
Administration of Adipose-Derived Stem Cells After the Onset of the Disease Does Not Lower the Levels of Inflammatory Cytokines IL1 and IL6 in a Rat Model of Necrotizing Enterocolitis

 , , , and
, , , and
Abstract
1. Introduction
1.1. Necrotizing Enterocolitis (NEC)
1.2. Stem Cells
1.3. Cytokines in NEC
1.4. Adipose-Derived Stem Cells and NEC
1.5. Aim of the Study
2. Materials and Methods
2.1. NEC Induction
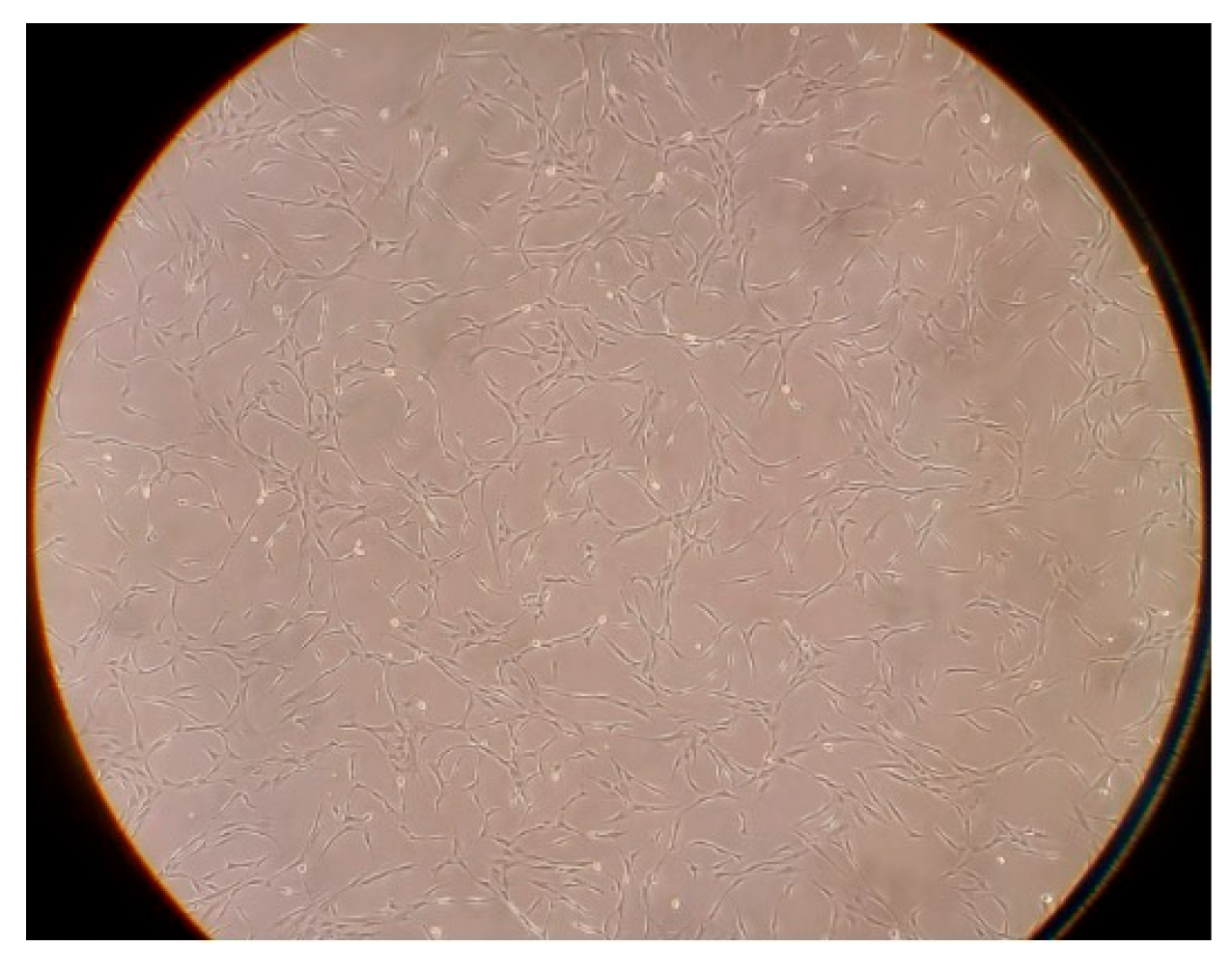
2.2. Stem Cells
2.3. Immunohistochemistry—Engraftment Analysis
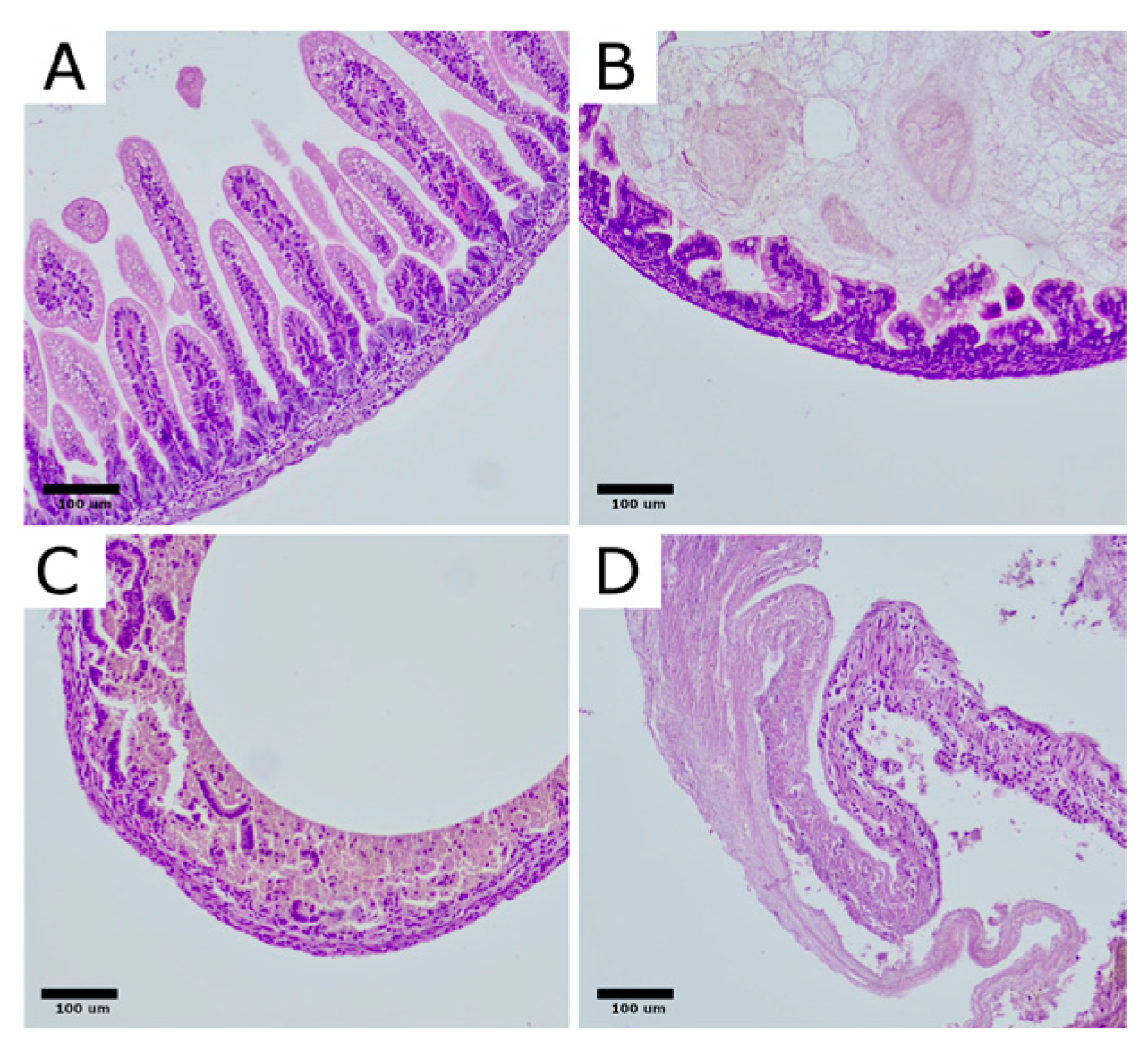
2.4. Histopathology
2.5. ELISA Analysis—Cytokine Concentrations
2.6. Statistical Analysis
3. Results
3.1. Engraftment
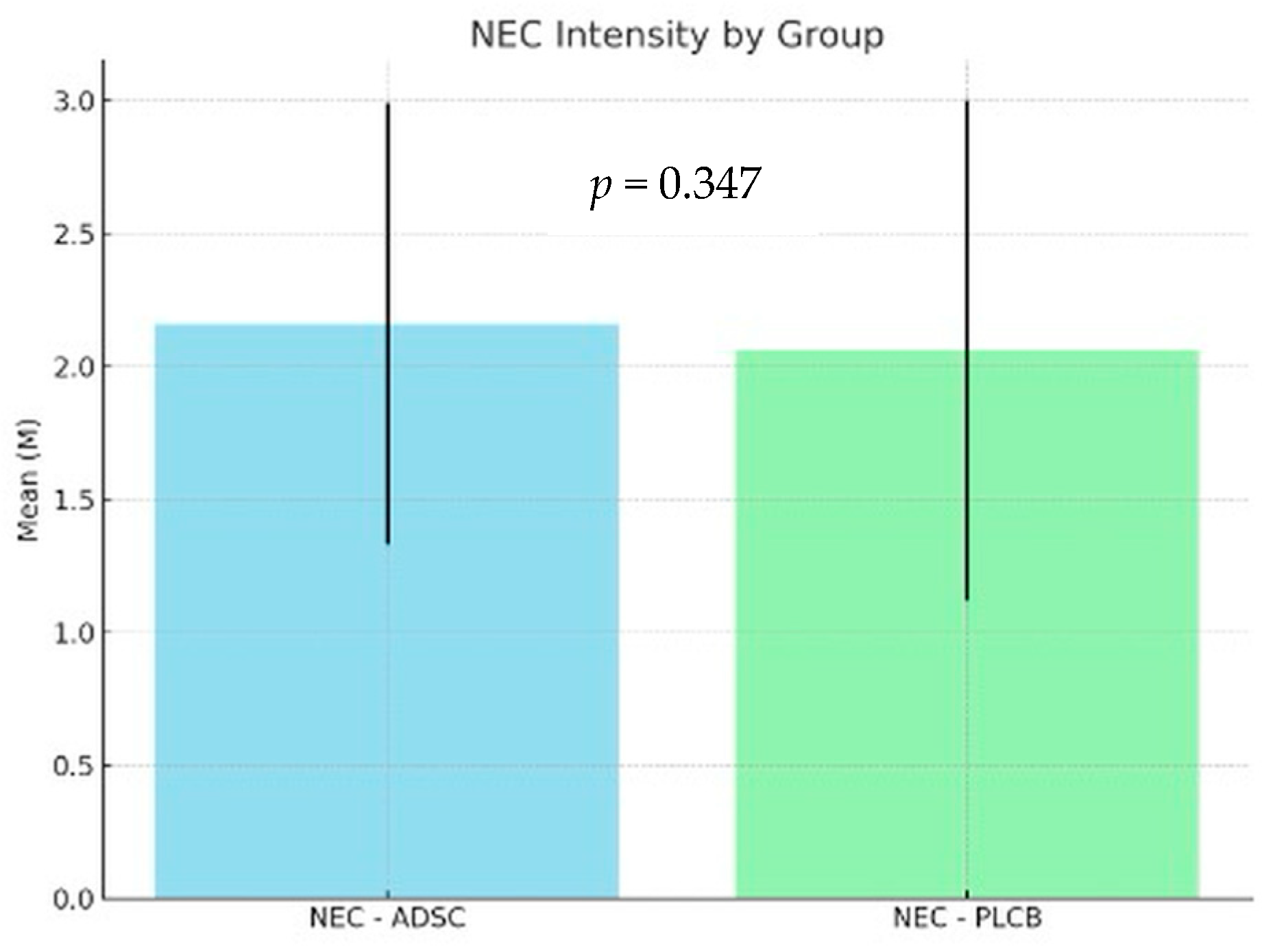
3.2. Histopathology
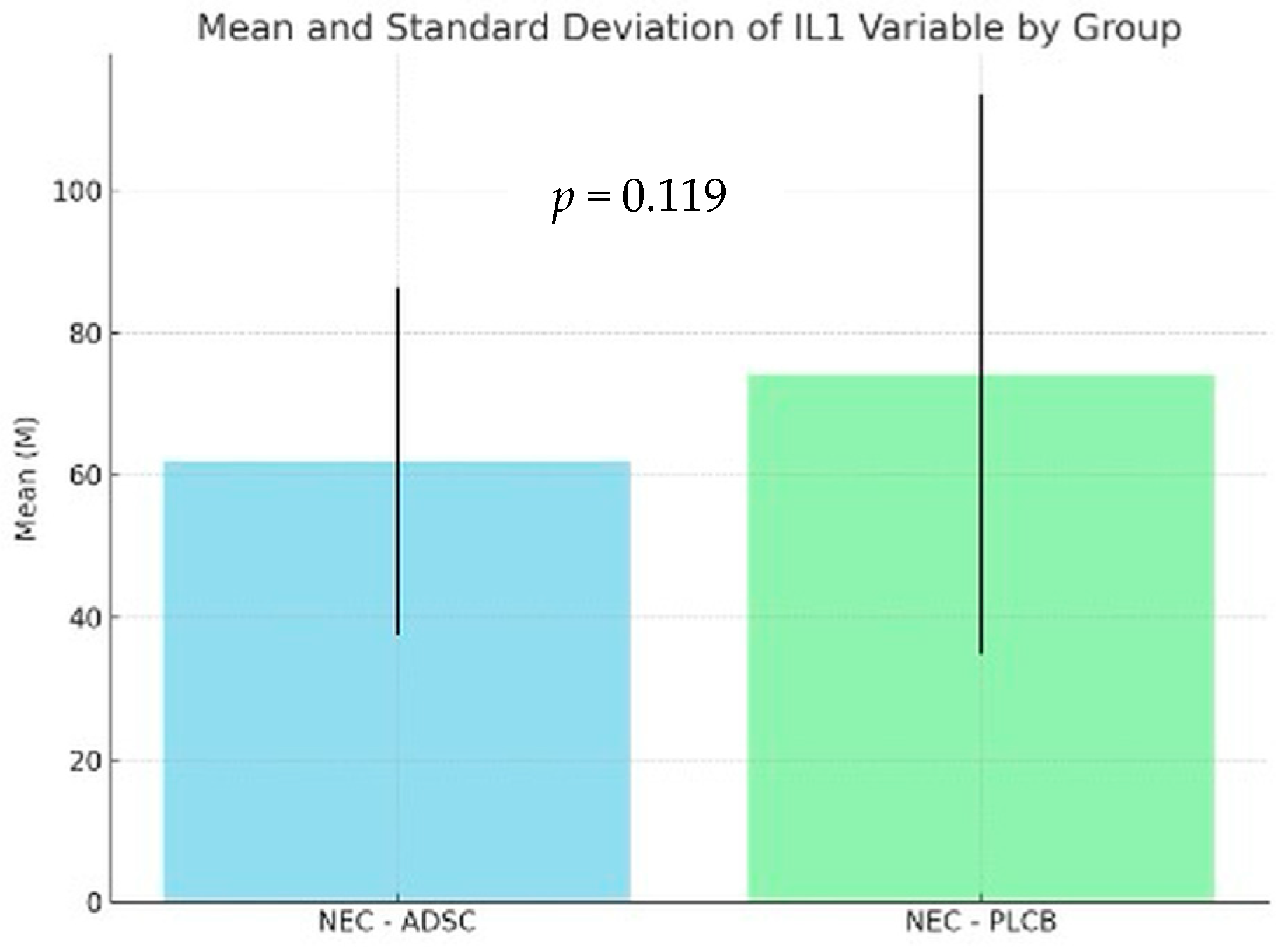
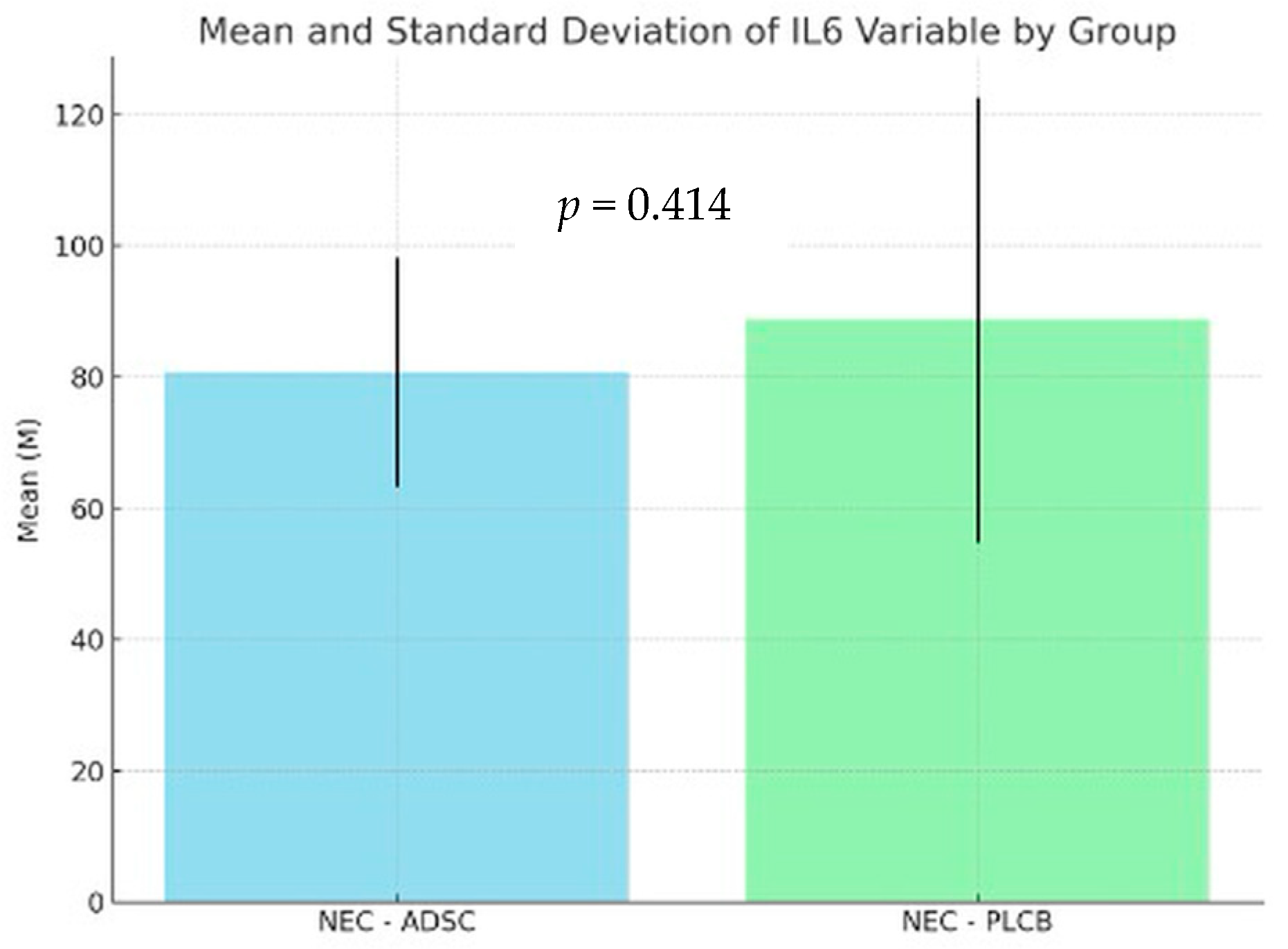
3.3. Cytokine Concentrations
3.4. Summary of the Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Neu, J. Necrotizing Enterocolitis: The Future. Neonatology 2020, 117, 240–244. [Google Scholar] [CrossRef]
- Alganabi, M.; Lee, C.; Bindi, E.; Li, B.; Pierro, A. Recent advances in understanding necrotizing enterocolitis. F1000Res 2019, 8, F1000 Faculty Rev–107. [Google Scholar] [CrossRef] [PubMed]
- Eaton, S.; Rees, C.M.; Hall, N.J. Current Research on the Epidemiology, Pathogenesis, and Management of Necrotizing Enterocolitis. Neonatology 2017, 111, 423–430. [Google Scholar] [CrossRef]
- Wolski, M. Modification of Experimental Model of Necrotizing Enterocolitis (NEC) in Rat Pups by Single Exposure to Hypothermia and Hypoxia and Impact of Mother’s Milk on Incidence of Disease. Med. Sci. Monit. 2024, 30, e943443. [Google Scholar] [CrossRef] [PubMed]
- Ginglen, J.G.; Butki, N. Necrotizing Enterocolitis; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2024. [Google Scholar]
- Lopez, C.M.; Sampah, M.E.; Duess, J.W.; Ishiyama, A.; Ahmad, R.; Sodhi, C.P.; Hackam, D.J. Models of necrotizing enterocolitis. Semin. Perinatol. 2023, 47, 151695. [Google Scholar] [CrossRef] [PubMed]
- Sodhi, C.; Richardson, W.; Gribar, S.; Hackam, D.J. The development of animal models for the study of necrotizing enterocolitis. Dis. Model. Mech. 2008, 1, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Neal, M.D.; Richardson, W.M.; Sodhi, C.P.; Russo, A.; Hackam, D.J. Intestinal stem cells and their roles during mucosal injury and repair. J. Surg. Res. 2011, 167, 1–8. [Google Scholar] [CrossRef]
- Markel, T.A.; Crisostomo, P.R.; Wairiuko, G.M.; Pitcher, J.; Tsai, B.M.; Meldrum, D.R. Cytokines in necrotizing enterocolitis. Shock 2006, 25, 329–337. [Google Scholar] [CrossRef]
- Mara, M.A.; Good, M.; Weitkamp, J.H. Innate and adaptive immunity in necrotizing enterocolitis. Semin. Fetal Neonatal Med. 2018, 23, 394–399. [Google Scholar] [CrossRef]
- Mohan Kumar, K.; Namachivayam, K.; Ho, T.T.; Torres, B.A.; Ohls, R.K.; Maheshwari, A. Cytokines and growth factors in the developing intestine and during necrotizing enterocolitis. Semin. Perinatol. 2017, 41, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Wei, G.; Schubiger, G.; Harder, F.; Müller, A.M. Stem cell plasticity in mammals and transdetermination in Drosophila: Common themes? Stem Cells 2000, 18, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Banas, A.; Teratani, T.; Yamamoto, Y.; Tokuhara, M.; Takeshita, F.; Quinn, G.; Okochi, H.; Ochiya, T. Adipose tissue-derived mesenchymal stem cells as a source of human hepatocytes. Hepatology 2007, 46, 219–228. [Google Scholar] [CrossRef] [PubMed]
- Strioga, M.; Viswanathan, S.; Darinskas, A.; Slaby, O.; Michalek, J. Same or not the same? Comparison of adipose tissue-derived versus bone marrow-derived mesenchymal stem and stromal cells. Stem Cells Dev. 2012, 21, 2724–2752. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Liu, T.; Song, K.; Fan, X.; Ma, X.; Cui, Z. Adipose-derived stem cell: A better stem cell than BMSC. Cell Biochem. Funct. 2008, 26, 664–675. [Google Scholar] [CrossRef]
- Ren, Y.; Wu, H.; Zhou, X.; Wen, J.; Jin, M.; Cang, M.; Guo, X.; Wang, Q.; Liu, D.; Ma, Y. Isolation, expansion, and differentiation of goat adipose-derived stem cells. Res. Vet. Sci. 2012, 93, 404–411. [Google Scholar] [CrossRef] [PubMed]
- Hall, M.N.; Rosenkrantz, W.S.; Hong, J.H.; Griffin, C.E.; Mendelsohn, C.M. Evaluation of the potential use of adipose-derived mesenchymal stromal cells in the treatment of canine atopic dermatitis: A pilot study. Vet. Ther. 2010, 11, E1–E14. [Google Scholar] [PubMed]
- Efimenko, A.; Starostina, E.; Kalinina, N.; Stolzing, A. Angiogenic properties of aged adipose derived mesenchymal stem cells after hypoxic conditioning. J. Transl. Med. 2011, 9, 10. [Google Scholar] [CrossRef]
- McCulloh, C.J.; Olson, J.K.; Wang, Y.; Vu, J.; Gartner, S.; Besner, G.E. Evaluating the efficacy of different types of stem cells in preserving gut barrier function in necrotizing enterocolitis. J. Surg. Res. 2017, 214, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Tayman, C.; Uckan, D.; Kilic, E.; Ulus, A.T.; Tonbul, A.; Murat Hirfanoglu, I.; Helvacioglu, F.; Haltas, H.; Koseoglu, B.; Tatli, M.M. Mesenchymal stem cell therapy in necrotizing enterocolitis: A rat study. Pediatr. Res. 2011, 70, 489–494. [Google Scholar] [CrossRef] [PubMed]
- McCulloh, C.J.; Olson, J.K.; Zhou, Y.; Wang, Y.; Besner, G.E. Stem cells and necrotizing enterocolitis: A direct comparison of the efficacy of multiple types of stem cells. J. Pediatr. Surg. 2017, 52, 999–1005. [Google Scholar] [CrossRef] [PubMed]
- Zani, A.; Cananzi, M.; Fascetti-Leon, F.; Lauriti, G.; Smith, V.V.; Bollini, S.; Ghionzoli, M.; D’Arrigo, A.; Pozzobon, M.; Piccoli, M.; et al. Amniotic fluid stem cells improve survival and enhance repair of damaged intestine in necrotising enterocolitis via a COX-2 dependent mechanism. Gut 2014, 63, 300–309. [Google Scholar] [CrossRef] [PubMed]
- Al-Ghadban, S.; Bunnell, B.A. Adipose Tissue-Derived Stem Cells: Immunomodulatory Effects and Therapeutic Potential. Physiology 2020, 35, 125–133. [Google Scholar] [CrossRef] [PubMed]
- McIntosh, K.; Zvonic, S.; Garrett, S.; Mitchell, J.B.; Floyd, Z.E.; Hammill, L.; Kloster, A.; Di Halvorsen, Y.; Ting, J.P.; Storms, R.W.; et al. The immunogenicity of human adipose-derived cells: Temporal changes in vitro. Stem Cells 2006, 24, 1246–1253. [Google Scholar] [CrossRef]
- Yañez, R.; Lamana, M.L.; García-Castro, J.; Colmenero, I.; Ramírez, M.; Bueren, J.A. Adipose tissue-derived mesenchymal stem cells have in vivo immunosuppressive properties applicable for the control of the graft-versus-host disease. Stem Cells 2006, 24, 2582–2591. [Google Scholar] [CrossRef] [PubMed]
- Engela, A.U.; Hoogduijn, M.J.; Boer, K.; Litjens, N.H.; Betjes, M.G.; Weimar, W.; Baan, C.C. Human adipose-tissue derived mesenchymal stem cells induce functional de-novo regulatory T cells with methylated FOXP3 gene DNA. Clin. Exp. Immunol. 2013, 173, 343–354. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Rey, E.; Gonzalez, M.A.; Varela, N.; O’Valle, F.; Hernandez-Cortes, P.; Rico, L.; Büscher, D.; Delgado, M. Human adipose-derived mesenchymal stem cells reduce inflammatory and T cell responses and induce regulatory T cells in vitro in rheumatoid arthritis. Ann. Rheum. Dis. 2010, 69, 241–248. [Google Scholar] [CrossRef]
- Stojanović, S.; Najman, S. The Effect of Conditioned Media of Stem Cells Derived from Lipoma and Adipose Tissue on Macrophages’ Response and Wound Healing in Indirect Co-culture System In Vitro. Int. J. Mol. Sci. 2019, 20, 1671. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Yuan, Q.; Xie, L. Mesenchymal Stem Cell-Based Immunomodulation: Properties and Clinical Application. Stem Cells Int. 2018, 2018, 3057624. [Google Scholar] [CrossRef]
- González, M.A.; Gonzalez-Rey, E.; Rico, L.; Büscher, D.; Delgado, M. Adipose-derived mesenchymal stem cells alleviate experimental colitis by inhibiting inflammatory and autoimmune responses. Gastroenterology 2009, 136, 978–989. [Google Scholar] [CrossRef]
- Dubey, N.K.; Mishra, V.K.; Dubey, R.; Deng, Y.H.; Tsai, F.C.; Deng, W.P. Revisiting the Advances in Isolation, Characterization and Secretome of Adipose-Derived Stromal/Stem Cells. Int. J. Mol. Sci. 2018, 19, 2200. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, R.; Mellows, B.; Sheard, J.; Antonioli, M.; Kretz, O.; Chambers, D.; Zeuner, M.T.; Tomkins, J.E.; Denecke, B.; Musante, L.; et al. Secretome of adipose-derived mesenchymal stem cells promotes skeletal muscle regeneration through synergistic action of extracellular vesicle cargo and soluble proteins. Stem Cell Res. Ther. 2019, 10, 116. [Google Scholar] [CrossRef] [PubMed]
- Lai, R.C.; Yeo, R.W.; Lim, S.K. Mesenchymal stem cell exosomes. Semin. Cell Dev. Biol. 2015, 40, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.S.; Park, B.S.; Sung, J.H.; Yang, J.M.; Park, S.B.; Kwak, S.J.; Park, J.S. Wound healing effect of adipose-derived stem cells: A critical role of secretory factors on human dermal fibroblasts. J. Dermatol. Sci. 2007, 48, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Baglio, S.R.; Rooijers, K.; Koppers-Lalic, D.; Verweij, F.J.; Pérez Lanzón, M.; Zini, N.; Naaijkens, B.; Perut, F.; Niessen, H.W.; Baldini, N.; et al. Human bone marrow- and adipose-mesenchymal stem cells secrete exosomes enriched in distinctive miRNA and tRNA species. Stem Cell Res. Ther. 2015, 6, 127. [Google Scholar] [CrossRef] [PubMed]
- Han, C.; Sun, X.; Liu, L.; Jiang, H.; Shen, Y.; Xu, X.; Li, J.; Zhang, G.; Huang, J.; Lin, Z.; et al. Exosomes and Their Therapeutic Potentials of Stem Cells. Stem Cells Int. 2016, 2016, 7653489. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.I.; Wang, J.; Zhou, X.; Xiong, Z.; Zhao, J.; Yu, R.; Huang, F.; Zhang, H.; Chen, L. Exosomes derived from human adipose mensenchymal stem cells accelerates cutaneous wound healing via optimizing the characteristics of fibroblasts. Sci. Rep. 2016, 6, 32993. [Google Scholar] [CrossRef]
- Li, X.; Xie, X.; Lian, W.; Shi, R.; Han, S.; Zhang, H.; Lu, L.; Li, M. Exosomes from adipose-derived stem cells overexpressing Nrf2 accelerate cutaneous wound healing by promoting vascularization in a diabetic foot ulcer rat model. Exp. Mol. Med. 2018, 50, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Cho, B.S.; Kim, J.O.; Ha, D.H.; Yi, Y.W. Exosomes derived from human adipose tissue-derived mesenchymal stem cells alleviate atopic dermatitis. Stem Cell Res. Ther. 2018, 9, 187. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Xu, Y.; Wan, Y.; Gao, J.; Chu, Y.; Li, J. Exosomes from adipose-derived mesenchymal stem cells prevent cardiomyocyte apoptosis induced by oxidative stress. Cell Death Discov. 2019, 5, 79. [Google Scholar] [CrossRef]
- Wolski, M.; Ciesielski, T.; Buczma, K.; Fus, Ł.; Girstun, A.; Trzcińska-Danielewicz, J.; Cudnoch-Jędrzejewska, A. Administration of Adipose Tissue Derived Stem Cells before the Onset of the Disease Lowers the Levels of Inflammatory Cytokines IL-1 and IL-6 in the Rat Model of Necrotizing Enterocolitis. Int. J. Mol. Sci. 2024, 25, 11052. [Google Scholar] [CrossRef]
- Yang, J.; Liu, X.X.; Fan, H.; Tang, Q.; Shou, Z.X.; Zuo, D.M.; Zou, Z.; Xu, M.; Chen, Q.Y.; Peng, Y.; et al. Extracellular Vesicles Derived from Bone Marrow Mesenchymal Stem Cells Protect against Experimental Colitis via Attenuating Colon Inflammation, Oxidative Stress and Apoptosis. PLoS ONE 2015, 10, e0140551. [Google Scholar] [CrossRef] [PubMed]
- Ocansey, D.K.; Wang, L.; Wang, J.; Yan, Y.; Qian, H.; Zhang, X.; Xu, W.; Mao, F. Mesenchymal stem cell-gut microbiota interaction in the repair of inflammatory bowel disease: An enhanced therapeutic effect. Clin. Transl. Med. 2019, 8, 31. [Google Scholar] [CrossRef]
- Shi, Y.; Wang, Y.; Li, Q.; Liu, K.; Hou, J.; Shao, C.; Wang, Y. Immunoregulatory mechanisms of mesenchymal stem and stromal cells in inflammatory diseases. Nat. Rev. Nephrol. 2018, 14, 493–507. [Google Scholar] [CrossRef]
- Zolocinska, A.; Siennicka, K.; Debski, T.; Gut, G.; Mazur, S.; Gajewska, M.; Kaminski, A.; Pojda, Z. Comparison of mouse, rat and rabbit models for adipose - Derived stem cells (ASC) research. Curr. Res. Transl. Med. 2020, 68, 205–210. [Google Scholar] [CrossRef]
- Mimatsu, H.; Onoda, A.; Kazama, T.; Nishijima, K.; Shimoyama, Y.; Go, S.; Ueda, K.; Takahashi, Y.; Matsumoto, T.; Hayakawa, M.; et al. Dedifferentiated fat cells administration ameliorates abnormal expressions of fatty acids metabolism-related protein expressions and intestinal tissue damage in experimental necrotizing enterocolitis. Sci. Rep. 2023, 13, 8266. [Google Scholar] [CrossRef]
- Pisano, C.; Besner, G.E. Potential role of stem cells in disease prevention based on a murine model of experimental necrotizing enterocolitis. J. Pediatr. Surg. 2019, 54, 413–416. [Google Scholar] [CrossRef] [PubMed]
- Liau, L.L.; Al-Masawa, M.E.; Koh, B.; Looi, Q.H.; Foo, J.B.; Lee, S.H.; Cheah, F.C.; Law, J.X. The Potential of Mesenchymal Stromal Cell as Therapy in Neonatal Diseases. Front. Pediatr. 2020, 8, 591693. [Google Scholar] [CrossRef] [PubMed]
- Akduman, H.; Dilli, D.; Ergün, E.; Cakmakcı, E.; Celebi, S.K.; Citli, R.; Zenciroğlu, A. Successful Mesenchymal Stem Cell Application in Supraventricular Tachycardia-Related Necrotizing Enterocolitis: A Case Report. Fetal Pediatr. Pathol. 2021, 40, 250–255. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | n | Min | Max | M | SD |
|---|---|---|---|---|---|
| NEC-ADSC | 55 | 0 | 10 | 3.10 | 2.58 |
| NEC-PLCB | 60 | 0 | 10 | 2.17 | 2.40 |
| NEC Score | NEC-ADSC | NEC-PLCB |
|---|---|---|
| 0 | 0 (0.00%) | 2 (3.33%) |
| 1 | 15 (27.27%) | 18 (30.00%) |
| 2 | 16 (29.09%) | 14 (23.33%) |
| 3 | 24 (43.64%) | 26 (43.33%) |
| Total | 55 (100.00%) | 60 (100.00%) |
| Group | n | Min | Max | M | SD |
|---|---|---|---|---|---|
| NEC-ADSC | 55 | 1 | 3 | 2.16 | 0.83 |
| NEC-PLCB | 60 | 0 | 3 | 2.06 | 0.94 |
| Group | n | Min | Max | M | SD |
|---|---|---|---|---|---|
| NEC-ADSC | 55 | 5 | 112.19 | 61.90 | 24.38 |
| NEC-PLCB | 62 | 10 | 189.49 | 74.18 | 39.31 |
| Group | n | Min | Max | M | SD |
|---|---|---|---|---|---|
| NEC-ADSC | 55 | 41.38 | 120.42 | 80.74 | 17.46 |
| NEC-PLCB | 62 | 25.30 | 180.40 | 88.67 | 33.95 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wolski, M.; Ciesielski, T.; Buczma, K.; Fus, Ł.; Girstun, A.; Trzcińska-Danielewicz, J.; Cudnoch-Jędrzejewska, A. Administration of Adipose-Derived Stem Cells After the Onset of the Disease Does Not Lower the Levels of Inflammatory Cytokines IL1 and IL6 in a Rat Model of Necrotizing Enterocolitis. Biomedicines 2024, 12, 2897. https://doi.org/10.3390/biomedicines12122897
Wolski M, Ciesielski T, Buczma K, Fus Ł, Girstun A, Trzcińska-Danielewicz J, Cudnoch-Jędrzejewska A. Administration of Adipose-Derived Stem Cells After the Onset of the Disease Does Not Lower the Levels of Inflammatory Cytokines IL1 and IL6 in a Rat Model of Necrotizing Enterocolitis. Biomedicines. 2024; 12(12):2897. https://doi.org/10.3390/biomedicines12122897
Chicago/Turabian StyleWolski, Marek, Tomasz Ciesielski, Kasper Buczma, Łukasz Fus, Agnieszka Girstun, Joanna Trzcińska-Danielewicz, and Agnieszka Cudnoch-Jędrzejewska. 2024. "Administration of Adipose-Derived Stem Cells After the Onset of the Disease Does Not Lower the Levels of Inflammatory Cytokines IL1 and IL6 in a Rat Model of Necrotizing Enterocolitis" Biomedicines 12, no. 12: 2897. https://doi.org/10.3390/biomedicines12122897
APA StyleWolski, M., Ciesielski, T., Buczma, K., Fus, Ł., Girstun, A., Trzcińska-Danielewicz, J., & Cudnoch-Jędrzejewska, A. (2024). Administration of Adipose-Derived Stem Cells After the Onset of the Disease Does Not Lower the Levels of Inflammatory Cytokines IL1 and IL6 in a Rat Model of Necrotizing Enterocolitis. Biomedicines, 12(12), 2897. https://doi.org/10.3390/biomedicines12122897