukcu, H.E.; Aydemir, S.; Doğan, R.; Sarac, I.; Aydın, S.Ş.; Kalkan, K.; Gülcü, O.; Tanboğa, İ.H. Significance of MPV, RDW and PDW with the Severity and Mortality of COVID-19 and Effects of Acetylsalicylic Acid Use. Clin. Appl. Thromb./Hemost. 2021, 27, 10760296211048808. [Google Scholar] [CrossRef] [PubMed]
- Ligi, D.; Della Franca, C.; Notarte, K.I.; Goldrich, N.; Kavteladze, D.; Henry, B.M.; Mannello, F. Platelet distribution width (PDW) as a significant correlate of COVID-19 infection severity and mortality. Clin. Chem. Lab. Med. (CCLM) 2024, 62, 385–395. [Google Scholar] [CrossRef]
- Leffondre, K.; Abrahamowicz, M.; Regeasse, A.; Hawker, G.A.; Badley, E.M.; Belzile, E. Statistical measures were proposed for identifying longitudinal patterns of change in quantitative health indicators. J. Clin. Epidemiol. 2004, 57, 1049–1062. [Google Scholar] [CrossRef]
- Hottz, E.D.; Azevedo-Quintanilha, I.G.; Palhinha, L.; Teixeira, L.; Barreto, E.A.; Pão, C.R.; Righy, C.; Franco, S.; Souza, T.M.; Kurtz, P.; et al. Platelet activation and platelet-monocyte aggregate formation trigger tissue factor expression in patients with severe COVID-19. Blood 2020, 36, 1330–1341. [Google Scholar] [CrossRef]
- Şahin, M.; Duru, N.S.; Elevli, M.; Civilibal, M. Assessment of platelet parameters in children with pneumonia. J. Pediatr. Inf. 2017, 11, e106–e112. [Google Scholar] [CrossRef]
- Aggarwal, M.; Dass, J.; Mahapatra, M. Hemostatic Abnormalities in COVID-19: An Update. Indian J. Hematol. Blood Transf. 2020, 36, 616–626. [Google Scholar] [CrossRef] [PubMed]
- Panigada, M.; Bottino, N.; Tagliabue, P.; Grasselli, G.; Novembrino, C.; Chantarangkul, V.; Pesenti, A.; Peyvandi, F.; Tripodi, A. Hypercoagulability of COVID-19 patients in intensive care unit: A report of thromboelastography findings and other parameters of hemostasis. J. Thromb. Haemost. 2020, 18, 1738–1742. [Google Scholar] [CrossRef] [PubMed]
- Zátroch, I.; Smudla, A.; Babik, B.; Tánczos, K.; Kóbori, L.; Szabó, Z.; Fazakas, J. Procoagulation, hypercoagulation and fibrinolytic “shut down” detected with ClotPro® viscoelastic tests in COVID-19 patients. Orvosi Hetil. 2020, 161, 899–907. [Google Scholar] [CrossRef] [PubMed]
- Bonaventura, A.; Vecchié, A.; Dagna, L.; Martinod, K.; Dixon, D.L.; Van Tassell, B.W.; Dentali, F.; Montecucco, F.; Massberg, S.; Levi, M.; et al. Endothelial dysfunction and immunothrombosis as key pathogenic mechanisms in COVID-19. Nat. Rev. Immunol. 2021, 21, 319–329. [Google Scholar] [CrossRef]
- Pelle, M.C.; Zaffina, I.; Lucà, S.; Forte, V.; Trapanese, V.; Melina, M.; Giofrè, F.; Arturi, F. Endothelial Dysfunction in COVID-19: Potential Mechanisms and Possible Therapeutic Options. Life 2022, 12, 1605. [Google Scholar] [CrossRef]
- O’Sullivan, J.M.; Gonagle, D.M.; Ward, S.E.; Preston, R.J.S.; O’Donnell, J.S. Endothelial cells orchestrate COVID-19 coagulopathy. Lancet Haematol. 2020, 7, 553–555. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| COVID-19 Patients n = 105 | Control Subjects n = 65 | |||
|---|---|---|---|---|
| Gender | male | 65 (61.9%) | 42 (64.6%) | |
| females | 40 (38.1%) | 23 (35.4%) | ||
| Age (mean ± SD) | 59.6 ± 14.78 | 58.91 ± 11.71 | ||
| Duration of hospitalization | 12.5 ± 7.9 | - | ||
| Comorbidities | Diabetes mellitus type II | 27 (25.7%) | - | |
| Hypertension | 34 (32.4%) | - | ||
| COPD | 15 (14.3%) | - | ||
| Parameter | COVID-19 Patients | Control Subjects | Significance * | ||
|---|---|---|---|---|---|
| Mean ± SD | Min–Max | Mean ± SD | Min–Max | ||
| Leukocyte (×109/L) | 9.66 ± 4.35 | 2.98–26.84 | 7.24 ± 1.53 | 4.80–9.90 | p < 0.001 |
| Neutrophils (×109/L) | 7.12 ± 4.12 | 1.44–25.02 | 4.60 ± 1.40 | 2.15–7.89 | p < 0.001 |
| Lymphocytes (×109/L) | 1.6 ± 0.97 | 0.21–4.64 | 1.97 ± 0.60 | 0.70–3.30 | p = 0.007 |
| Erythrocytes (×1012/L) | 4.41 ± 0.71 | 2.37–6.18 | 4.47 ± 0.45 | 3.67–5.70 | p = 0.080 |
| Hemoglobin (g/L) | 129.05 ± 24.39 | 73–179 | 141.88 ± 10.41 | 188–167 | p < 0.001 |
| Hematocrit (L/L) | 0.39 ± 0.07 | 0.23–0.54 | 0.43 ± 0.035 | 0.35–0.50 | p < 0.001 |
| Platelets (×109/L) | 250.75 ± 83.52 | 54–482 | 240.16 ± 64.26 | 151–401 | p = 0.463 |
| MPV (fl) | 7.41 ± 1.51 | 6.90–13.20 | 8.66 ± 0.71 | 7.40–10.30 | p < 0.001 |
| PDW (ratio) | 16.31 ± 2.20 | 9.30–21.70 | 16.32 ± 0.60 | 14.50–17.10 | p = 0.002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Djordjevic, J.; Ignjatovic, V.; Vukomanovic, V.; Vuleta, K.; Ilic, N.; Slovic, Z.; Stanojevic Pirkovic, M.; Mihaljevic, O. Laboratory Puzzle of Oxidative Stress, Parameters of Hemostasis and Inflammation in Hospitalized Patients with COVID-19. Biomedicines 2024, 12, 636. https://doi.org/10.3390/biomedicines12030636
Djordjevic J, Ignjatovic V, Vukomanovic V, Vuleta K, Ilic N, Slovic Z, Stanojevic Pirkovic M, Mihaljevic O. Laboratory Puzzle of Oxidative Stress, Parameters of Hemostasis and Inflammation in Hospitalized Patients with COVID-19. Biomedicines. 2024; 12(3):636. https://doi.org/10.3390/biomedicines12030636
Chicago/Turabian StyleDjordjevic, Jelena, Vesna Ignjatovic, Vladimir Vukomanovic, Katarina Vuleta, Nevenka Ilic, Zivana Slovic, Marijana Stanojevic Pirkovic, and Olgica Mihaljevic. 2024. "Laboratory Puzzle of Oxidative Stress, Parameters of Hemostasis and Inflammation in Hospitalized Patients with COVID-19" Biomedicines 12, no. 3: 636. https://doi.org/10.3390/biomedicines12030636
APA StyleDjordjevic, J., Ignjatovic, V., Vukomanovic, V., Vuleta, K., Ilic, N., Slovic, Z., Stanojevic Pirkovic, M., & Mihaljevic, O. (2024). Laboratory Puzzle of Oxidative Stress, Parameters of Hemostasis and Inflammation in Hospitalized Patients with COVID-19. Biomedicines, 12(3), 636. https://doi.org/10.3390/biomedicines12030636