

How to Generate Self-Efficacy despite Pain: The Role of Catastrophizing and Avoidance in Women with Fibromyalgia

Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Measures
2.3.1. Pain Severity
2.3.2. Pain Catastrophizing
2.3.3. Pain Avoidance
2.3.4. Pain Self-Efficacy
2.3.5. Symptom Severity Scale (SSS)
2.3.6. Demographic and Clinical Characteristics
2.4. Procedure
2.5. Statistical Analyses
3. Results
3.1. Sample Characteristics
3.2. Correlations
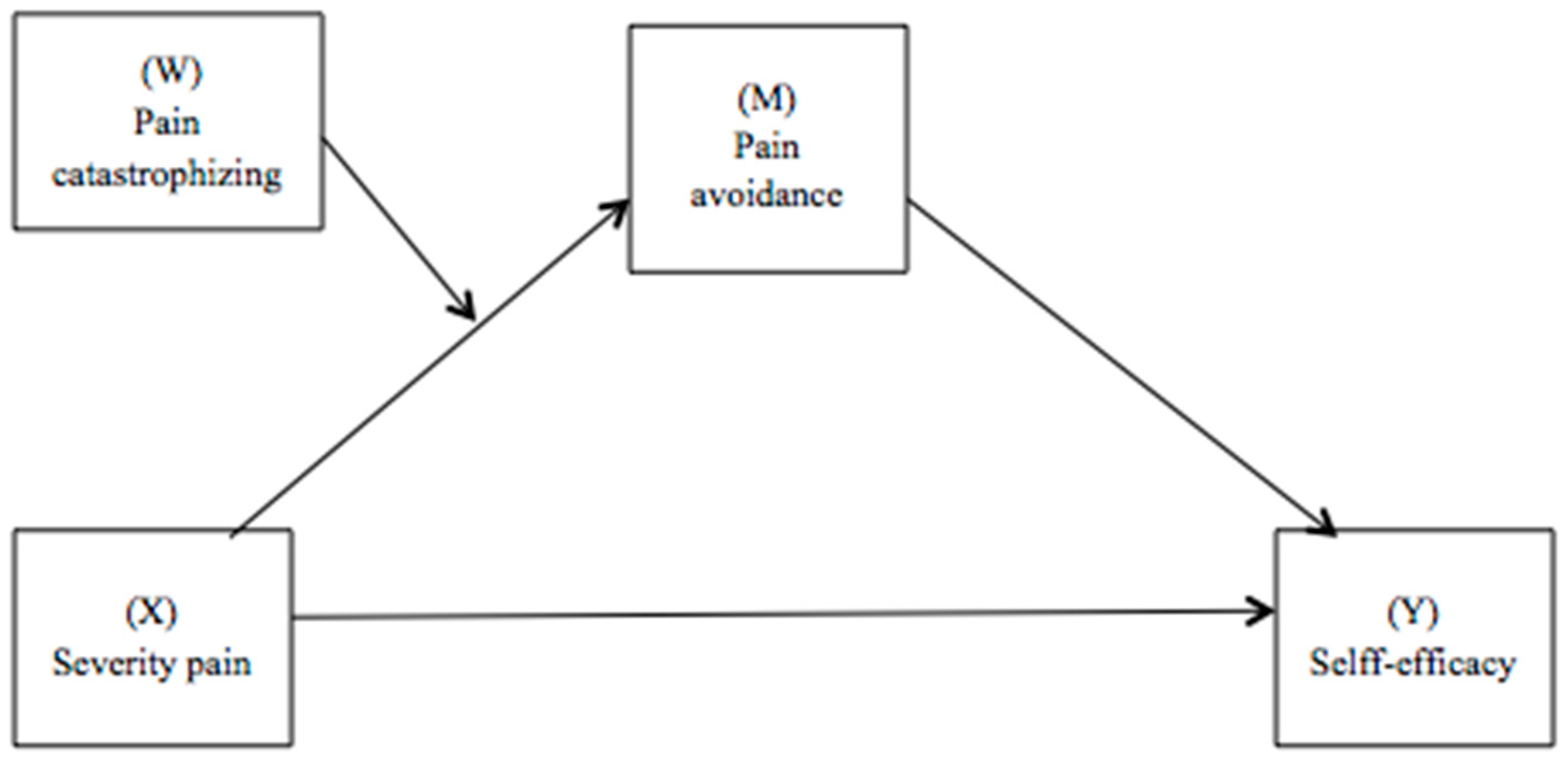
3.3. Moderated Mediation Model
4. Discussion
4.1. Limitations
4.2. Clinical Implications and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B.; Yunus, M.B. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res. 2010, 62, 600–610. [Google Scholar] [CrossRef] [PubMed]
- Sumpton, J.E.; Moulin, D.E. Fibromyalgia: Presentation and Management with a Focus on Pharmacological Treatment. Pain Res. Manag. 2008, 13, 477–483. [Google Scholar] [CrossRef] [PubMed]
- Clauw, D.J. Fibromyalgia: A clinical review. JAMA 2014, 311, 1547. [Google Scholar] [CrossRef] [PubMed]
- Häuser, W.; Ablin, J.; Fitzcharles, M.-A.; Littlejohn, G.; Luciano, J.V.; Usui, C.; Walitt, B. Fibromyalgia. Nat. Rev. Dis. Prim. 2015, 1, 15022. [Google Scholar] [CrossRef] [PubMed]
- Lami, M.J.; Martínez, M.P.; Miró, E.; Sánchez, A.I.; Guzmán, M.A. Catastrophizing, Acceptance, and Coping as Mediators Between Pain and Emotional Distress and Disability in Fibromyalgia. J. Clin. Psychol. Med. Settings 2018, 25, 80–92. [Google Scholar] [CrossRef] [PubMed]
- García, J.; Simón, M.A.; Durán, M.; Canceller, J.; Aneiros, F.J. Differential efficacy of a cognitive-behavioral intervention versus pharmacological treatment in the management of fibromyalgic syndrome. Psychol. Health Med. 2006, 11, 498–506. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, M.D.; Ballantyne, J.C. Must we reduce pain intensity to treat chronic pain? Pain 2016, 157, 65–69. [Google Scholar] [CrossRef]
- Lledó-Boyer, A.; Pastor-Mira, M.A.; Pons-Calatayud, N.; López-Roig, S.; Rodríguez-Marín, J.; Bruehl, S. Control beliefs, coping and emotions: Exploring relationships to explain fibromyalgia health outcomes. Int. J. Clin. Health Psychol. 2010, 10, 459–476. [Google Scholar]
- Van Liew, C.; Brown, K.C.; Cronan, T.A.; Bigatti, S.M. The effects of self-efficacy on depression and pain in fibromyalgia syndrome: Does initial depression matter? J. Musculoskelet. Pain 2013, 21, 113–125. [Google Scholar] [CrossRef]
- Peñacoba Puente, C.; Velasco Furlong, L.; Écija Gallardo, C.; Cigarán Méndez, M.; Bedmar Cruz, D.; Fernández-de-las-Peñas, C. Self-Efficacy and Affect as Mediators Between Pain Dimensions and Emotional Symptoms and Functional Limitation in Women With Fibromyalgia. Pain Manag. Nurs. 2015, 16, 60–68. [Google Scholar] [CrossRef]
- Pastor, M.A.; Lledó, A.; Pons, N.; López-Roig, S. Dolor y Fibromialgia. Aportaciones Desde la Psicología. In Fibromialgia y Promoción de la Salud. Herramientas de Intervención Psicosocial; Peñacoba, C., Ed.; Dykinson: Madrid, Spain, 2012. [Google Scholar]
- Andrade, A.; Steffens, R.d.A.K.; Vilarino, G.T.; Sieczkowska, S.M.; Coimbra, D.R. Does volume of physical exercise have an effect on depression in patients with fibromyalgia? J. Affect. Disord. 2017, 208, 214–217. [Google Scholar] [CrossRef] [PubMed]
- Crombez, G.; Eccleston, C.; Van Damme, S.; Vlaeyen, J.W.S.; Karoly, P. Fear-Avoidance Model of Chronic Pain: The next generation. Clin. J. Pain 2012, 28, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Nijs, J.; Roussel, N.; Van Oosterwijck, J.; De Kooning, M.; Ickmans, K.; Struyf, F.; Meeus, M.; Lundberg, M. Fear of movement and avoidance behaviour toward physical activity in chronic-fatigue syndrome and fibromyalgia: State of the art and implications for clinical practice. Clin. Rheumatol. 2013, 32, 1121–1129. [Google Scholar] [CrossRef] [PubMed]
- Crombez, G.; De Paepe, A.L.; Veirman, E.; Eccleston, C.; Verleysen, G.; Van Ryckeghem, D.M.L. Let’s talk about pain catastrophizing measures: An item content analysis. PeerJ 2020, 8, e8643. [Google Scholar] [CrossRef] [PubMed]
- Edwards, R.R.; Bingham, C.O.; Bathon, J.; Haythornthwaite, J.A. Catastrophizing and pain in arthritis, fibromyalgia, and other rheumatic diseases. Arthritis Rheum. 2006, 55, 325–332. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, M.J.L.; Bishop, S.R.; Pivik, J. The Pain Catastrophizing Scale: Development and validation. Psychol. Assess. 1995, 7, 524–532. [Google Scholar] [CrossRef]
- Kim, J.; Loggia, M.L.; Cahalan, C.M.; Harris, R.E.; Beissner, F.; Garcia, R.G.; Kim, H.; Barbieri, R.; Wasan, A.D.; Edwards, R.R.; et al. The Somatosensory Link in Fibromyalgia: Functional Connectivity of the Primary Somatosensory Cortex Is Altered by Sustained Pain and Is Associated with Clinical/Autonomic Dysfunction. Arthritis Rheumatol. 2015, 67, 1395–1405. [Google Scholar] [CrossRef]
- Taylor, S.S.; Davis, M.C.; Yeung, E.W.; Zautra, A.J.; Tennen, H.A. Relations between adaptive and maladaptive pain cognitions and within-day pain exacerbations in individuals with fibromyalgia. J. Behav. Med. 2017, 40, 458–467. [Google Scholar] [CrossRef]
- Estévez-López, F.; Álvarez-Gallardo, I.C.; Segura-Jiménez, V.; Soriano-Maldonado, A.; Borges-Cosic, M.; Pulido-Martos, M.; Aparicio, V.A.; Carbonell-Baeza, A.; Delgado-Fernández, M.; Geenen, R. The discordance between subjectively and objectively measured physical function in women with fibromyalgia: Association with catastrophizing and self-efficacy cognitions. The al-Ándalus project. Disabil. Rehabil. 2018, 40, 329–337. [Google Scholar] [CrossRef]
- Catala, P.; Suso-Ribera, C.; Gutierrez, L.; Perez, S.; Lopez-Roig, S.; Peñacoba, C. Is Thought Management a Resource for Functioning in Women with Fibromyalgia Irrespective of Pain Levels? Pain Med. 2021, 22, 1827–1836. [Google Scholar] [CrossRef]
- Écija, C.; Luque-Reca, O.; Suso-Ribera, C.; Catala, P.; Peñacoba, C. Associations of Cognitive Fusion and Pain Catastrophizing with Fibromyalgia Impact through Fatigue, Pain Severity, and Depression: An Exploratory Study Using Structural Equation Modeling. J. Clin. Med. 2020, 9, 1763. [Google Scholar] [CrossRef] [PubMed]
- Westland, J.C. Lower bounds on sample size in structural equation modeling. Electronic commerce research and applications. Electron. Commer. Res. Appl. 2010, 9, 476–487. [Google Scholar] [CrossRef]
- Wolfe, F.; Smythe, H.A.; Yunus, M.B.; Bennett, R.M.; Bombardier, C.; Goldenberg, D.L.; Tugwell, P.; Campbell, S.M.; Abeles, M.; Clark, P.; et al. The American College of Rheumatology 1990 Criteria for the Classification of Fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis Rheum. 1990, 33, 160–172. [Google Scholar] [CrossRef] [PubMed]
- Cleeland, C.S.; Ryan, K.M. Pain assessment: Global use of the Brief Pain Inventory. Ann. Acad. Med. Singap. 1994, 23, 129–138. [Google Scholar] [PubMed]
- Jensen, M.P.; Turner, L.R.; Turner, J.A.; Romano, J.M. The use of multiple-item scales for pain intensity measurement in chronic pain patients. Pain 1996, 67, 35–40. [Google Scholar] [CrossRef] [PubMed]
- García Campayo, J.; Rodero, B.; Alda, M.; Sobradiel, N.; Montero, J.; Moreno, S. Validation of the Spanish version of the Pain Catastrophizing Scale in fibromyalgia. Med. Clin. 2008, 131, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Esteve, R.; Ramírez-Maestre, C.; Peters, M.L.; Serrano-Ibáñez, E.R.; Ruíz-Párraga, G.T.; López-Martínez, A.E. Development and Initial Validation of the Activity Patterns Scale in Patients with Chronic Pain. J. Pain 2016, 17, 451–461. [Google Scholar] [CrossRef]
- Martín-Aragón, M.; Pastor, M.A.; Rodríguez-Marín, J.; March, M.J.; Lledó, A.; López-Roig, S.; Terol, M.C. Percepción de autoeficacia en dolor crónico. Adaptación y validación de la Chronic Pain Self-Efficacy Scale. Rev. Psicol. Salud 1999, 11, 1–2. [Google Scholar]
- IBM Corp. IBM Corp IBM SPSS Statistics for Windows, Version 22.0; IBM Corp: New York, NY, USA, 2017. [Google Scholar]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis Second Edition A Regression-Based Approach; The Guilford Press: New York, NY, USA, 2017; ISBN 9781462534654. [Google Scholar]
- Crombez, G.; Van Damme, S.; Eccleston, C. Hypervigilance to pain: An experimental and clinical analysis. Pain 2005, 116, 4–7. [Google Scholar] [CrossRef]
- Pastor-Mira, M.A.; López-Roig, S.; Martínez-Zaragoza, F.; León, E.; Abad, E.; Lledó, A.; Peñacoba, C. Goal Preferences, Affect, Activity Patterns and Health Outcomes in Women with Fibromyalgia. Front. Psychol. 2019, 10, 1912. [Google Scholar] [CrossRef]
- Karsdorp, P.A.; Vlaeyen, J.W.S. Goals matter: Both achievement and pain-avoidance goals are associated with pain severity and disability in patients with low back and upper extremity pain. Pain 2011, 152, 1382–1390. [Google Scholar] [CrossRef] [PubMed]
- Vervoort, T.; Trost, Z. Examining Affective-Motivational Dynamics and Behavioral Implications within the Interpersonal Context of Pain. J. Pain 2017, 18, 1174–1183. [Google Scholar] [CrossRef] [PubMed]
- Lami, M.J.; Martínez, M.P.; Miró, E.; Sánchez, A.I.; Prados, G.; Cáliz, R.; Vlaeyen, J.W.S. Efficacy of Combined Cognitive-Behavioral Therapy for Insomnia and Pain in Patients with Fibromyalgia: A Randomized Controlled Trial. Cognit. Ther. Res. 2018, 42, 63–79. [Google Scholar] [CrossRef]
- Beal, C.C.; Stuifbergen, A.K.; Brown, A. Predictors of a health promoting lifestyle in women with fibromyalgia syndrome. Psychol. Health Med. 2009, 14, 343–353. [Google Scholar] [CrossRef] [PubMed]
- Oliver, K. Predictors of Exercise Behaviors among Fibromyalgia Patients. Prev. Med. 2002, 35, 383–389. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, S.R.; Tully, M.A.; Ryan, B.; Bleakley, C.M.; Baxter, G.D.; Bradley, J.M.; McDonough, S.M. Walking Exercise for Chronic Musculoskeletal Pain: Systematic Review and Meta-Analysis. Arch. Phys. Med. Rehabil. 2015, 96, 724–734.e3. [Google Scholar] [CrossRef]
- Pastor, M.-Á.; López-Roig, S.; Sanz, Y.; Peñacoba, C.; Cigarán, M.; Lledó, A.; Velasco, L.; Écija, C. Andar como forma de ejercicio físico en la Fibromialgia: Un estudio de identificación de creencias desde la Teoría de la Acción Planeada. An. Psicol. 2015, 31, 433. [Google Scholar] [CrossRef]
- Ellingson, L.D.; Stegner, A.J.; Schwabacher, I.J.; Lindheimer, J.B.; Cook, D.B. Catastrophizing Interferes with Cognitive Modulation of Pain in Women with Fibromyalgia. Pain Med. 2018, 19, 2408–2422. [Google Scholar] [CrossRef]
- Vlaeyen, J.W.S.; Kole-Snijders, A.M.J.; Boeren, R.G.B.; van Eek, H. Fear of movement/(re)injury in chronic low back pain and its relation to behavioral performance. Pain 1995, 62, 363–372. [Google Scholar] [CrossRef]
- Clauw, D.J.; Arnold, L.M.; McCarberg, B.H. The Science of Fibromyalgia. Mayo Clin. Proc. 2011, 86, 907–911. [Google Scholar] [CrossRef]
- Govender, C.; Cassimjee, N.; Schoeman, J.; Meyer, H. Psychological characteristics of FMS patients. Scand. J. Caring Sci. 2009, 23, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Esteve, R.; López-Martínez, A.E.; Peters, M.L.; Serrano-Ibáñez, E.R.; Ruíz-Párraga, G.T.; González-Gómez, H.; Ramírez-Maestre, C. Activity Pattern Profiles: Relationship with Affect, Daily Functioning, Impairment, and Variables Related to Life Goals. J. Pain 2017, 18, 546–555. [Google Scholar] [CrossRef] [PubMed]
- Velasco, L.; López-Gómez, I.; Gutiérrez, L.; Écija, C.; Catalá, P.; Peñacoba, C. Exploring the Preference for Fatigue-avoidance Goals as a Mediator between Pain Catastrophizing, Functional Impairment, and Walking Behavior in Women with Fibromyalgia. Clin. J. Pain 2022, 38, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Bennett, R.; Nelson, D. Cognitive behavioral therapy for fibromyalgia. Nat. Clin. Pract. Rheumatol. 2006, 2, 416–424. [Google Scholar] [CrossRef]
- Häuser, W.; Bernardy, K.; Arnold, B.; Offenbächer, M.; Schiltenwolf, M. Efficacy of multicomponent treatment in fibromyalgia syndrome: A meta-analysis of randomized controlled clinical trials. Arthritis Rheum. 2009, 61, 216–224. [Google Scholar] [CrossRef]
- Ang, D.C.; Kaleth, A.S.; Bigatti, S.; Mazzuca, S.A.; Jensen, M.P.; Hilligoss, J.; Slaven, J.; Saha, C. Research to Encourage Exercise for Fibromyalgia (REEF). Clin. J. Pain 2013, 29, 296–304. [Google Scholar] [CrossRef]
- Jones, K.D.; Burckhardt, C.S.; Bennett, J.A. Motivational interviewing may encourage exercise in persons with fibromyalgia by enhancing self efficacy. Arthritis Rheum. 2004, 51, 864–867. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Psychosocial Characteristics | Mean (SD) | Sample Range | 2. | 3. | 4. | 5. | 6. | 7. |
|---|---|---|---|---|---|---|---|---|
| 1. Pain severity | 7.40 (1.80) | 1–10 | 0.309 ** | 0.268 * | −0.234 * | 0.330 ** | 0.161 * | 0.234 ** |
| 2. Pain catastrophizing | 29.73 (11.24) | 6–52 | 0.220 * | −0.481 ** | 0.360 ** | 0.057 | −0.029 | |
| 3. Pain avoidance | 6.76 (2.78) | 0–12 | −0.270 ** | 0.065 | 0.284 | 0.081 | ||
| 4. Self-efficacy | 14.31 (9.02) | 0–35 | −0.345 ** | −0.051 | −0.020 | |||
| 5. General index of symptoms | 9.55 (1.77) | 3–12 | −0.043 | 0.106 | ||||
| 6. Diagnosis of FM | 12.32 (2.82) | 1–46 | 0.541 ** | |||||
| 7. Duration of FM | 24.22 (13.85) | 5–63 |
| VD: Pain Avoidance | R2 | F | p | Beta | t | p |
|---|---|---|---|---|---|---|
| Model summary | 0.38 | 2.71 | 0.010 | |||
| VI: Pain severity | −0.92 | −2.14 | 0.034 | |||
| W: Pain catastrophizing | −0.17 | −1.90 | 0.05 | |||
| Pain catastrophizing × Severity pain | 0.02 | 2.36 | 0.001 | |||
| General index of symptoms (covariate) | 0.08 | 0.54 | 0.583 | |||
| Time since FM diagnosis (covariate) | 0.02 | 0.38 | 0.702 | |||
| Time since onset of symptoms (covariate) | 0.04 | 0.32 | 0.743 | |||
| VD: Self-efficacy | R2 | F | p | Beta | t | p |
| Model summary | 0.49 | 6.21 | <0.001 | |||
| VI: Pain severity | −0.59 | 0.51 | 0.249 | |||
| M: Pain avoidance | −0.91 | 0.30 | 0.004 | |||
| General index of symptoms (covariate) | 0.08 | 0.54 | 0.583 | |||
| Time since FM diagnosis (covariate) | 0.02 | 0.38 | 0.702 | |||
| Time since onset of symptoms (covariate) | 0.04 | 0.32 | 0.743 |
| Pain Catastrophizing | Beta | SE | LL 95% CI | UL 95% CI |
|---|---|---|---|---|
| 1SD below the mean | 0.35 | 0.27 | −0.06 | 1.01 |
| Mean | 0.05 | 0.17 | −0.24 | 0.41 |
| 1SD above the mean | −0.24 | 0.26 | −0.77 | −0.04 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Catalá, P.; Gutiérrez, L.; Écija, C.; Peñacoba, C. How to Generate Self-Efficacy despite Pain: The Role of Catastrophizing and Avoidance in Women with Fibromyalgia. Biomedicines 2024, 12, 47. https://doi.org/10.3390/biomedicines12010047
Catalá P, Gutiérrez L, Écija C, Peñacoba C. How to Generate Self-Efficacy despite Pain: The Role of Catastrophizing and Avoidance in Women with Fibromyalgia. Biomedicines. 2024; 12(1):47. https://doi.org/10.3390/biomedicines12010047
Chicago/Turabian StyleCatalá, Patricia, Lorena Gutiérrez, Carmen Écija, and Cecilia Peñacoba. 2024. "How to Generate Self-Efficacy despite Pain: The Role of Catastrophizing and Avoidance in Women with Fibromyalgia" Biomedicines 12, no. 1: 47. https://doi.org/10.3390/biomedicines12010047
APA StyleCatalá, P., Gutiérrez, L., Écija, C., & Peñacoba, C. (2024). How to Generate Self-Efficacy despite Pain: The Role of Catastrophizing and Avoidance in Women with Fibromyalgia. Biomedicines, 12(1), 47. https://doi.org/10.3390/biomedicines12010047