
Novel Interventions on Comorbidities in Patients with Fetal Alcohol Spectrum Disorder (FASD): An Integrative Review


 ,
,  ,
,  ,
, 
Abstract
1. Introduction
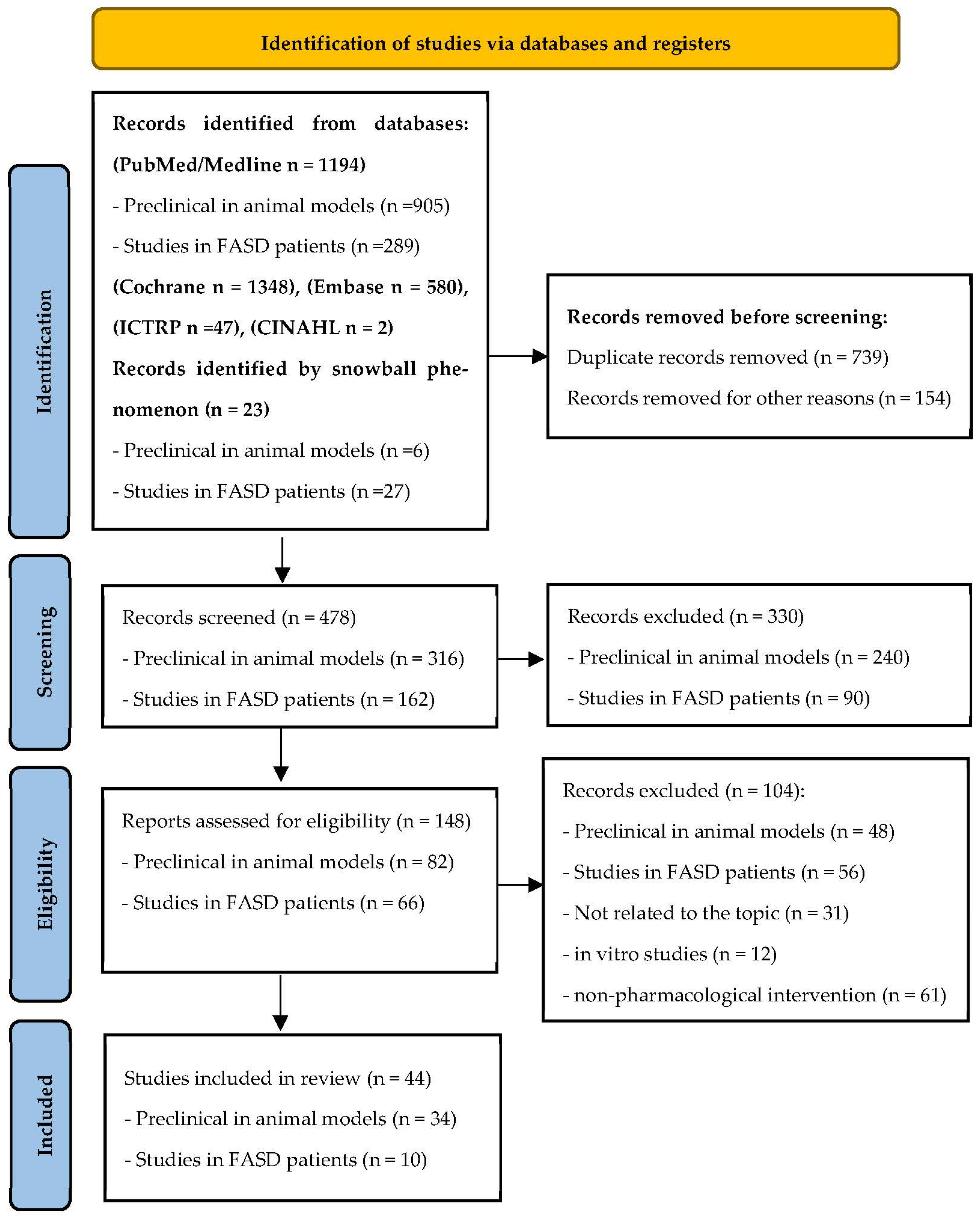
2. Materials and Methods
3. Results
3.1. Characteristics of the Included Studies
3.2. Results from Animal Studies

{kind=link}
| Author Year Country | Pharmacological Intervention | Study Design and Objectives | Population | EtOH Exposure | Dose/Intervention Period | Variables Studied | Key Results |
|---|---|---|---|---|---|---|---|
| Patten et al. [43], 2013 Canada | Omega-3 fatty acids | RCT to determine whether feeding an omega-3 fatty acid-enriched diet from birth is able to overcome the deficits in synaptic plasticity that occur with PNE | Sprague-Dawley rats (N = 24) Offspring (N = 10 each group) | Prenatal exposure to EtOH Offspring exposure | Dams: ‣on GD1: prenatal diets EtOH or Pair-fed or Ad libitum control ‣on GD 15: BAC assessment. When pups were born, the dams were placed on either a regular chow diet or an omega-3-enriched diet Pups: ‣at P22: they were continued on The same postnatal diet as their mothers until they reached an experimental age (P55–70) ‣at P70: animals were used for in vivo electrophysiological experiments ‣Pre-stimulation: pulse 0.12 ms (duration) at 0.067 Hz LTP induced by applying TBS ‣Post-stimulation: 60 min at 0.067 Hz | EtOH, LTP, omega-3 fatty acids | omega-3 fatty acids can reduce oxidative stress and enhance antioxidant protection in PNE animals |
| Naseer et al. [52], 2014 | Osmotin | In vitro and in vivo study to examine the neuroprotective effects of adiponectin-activated pathways against FAS | Rats Sprague-Dawley rats (P7) | exposed to EtOH for 12 and 24 h no prenatal exposure to EtOH | ‣CT: no treatment ‣TG1: EtOH (100 mM) ‣TG2: Osm (0.16 mM) + ‣EtOH (100 mM) after 24 h staining with FJB and PI ‣20% EtOH in normal saline (4 mg/g body weight) | Osm, EtOH, caspase-3, AMPK activity | ‣AMPK-activating drugs such as metformin, adiponectin, and osmotin prevent the effects of FAS ‣Osmotin is an experimental alternative to adiponectin |
| Liang et al. [47], 2014 USA | Dihydromyricetin | RCT to study the effect of FAE on physiology, behavior, and GABAAR function of early adolescent rats to test the utility of DHM as a preventative treatment for FAE-induced disturbances | Sprague-Dawley young rats | Prenatal exposure to EtOH Offspring exposure | ‣Dams: pregnant dams received the following treatments: (1) EtOH (1.5 g/kg, gavage); (2) EtOH (2.5 g/kg); (3) EtOH (5 g/kg); (4) EtOH (1.5 g/kg) + DHM (1 mg/kg); (5) EtOH (2.5 g/kg) + DHM (1 mg/kg); (6) EtOH (5.0 g/kg) + DHM (1 mg/kg); (7) DHM (1 mg/kg); (8) vehicle (water, 20 mL/kg) ‣Offspring: Behavioral and electrophysiological experiments were performed on P25-35 | EtOH; DHM; anxiety-related behavior; Plasma EtOH Concentration assessment; brain analysis | The absence of adverse side effects and the ability of DHM to completely prevent FAE consequences suggest that DHM is an attractive candidate for development as a treatment for the prevention of FASD |
| Bearer et al. [38], 2015 USA | Choline | RCT to determine if choline supplementation prior to an acute exposure to ethanol on P5 would reduce the effects of EtOH on the dowel crossing test | C57B16/J mice pups | No prenatal exposure to EtOH | Prenatal treatment from E 4.5 to P21: pups received choline-deficient pellet diet Postnatal treatment (from P2): Pre-exposure treatment: S group: 10 μL C group: 10 μL of 18/8 mg/mL Exposure (on P5): EtOH group (6 g/kg) Intralipid® group Post-exposure (from P6 to P20): S group: 10 μL C group: 10 μL of 18/8 mg/mL On P30: balance and coordination assessment (6 animals per sex per treatment group) | BAC; balance and coordination; Dowel Crossing Test | Choline fortification of common foodstuffs may reduce the effects of alcohol |
| Wellmann et al. [53], 2016 USA | Docosahexaenoic acid (DHA) | RCT to evaluate if DHA reduction underlies (or contributes to) the neurobehavioral problems observed in FASD, to determine if postnatal DHA supplementation will ameliorate neurobehavioral problems in animal model of FASD | Long-Evans rats | Prenatal exposure to EtOH Offspring exposure | Dams: Timed pregnant rats were assigned to one of 3 groups: ‣ad libitum access to an ethanol-containing liquid diet; ‣pair fed an isocaloric isonutritive non-alcohol liquid diet; ‣ad libitum access to chow and water. Pups: From P11 to P20 pups were assigned to: ‣DHA (10 g/kg in artificial rat milk); ‣artificial rat milk 0.01 mL/g; ‣CT. | P14: iUSVs assessment. P28 or P42: Social behavior and play-induced USVs assessment. P33 or P42: somatosensory performance assessment. P35: anxiety assessment. | DHA administration may have therapeutic value to reverse some of ethanol’s damaging effects |
| Balaraman et al. [39], 2017 USA | Choline | RCT to examine whether the nutrient choline would modify ethanol’s effects on miRNAs | Sprague-Dawley rats (N = 48; 6 for each experimental group) | No prenatal alcohol exposure | From P4 to P21: ‣EtOH (2.625 g/kg) + C (100 mg/kg/day) +  (or (or  ) )‣EtOH (2.625 g/kg) + S + (or )‣Sham + C (100 mg/kg/day) + (or )‣Sham + S + (or ) | EtOH, choline, P22: brain examination, with dissection of the hippocampus and isolation of RNA | Choline modification of EtOH effects on miRNAs provide another avenue through which choline may protect against ethanol’s teratogenic effects |
| Waddell et al. [40], 2017 USA | Choline | RCT to test if working memory training during adolescence combined with choline supplementation would improve cognitive flexibility in rat model of FASD more effectively than either intervention alone | Rats (GD3) | Prenatal exposure to EtOH Offspring exposure | Dams: ‣CT group (N = 9) ‣ET group (N = 10): diet containing 3% ethanol for the duration of the exposure From P16 to P30: ‣SC saline (0.9% Sal; pH 7.4) group ‣SC choline (Cho; 100 mg/kg) group From P30 to P38: ‣Tr group ‣Utr group Offspring assigned to one of 4 postnatal groups: Sal-Utr; Sal-Tr; Cho-Utr; Cho-Tr | EtOH, Choline, working memory | Possible beneficial effect of choline in FASD; it may be more efficacious when coupled with cognitive training |
| Sogut et al. [50], 2017 Turkey | Folic acid and betaine | RCT to investigate prenatal EtOH exposure-related neuroapoptosis on the cerebral cortex tissues of newborn rats and possible neuroprotective effects of betaine, folic acid, and combined therapy | Sprague-Dawley rats Pregnant rats N = n.d. Offspring N = 65 | Pregnant rats were divided into 5 experimental groups: control, EtOH, EtOH + betaine, EtOH + folic acid, and EtOH + betaine + folic acid combined therapy groups | Betaine, Calpain, cathepsin B and L, enzyme activities Caspase-3, Cytochrome c, Folic acid | Folic acid, betaine, and combined therapy of these supplements may reduce neuroapoptosis related to prenatal alcohol consumption and might be effective in preventing FAS | |
| Wang et al. [57], 2018 USA | Minocycline | In vitro and in vivo study to demonstrate the neuroprotective role of minocycline | C57BL/6 Mice | No prenatal EtOH exposure | On PD5, pups were randomly assigned to: CG, minocycline group, EtOH group, and EtOH + minocycline | Minocycline, EtOH, microglial cells and neurons | minocycline may ameliorate EtOH neurotoxicity in the development by alleviating GSK3β-mediated neuroinflammation |
| Skorput et al. [58], 2019 USA | NKCC1 inhibitor Bumetanide | In vivo and ex vivo study to assess whether the NKCC1 cotransporter is a tractable pharmacological target for normalizing in utero ethanol exposure-induced escalation of tangential migration to the prefrontal cortex | Nkx2.1Cre/Ai14 mice harboring Tomato-fluorescent (Nkx2.1+) | Dams EtOH exposure Dams CT | ‣5% w/w EtOH alone, from E13.5 to E16.5 ‣5% w/w EtOH + Bumetanide DMSO solution: 0.15 mg/kg/day, 3 days ‣Isocaloric control diet containing maltose | ‣Density of Nkx2.1+ profiles in the embryonic prefrontal cortex at E16.5 ‣PV+ interneurons in the PFC of young adult mice exposed to EtOH and EtOH + Bumetanide | ‣EtOH alone ↑ Density of Nkx2.1+ neurons ‣Bumetanide ↓ ethanol-induced enhancement of tangential migration of GABAergic cortical interneurons vs. CT |
| Ren et al. [59], 2019 USA | Minocycline | RCT to determine whether minocycline’s neuroprotective and anti-inflammatory properties can reduce EtOH-induced damage to spinal cord neuron development | C57BL/6 mice | No prenatal EtOH exposure | On PD5: ‣CT (SC injections of sterile saline) ‣Min group (2 SC injections/30 mg/kg) ‣EtOH group (5 g/kg) ‣EtOH (5 g/kg) + Min (2 SC injections/30 mg/kg) BAC = 338 mg/dL 8 h after the first injection | EtOH, minocycline, spinal cord | Minocycline may have neuroprotective property against ethanol-induced spinal cord damage. More investigation of the dosage and timeline of minocycline’s action is necessary. |
| Montagud-Romero et al. [49], 2019 | Trichostatin A (TSA) | RCT to assess the effects of TSA on emotional and cognitive impairments caused by PLAE | C57BL/6 mice | Prenatal exposure to EtOH (N = 30) Offspring (N = 80 males) | Dams: binge alcohol drinking model during gestation and lactation (20% v/v alcohol solution) Pups: From P28 to P35: treatment with TSA from P36 to P55 behavior assessment | EtOH, TSA, anxiogenic-like responses, and memory deterioration | potential benefits of HDAC inhibitors for some aspects FASD |
| Cantacorps et al. [46], 2020 Spain | Curcumin | RCT to assess the effects of curcumin in counteracting behavioral and molecular alterations induced by EtOH exposure during development | C57BL/6 mice (N = 24 for PAE) | Prenatal exposure to EtOH Offspring | Dams: ‣DID test ‣CG: water EG: 20% EtOH (oral) Pups: ‣P28: daily treatment with curcumin and vehicle solution ‣P60: EPM ‣P61: Y-maze ‣P62: NOR ‣P66: T-maze ‣P70: brain extraction | Curcumin; anxiety-like behavior; working memory; recognition memory; spatial ability | Curcumin could be a useful treatment for attenuating the alcohol-induced deficits observed in FASD |
| Cadena et al. [51], 2020 USA | Folic Acid | RCT to test FA ability to protect against behavioral defects induced by EtOH exposure | zebrafish | No prenatal exposure to EtOH | Healthy embryos were maintained in embryo medium until 2 hpf ‣CT group: animals transferred to embryo medium, no treatment ‣EtOH group: embryo medium containing 100 mM EtOH ‣EtOH + FA group: embryo medium containing 100 mM EtOH and 75 μM FA ‣FA group: embryo medium containing 75 μM FA | FA, EtOH, Teratogenic effects on morphological development (COA, ED, EY, PE, SB, SD, TD, YSE, YSR, HR, LP) Behavior (locomotor activity, sleep, anxiety like-behavior, visual ability) | FA alone produced different behavioral responses, indicating that FA may independently modify fish development. This zebrafish behavior on FASD model also provides an opportunity to test whether other compounds reduce the EtOH toxic effects. |
| Bottom et al. [41], 2020 USA | Choline | RCT to assess the ability of concurrent choline supplementation to ameliorate atypical neocortical and behavioral development following fully or partially PAE | CD-1 Mice | Prenatal exposure to EtOH Offspring | Dams (N = 10 for each group): ‣group 1: Water (Control) ‣group 2: 25% EtOH in water ‣group 3: 25% EtOH in water with 642 mg/L choline chloride ‣group 4: 642 mg/L choline chloride in water (CW). Separate subsets of dams were sacrificed at either GD9 and 19 for BEC and POSM measurements during gestation (n = 10, all groups). Pups: ‣Experimental analyses in brain: 1 ± 1 pups (P0) were selected pseudo-randomly from each litter. ‣Behavioral analysis: subsets of each litter in all groups were cross-fostered to alcohol-naïve mothers until P20 when behavioral testing of 3 ± 1 pups per litter took place. | EtOH, Choline, BEC, POSM, anxiety-like behaviors, motor function | Choline supplementation may represent a potent preventative measure for the adverse outcomes associated with PAE |
| Mohammad et al. [60], 2020 USA | Kcnn2 blockers | In vivo study to assess if PAE leads to deficits in gross and fine motor skill learning | Mice | Prenatal exposure to EtOH | Dams exposed to EtOH (1.0 g/kg weight), at E 16 and 17, during which upper cortical layer neurons are predominantly generated | Kcnn2, motor cortex, motor learning deficits | Kcnn2 blockers may be a novel intervention for learning disabilities in FASD |
| Ju et al. [1], 2020 Republic of Korea | HX106 | RCT to assess the effects of HX106 on PAE-induced ADHD-like phenotype and metabolic changes in the offspring mice | ICR mice (28–30 g weight) | Prenatal exposure to EtOH Offspring | Female at GD 3. Stabilized animals divided into 3 groups (from GD 6 to GD 15): ‣CT: saline (0.9% NaCl) ‣EtOH 2 groups: 6 g/kg/day; 50 v/v%) Pups (from P21; n = 10 per each group) ‣CT group: saline ‣OPAE groups: saline + HX106 at 200 mg/kg/day | ADHD-Like Symptoms, HX106, EtOH | ADHD pathology may involve metabolic disruptions and HX106 can be a promising supplement to attenuate the hyperactivity appearance in PAE-induced ADHD-like neuropathology |
| Almeida-Toledano et al. [61], 2021 Spain | Epigallocatechin Gallate | RCT to describe the effect of EGCG administration on oxidative stress, fetal growth, placental development, and neurogenesis processes in 2 human-like patterns of alcohol use FAS mouse models | 283 mouse fetuses | ‣Group 1: 42 Med control ‣group 2: 47 Med EtOH ‣group 3: 45 EtOH Med + EGCG ‣group 4: 54 Bin control ‣group 5: 44 Bin EtOH ‣group 6: 47 Bin + EGCG EtOH | Blood EtOH levels; EGCG; fetal growth; EtOH effect on oxidative stress; neuronal maturation and plasticity; astrocyte differentiation | EGCG is a promising antioxidant therapy to attenuate the consequences of PAE | |
| Gibula-Tarlowska et al. [56], 2021 Poland | CE-123 DAT inhibitor | RCT to demonstrate that dopamine signaling is one of the main factors underlying hyperactive, inattentive, and impulsive behaviors | Male rat (N = 163) | No prenatal exposure to EtOH | EtOH on P4-9. ‣Weaning: P20 group 1 was tested in early adolescence (P21) ‣group 2 was tested as adults (P45-50) group 3 was tested at P50 | BEC; Locomotor activity test; EPM test; Barnes maze task | CE-123 may be helpful in overcoming behavioral disorders in subjects perinatally exposed to ethanol |
| Lopatynska-Mazurek et al. [45], 2021 Poland | Rapamycin | Prospective cohort study to evaluate the hypothesis that development of emotional learning deficits and depressive-like behaviors in adult rats exposed to EtOH during the neonatal period are a function of oxidative stress that, in turn, depends on the mTOR signaling pathway | Male rats (N = 64) | No prenatal exposure to EtOH | from P4 to P9: ‣S (0.9%) + SI ‣Rapamycin + SI ‣Torin 2 + SI ‣FK-506 + SI ‣S (0.9%) + EtOH (5 g/Kg/day) ‣Rapamycin + EtOH (5 g/Kg/day) ‣Torin 2 + EtOH (5 g/Kg/day) ‣FK-506 + EtOH (5 g/Kg/day) ‣P60 (adults): aversive learning and memory processes assessment; depressive-like behavior assessment | EtOH, Rapamycin, Torin, FK-506 | Rapamycin but not Torin-2 or FK-506 could have protective effects against the ethanol-induced LPO and AP site levels in the hippocampus and prefrontal cortex. Rapamycin could be useful as a preventive therapy in disorders related to PAE. |
| García-Baos et al. (2021) [62] Spain | Cannabidiol | RDBPC to explore CBD therapeutic effects demonstrating that it might reduce through an anti-inflammatory mechanism. Cognitive deficits induced by EtOH exposure. | C57BL/6 mice | Prenatal exposure to EtOH Offspring | Pregnant females: DID test during PLAE. Day 4: six binge-like drinking sessions. Dose ethyl alcohol n.d. Offspring: CBD 20 mg/kg during 10 consecutive days from P25 until P34 Behavioral assessment: P60–P66 P70: PFC and HPC extraction | CBD, EtOH, spatial, working and recognition memory | CBD appears to be a promising therapeutic drug since it could hamper cognitive impairments caused by several pathological conditions, potentially through neuroimmune modulation |
| Grafe et al. [42], 2021 Canada | Choline | RCT to examine the impact of acute choline administration on synaptic transmission in the in vitro DG and how these mechanisms may be altered by EtOH exposure of male and female offspring | Sprague-Dawley rats | GD1 2 experimental groups: ‣PNE diet was a protein and liquid diet containing 35.5% ethanol-derived calories. Dams were gradually introduced to the ethanol diet and subsequently consumed only the ethanol diet from GD 22 until the day before birth. ‣On GD 21: dams were returned to a solid control chow diet and remained on this diet until parturition. CT diet. | EtOH, choline, NMDA, M1 receptors | choline can modulate hippocampal transmission at the level of the synapse and it can have unique effects following EtOH exposure | |
| Sharma et al. [2], 2021 India | Papaverine | RCT to assess the outcome of papaverine administration on PAE affected behavioral (hyperactivity, repetitive behavior, and anxiety) and biochemical markers in several brain areas associated with ADHD | N = 40 Adults albino wistar rats | Prenatal exposure to EtOH Offspring | Dams (from GD8 to GD20): ‣EtOH (20% w/v; 6 g kg−1 day−1-weekdays; 4 g kg−1 day−1-weekends; N = 8); CT group: received calorifically equivalent sucrose solution (30% w/v; N = 5) Pups (from P21 to P48), 4 Exp groups (each with 8 males): ‣Group I and II (VEH/Drug per-se); sucrose solution-treated females were administered with normal saline—2 mL kg−1 i.p., or Papaverine—30 mg kg−1 day−1, i.p., as per the treatment assigned. ‣Group III (PAE); females treated with EtOH during gestation were treated with NS—2 mL kg−1, i.p. ‣Groups IV and V (Papaverine treatment); PAE pups were divided further into PAE + P (15/30) groups and received papaverine (15/30 mg/kg day−1 i.p.) in a volume of 2 mL kg−1. ‣Behavioral assessment: P44 to P48. | ADHD-Like Symptoms; papaverine; EtOH | Papaverine, a selective PDE10A inhibitor rectified behavioral phenotypes associated with ADHD, possibly by altering the protein markers associated with neuronal survival, neuronal transcription factor, brain inflammation, and brain oxidative stress. Implicating PDE10A as a possible target for furthering our understanding of ADHD phenotypes. |
| Chen et al. [63], 2022 Taiwan | AST | RCT to explore how AST treatment can ameliorate morphological changes in the hippocampus and cognitive impairment in FASD rats by reducing oxidative stress and neuroinflammation in the brain | 40 male rat pups | No prenatal exposure to EtOH | 4 groups: CT; normal with AST; FASD group; ethanol-inhaled with AST treatment. FASD induction started on P2 and continued until P10. To investigate AST effects in a FASD rat model, it was administered on P53 and kept until sacrifice (P60). | EtOH, AST, MWM task, BWT | AST could be considered to treat FASD |
| Sabzali et al. [44], 2022 Iran | Metformin | In vivo and ex vivo study to evaluate the protective effects of metformin on EtOH-related neuroinflammation, as well as neuron apoptosis in the hippocampus of adult male rat model of FASD | 60 Wistar male rat pups (8–10 g) | No prenatal exposure to EtOH | EtOH in milk solution (5.25 and 27.8 g/kg, respectively) by intragastric intubation at 2–10 days after birth | tumor necrosis factor-α (TNF-α) and antioxidant enzyme concentrations | Metformin reduces cell apoptosis in the hippocampus. It can be considered a promising therapeutic option for FASD; however, more research is required. |
| Burton et al. [64], 2022 USA | Smoothened Agonist (SAG); purmorphamine (PUR) | In vivo study to demonstrate that a Shh pathway agonist given at an appropriate dose and timing relative to ETOH exposure during embryogenesis may alleviate the effects of PAE | Zebrafish embryos (AB strain, ZFIN ID: ZDB-GENO-960809-7) | Zebrafish embryos exposed to EtOH from 8–10 hpf | Embryos exposed to varying concentrations of SAG or PUR at 6–8 hpf or 10–12 hpf by diluting with egg water | EtOH, Eye size data, gene expression, novel tank diving data, midbrain hindbrain data, and pax6a in situ expression data | Pharmacological activation of the Shh pathway at specific developmental timing markedly diminishes the severity of alcohol-induced birth defects as altered eye size and midline brain development |
| Farhadi et al. [65], 2022 Iran | Crocin | RCT to evaluate the protective impact of crocin on ethanol-related neuroinflammation | 72 wistar rat pups (8 to 10 g) | No prenatal exposure to EoTH | Pups treated from P2 to P10. Group 1: CT Group 2: milk + saline solution (dose n.a.) Group 3: milk solution + ethanol (total daily dose of ethanol (5.25 g/kg) Groups 4, 5, 6: milk solution + ethanol + crocin (15, 30, and 45 mg/kg) | EtOH; Crocin; astrogliosis evaluation; inflammation measurement; enzyme evaluation; spatial memory | Crocin is applicable for the treatment of FASD |
| Gasparyan et al. [66] 2023 Spain | Cannabidiol | RCT to evaluate the effects of early and chronic CBD administration on offspring exposed to an animal model of FASD | N = 190 c57bl/6j mice 50 female and 20 male 5-week-old mice Offspring: 120 (60 males and 60 females) | Prenatal exposure to EtOH Offspring | PAE: N = 15 females exposed to 2 bottles with tap water. N = 35 females exposed to 2 bottles, one always with tap water and the other increasing EtOH concentrations. PAE: at GD7, EtOH gavage was started until the pup’s weaning at P21. Pups: treated with CBD 30 mg/kg/day or VEH from the day of weaning for 10 weeks. | CBD, ethanol, anxiety-like behaviors, depressive-like behaviors; ASR; recognition memory; long-term aversive memory; gene expression analyses; brain analysis | Potential suitability of CBD in children and young adults with FASD |
, male gender; , female gender; ADHD, attention deficit hyperactivity disorder; AP, apurinic/apyrimidinic; AST, astaxanthin; EC or BAC, blood ethanol concentration; Bin, binge; BWT, beam walking test; C or Cho, choline; CBD, cannabidiol; Cho-Tr, choline-trained; Cho-Utr, choline-untrained; COA, coagulation; CT, control group; DAT, dopamine transporter; DHA, docosahexaenoic acid; DHM, dihydromyricetin; DG, dentate gyrus; DID, drinking in the dark; E, embryonic day; ED, large inter-eye distance; EGCG, epigallocatechin-3-gallate; EPM, elevated pus maze test; ET, ethanol-exposed group; EtOH, ethanol or alcohol; EY, small eyes; FAE, Fetal alcohol exposure; FAS, fetal alcohol syndrome; FJB, fluoro-jade B; FST, forced swimming test; GABAAR, γ-aminobutyric acid type A receptor; GD, gestational day; GFAP, glial fibrillary acidic protein; GSH-Px, glutathione peroxidase; GSK3β, glycogen synthase kinase 3 beta; HAT, histone acetyltransferase; HDAC, histone deacetylases enzymes; HPC, hippocampus; hpf, hour post-fertilization; HR, hatching rate; larvae paralysis; iUSVs, isolation-induced ultrasonic vocalizations; LPO, lipid peroxidation; LTD, long-term depression; LTP, long-term potentiation; Med, mediterranean; Min, minocycline; mIPSCs, inhibitory postsynaptic currents; mTOR, mammalian target of the rapamycin; MWM, morris water maze; n.d., not declared; NMDA, N-methyl-d-aspartate; NOR, novel object recognition test; OPAE, Offspring prenatal alcohol exposure; Osm, osmotin; P or PD, postnatal day; PAE, prenatal alcohol exposure; PE, pericardial edema; PFC, prefrontal cortex; PI, propidium iodide; PLAE, prenatal and lactational alcohol exposure; PNTG, postnatal treatment group; PNUn, postnatal untreated group; POSM, plasma osmolality; PUFAs, polyunsaturated fatty acids; RCT, randomized controlled trial; RDBPC, randomized double blind placebo control study; S, saline; Sal-Tr, saline-trained; Sal-Utr, saline-untrained; SB, delayed swim bladder inflation; SC, subcutaneous; SD, spine deformation; Shh, sonic hedgehog; SI, sham intubation; SOD, superoxide dismutase; TBS, theta burst stimulation; TD, tail deformation; TG, treatment group; THIP, gaboxadol hydrochloride; TNF-α, tumor necrosis factor-α; Tr, working memory training; TSA, trichostatin A; Utr, untrained; VEH, vehicle; YSE, yolk sac edema/unusual large yolk sac; YSR, delayed yolk sac resorption.3.3. Results from Human Studies
| Author Year Country | Study Design and Objectives | Pharmacological Intervention | Dose Intervention Period | Population (N) | Patient Age, Mean (SD) | Variables Studied | Key Results/Assessment |
|---|---|---|---|---|---|---|---|
| Wozniak J.R. et al. [71], 2013 USA | RDBPC to evaluate tolerability and bioavailability of choline as supplement for FASD children | Postnatal choline bitartrate (1.25 g) | 514 mg/day, 9 m | Children: ‣10 active ‣9 placebo | 2–5 y (range) | ‣Feasibility ‣Tolerability ‣Adverse effects ‣Serum choline levels | ‣Minimal and equivalent adverse effects were observed in choline and placebo groups. Fishy body odor was reported for choline group ‣Acceptable feasibility and tolerability |
| Wozniak J.R. et al. [72] 2015 USA | RDBPC to assess hippocampal-dependent memory improvement by postnatal choline supplementation in FASD children | Postnatal choline bitartrate (1.25 g) | 514 mg/day, 9 m | Children: ‣31 active ‣29 placebo | 3.8 y (0.80) | ‣Mullen Scales of Early Learning (global cognitive functioning) ‣Elicited imitation memory tasks | ‣No choline effects were observed in global cognitive functioning ‣Choline ↑ hippocampal-dependent memory tasks especially in younger children (≤4 y) and best score were obtained in long-delayed memory |
| Coles C.D. et al. [67], 2015 USA Ukraine | PCS to evaluate mother nutritional supplements use impact on children prenatally exposed to alcohol | ‣prenatal MVM ‣prenatal MVM + Choline | ‣nd ‣nd + 750 mg Choline from first prenatal clinic visit until delivery | 367 Children | ‣Children development assessment through BSID-II at 6 m of age | ‣MVM ↑ cognitive development ‣Choline has no effect on cognitive development and negative effects on motor outcomes ‣No differences between prenatally alcohol-exposed and non-exposed children | |
| Nguyen T.T. et al. [73], 2016 USA | RDBPC to investigate if choline supplements have positive effects on the memory impairments, executive function, and attention deficits in school-aged (5–10 y) FASDs children | Postnatal Glicerophospho-choline | 625 mg/day, 6 wk | 55 Children: ‣29 active ‣26 placebo | 8.3 y (1.75) | ‣Cognitive abilities in the domains of learning and memory, executive function, (attention, fine motor functioning) | ‣Choline supplements did not improve memory, executive and attention functioning in school-aged (5–10 y) children with FASDs |
| Jacobson S.W. et al. [68], 2018 South Africa | RDBPC to assess adherence and side effects to choline supplementation in heavy drinking pregnant women | Prenatal choline bitartrate | 2 g/day, from mid-pregnancy until delivery | Mothers: ‣34 active ‣35 placebo | 26.4 y (5.7) | ‣Adherence ‣Side effects ‣Choline plasma concentration | ‣Choline adherence was excellent (≥84%) and good to excellent (≥68%) for 42% and 58% of participants, respectively. It was not related to maternal education, depression, intellectual function, stressful life events or socioeconomic status. ‣Increase in nausea/dyspepsia symptoms, especially when choline is consumed on an empty stomach. ‣Choline levels in plasma were significantly higher than those of the placebo group. |
| Jacobson S.W. et al. [69], 2018 South Africa | RDBPC to assess prenatal choline supplementation effects on EBC, on growth, recognition memory and information processing speed deficit | Prenatal choline bitartrate | 2 g/day, 9–27 wk (range) | 62 Infants: ‣31 active ‣31 placebo | ‣6.5 m ‣1 y | ‣EBC assessed at 6.5 m ‣Infant growth assessed at 6.5 m and 1 y ‣Visual recognition memory assessed at 6.5 m and 1 y through FTII ‣FASD diagnosis | ‣Prenatal choline supplementation ↑ conditioned responses more than placebo, especially in mother with high adherence to the treatment. ‣Newborns in the placebo and choline group were both small at birth. Infants in choline group; nevertheless, a weight and head circumference growth increase between 6.5 m and 1 y ‣FAS and pFAS diagnosis incidence for the choline and placebo group was almost the same |
| Sarkar et al. [74], 2019 USA | RDBPC to assess if choline can reduce DNA methylation and improve POMC and PER2 gene expression by analyzing blood sample of FASD children treated with the supplement | Postnatal choline bitartrate | 514 mg/day, 9 m | 32 Children: ‣16 active ‣16 placebo | 2.5–5 y (range) | ‣POMC and PER2 mRNA levels measured by quantitative real-time PCR ‣DNA methylation assessed by methylation-specific real time PCR assay | ‣Choline increased POMC and PER2 gene expression following 9 m of treatment ‣Choline reduced PER2 and POMC DNA methylation following 9 m of treatment |
| Wozniak J.R. et al. [75], 2020 USA | RDBPC follow-up study evaluating postnatal choline supplementation potential on long-term cognitive and behavioral functions of PAE children | Postnatal choline | 514 mg/day, 9 m | 31 Children: ‣15 active ‣16 placebo | 8.6 y (1.0) | ‣Cognitive, memory, executive, behavioral and emotional functioning | ‣Significant non-verbal Visual-Spatial Reasoning and non-verbal Working Memory components in the choline group vs. placebo ‣choline had non-significant effects on quantitative reasoning, fluid reasoning, and a range of verbally-mediated skills ‣Choline group had fewer ADHD-related behavioral problems than the placebo group |
| Warton F.L. et al. [70], 2021 South Africa | Follow-up study observing if prenatal choline supplementation protected PAE newborn brain from volume reduction and improved infant recognition memory | Prenatal choline | 2 g/day | 50 Children: ‣27 active ‣23 placebo | 2.8 wk median | ‣MRI data of newborn brains ‣Recognition memory through FTII at 12 months | ‣Larger total intracranial volume in choline group vs. placebo ‣Larger right putamen and corpus callosum were associated with improved recognition memory |
| Gimbel B.A. et al. [76], 2022 USA | Follow-up study evaluating postnatal choline effects on executive functioning and white matter microstructure | Postnatal choline bitartrate | 514 mg/day, 9 m | 18 Children: ‣9 active ‣9 placebo | 11.0 y | ‣Executive functioning ‣Differences in corpus callosum and white matter microstructure through diffusion-weighted MRI and the NODDI biophysical model | ‣Improved executive functioning in choline group vs. placebo ‣Lower corpus callosum orientation dispersion index (more coherent fibers) in choline group vs. placebo |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jones, K.L.; Smith, D.W.; Ulleland, C.N. Pattern of malformation in offspring of chronic alcoholic mothers. Lancet 1973, 301, 1267–1271. [Google Scholar] [CrossRef]
- Riley, E.P.; Infante, M.A.; Warren, K.R. Fetal Alcohol Spectrum Disorders: An Overview. Neuropsychol. Rev. 2011, 21, 73–80. [Google Scholar] [CrossRef]
- Brown, J.M.; Bland, R.; Jonsson, E.; Greenshaw, A.J.; Riley, E.P.; Infante, M.A.; Warren, K.R.; Jones, K.L.; Smith, D.W.; Ulleland, C.N. The Standardization of Diagnostic Criteria for Fetal Alcohol Spectrum Disorder (FASD): Implications for Research, Clinical Practice and Population Health. Can. J. Psychiatry 2011, 64, 73–80. [Google Scholar] [CrossRef]
- Elliott, L.; Coleman, K.; Suebwongpat, A.; Norris, S. Fetal Alcohol Spectrum Disorders (FASD): Systematic Reviews of Prevention, Diagnosis and Management; Health Services Assessment Collaboration, University of Canterbury: Christchurch, New Zealand, 2008. [Google Scholar]
- May, P.A.; Gossage, J.P. Maternal Risk Factors for Fetal Alcohol Spectrum Disorders: Not as Simple as It Might Seem. Alcohol Res. Health J. Natl. Inst. Alcohol Abuse Alcohol. 2011, 34, 15–26. [Google Scholar]
- Bell, J.C.; Raynes-Greenow, C.; Turner, R.M.; Bower, C.; Nassar, N.; O’Leary, C.M. Maternal Alcohol Consumption during Pregnancy and the Risk of Orofacial Clefts in Infants: A Systematic Review and Meta-Analysis. Paediatr. Perinat. Epidemiol. 2014, 28, 322–332. [Google Scholar] [CrossRef]
- Caputo, C.; Wood, E.; Jabbour, L. Impact of Fetal Alcohol Exposure on Body Systems: A Systematic Review. Birth Defects Res. Part C Embryo Today Rev. 2016, 108, 174–180. [Google Scholar] [CrossRef]
- Abel, E.L. An Update on Incidence of FAS: FAS Is Not an Equal Opportunity Birth Defect. Neurotoxicol. Teratol. 1995, 17, 437–443. [Google Scholar] [CrossRef] [PubMed]
- Maya-Enero, S.; Ramis-Fernández, S.M.; Astals-Vizcaino, M.; García-Algar, Ó. Neurocognitive and Behavioral Profile of Fetal Alcohol Spectrum Disorder. An. Pediatría Engl. Ed. 2021, 95, 208.e1–208.e9. [Google Scholar] [CrossRef]
- Pei, J.; Flannigan, K. Interventions for Fetal Alcohol Spectrum Disorder: Meeting Needs Across the Lifespan. Int. J. Neurorehabilit. 2016, 3, 192. [Google Scholar] [CrossRef]
- Flannigan, K.; Kapasi, A.; Pei, J.; Murdoch, I.; Andrew, G.; Rasmussen, C. Characterizing Adverse Childhood Experiences among Children and Adolescents with Prenatal Alcohol Exposure and Fetal Alcohol Spectrum Disorder. Child Abus. Negl. 2021, 112, 104888. [Google Scholar] [CrossRef]
- Passmore, H.M.; Mutch, R.C.; Burns, S.; Watkins, R.; Carapetis, J.; Hall, G.; Bower, C. Fetal Alcohol Spectrum Disorder (FASD): Knowledge, Attitudes, Experiences and Practices of the Western Australian Youth Custodial Workforce. Int. J. Law Psychiatry 2018, 59, 44–52. [Google Scholar] [CrossRef]
- Roszel, E.L. Central Nervous System Deficits in Fetal Alcohol Spectrum Disorder. Nurse Pract. 2015, 40, 24–33. [Google Scholar] [CrossRef]
- Caley, L.M.; Kramer, C.; Robinson, L.K. Fetal Alcohol Spectrum Disorder. J. Sch. Nurs. 2005, 21, 139–146. [Google Scholar] [CrossRef]
- Kalberg, W.O.; May, P.A.; Buckley, D.; Hasken, J.M.; Marais, A.-S.; Vries, M.M.D.; Bezuidenhout, H.; Manning, M.A.; Robinson, L.K.; Adam, M.P.; et al. Early-Life Predictors of Fetal Alcohol Spectrum Disorders. Pediatrics 2019, 144, e20182141. [Google Scholar] [CrossRef]
- Streissguth, A.P.; Bookstein, F.L.; Barr, H.M.; Sampson, P.D.; O’Malley, K.; Young, J.K. Risk Factors for Adverse Life Outcomes in Fetal Alcohol Syndrome and Fetal Alcohol Effects. J. Dev. Behav. Pediatr. JDBP 2004, 25, 228–238. [Google Scholar] [CrossRef]
- Premji, S.; Benzies, K.; Serrett, K.; Hayden, K.A. Research-Based Interventions for Children and Youth with a Fetal Alcohol Spectrum Disorder: Revealing the Gap. Child Care Health Dev. 2007, 33, 389–397. [Google Scholar] [CrossRef]
- Bertrand, J.; Floyd, R.; Weber, M.; O’Connor, M.; Riley, E.; Johnson, K.; Cohen, D. National Task Force on FAS/FAE. Fetal Alcohol Syndrome: Guidelines for Referral and Diagnosis; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2004. [CrossRef]
- Petrenko, C.L.M.; Tahir, N.; Mahoney, E.C.; Chin, N.P. Prevention of Secondary Conditions in Fetal Alcohol Spectrum Disorders: Identification of Systems-Level Barriers. Matern. Child Health J. 2014, 18, 1496–1505. [Google Scholar] [CrossRef]
- Marrus, N.; Hall, L. Intellectual Disability and Language Disorder. Child Adolesc. Psychiatr. Clin. N. Am. 2017, 26, 539–554. [Google Scholar] [CrossRef]
- Terband, H.; Spruit, M.; Maassen, B. Speech Impairment in Boys with Fetal Alcohol Spectrum Disorders. Am. J. Speech Lang. Pathol. 2018, 27, 1405–1425. [Google Scholar] [CrossRef] [PubMed]
- Temple, V.K.; Cook, J.L.; Unsworth, K.; Rajani, H.; Mela, M. Mental Health and Affect Regulation Impairment in Fetal Alcohol Spectrum Disorder (FASD): Results from the Canadian National FASD Database. Alcohol Alcohol. 2019, 54, 545–550. [Google Scholar] [CrossRef]
- Mattson, S.N.; Crocker, N.; Nguyen, T.T. Fetal Alcohol Spectrum Disorders: Neuropsychological and Behavioral Features. Neuropsychol. Rev. 2011, 21, 81–101. [Google Scholar] [CrossRef] [PubMed]
- Popova, S.; Lange, S.; Shield, K.; Mihic, A.; Chudley, A.E.; Mukherjee, R.A.S.; Bekmuradov, D.; Rehm, J. Comorbidity of Fetal Alcohol Spectrum Disorder: A Systematic Review and Meta-Analysis. Lancet 2016, 387, 978–987. [Google Scholar] [CrossRef] [PubMed]
- Weyrauch, D.; Schwartz, M.; Hart, B.; Klug, M.G.; Burd, L. Comorbid Mental Disorders in Fetal Alcohol Spectrum Disorders: A Systematic Review. J. Dev. Behav. Pediatr. 2017, 38, 283–291. [Google Scholar] [CrossRef] [PubMed]
- Lange, S.; Rehm, J.; Anagnostou, E.; Popova, S. Prevalence of Externalizing Disorders and Autism Spectrum Disorders among Children with Fetal Alcohol Spectrum Disorder: Systematic Review and Meta-Analysis. Biochem. Cell Biol. 2018, 96, 241–251. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Bastons-Compta, A.; Astals, M.; Andreu-Fernandez, V.; Navarro-Tapia, E.; Garcia-Algar, O. Postnatal Nutritional Treatment of Neurocognitive Deficits in Fetal Alcohol Spectrum Disorder. Biochem. Cell Biol. 2017, 96, 213–221. [Google Scholar] [CrossRef] [PubMed]
- CDC. FASDs: Treatments. Available online: https://www.cdc.gov/ncbddd/fasd/treatments.html (accessed on 6 December 2023).
- Kalberg, W.O.; Buckley, D. FASD: What Types of Intervention and Rehabilitation Are Useful? Neurosci. Biobehav. Rev. 2007, 31, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Petrenko, C.L.M. Positive Behavioral Interventions and Family Support for Fetal Alcohol Spectrum Disorders. Curr. Dev. Disord. Rep. 2015, 2, 199–209. [Google Scholar] [CrossRef] [PubMed]
- Petrenko, C.L.M.; Alto, M.E. Interventions in Fetal Alcohol Spectrum Disorders: An International Perspective. Eur. J. Med. Genet. 2017, 60, 79–91. [Google Scholar] [CrossRef]
- Ozsarfati, J.; Koren, G. Medications Used in the Treatment of Disruptive Behavior in Children with FASD—A Guide. J. Popul. Ther. Clin. Pharmacol. J. Ther. Popul. Pharmacol. Clin. 2015, 22, e59–e67. [Google Scholar]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; Group, P.-P. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015: Elaboration and Explanation. BMJ 2015, 350, g7647. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A Web and Mobile App for Systematic Reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- Bearer, C.F.; Wellmann, K.A.; Tang, N.; He, M.; Mooney, S.M. Choline Ameliorates Deficits in Balance Caused by Acute Neonatal Ethanol Exposure. Cerebellum 2015, 14, 413–420. [Google Scholar] [CrossRef]
- Balaraman, S.; Idrus, N.M.; Miranda, R.C.; Thomas, J.D. Postnatal Choline Supplementation Selectively Attenuates Hippocampal microRNA Alterations Associated with Developmental Alcohol Exposure. Alcohol 2017, 60, 159–167. [Google Scholar] [CrossRef]
- Waddell, J.; Mooney, S. Choline and Working Memory Training Improve Cognitive Deficits Caused by Prenatal Exposure to Ethanol. Nutrients 2017, 9, 1080. [Google Scholar] [CrossRef] [PubMed]
- Bottom, R.T.; Abbott, C.W.; Huffman, K.J. Rescue of Ethanol-Induced FASD-like Phenotypes via Prenatal Co-Administration of Choline. Neuropharmacology 2020, 168, 107990. [Google Scholar] [CrossRef] [PubMed]
- Grafe, E.L.; Fontaine, C.J.; Thomas, J.D.; Christie, B.R. Effects of Prenatal Ethanol Exposure on Choline-Induced Long-Term Depression in the Hippocampus. J. Neurophysiol. 2021, 126, 1622–1634. [Google Scholar] [CrossRef]
- Patten, A.R.; Sickmann, H.M.; Dyer, R.A.; Innis, S.M.; Christie, B.R. Omega-3 Fatty Acids Can Reverse the Long-Term Deficits in Hippocampal Synaptic Plasticity Caused by Prenatal Ethanol Exposure. Neurosci. Lett. 2013, 551, 7–11. [Google Scholar] [CrossRef]
- Sabzali, M.; Eidi, A.; Khaksari, M.; Khastar, H. Anti-Inflammatory, Antioxidant, and Antiapoptotic Action of Metformin Attenuates Ethanol Neurotoxicity in the Animal Model of Fetal Alcohol Spectrum Disorders. Neurotox. Res. 2022, 40, 605–613. [Google Scholar] [CrossRef]
- Lopatynska-Mazurek, M.; Komsta, L.; Gibula-Tarlowska, E.; Kotlinska, J.H. Aversive Learning Deficits and Depressive-Like Behaviors Are Accompanied by an Increase in Oxidative Stress in a Rat Model of Fetal Alcohol Spectrum Disorders: The Protective Effect of Rapamycin. Int. J. Mol. Sci. 2021, 22, 7083. [Google Scholar] [CrossRef]
- Cantacorps, L.; Montagud-Romero, S.; Valverde, O. Curcumin Treatment Attenuates Alcohol-Induced Alterations in a Mouse Model of Foetal Alcohol Spectrum Disorders. Prog. Neuropsychopharmacol. Biol. Psychiatry 2020, 100, 109899. [Google Scholar] [CrossRef]
- Liang, J.; Shen, Y.; Shao, X.M.; Scott, M.B.; Ly, E.; Wong, S.; Nguyen, A.; Tan, K.; Kwon, B.; Olsen, R.W.; et al. Dihydromyricetin Prevents Fetal Alcohol Exposure-Induced Behavioral and Physiological Deficits: The Roles of GABAA Receptors in Adolescence. Neurochem. Res. 2014, 39, 1147–1161. [Google Scholar] [CrossRef] [PubMed]
- Andreu-Fernández, V.; Serra-Delgado, M.; Almeida-Toledano, L.; García-Meseguer, À.; Vieiros, M.; Ramos-Triguero, A.; Muñoz-Lozano, C.; Navarro-Tapia, E.; Martínez, L.; García-Algar, Ó.; et al. Effect of Postnatal Epigallocatechin-Gallate Treatment on Cardiac Function in Mice Prenatally Exposed to Alcohol. Antioxidants 2023, 12, 1067. [Google Scholar] [CrossRef] [PubMed]
- Montagud-Romero, S.; Cantacorps, L.; Valverde, O. Histone Deacetylases Inhibitor Trichostatin A Reverses Anxiety-like Symptoms and Memory Impairments Induced by Maternal Binge Alcohol Drinking in Mice. J. Psychopharmacol. 2019, 33, 1573–1587. [Google Scholar] [CrossRef] [PubMed]
- Sogut, I.; Uysal, O.; Oglakci, A.; Yucel, F.; Kartkaya, K.; Kanbak, G. Prenatal Alcohol–Induced Neuroapoptosis in Rat Brain Cerebral Cortex: Protective Effect of Folic Acid and Betaine. Childs Nerv. Syst. 2017, 33, 407–417. [Google Scholar] [CrossRef] [PubMed]
- Cadena, P.G.; Cadena, M.R.S.; Sarmah, S.; Marrs, J.A. Folic Acid Reduces the Ethanol-Induced Morphological and Behavioral Defects in Embryonic and Larval Zebrafish (Danio rerio) as a Model for Fetal Alcohol Spectrum Disorder (FASD). Reprod. Toxicol. 2020, 96, 249–257. [Google Scholar] [CrossRef] [PubMed]
- Naseer, M.I.; Ullah, I.; Narasimhan, M.L.; Lee, H.Y.; Bressan, R.A.; Yoon, G.H.; Yun, D.J.; Kim, M.O. Neuroprotective Effect of Osmotin against Ethanol-Induced Apoptotic Neurodegeneration in the Developing Rat Brain. Cell Death Dis. 2014, 5, e1150. [Google Scholar] [CrossRef] [PubMed]
- Wellmann, K.A.; George, F.; Brnouti, F.; Mooney, S.M. Docosahexaenoic Acid Partially Ameliorates Deficits in Social Behavior and Ultrasonic Vocalizations Caused by Prenatal Ethanol Exposure. Behav. Brain Res. 2015, 286, 201–211. [Google Scholar] [CrossRef] [PubMed]
- Sharma, N.; Dhiman, N.; Golani, L.K.; Sharma, B. Papaverine Ameliorates Prenatal Alcohol-induced Experimental Attention Deficit Hyperactivity Disorder by Regulating Neuronal Function, Inflammation, and Oxidative Stress. Int. J. Dev. Neurosci. 2021, 81, 71–81. [Google Scholar] [CrossRef]
- Ju, I.G.; Lee, M.Y.; Jeon, S.H.; Huh, E.; Kim, J.H.; Lee, J.K.; Lee, C.H.; Oh, M.S. GC-TOF-MS-Based Metabolomic Analysis and Evaluation of the Effects of HX106, a Nutraceutical, on ADHD-Like Symptoms in Prenatal Alcohol Exposed Mice. Nutrients 2020, 12, 3027. [Google Scholar] [CrossRef]
- Gibula-Tarlowska, E.; Korz, V.; Lopatynska-Mazurek, M.; Chlopas-Konowalek, A.; Grochecki, P.; Kalaba, P.; Dragacevic, V.; Kotlinski, R.; Kujawski, R.; Szulc, M.; et al. CE-123, a Novel Dopamine Transporter Inhibitor, Attenuates Locomotor Hyperactivity and Improves Cognitive Functions in Rat Model of Fetal Alcohol Spectrum Disorders. Behav. Brain Res. 2021, 410, 113326. [Google Scholar] [CrossRef]
- Wang, X.; Zhang, K.; Yang, F.; Ren, Z.; Xu, M.; Frank, J.A.; Ke, Z.; Luo, J. Minocycline Protects Developing Brain against Ethanol-Induced Damage. Neuropharmacology 2018, 129, 84–99. [Google Scholar] [CrossRef] [PubMed]
- Skorput, A.G.; Lee, S.M.; Yeh, P.W.; Yeh, H.H. The NKCC1 Antagonist Bumetanide Mitigates Interneuronopathy Associated with Ethanol Exposure in Utero. eLife 2019, 8, 48648. [Google Scholar] [CrossRef] [PubMed]
- Ren, Z.; Wang, X.; Xu, M.; Frank, J.A.; Luo, J. Minocycline Attenuates Ethanol-Induced Cell Death and Microglial Activation in the Developing Spinal Cord. Alcohol 2019, 79, 25–35. [Google Scholar] [CrossRef] [PubMed]
- Mohammad, S.; Page, S.J.; Wang, L.; Ishii, S.; Li, P.; Sasaki, T.; Basha, A.; Salzberg, A.; Quezado, Z.; Imamura, F.; et al. Kcnn2 Blockade Reverses Learning Deficits in a Mouse Model of Fetal Alcohol Spectrum Disorders. Nat. Neurosci. 2020, 23, 533–543. [Google Scholar] [CrossRef] [PubMed]
- Almeida-Toledano, L.; Andreu-Fernández, V.; Aras-López, R.; García-Algar, Ó.; Martínez, L.; Gómez-Roig, M.D. Epigallocatechin Gallate Ameliorates the Effects of Prenatal Alcohol Exposure in a Fetal Alcohol Spectrum Disorder-Like Mouse Model. Int. J. Mol. Sci. 2021, 22, 715. [Google Scholar] [CrossRef] [PubMed]
- García-Baos, A.; Puig-Reyne, X.; García-Algar, Ó.; Valverde, O. Cannabidiol Attenuates Cognitive Deficits and Neuroinflammation Induced by Early Alcohol Exposure in a Mice Model. Biomed. Pharmacother. 2021, 141, 111813. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.-H.; Hong, C.-L.; Wang, Y.-T.; Wang, T.-J.; Chen, J.-R. The Effect of Astaxanthin Treatment on the Rat Model of Fetal Alcohol Spectrum Disorders (FASD). Brain Res. Bull. 2022, 183, 57–72. [Google Scholar] [CrossRef]
- Burton, D.F.; Boa-Amponsem, O.M.; Dixon, M.S.; Hopkins, M.J.; Herbin, T.; Toney, S.; Tarpley, M.; Rodriguez, B.V.; Fish, E.W.; Parnell, S.E.; et al. Pharmacological Activation of the Sonic Hedgehog Pathway with a Smoothened Small Molecule Agonist Ameliorates the Severity of Alcohol-induced Morphological and Behavioral Birth Defects in a Zebrafish Model of Fetal Alcohol Spectrum Disorder. J. Neurosci. Res. 2022, 100, 1585–1601. [Google Scholar] [CrossRef]
- Farhadi, L.; Hojati, V.; Khaksari, M.; Vaezi, G. Neuroprotective Effects of Crocin Against Ethanol Neurotoxicity in the Animal Model of Fetal Alcohol Spectrum Disorders. Neurochem. Res. 2022, 47, 1001–1011. [Google Scholar] [CrossRef] [PubMed]
- Gasparyan, A.; Navarro, D.; Navarrete, F.; Austrich-Olivares, A.; Scoma, E.R.; Hambardikar, V.D.; Acosta, G.B.; Solesio, M.E.; Manzanares, J. Cannabidiol Repairs Behavioral and Brain Disturbances in a Model of Fetal Alcohol Spectrum Disorder. Pharmacol. Res. 2023, 188, 106655. [Google Scholar] [CrossRef] [PubMed]
- Coles, C.D.; Kable, J.A.; Keen, C.L.; Lyons Jones, K.; Wertelecki, W.; Granovska, I.V.; Pashtepa, A.O.; Chambers, C.D.; The CIFASD. Dose and Timing of Prenatal Alcohol Exposure and Maternal Nutritional Supplements: Developmental Effects on 6-Month-Old Infants. Matern. Child Health 2015, 19, 2605–2614. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, S.W.; Carter, R.C.; Molteno, C.D.; Meintjes, E.M.; Senekal, M.S.; Lindinger, N.M.; Dodge, N.C.; Zeisel, S.H.; Duggan, C.P.; Jacobson, J.L. Feasibility and Acceptability of Maternal Choline Supplementation in Heavy Drinking Pregnant Women: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial. Alcohol. Clin. Exp. Res. 2018, 42, 1315–1326. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, S.W.; Carter, R.C.; Molteno, C.D.; Stanton, M.E.; Herbert, J.S.; Lindinger, N.M.; Lewis, C.E.; Dodge, N.C.; Hoyme, H.E.; Zeisel, S.H.; et al. Efficacy of Maternal Choline Supplementation During Pregnancy in Mitigating Adverse Effects of Prenatal Alcohol Exposure on Growth and Cognitive Function: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial. Alcohol. Clin. Exp. Res. 2018, 42, 1327–1341. [Google Scholar] [CrossRef]
- Warton, F.L.; Molteno, C.D.; Warton, C.M.R.; Wintermark, P.; Lindinger, N.M.; Dodge, N.C.; Zöllei, L.; van der Kouwe, A.J.W.; Carter, R.C.; Jacobson, J.L.; et al. Maternal Choline Supplementation Mitigates Alcohol Exposure Effects on Neonatal Brain Volumes. Alcohol. Clin. Exp. Res. 2021, 45, 1762–1774. [Google Scholar] [CrossRef]
- Wozniak, J.R.; Fuglestad, A.J.; Eckerle, J.K.; Kroupina, M.G.; Miller, N.C.; Boys, C.J.; Brearley, A.M.; Fink, B.A.; Hoecker, H.L.; Zeisel, S.H.; et al. Choline Supplementation in Children with Fetal Alcohol Spectrum Disorders Has High Feasibility and Tolerability. Nutr. Res. 2013, 33, 897–904. [Google Scholar] [CrossRef]
- Wozniak, J.R.; Fuglestad, A.J.; Eckerle, J.K.; Fink, B.A.; Hoecker, H.L.; Boys, C.J.; Radke, J.P.; Kroupina, M.G.; Miller, N.C.; Brearley, A.M.; et al. Choline Supplementation in Children with Fetal Alcohol Spectrum Disorders: A Randomized, Double-Blind, Placebo-Controlled Trial. Am. J. Clin. Nutr. 2015, 102, 1113–1125. [Google Scholar] [CrossRef]
- Nguyen, T.T.; Risbud, R.D.; Mattson, S.N.; Chambers, C.D.; Thomas, J.D. Choline Supplementation in School-Aged Children With Fetal Alcohol Spectrum Disorders. Am. J. Clin. Nutr. 2016, 104, 1683–1692. [Google Scholar] [CrossRef]
- Sarkar, D.K.; Gangisetty, O.; Wozniak, J.R.; Eckerle, J.K.; Georgieff, M.K.; Foroud, T.M.; Wetherill, L.; Wertelecki, W.; Chambers, C.D.; Riley, E.; et al. Persistent Changes in Stress-Regulatory Genes in Pregnant Women or Children Exposed Prenatally to Alcohol. Alcohol. Clin. Exp. Res. 2019, 43, 1887–1897. [Google Scholar] [CrossRef]
- Wozniak, J.R.; Fink, B.A.; Fuglestad, A.J.; Eckerle, J.K.; Boys, C.J.; Sandness, K.E.; Radke, J.P.; Miller, N.C.; Lindgren, C.; Brearley, A.M.; et al. Four-Year Follow-up of a Randomized Controlled Trial of Choline for Neurodevelopment in Fetal Alcohol Spectrum Disorder. J. Neurodev. Disord. 2020, 12, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Gimbel, B.A.; Anthony, M.E.; Ernst, A.M.; Roediger, D.J.; de Water, E.; Eckerle, J.K.; Boys, C.J.; Radke, J.P.; Mueller, B.A.; Fuglestad, A.J.; et al. Long-Term Follow-up of a Randomized Controlled Trial of Choline for Neurodevelopment in Fetal Alcohol Spectrum Disorder: Corpus Callosum White Matter Microstructure and Neurocognitive Outcomes. J. Neurodev. Disord. 2022, 14, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Oesterheld, J.R.; Kofoed, L.; Tervo, R.; Fogas, B.; Wilson, A.; Fiechtner, H. Effectiveness of Methylphenidate in Native American Children with Fetal Alcohol Syndrome and Attention Deficit/Hyperactivity Disorder: A Controlled Pilot Study. J. Child Adolesc. Psychopharmacol. 1998, 8, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Doig, J.; McLennan, J.D.; Gibbard, W.B. Medication Effects on Symptoms of Attention-Deficit/Hyperactivity Disorder in Children with Fetal Alcohol Spectrum Disorder. J. Child Adolesc. Psychopharmacol. 2008, 18, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Peadon, E.; Thomas, D.E.; Elliott, E.J. Pharmacological Interventions for ADHD Symptoms in Children with Fetal Alcohol Spectrum Disorders (FASD). Cochrane Database Syst. Rev. 2017, CD009724. [Google Scholar] [CrossRef]
- Frankel, F.; Paley, B.; Marquardt, R.; O’Connor, M. Stimulants, Neuroleptics, and Children’s Friendship Training for Children with Fetal Alcohol Spectrum Disorders. J. Child Adolesc. Psychopharmacol. 2006, 16, 777–789. [Google Scholar] [CrossRef]
- Mela, M.; Okpalauwaekwe, U.; Anderson, T.; Eng, J.; Nomani, S.; Ahmed, A.; Barr, A.M. The Utility of Psychotropic Drugs on Patients with Fetal Alcohol Spectrum Disorder (FASD): A Systematic Review. Psychiatry Clin. Psychopharmacol. 2018, 28, 436–445. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andreu-Fernández, V.; La Maida, N.; Marquina, M.; Mirahi, A.; García-Algar, O.; Pichini, S.; Minutillo, A. Novel Interventions on Comorbidities in Patients with Fetal Alcohol Spectrum Disorder (FASD): An Integrative Review. Biomedicines 2024, 12, 496. https://doi.org/10.3390/biomedicines12030496
Andreu-Fernández V, La Maida N, Marquina M, Mirahi A, García-Algar O, Pichini S, Minutillo A. Novel Interventions on Comorbidities in Patients with Fetal Alcohol Spectrum Disorder (FASD): An Integrative Review. Biomedicines. 2024; 12(3):496. https://doi.org/10.3390/biomedicines12030496
Chicago/Turabian StyleAndreu-Fernández, Vicente, Nunzia La Maida, Maribel Marquina, Afrouz Mirahi, Oscar García-Algar, Simona Pichini, and Adele Minutillo. 2024. "Novel Interventions on Comorbidities in Patients with Fetal Alcohol Spectrum Disorder (FASD): An Integrative Review" Biomedicines 12, no. 3: 496. https://doi.org/10.3390/biomedicines12030496
APA StyleAndreu-Fernández, V., La Maida, N., Marquina, M., Mirahi, A., García-Algar, O., Pichini, S., & Minutillo, A. (2024). Novel Interventions on Comorbidities in Patients with Fetal Alcohol Spectrum Disorder (FASD): An Integrative Review. Biomedicines, 12(3), 496. https://doi.org/10.3390/biomedicines12030496