
An Italian Real-World Study Highlights the Importance of Some Clinicopathological Characteristics Useful in Identifying Metastatic Breast Cancer Patients Resistant to CDK4/6 Inhibitors and Hormone Therapy

 , , , , , ,
, , , , , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Source and Patient Selection
2.2.1. Inclusion Criteria
2.2.2. Exclusion Criteria
3. Statistical Methods
4. Results
4.1. Baseline Characteristics
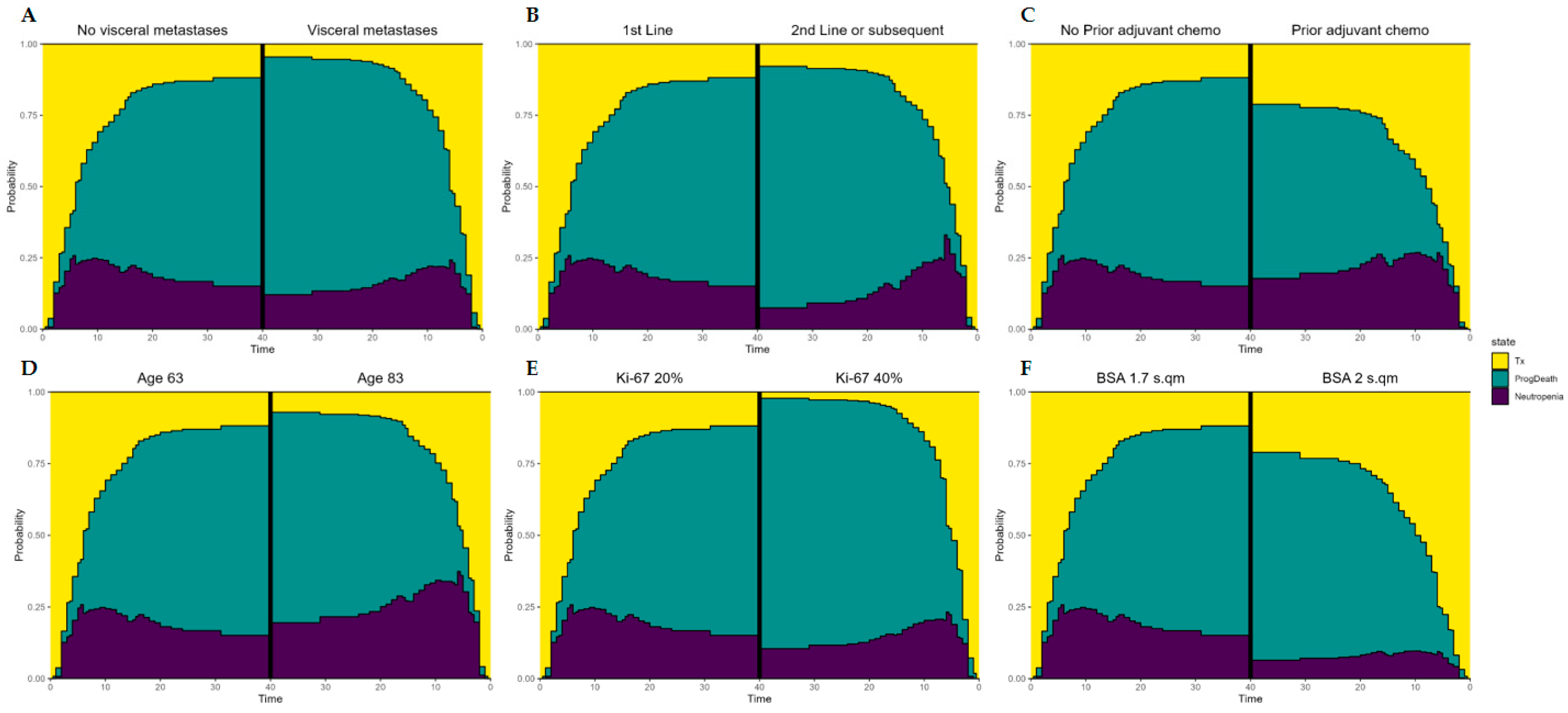
4.2. Role of Clinicopathological Characteristics concerning the Progression
5. Discussion
Clinical and Practical Aspects of the Study
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef]
- Osborne, C.K.; Schiff, R. Mechanisms of endocrine resistance in breast cancer. Annu. Rev. Med. 2011, 62, 233–247. [Google Scholar] [CrossRef]
- AlFakeeh, A.; Brezden-Masley, C. Overcoming endocrine resistance in hormone receptor-positive breast cancer. Curr. Oncol. 2018, 25, S18–S27. [Google Scholar] [CrossRef] [PubMed]
- Riggins, R.B.; Schrecengost, R.S.; Guerrero, M.S.; Bouton, A.H. Pathways to tamoxifen resistance. Cancer Lett. 2007, 256, 1–24. [Google Scholar] [CrossRef]
- Ha, M.J.; Singareeka Raghavendra, A.; Kettner, N.M.; Qiao, W.; Damodaran, S.; Layman, R.M.; Hunt, K.K.; Shen, Y.; Tripathy, D.; Keyomarsi, K. Palbociclib plus endocrine therapy significantly enhances overall survival of HR+/HER2− metastatic breast cancer patients compared to endocrine therapy alone in the second-line setting: A large institutional study. Int. J. Cancer 2022, 150, 2025–2037. [Google Scholar] [CrossRef] [PubMed]
- Lei, J.T.; Anurag, M.; Haricharan, S.; Gou, X.; Ellis, M.J. Endocrine therapy resistance: New insights. Breast 2019, 48 (Suppl. S1), S26–S30. [Google Scholar] [CrossRef] [PubMed]
- Haricharan, S.; Punturi, N.; Singh, P.; Holloway, K.R.; Anurag, M.; Schmelz, J.; Schmidt, C.; Lei, J.T.; Suman, V.; Hunt, K.; et al. Loss of MutL disrupts CHK2-Dependent cell-cycle control through CDK4/6 to promote intrinsic endocrine therapy resistance in primary breast cancer. Cancer Discov. 2017, 7, 1168–1183. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Huo, X.; Zhao, F.; Ren, D.; Ahmad, R.; Yuan, X.; Du, F.; Zhao, J. Association of Cyclin-Dependent Kinases 4 and 6 Inhibitors with Survival in Patients with Hormone Receptor-Positive Metastatic Breast Cancer: A Systematic Review and Meta-analysis. JAMA Netw. Open 2020, 3, e2020312. [Google Scholar] [CrossRef] [PubMed]
- Wander, S.A.; Han, H.S.; Zangardi, M.L.; Niemierko, A.; Mariotti, V.; Kim, L.S.L.; Xi, J.; Pandey, A.; Dunne, S.; Nasrazadani, A.; et al. Clinical Outcomes with Abemaciclib after Prior CDK4/6 Inhibitor Progression in Breast Cancer: A Multicenter Experience. J. Natl. Compr. Cancer Netw. 2021, 24, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Spring, L.M.; Wander, S.A.; Zangardi, M.; Bardia, A. CDK 4/6 Inhibitors in Breast Cancer: Current Controversies and Future Directions. Curr. Oncol. Rep. 2019, 21, 25. [Google Scholar] [CrossRef]
- McCartney, A.; Migliaccio, I.; Bonechi, M.; Biagioni, C.; Romagnoli, D.; De Luca, F.; Galardi, F.; Risi, E.; De Santo, I.; Benelli, M.; et al. Mechanisms of Resistance to CDK4/6 Inhibitors: Potential Implications and Biomarkers for Clinical Practice. Front. Oncol. 2019, 9, 666. [Google Scholar] [CrossRef] [PubMed]
- Asghar, U.S.; Kanani, R.; Roylance, R.; Mittnacht, S. Systematic Review of Molecular Biomarkers Predictive of Resistance to CDK4/6 Inhibition in Metastatic Breast Cancer. JCO Precis. Oncol. 2022, 6, e2100002. [Google Scholar] [CrossRef] [PubMed]
- Mavratzas, A.; Marmé, F. Treatment of Luminal Metastatic Breast Cancer beyond CDK4/6 Inhibition: Is There a Standard of Care in Clinical Practice? Breast Care 2021, 16, 115–128. [Google Scholar] [CrossRef] [PubMed]
- O’Leary, B.; Cutts, R.J.; Liu, Y.; Hrebien, S.; Huang, X.; Fenwick, K.; André, F.; Loibl, S.; Loi, S.; Garcia-Murillas, I.; et al. The Genetic Landscape and Clonal Evolution of Breast Cancer Resistance to Palbociclib plus Fulvestrant in the PALOMA-3 Trial. Cancer Discov. 2018, 8, 1390–1403. [Google Scholar] [CrossRef] [PubMed]
- Condorelli, R.; Spring, L.; O’Shaughnessy, J.; Lacroix, L.; Bailleux, C.; Scott, V.; Dubois, J.; Nagy, R.J.; Lanman, R.B.; Iafrate, A.J.; et al. Polyclonal RB1 mutations and acquired resistance to CDK 4/6 inhibitors in patients with metastatic breast cancer. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2018, 29, 640–645. [Google Scholar] [CrossRef] [PubMed]
- Finn, R.S.; Liu, Y.; Zhu, Z.; Martin, M.; Rugo, H.S.; Diéras, V.; Im, S.-A.; Gelmon, K.A.; Harbeck, N.; Lu, D.R.; et al. Biomarker Analyses of Response to Cyclin-Dependent Kinase 4/6 Inhibition and Endocrine Therapy in Women with Treatment-Naïve Metastatic Breast Cancer. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2020, 26, 110–121. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.H.; Kim, T.-Y.; Kim, G.M.; Kang, S.Y.; Park, I.H.; Kim, J.H.; Lee, K.E.; Ahn, H.K.; Lee, M.H.; Kim, H.-J.; et al. Palbociclib plus exemestane with gonadotropin-releasing hormone agonist versus capecitabine in premenopausal women with hormone receptor-positive, HER2-negative metastatic breast cancer (KCSG-BR15-10): A multicentre, open-label, randomized, phase 2 trial. Lancet Oncol. 2019, 20, 1750–1759. [Google Scholar] [CrossRef]
- Gomatou, G.; Trontzas, I.; Ioannou, S.; Drizou, M.; Syrigos, N.; Kotteas, E. Mechanisms of resistance to cyclin-dependent kinase 4/6 inhibitors. Mol. Biol. Rep. 2021, 48, 915–925. [Google Scholar] [CrossRef]
- Dustin, D.; Gu, G.; Fuqua, S.A. ESR1 Mutations in Breast Cancer. Cancer 2019, 125, 3714–3728. [Google Scholar] [CrossRef]
- Ahn, S.G.; Bae, S.J.; Kim, Y.; Ji, J.H.; Chu, C.; Kim, D.; Lee, J.; Cha, Y.J.; Lee, K.-A.; Jeong, J. Primary endocrine resistance of ER+ breast cancer with ESR1 mutations interrogated by droplet digital PCR. NPJ Breast Cancer 2022, 8, 58. [Google Scholar] [CrossRef]
- Vasan, N.; Toska, E.; Scaltriti, M. Overview of the relevance of PI3K pathway in HR-positive breast cancer. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2019, 30, x3–x11. [Google Scholar] [CrossRef]
- Rugo, H.S. Addressing unmet need in the management of patients with ER+/HER2-, ESR1-mutated metastatic breast cancer: Clinician’s perspective. Clin. Adv. Hematol. Oncol. 2023, 21, 623–632. [Google Scholar]
- Bravaccini, S.; Roncadori, A.; Balzi, W.; Martinelli, G.; Montella, M.T.; Palleschi, M.; Maltoni, R. Which are the clinicopathological characteristics useful to define the metastatic breast cancer patients that will respond to CDK4/6 inhibitors and hormone therapy? An Italian real-world experience. In Proceedings of the American Association for Cancer Research Annual Meeting, Orlando, FL, USA, 14–19 April 2023; AACR: Philadelphia, PA, USA. [Google Scholar]
- Meira-Machado, L.; de Uña-Alvarez, J.; Cadarso-Suárez, C.; Andersen, P.K. Multi-state models for the analysis of time-to-event data. Stat. Methods Med. Res. 2009, 18, 195–222. [Google Scholar] [CrossRef] [PubMed]
- Hunter, R.J.; Park, J.; Asprer, K.J.; Doan, A.H. Updated Review Article: Cyclin-Dependent Kinase 4/6 Inhibitor Impact, FDA Approval, and Resistance Pathways. J. Pharm. Technol. 2023, 39, 298–308. [Google Scholar] [CrossRef] [PubMed]
- Cristofanilli, M.; Rugo, H.S.; Im, S.A.; Slamon, D.J.; Harbeck, N.; Bondarenko, I.; Masuda, N.; Colleoni, M.; DeMichele, A.; Loi, S.; et al. Overall Survival with Palbociclib and Fulvestrant in Women with HR+/HER2− ABC: Updated Exploratory Analyses of PALOMA-3, a Double-blind, Phase III Randomized Study. Clin. Cancer Res. 2022, 28, 3433–3442. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Zou, W.; Zhang, J.; Zhang, Y.; Xu, Q.; Li, S.; Chen, C. Mechanisms of CDK4/6 inhibitor resistance in luminal breast cancer. Front. Pharmacol. 2020, 11, 580251. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Razavi, P.; Li, Q.; Toy, W.; Liu, B.; Ping, C.; Hsieh, W.; Sanchez-Vega, F.; Brown, D.N.; Da Cruz Paula, A.F.; et al. Loss of the FAT1 tumor suppressor promotes resistance to CDK4/6 inhibitors via the hippo pathway. Cancer Cell 2018, 34, 893–905.e8. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.J.; Cheng, J.; Bloomquist, E.; Sanchez, J.; Wedam, S.B.; Singh, H.; Amiri-Kordestani, L.; Ibrahim, A.; Sridhara, R.; Goldberg, K.B.; et al. CDK4/6 inhibitor treatment for patients with hormone receptor-positive, HER2-negative, advanced or metastatic breast cancer: A US Food and Drug Administration pooled analysis. Lancet Oncol. 2020, 21, 250–260. [Google Scholar] [CrossRef] [PubMed]
- Cordani, N.; Mologni, L.; Piazza, R.; Tettamanti, P.; Cogliati, V.; Mauri, M.; Villa, M.; Malighetti, F.; Di Bella, C.; Jaconi, M.; et al. TWIST1 Upregulation Is a Potential Target for Reversing Resistance to the CDK4/6 Inhibitor in Metastatic Luminal Breast Cancer Cells. Int. J. Mol. Sci. 2023, 24, 16294. [Google Scholar] [CrossRef]
- Shikanai, A.; Horimoto, Y.; Ishizuka, Y.; Uomori, T.; Nakai, K.; Arakawa, A.; Saito, M. Clinicopathological Features Related to the Efficacy of CDK4/6 Inhibitor-Based Treatments in Metastatic Breast Cancer. Breast Cancer 2022, 16, 11782234211065148. [Google Scholar] [CrossRef]
- Palleschi, M.; Maltoni, R.; Ravaioli, S.; Vagheggini, A.; Mannozzi, F.; Fanini, F.; Pirini, F.; Tumedei, M.M.; Barzotti, E.; Cecconetto, L.; et al. Ki67 and PR in Patients Treated with CDK4/6 Inhibitors: A Real-World Experience. Diagnostics 2020, 10, 573. [Google Scholar] [CrossRef] [PubMed]
- Toi, M.; Boyle, F.; Im, Y.H.; Reinisch, M.; Molthrop, D.; Jiang, Z.; Wei, R.; Sapunar, F.; Grimes, B.R.; Nabinger, S.C.; et al. Adjuvant Abemaciclib Combined with Endocrine Therapy: Efficacy Results in monarchE Cohort 1. Oncologist 2023, 28, e77–e81. [Google Scholar] [CrossRef] [PubMed]
- Kimura, M.; Usami, E.; Yoshimura, T. Association between severe neutropenia and progression-free survival in patients with advanced or recurrent breast cancer treated with palbociclib. Pharmazie 2020, 75, 662–665. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Baseline Characteristics | (n = 177) |
|---|---|
| Age | |
| Median (min/max) | 63 (38–92) |
| ≤65 y | 103 (58.2%) |
| >65 y | 74 (41.8%) |
| Menopausal status | |
| Postmenopause | 152 (85.9%) |
| Pre/perimenopause | 25 (14.1%) |
| BMI | |
| ≤25 | 90 (50.8%) |
| >25 | 87 (49.2%) |
| Previous hormonal therapy (HT) | |
| No | 42 (23.7%) |
| Yes | 135 (76.3%) |
| Prior aromatase inhibitor (from the total number of patients receiving HT) | |
| No | 33 (24.4%) |
| Yes | 102 (75.6%) |
| Prior adjuvant chemotherapy | |
| No | 106 (59.9%) |
| Yes | 71 (40.1%) |
| ER status (positive if the value ≥ 10%) | |
| Positive | 175 (98.9%) |
| Negative | 2 (1.1%) |
| PgR status (positive if the value ≥ 10%) | |
| Positive | 139 (78.5%) |
| Negative | 38 (21.5%) |
| Previous lines | |
| First line | 95 (53.7%) |
| ≥2 lines | 82 (46.3%) |
| Metastatic site | |
| Bone only | 45 (25.4%) |
| Visceral | 67 (37.9%) |
| Other | 65 (36.7%) |
| Organs involved, N° | |
| 1 | 75 (42.4%) |
| 2 | 73 (41.2%) |
| ≥3 | 29 (16.4%) |
| Neutropenia | |
| Absent | 79 (44.6%) |
| Present | 98 (55.4%) |
| Ki67 (%) | |
| Median (min/max) | 20 (0–80) |
| <20% | 85 (48.0%) |
| ≥20% | 92 (52.0%) |
| HT | |
| Fulvestrant | 111 (62.7%) |
| Letrozole | 66 (37.3%) |
| Grading | |
| 1 | 3 (1.9%) |
| 2 | 98 (62.8%) |
| 3 | 55 (35.3%) |
| Missing/not known | 21 |
| Parameter | Coefficient | CI-Low | CI-High | p-Value | |
|---|---|---|---|---|---|
| Treatment > Neutropenia | Previous lines (2L+) | 1.455 | 0.933 | 2.269 | 0.0982 |
| Baseline BSA | 0.026 | 0.005 | 0.123 | <0.0001 | |
| Age | 1.023 | 1.003 | 1.043 | 0.0229 | |
| Treatment > progression/death | Ki67 (%) | 1.040 | 1.022 | 1.058 | <0.0001 |
| Visceral metastases | 1.680 | 1.022 | 2.762 | 0.0408 | |
| Prior adjuvant chemotherapy | 0.565 | 0.335 | 0.954 | 0.0326 | |
| Neutropenia > progression/death | Previous lines (2L+) | 1.893 | 1.059 | 3.384 | 0.0312 |
| Neutropenia | 2.311 | 1.109 | 4.815 | 0.0253 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maltoni, R.; Roncadori, A.; Balzi, W.; Mazza, M.; Nicolini, F.; Palleschi, M.; Ulivi, P.; Bravaccini, S. An Italian Real-World Study Highlights the Importance of Some Clinicopathological Characteristics Useful in Identifying Metastatic Breast Cancer Patients Resistant to CDK4/6 Inhibitors and Hormone Therapy. Biomedicines 2024, 12, 498. https://doi.org/10.3390/biomedicines12030498
Maltoni R, Roncadori A, Balzi W, Mazza M, Nicolini F, Palleschi M, Ulivi P, Bravaccini S. An Italian Real-World Study Highlights the Importance of Some Clinicopathological Characteristics Useful in Identifying Metastatic Breast Cancer Patients Resistant to CDK4/6 Inhibitors and Hormone Therapy. Biomedicines. 2024; 12(3):498. https://doi.org/10.3390/biomedicines12030498
Chicago/Turabian StyleMaltoni, Roberta, Andrea Roncadori, William Balzi, Massimiliano Mazza, Fabio Nicolini, Michela Palleschi, Paola Ulivi, and Sara Bravaccini. 2024. "An Italian Real-World Study Highlights the Importance of Some Clinicopathological Characteristics Useful in Identifying Metastatic Breast Cancer Patients Resistant to CDK4/6 Inhibitors and Hormone Therapy" Biomedicines 12, no. 3: 498. https://doi.org/10.3390/biomedicines12030498
APA StyleMaltoni, R., Roncadori, A., Balzi, W., Mazza, M., Nicolini, F., Palleschi, M., Ulivi, P., & Bravaccini, S. (2024). An Italian Real-World Study Highlights the Importance of Some Clinicopathological Characteristics Useful in Identifying Metastatic Breast Cancer Patients Resistant to CDK4/6 Inhibitors and Hormone Therapy. Biomedicines, 12(3), 498. https://doi.org/10.3390/biomedicines12030498