

Could Children’s Myopization Have Been Avoided during the Pandemic Confinement? The Conjunctival Ultraviolet Autofluorescence (CUVAF) Biomarker as an Answer

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Ethics Approval
2.2. Inclusion and Exclusion Criteria
2.3. Data Collection
2.4. Statistical Analyses
3. Results
3.1. Characteristics of the Study Sample
3.2. Association between Baseline Refractive Error and Outdoor Activities (Measured by CUVAF and Questionnaires)
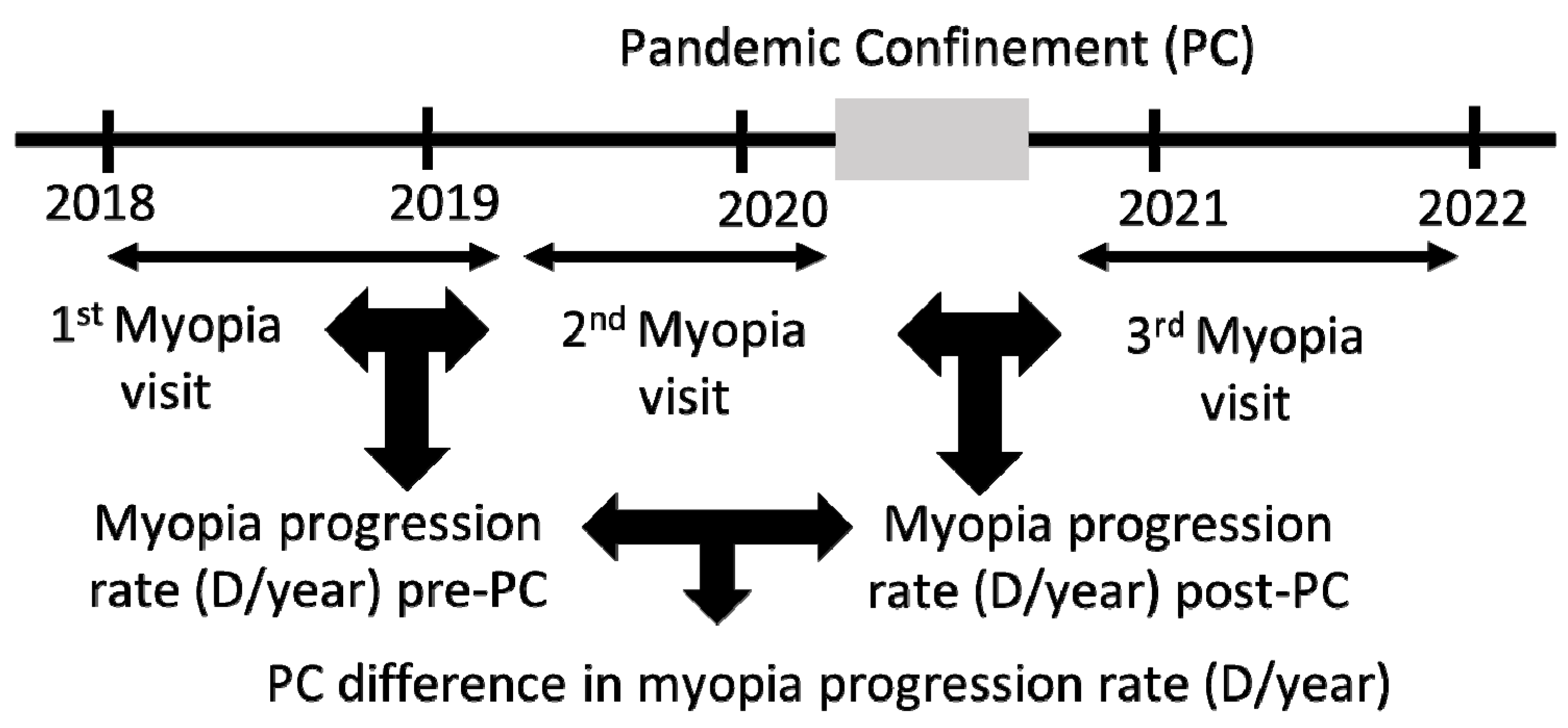
3.3. Rate of Myopia Progression
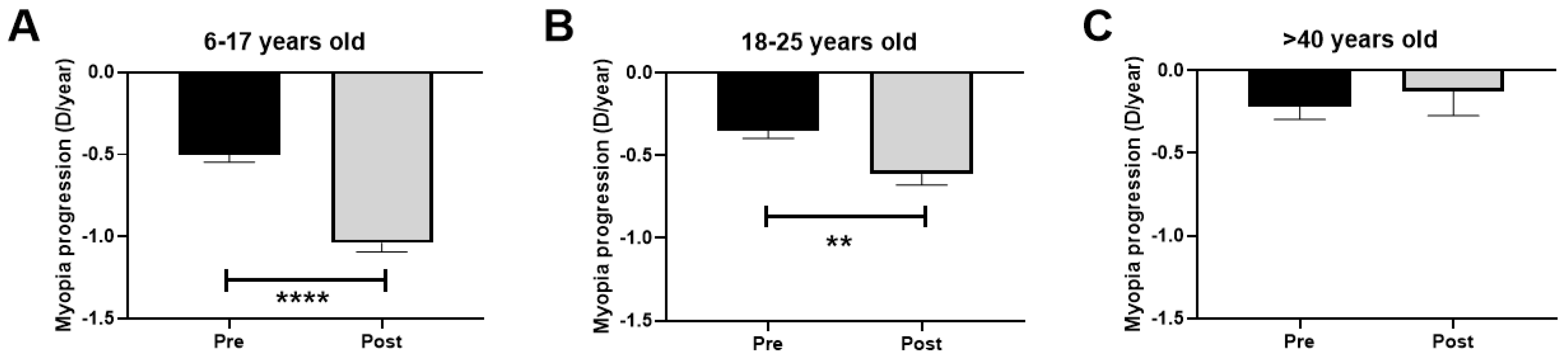
3.4. Difference in Myopia Progression Rate in Children and Young Adults after COVID-19 Confinement in Relation to Outdoor Activities (Measured by CUVAF)
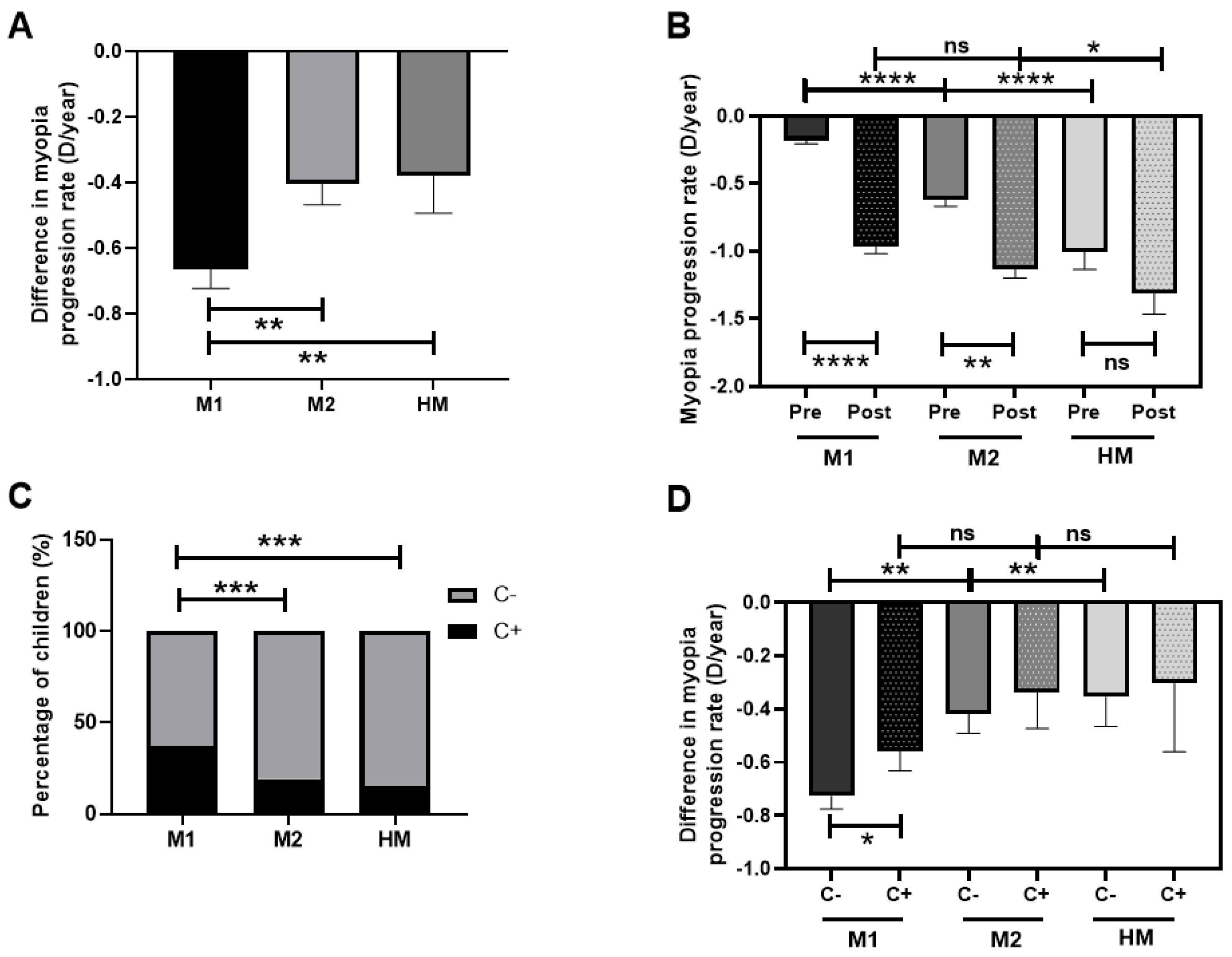
3.5. Myopia Progression Rate after COVID-19 Confinement Regarding Myopia Classification and Outdoor Activities (Measured by CUVAF) in Children
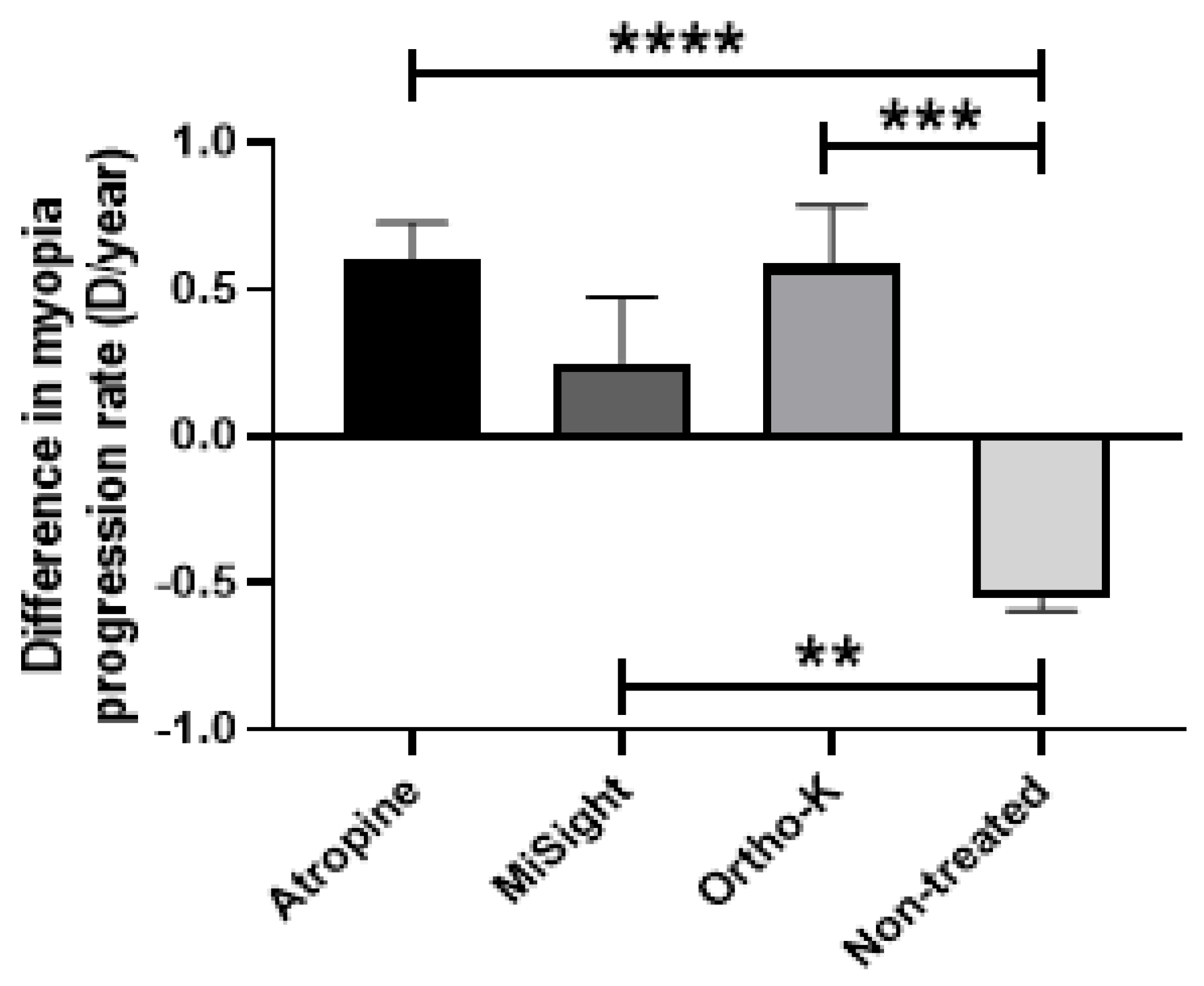
3.6. Difference in Myopia Progression Rate after COVID-19 Confinement Regarding Different Types of Myopia Treatments in Children
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Herranz Guillén, J.L. Nicholas Wade. In Una Herencia Incómoda: Genes, Raza e Historia Humana; Ariel: Barcelona, Spain, 2015; 295p, ISBN 978-84-344-1925-4. [Google Scholar]
- Sherwin, J.C.; McKnight, C.M.; Hewitt, A.W.; Griffiths, L.R.; Coroneo, M.T.; Mackey, D.A. Reliability and validity of conjunctival ultraviolet autofluorescence measurement. Br. J. Ophthalmol. 2012, 96, 801–805. [Google Scholar] [CrossRef]
- Monici, M. Cell and tissue autofluorescence research and diagnostic applications. Biotechnol. Annu. Rev. 2005, 11, 227–256. [Google Scholar]
- Haworth, K.M.; Chandler, H.L. Seasonal Effect on Ocular Sun Exposure and Conjunctival UV Autofluorescence. Optom. Vis. Sci. 2017, 94, 219–228. [Google Scholar] [CrossRef]
- Wolffsohn, J.S.; Drew, T.; Sulley, A. Conjunctival UV autofluorescence—Prevalence and risk factors. Contact Lens Anterior Eye 2014, 37, 427–430. [Google Scholar] [CrossRef]
- Gutierrez Rodriguez, N.; Ortega Claici, A.; Ramos Castañeda, J.A.; González-Zamora, J.; Bilbao-Malavé, V.; de la Puente, M.; Fernandez-Robredo, P.; Garzón-Parra, S.J.; Garza-Leon, M.; Recalde, S. Conjunctival ultraviolet autofluorescence as a biomarker of outdoor exposure in myopia: A systematic review and meta-analysis. Sci. Rep. 2024, 14, 1097. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Li, Y.; Musch, D.C.; Wei, N.; Qi, X.; Ding, G.; Li, X.; Li, J.; Song, L.; Zhang, Y.; et al. Progression of Myopia in School-Aged Children after COVID-19 Home Confinement. JAMA Ophthalmol. 2021, 139, 293–300. [Google Scholar] [CrossRef] [PubMed]
- Soriano, V.; Ganado-Pinilla, P.; Sanchez-Santos, M.; Gómez-Gallego, F.; Barreiro, P.; de Mendoza, C.; Corral, O. Main differences between the first and second waves of COVID-19 in Madrid, Spain. Int. J. Infect. Dis. 2021, 105, 374–376. [Google Scholar] [CrossRef] [PubMed]
- Griffin, D.O.; Brennan-Rieder, D.; Ngo, B.; Kory, P.; Confalonieri, M.; Shapiro, L.; Iglesias, J.; Dube, M.; Nanda, N.; In, G.K.; et al. The Importance of Understanding the Stages of COVID-19 in Treatment and Trials. AIDS Rev. 2021, 23, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Holden, B.A.; Fricke, T.R.; Wilson, D.A.; Jong, M.; Naidoo, K.S.; Sankaridurg, P.; Wong, T.Y.; Naduvilath, T.J.; Resnikoff, S. Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050. Ophthalmology 2016, 123, 1036–1042. [Google Scholar] [CrossRef] [PubMed]
- Bilbao-Malavé, V.; González-Zamora, J.; Gándara, E.; de la Puente, M.; Escriche, E.; Bezunartea, J.; Marizkurrena, A.; Alonso, E.; Hernández, M.; Fernández-Robredo, P.; et al. A Cross-Sectional Observational Study of the Relationship between Outdoor Exposure and Myopia in University Students, Measured by Conjunctival Ultraviolet Autofluorescence (CUVAF). J. Clin. Med. 2022, 11, 4264. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.; Pezic, A.; Mackey, D.A.; Carlin, J.B.; Kemp, A.; Ellis, J.A.; Cameron, F.J.; Rodda, C.P.; Dwyer, T.; Coroneo, M.T.; et al. Conjunctival Ultraviolet Autofluorescence as a Measure of Past Sun Exposure in Children. Cancer Epidemiol. Biomark. Prev. 2017, 26, 1146–1153. [Google Scholar] [CrossRef]
- Sherwin, J.C.; Hewitt, A.W.; Kearns, L.S.; Coroneo, M.T.; Griffiths, L.R.; Mackey, D.A. Distribution of conjunctival ultraviolet autofluorescence in a population-based study: The Norfolk Island Eye Study. Eye 2011, 25, 893–900. [Google Scholar] [CrossRef] [PubMed]
- Kearney, S.; O’Donoghue, L.; Pourshahidi, L.K.; Richardson, P.; Laird, E.; Healy, M.; Saunders, K.J. Conjunctival ultraviolet autofluorescence area, but not intensity, is associated with myopia. Clin. Exp. Optom. 2019, 102, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Ooi, J.L.; Sharma, N.S.; Papalkar, D.; Sharma, S.; Oakey, M.; Dawes, P.; Coroneo, M.T. Ultraviolet fluorescence photography to detect early sun damage in the eyes of school-aged children. Am. J. Ophthalmol. 2006, 141, 294–298. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Kawasaki, H.; Liu, Y.; Wang, Z. The prevalence of myopia and the factors associated with it among university students in Nanjing: A cross-sectional study. Medicine 2019, 98, e14777. [Google Scholar] [CrossRef] [PubMed]
- Williams, K.M.; Bentham, G.C.G.; Young, I.S.; McGinty, A.; McKay, G.J.; Hogg, R.; Hammond, C.J.; Chakravarthy, U.; Rahu, M.; Seland, J.; et al. Association between Myopia, Ultraviolet B Radiation Exposure, Serum Vitamin D Concentrations, and Genetic Polymorphisms in Vitamin D Metabolic Pathways in a Multicountry European Study. JAMA Ophthalmol. 2017, 135, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Morgan, I.G.; French, A.N.; Ashby, R.S.; Guo, X.; Ding, X.; He, M.; Rose, K.A. The epidemics of myopia: Aetiology and prevention. Prog Retin Eye Res. 2018, 62, 134–149. [Google Scholar] [CrossRef]
- Xiong, S.; Sankaridurg, P.; Naduvilath, T.; Zang, J.; Zou, H.; Zhu, J.; Lv, M.; He, X.; Xu, X. Time spent in outdoor activities in relation to myopia prevention and control: A meta-analysis and systematic review. Acta Ophthalmol. 2017, 95, 551–566. [Google Scholar] [CrossRef]
- Jones-Jordan, L.A.; Sinnott, L.T.; Chu, R.H.; Cotter, S.A.; Kleinstein, R.N.; Manny, R.E.; Mutti, D.O.; Twelker, J.D.; Zadnik, K.; CLEERE Study Group. Myopia Progression as a Function of Sex, Age, and Ethnicity. Investig. Ophthalmol. Vis. Sci. 2021, 62, 36. [Google Scholar] [CrossRef]
- Jonas, J.B.; Ang, M.; Cho, P.; Guggenheim, J.A.; He, M.G.; Jong, M.; Logan, N.S.; Liu, M.; Morgan, I.; Ohno-Matsui, K.; et al. IMI Prevention of Myopia and Its Progression. Investig. Ophthalmol. Vis. Sci. 2021, 62, 6. [Google Scholar] [CrossRef]
- Vagge, A.; Ferro Desideri, L.; Nucci, P.; Serafino, M.; Giannaccare, G.; Traverso, C.E. Prevention of Progression in Myopia: A Systematic Review. Diseases 2018, 6, 92. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | 6–17 | 18–25 | >40 | p | |
|---|---|---|---|---|---|
| N (%) | 298 (100) | 202 (68) | 80 (27) | 16 (5) | |
| Gender (F) (%) | 69% | 66% | 75% | 75% | ns |
| Age (years) | 19.8 | 13.9 | 21.5 | 44.4 | *** |
| Age of onset of myopia (years) | 9.3 | 8.4 | 11.1 | 9.5 | * |
| Diopters (D) | −3.96 | −3.5 | −4.05 | −5.8 | ** |
| N° of high myopes (HM) (%) | 18.2% | 16% | 27% | 62.5% | *** |
| >30 h of NA/week (%) | 78.2% | 77% | 82% | 50% | ** |
| Increased NA during PC | 81% | 80% | 83% | 75% | ns |
| >10 h of OA/week (%) | 38.2% | 32% | 38% | 62.5% | * |
| Decreased OA during PC (%) | 74% | 78% | 73% | 65% | ns |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de la Puente, M.; Irigoyen-Bañegil, C.; Ortega Claici, A.; González-Zamora, J.; Bilbao-Malavé, V.; Fernandez-Robredo, P.; Hernández, M.; Barrio, J.; García-Layana, A.; Recalde, S. Could Children’s Myopization Have Been Avoided during the Pandemic Confinement? The Conjunctival Ultraviolet Autofluorescence (CUVAF) Biomarker as an Answer. Biomedicines 2024, 12, 347. https://doi.org/10.3390/biomedicines12020347
de la Puente M, Irigoyen-Bañegil C, Ortega Claici A, González-Zamora J, Bilbao-Malavé V, Fernandez-Robredo P, Hernández M, Barrio J, García-Layana A, Recalde S. Could Children’s Myopization Have Been Avoided during the Pandemic Confinement? The Conjunctival Ultraviolet Autofluorescence (CUVAF) Biomarker as an Answer. Biomedicines. 2024; 12(2):347. https://doi.org/10.3390/biomedicines12020347
Chicago/Turabian Stylede la Puente, Miriam, Cristina Irigoyen-Bañegil, Aura Ortega Claici, Jorge González-Zamora, Valentina Bilbao-Malavé, Patricia Fernandez-Robredo, María Hernández, Jesús Barrio, Alfredo García-Layana, and Sergio Recalde. 2024. "Could Children’s Myopization Have Been Avoided during the Pandemic Confinement? The Conjunctival Ultraviolet Autofluorescence (CUVAF) Biomarker as an Answer" Biomedicines 12, no. 2: 347. https://doi.org/10.3390/biomedicines12020347
APA Stylede la Puente, M., Irigoyen-Bañegil, C., Ortega Claici, A., González-Zamora, J., Bilbao-Malavé, V., Fernandez-Robredo, P., Hernández, M., Barrio, J., García-Layana, A., & Recalde, S. (2024). Could Children’s Myopization Have Been Avoided during the Pandemic Confinement? The Conjunctival Ultraviolet Autofluorescence (CUVAF) Biomarker as an Answer. Biomedicines, 12(2), 347. https://doi.org/10.3390/biomedicines12020347