

Muscle Dysfunction and Functional Status in COVID-19 Patients during Illness and after Hospital Discharge

Abstract
1. Background
2. Methods
2.1. Data Collection, Patients—Ethics, Enrolment Criteria
2.2. Study Protocol
2.3. Ultrasonography
2.4. Statistical Analysis
3. Results
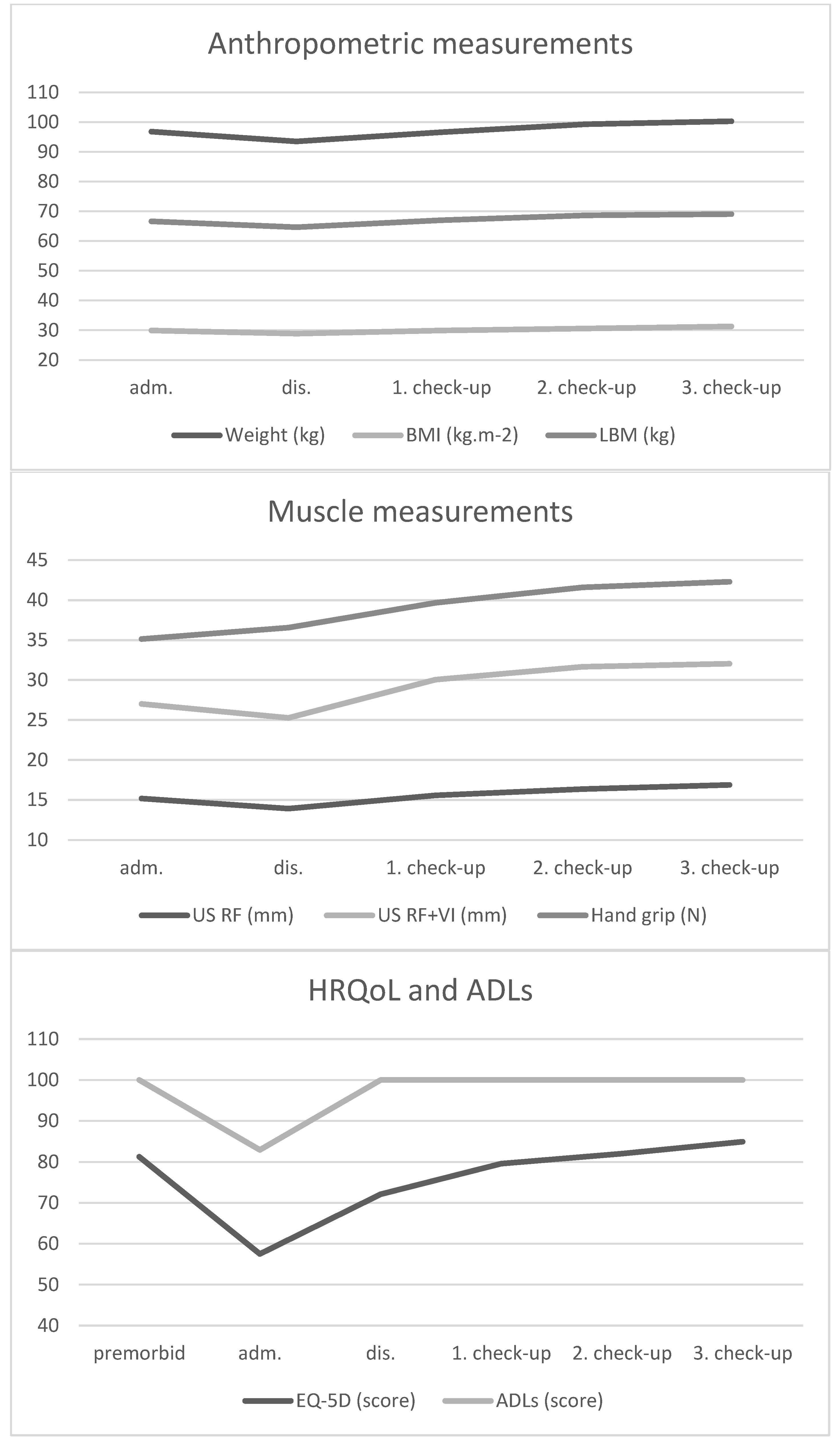
3.1. Change of Monitored Parameters during Hospitalization and Follow-Up
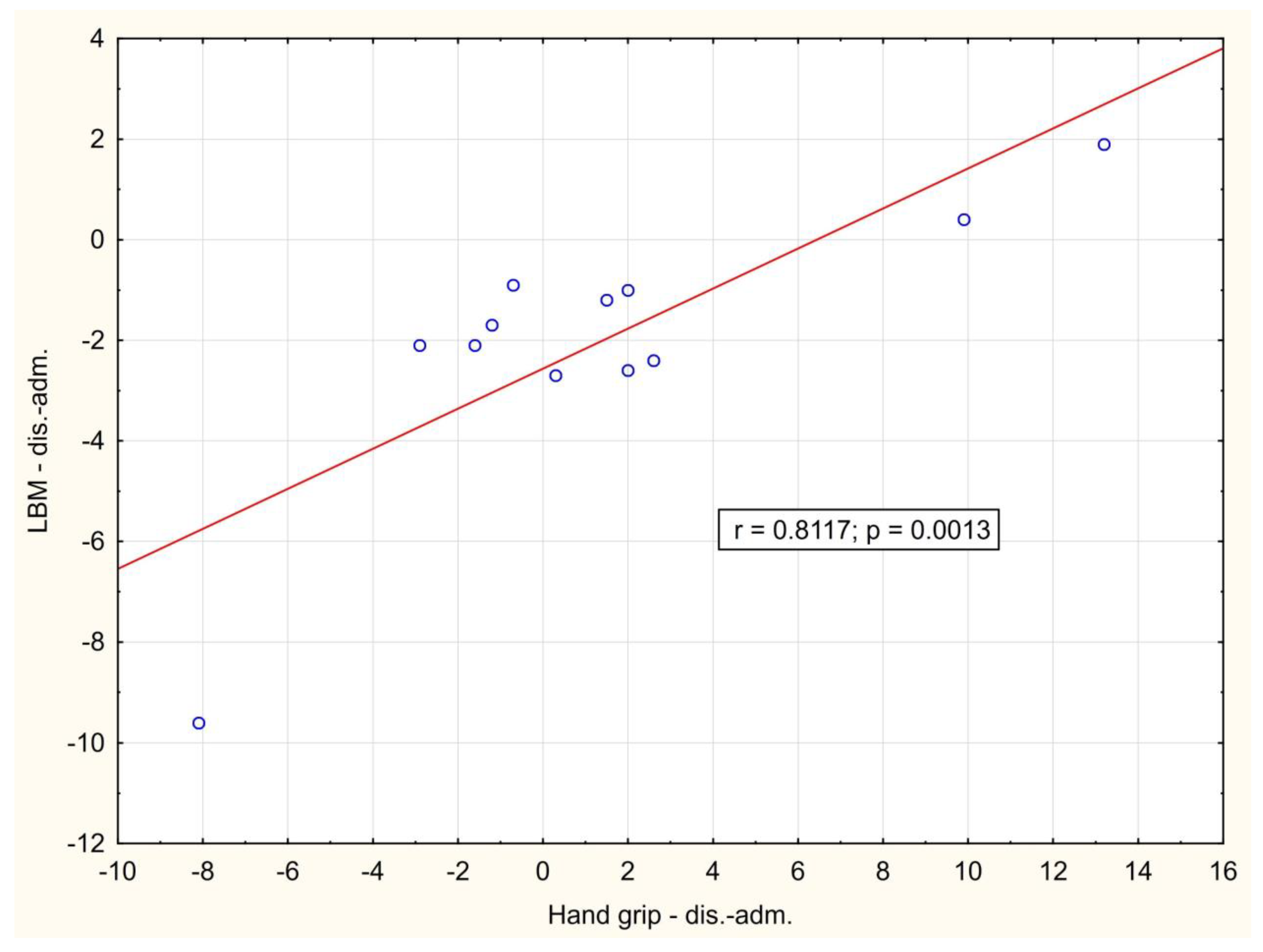
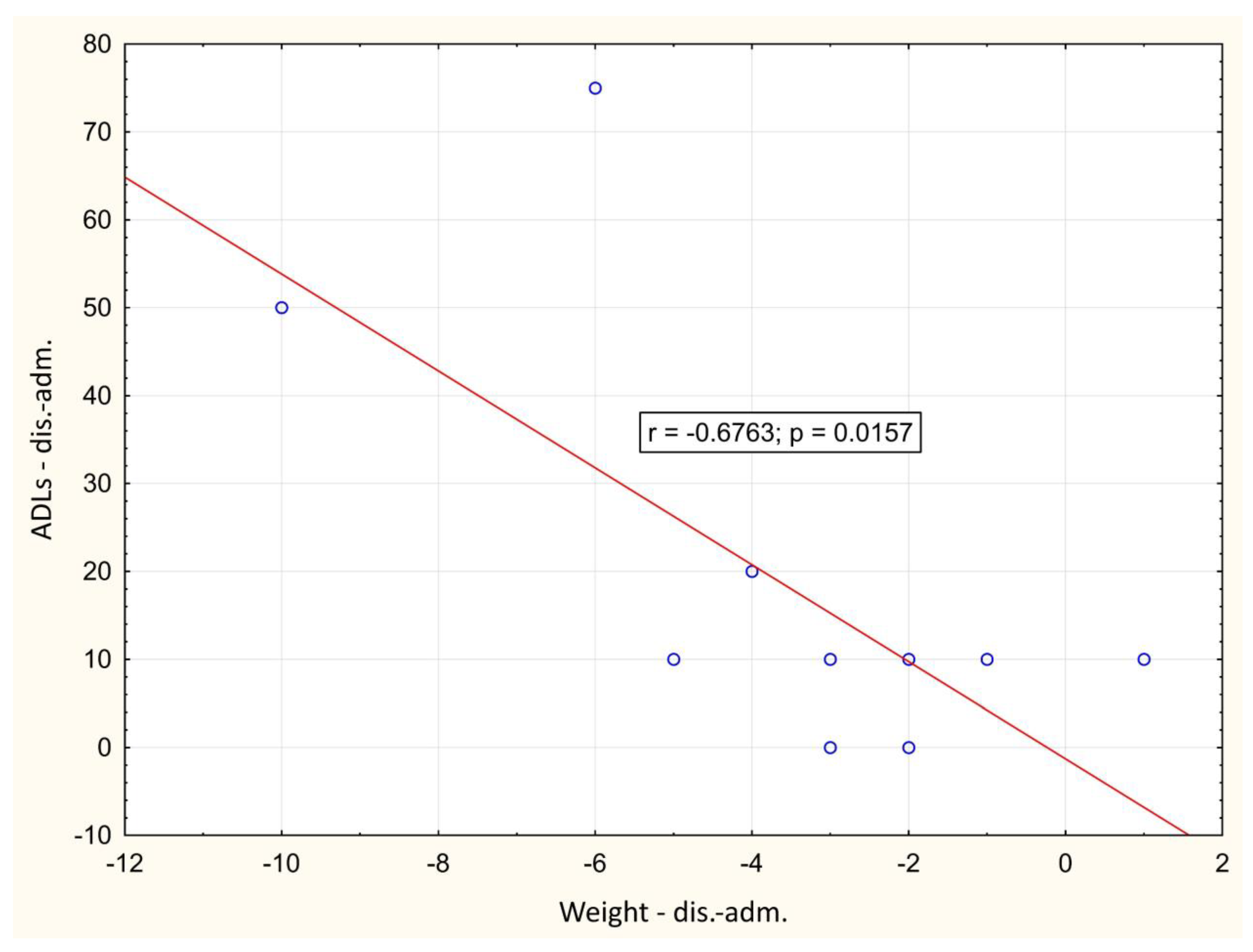
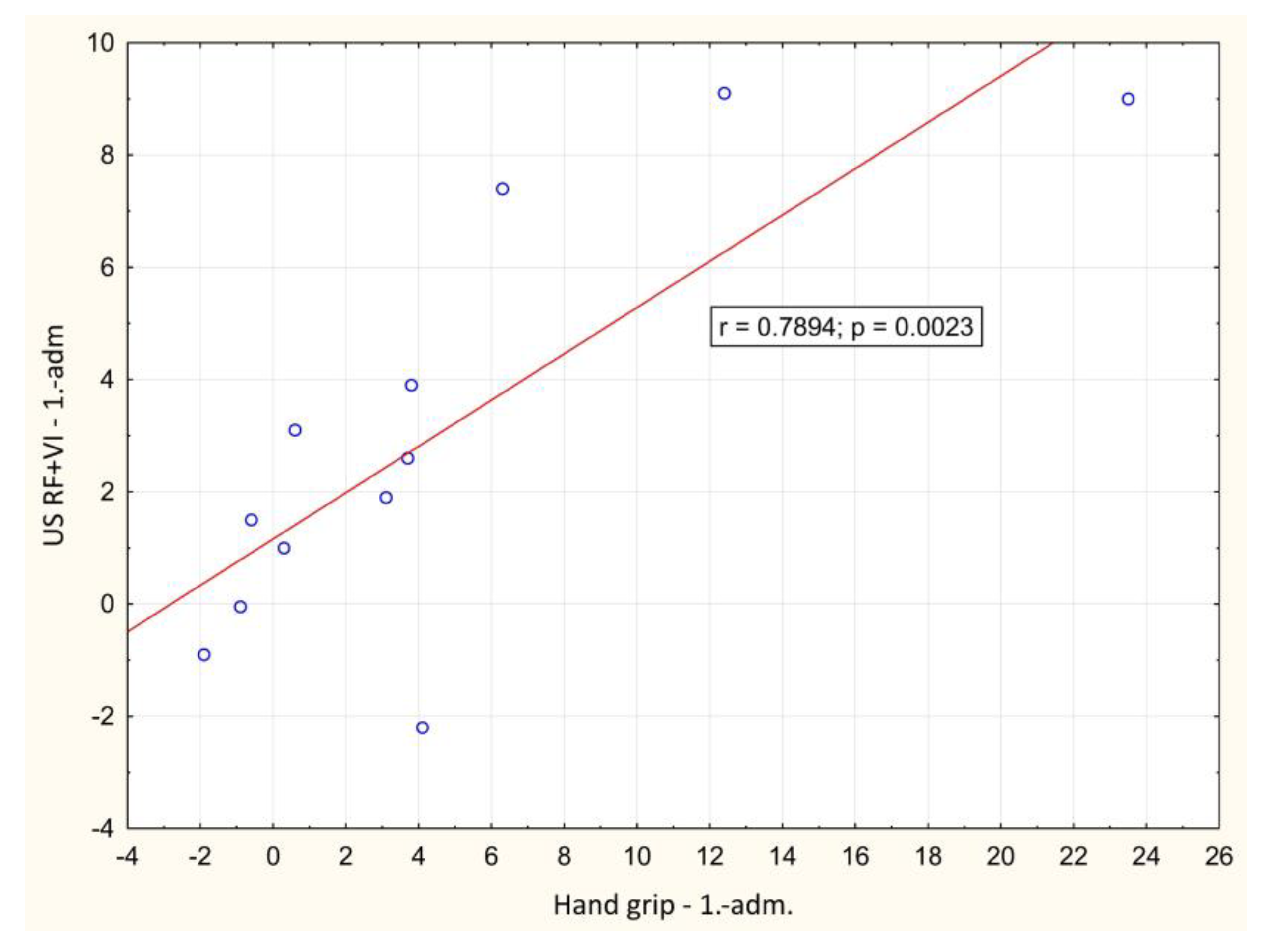
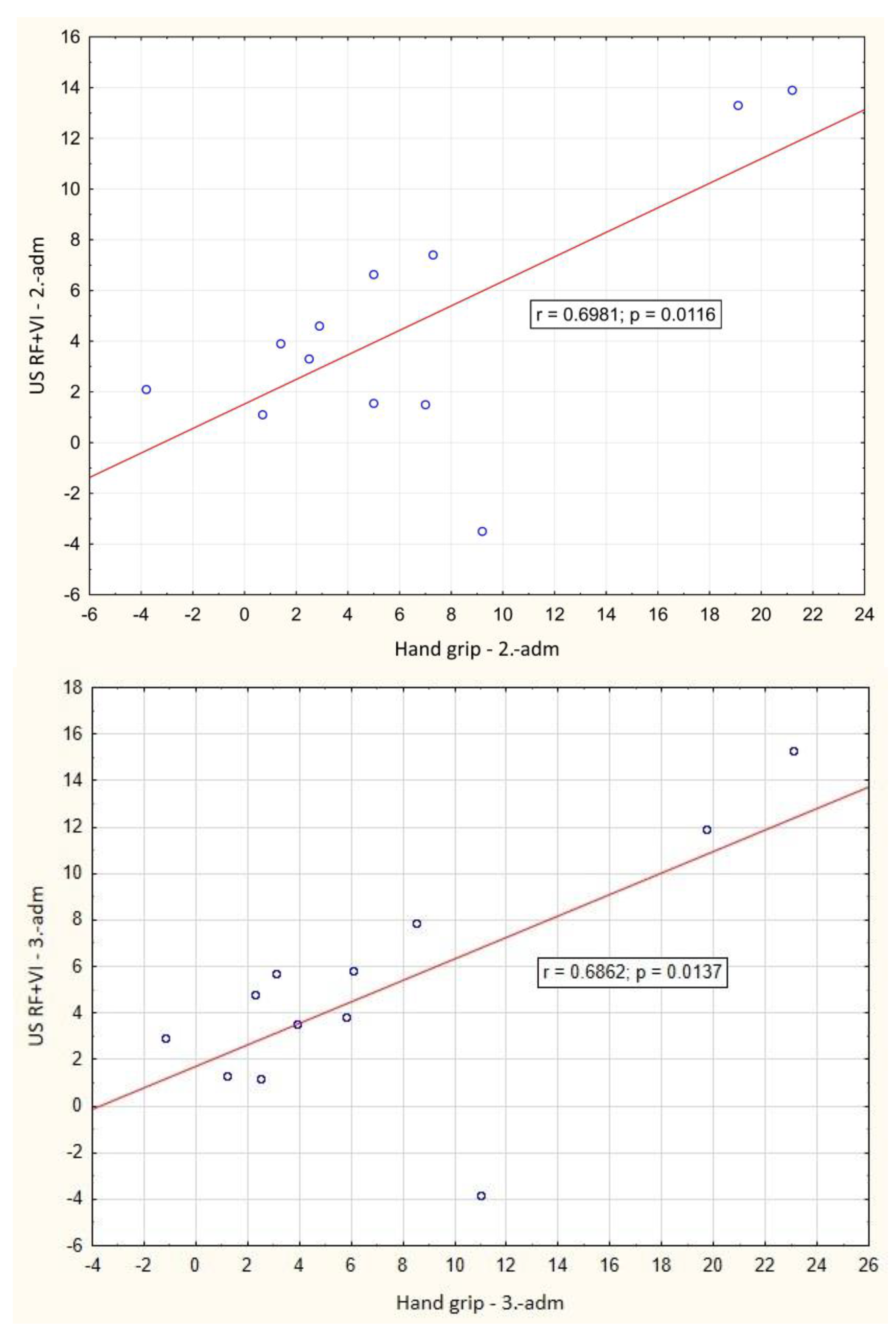
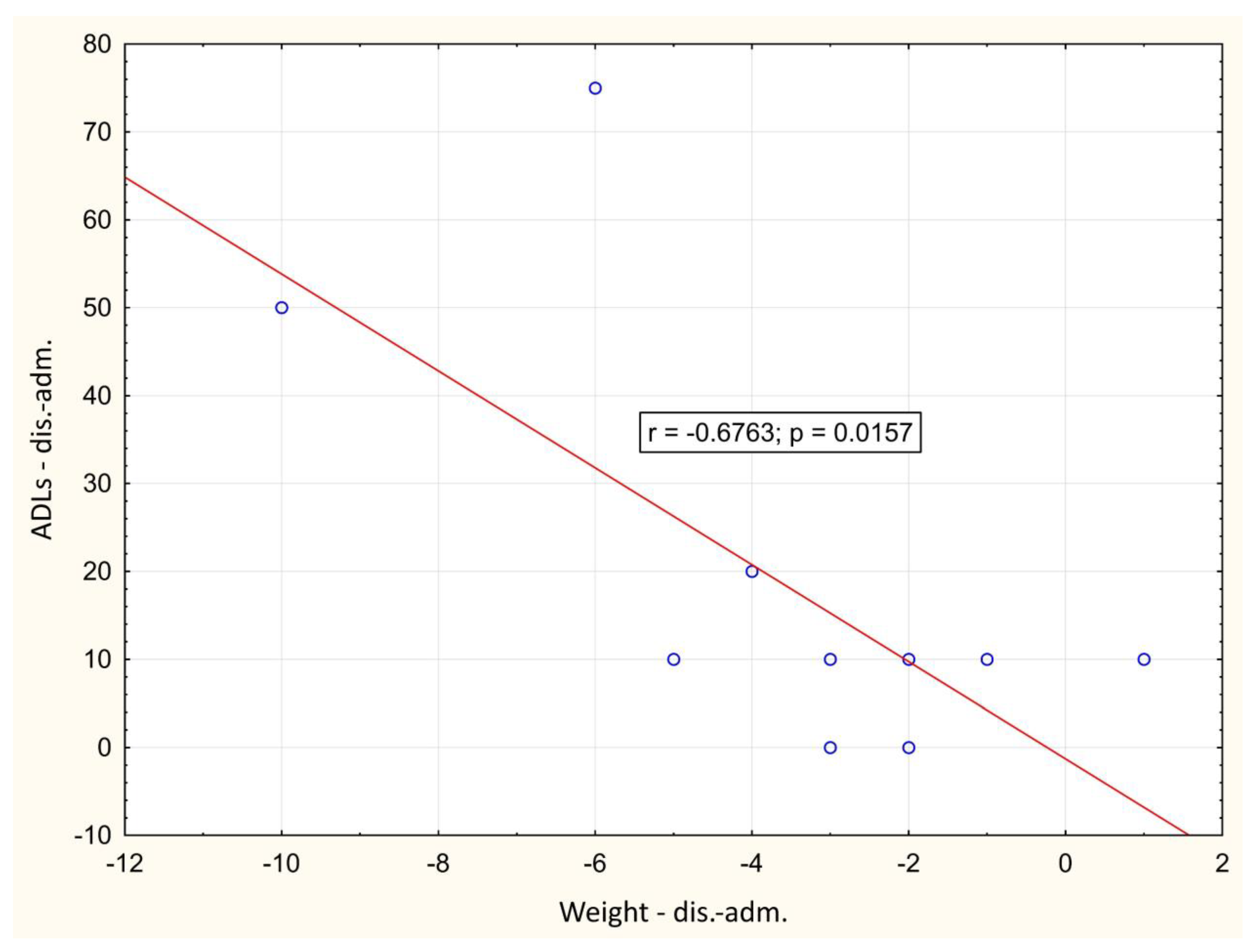
3.2. Correlation between Monitored Parameters
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pascarella, G.; Strumia, A.; Piliego, C.; Bruno, F.; Del Buono, R.; Costa, F.; Scarlata, S.; Agrò, F.E. COVID-19 diagnosis and management: A comprehensive review. J. Intern. Med. 2020, 288, 192–206. [Google Scholar] [CrossRef] [PubMed]
- Anka, A.U.; Tahir, M.I.; Abubakar, S.D.; Alsabbagh, M.; Zian, Z.; Hamedifar, H.; Sabzevari, A.; Azizi, G. Coronavirus disease 2019 (COVID-19): An overview of the immunopathology, serological diagnosis and management. Scand. J. Immunol. 2021, 93, e12998. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. China Medical Treatment Expert Group for Covid-19. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Li, X.; Gu, X.; Zhang, H.; Ren, L.; Guo, L.; Liu, M.; Wang, Y.; Cui, D.; Wang, Y.; et al. Health outcomes in people 2 years after surviving hospitalisation with COVID-19: A longitudinal cohort study. Lancet Respir. Med. 2022, 10, 863–876. [Google Scholar] [CrossRef] [PubMed]
- Carod-Artal, F.J. Post-COVID-19 syndrome: Epidemiology, diagnostic criteria and pathogenic mechanisms involved. Rev. Neurol. 2021, 72, 384–396. (In Spanish) [Google Scholar] [CrossRef] [PubMed]
- Malik, P.; Patel, K.; Pinto, C.; Jaiswal, R.; Tirupathi, R.; Pillai, S.; Patel, U. Post-acute COVID-19 syndrome (PCS) and health-related quality of life (HRQoL)—A systematic review and meta-analysis. J. Med. Virol. 2022, 94, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Di Filippo, L.; De Lorenzo, R.; D’Amico, M.; Sofia, V.; Roveri, L.; Mele, R.; Saibene, A.; Rovere-Querini, P.; Conte, C. COVID-19 is associated with clinically significant weight loss and risk of malnutrition, independent of hospitalisation: A post-hoc analysis of a prospective cohort study. Clin. Nutr. 2021, 40, 2420–2426. [Google Scholar] [CrossRef]
- Wierdsma, N.J.; Kruizenga, H.M.; Konings, L.A.; Krebbers, D.; Jorissen, J.R.; Joosten, M.-H.I.; van Aken, L.H.; Tan, F.M.; van Bodegraven, A.A.; Soeters, M.R.; et al. Poor nutritional status, risk of sarcopenia and nutrition related complaints are prevalent in COVID-19 patients during and after hospital admission. Clin. Nutr. ESPEN 2021, 43, 369–376. [Google Scholar] [CrossRef]
- Beaudart, C.; Zaaria, M.; Pasleau, F.; Reginster, J.-Y.; Bruyère, O. Health Outcomes of Sarcopenia: A Systematic Review and Meta-Analysis. PLoS ONE 2017, 12, e0169548. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Buckinx, F.; Landi, F.; Cesari, M.; Fielding, R.A.; Visser, M.; Engelke, K.; Maggi, S.; Dennison, E.; Al-Daghri, N.M.; Allepaerts, S.; et al. Pitfalls in the measurement of muscle mass: A need for a reference standard. J. Cachexia Sarcopenia Muscle 2018, 9, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Looijaard, W.G.; Molinger, J.; Weijs, P.J. Measuring and monitoring lean body mass in critical illness. Curr. Opin. Crit. Care 2018, 24, 241–247. [Google Scholar] [CrossRef] [PubMed]
- De Rosa, S.; Umbrello, M.; Pelosi, P.; Battaglini, D. Update on Lean Body Mass Diagnostic Assessment in Critical Illness. Diagnostics 2023, 13, 888. [Google Scholar] [CrossRef] [PubMed]
- Perkisas, S.; Bastijns, S.; Baudry, S.; Bauer, J.; Beaudart, C.; Beckwée, D.; Cruz-Jentoft, A.; Gasowski, J.; Hobbelen, H.; Jager-Wittenaar, H.; et al. Application of ultrasound for muscle assessment in sarcopenia: 2020 SARCUS update. Eur. Geriatr. Med. 2021, 12, 45–59. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Wu, J.; Gu, Q.; Gu, Y.; Zhao, Y.; Ge, X.; Sun, X.; Lian, J.; Zeng, Q. Changes in muscle ultrasound for the diagnosis of intensive care unit acquired weakness in critically ill patients. Sci. Rep. 2021, 11, 18280. [Google Scholar] [CrossRef] [PubMed]
- Tillquist, M.; Kutsogiannis, D.J.; Wischmeyer, P.E.; Kummerlen, C.; Leung, R.; Stollery, D.; Karvellas, C.J.; Preiser, J.; Bird, N.; Kozar, R.; et al. Bedside Ultrasound Is a Practical and Reliable Measurement Tool for Assessing Quadriceps Muscle Layer Thickness. J. Parenter. Enter. Nutr. 2013, 38, 886–890. [Google Scholar] [CrossRef] [PubMed]
- Hadda, V.; Kumar, R.; Khilnani, G.C.; Kalaivani, M.; Madan, K.; Tiwari, P.; Mittal, S.; Mohan, A.; Bhalla, A.S.; Guleria, R. Trends of loss of peripheral muscle thickness on ultrasonography and its relationship with outcomes among patients with sepsis. J. Intensive Care 2018, 6, 81. [Google Scholar] [CrossRef]
- Umbrello, M.; Guglielmetti, L.; Formenti, P.; Antonucci, E.; Cereghini, S.; Filardo, C.; Montanari, G.; Muttini, S. Qualitative and quantitative muscle ultrasound changes in patients with COVID-19–related ARDS. Nutrition 2021, 91–92, 111449. [Google Scholar] [CrossRef]
- Damanti, S.; Cilla, M.; Tuscano, B.; De Lorenzo, R.; Manganaro, G.; Merolla, A.; Pacioni, G.; Pomaranzi, C.; Tiraferri, V.; Martinenghi, S.; et al. Evaluation of Muscle Mass and Stiffness with Limb Ultrasound in COVID-19 Survivors. Front. Endocrinol. 2022, 13, 801133. [Google Scholar] [CrossRef]
- Martín, C.A.G.; Zepeda, E.M.; Méndez, O.A.L. Bedside Ultrasound Measurement of Rectus Femoris: A Tutorial for the Nutrition Support Clinician. J. Nutr. Metab. 2017, 2017, 2767232. [Google Scholar] [CrossRef]
- Puthucheary, Z.A.; Rawal, J.; McPhail, M.; Connolly, B.; Ratnayake, G.; Chan, P.; Hopkinson, N.S.; Padhke, R.; Dew, T.; Sidhu, P.S.; et al. Acute Skeletal Muscle Wasting in Critical Illness. JAMA 2013, 310, 1591–1600. [Google Scholar] [CrossRef] [PubMed]
- Koratala, A.; Ronco, C.; Kazory, A. Diagnosis of Fluid Overload: From Conventional to Contemporary Concepts. Cardiorenal Med. 2022, 12, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Moonen, H.P.F.X.; Van Zanten, A.R.H. Bioelectric impedance analysis for body composition measurement and other potential clinical applications in critical illness. Curr. Opin. Crit. Care 2021, 27, 344–353. [Google Scholar] [CrossRef] [PubMed]
- Peolsson, A.; Hedlund, R.; Öberg, B. Intra-and inter-tester reliability and reference values for hand strength. J. Rehabil. Med. 2001, 33, 36–41. [Google Scholar] [CrossRef]
- Bittner, E.A.; Martyn, J.A.; George, E.; Frontera, W.R.; Eikermann, M. Measurement of muscle strength in the intensive care unit. Crit. Care Med. 2009, 37, S321–S330. [Google Scholar] [CrossRef] [PubMed]
- Cottereau, G.; Messika, J.; Megarbane, B.; Guérin, L.; da Silva, D.; Bornstain, C.; Santos, M.; Ricard, J.-D.; Sztrymf, B. Handgrip strength to predict extubation outcome: A prospective multicenter trial. Ann. Intensiv. Care 2021, 11, 144. [Google Scholar] [CrossRef]
- Mayer, K.P.; Bastin, M.L.T.; Montgomery-Yates, A.A.; Pastva, A.M.; Dupont-Versteegden, E.E.; Parry, S.M.; Morris, P.E. Acute skeletal muscle wasting and dysfunction predict physical disability at hospital discharge in patients with critical illness. Crit. Care 2020, 24, 637. [Google Scholar] [CrossRef] [PubMed]
- Soares, M.N.; Eggelbusch, M.; Naddaf, E.; Gerrits, K.H.L.; van der Schaaf, M.; van den Borst, B.; Wiersinga, W.J.; van Vugt, M.; Weijs, P.J.M.; Murray, A.J.; et al. Skeletal muscle alterations in patients with acute Covid-19 and post-acute sequelae of Covid-19. J. Cachex. Sarcopenia Muscle 2022, 13, 11–22. [Google Scholar] [CrossRef]
- Sanaie, S.; Hosseini, M.-S.; Karrubi, F.; Iranpour, A.; Mahmoodpoor, A. Impact of Body Mass Index on the Mortality of Critically Ill Patients Admitted to the Intensive Care Unit: An Observational Study. Anesthesiol. Pain Med. 2020, 11, e108561. [Google Scholar] [CrossRef]
- Prescott, H.C.; Chang, V.W.; O’Brien, J.M., Jr.; Langa, K.M.; Iwashyna, T.J. Obesity and 1-Year Outcomes in Older Americans with Severe Sepsis. Crit. Care Med. 2014, 42, 1766–1774. [Google Scholar] [CrossRef]
- Akinnusi, M.E.; Pineda, L.A.; El Solh, A.A. Effect of obesity on intensive care morbidity and mortality: A meta-analysis. Crit. Care Med. 2008, 36, 151–158. [Google Scholar] [CrossRef]
- de Leeuw, A.J.M.; Luttikhuis, M.A.M.O.; Wellen, A.C.; Müller, C.; Calkhoven, C.F. Obesity and its impact on COVID-19. J. Mol. Med. 2021, 99, 899–915. [Google Scholar] [CrossRef] [PubMed]
- Ponti, G.; Maccaferri, M.; Ruini, C.; Tomasi, A.; Ozben, T. Biomarkers associated with COVID-19 disease progression. Crit. Rev. Clin. Lab. Sci. 2020, 57, 389–399. [Google Scholar] [CrossRef]
- Bivona, G.; Agnello, L.; Ciaccio, M. Biomarkers for Prognosis and Treatment Response in COVID-19 Patients. Ann. Lab. Med. 2021, 41, 540–548. [Google Scholar] [CrossRef] [PubMed]
- Paces, J.; Strizova, Z.; Smrz, D.; Cerny, J. COVID-19 and the Immune System. Physiol. Res. 2020, 69, 379–388. [Google Scholar] [CrossRef] [PubMed]
- McGonagle, D.; Sharif, K.; O’Regan, A.; Bridgewood, C. The Role of Cytokines including Interleukin-6 in COVID-19 induced Pneumonia and Macrophage Activation Syndrome-Like Disease. Autoimmun. Rev. 2020, 19, 102537. [Google Scholar] [CrossRef] [PubMed]
- Zeng, F.; Huang, Y.; Guo, Y.; Yin, M.; Chen, X.; Xiao, L.; Deng, G. Association of inflammatory markers with the severity of COVID-19: A meta-analysis. Int. J. Infect. Dis. 2020, 96, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Annetta, M.G.; Pittiruti, M.; Silvestri, D.; Grieco, D.L.; Maccaglia, A.; La Torre, M.F.; Magarelli, N.; Mercurio, G.; Caricato, A.; Antonelli, M. Ultrasound assessment of rectus femoris and anterior tibialis muscles in young trauma patients. Ann. Intensive Care 2017, 7, 104. [Google Scholar] [CrossRef] [PubMed]
- Parry, S.M.; Burtin, C.; Denehy, L.; Puthucheary, Z.A.; Bear, D. Ultrasound Evaluation of Quadriceps Muscle Dysfunction in Respiratory Disease. Cardiopulm. Phys. Ther. J. 2019, 30, 15–23. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 16) | |
|---|---|
| Sex | Male (n = 13), Female (n = 3) |
| Age (years) | 64 ± 9.5 |
| Length of hospital stay (days) | 15.9 ± 7.1 |
| Delay from symptoms onset to hospital admission (days) | 10.6 ± 3.4 |
| Weight (kg) | 96.83 ± 10.2 |
| BMI (kg m−2) | 29.93 ± 2.4 |
| Hand grip strength (N) | 35.13 ± 8.9 |
| US RF (mm) | 15.19 ± 3.9 |
| US RF+VI (mm) | 27.01 ± 6.3 |
| LBM (kg) | 66.66 ± 8.7 |
| EQ-5D | 57.50 ± 20.1 |
| ADLs | 82.92 ± 22.6 |
| CRP (mg/L) | 128.70 ± 51.6 |
| Albumin (g/L) | 28.52 ± 4 |
| NLR | 8.03 ± 2.8 |
| AVG (adm.) | AVG (dis.) | AVG (1. Check-Up) | AVG (2. Check-Up) | AVG (3. Check-Up) | |
|---|---|---|---|---|---|
| Weight (kg) | 96.83 ± 10.2 | 93.50 ± 9.92 * | 96.59 ± 9.58 * | 99.33 ± 10.55 | 100.28 ± 10.82 |
| BMI (kg m−2) | 29.93 ± 2.4 | 28.88 ± 2.4 * | 29.96 ± 2.17 * | 30.65 ± 2.25 | 31.29 ± 2.74 |
| Hand grip (N) | 35.13 ± 8.9 | 36.55 ± 6.7 | 39.67 ± 6.9 * | 41.59 ± 7.2 | 42.30 ± 7.0 |
| US RF (mm) | 15.19 ± 3.9 | 13.91 ± 2.8 * | 15.55 ± 2.6 * | 16.36 ± 2.5 | 16.87 ± 2.3 |
| US RF + VI (mm) | 27.01 ± 6.3 | 25.26 ± 5.3 * | 30.04 ± 5.7 * | 31.66 ± 5.5 | 32.04 ± 5.6 |
| LBM (kg) | 66.66 ± 8.7 | 64.66 ± 8.7 * | 67.05 ± 8.4 * | 68.66 ± 8.9 | 69.06 ± 9.5 |
| EQ-5D | 57.50 ± 20.1 | 72.08 ± 12.4 * | 79.58 ± 8.6 | 82.00 ± 11.0 | 84.92 ± 8.6 |
| ADLs | 82.92 ± 22.6 | 100.00 ± 0 * | 100.00 ± 0 | 100.00 ± 0 | 100.00 ± 0 |
| CRP (mg/L) | 128.70 ± 51.6 | 15.59 ± 26.2 * | 3.18 ± 2.0 | 10.86 ± 30.9 | 6.90 ± 17.3 |
| Albumin (g/L) | 28.52 ± 4 | 28.52 ± 7.1 | 44.23 ± 6.5 * | 46.39 ± 2.9 | 45.40 ± 2.4 |
| NLR | 8.03 ± 2.8 | 3.31 ± 2.6 * | 1.68 ± 1.0 | 1.87 ± 0.9 | 1.93 ± 0.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Psenicka, O.; Brutvan, T.; Kratky, J.; Krizova, J. Muscle Dysfunction and Functional Status in COVID-19 Patients during Illness and after Hospital Discharge. Biomedicines 2024, 12, 460. https://doi.org/10.3390/biomedicines12020460
Psenicka O, Brutvan T, Kratky J, Krizova J. Muscle Dysfunction and Functional Status in COVID-19 Patients during Illness and after Hospital Discharge. Biomedicines. 2024; 12(2):460. https://doi.org/10.3390/biomedicines12020460
Chicago/Turabian StylePsenicka, Otakar, Tomas Brutvan, Jan Kratky, and Jarmila Krizova. 2024. "Muscle Dysfunction and Functional Status in COVID-19 Patients during Illness and after Hospital Discharge" Biomedicines 12, no. 2: 460. https://doi.org/10.3390/biomedicines12020460
APA StylePsenicka, O., Brutvan, T., Kratky, J., & Krizova, J. (2024). Muscle Dysfunction and Functional Status in COVID-19 Patients during Illness and after Hospital Discharge. Biomedicines, 12(2), 460. https://doi.org/10.3390/biomedicines12020460