
Association between the Use of Proton Pump Inhibitors and Cardiovascular Diseases: A Nested Case-Control Study Using a National Health Screening Cohort
 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Exposure (Proton Pump Inhibitors)
2.2. Outcome (Cardiovascular Diseases; CVDs)
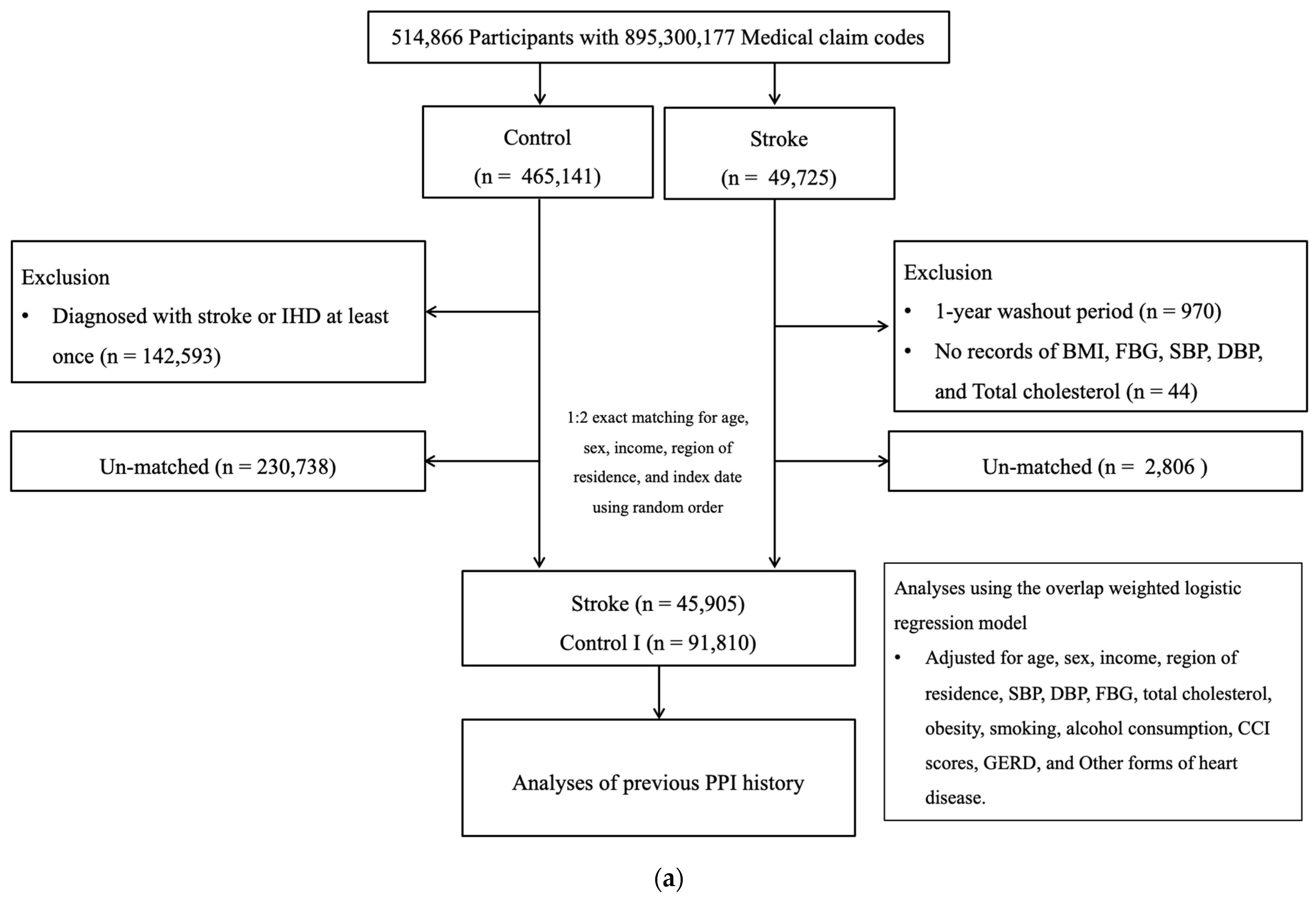
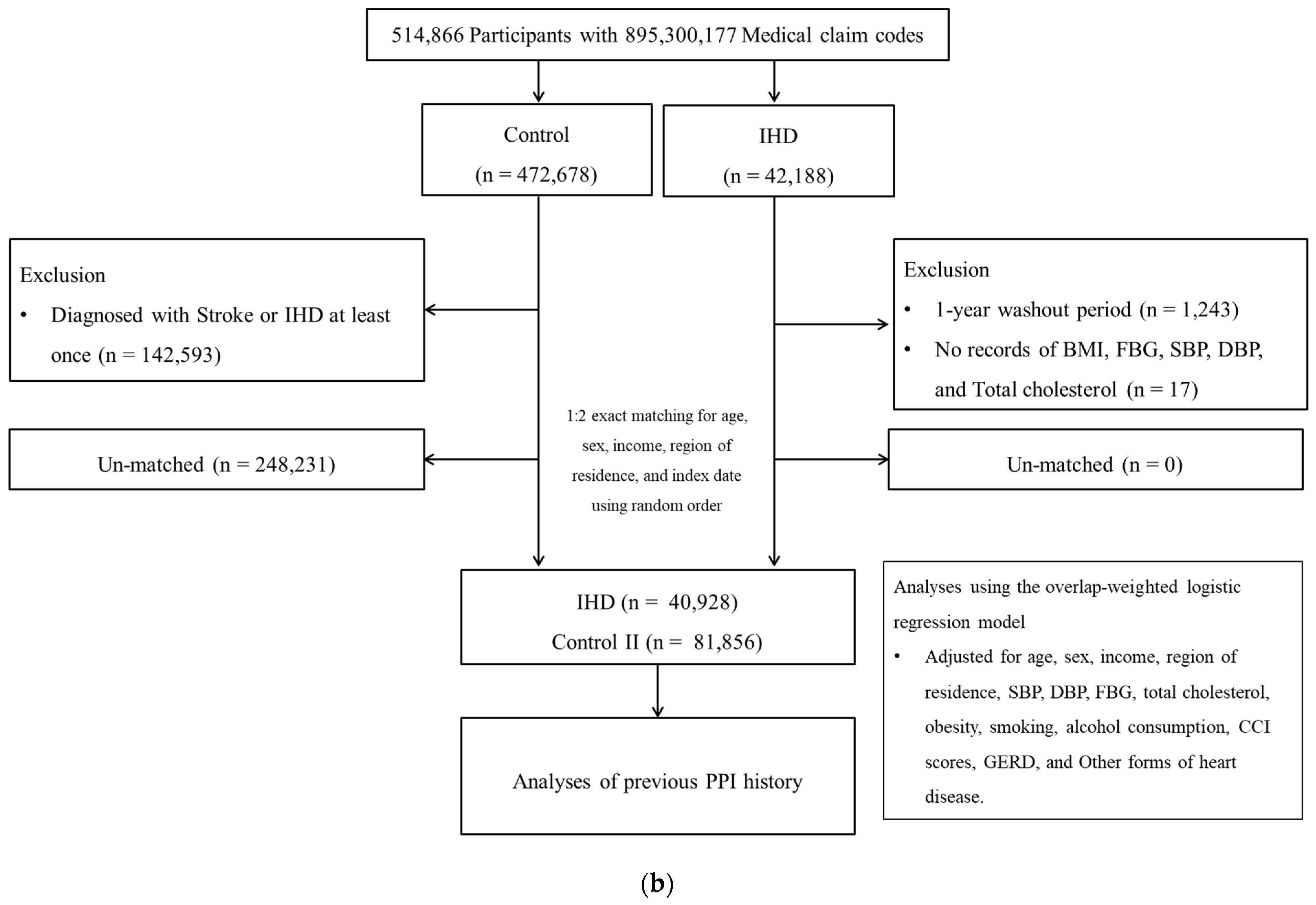
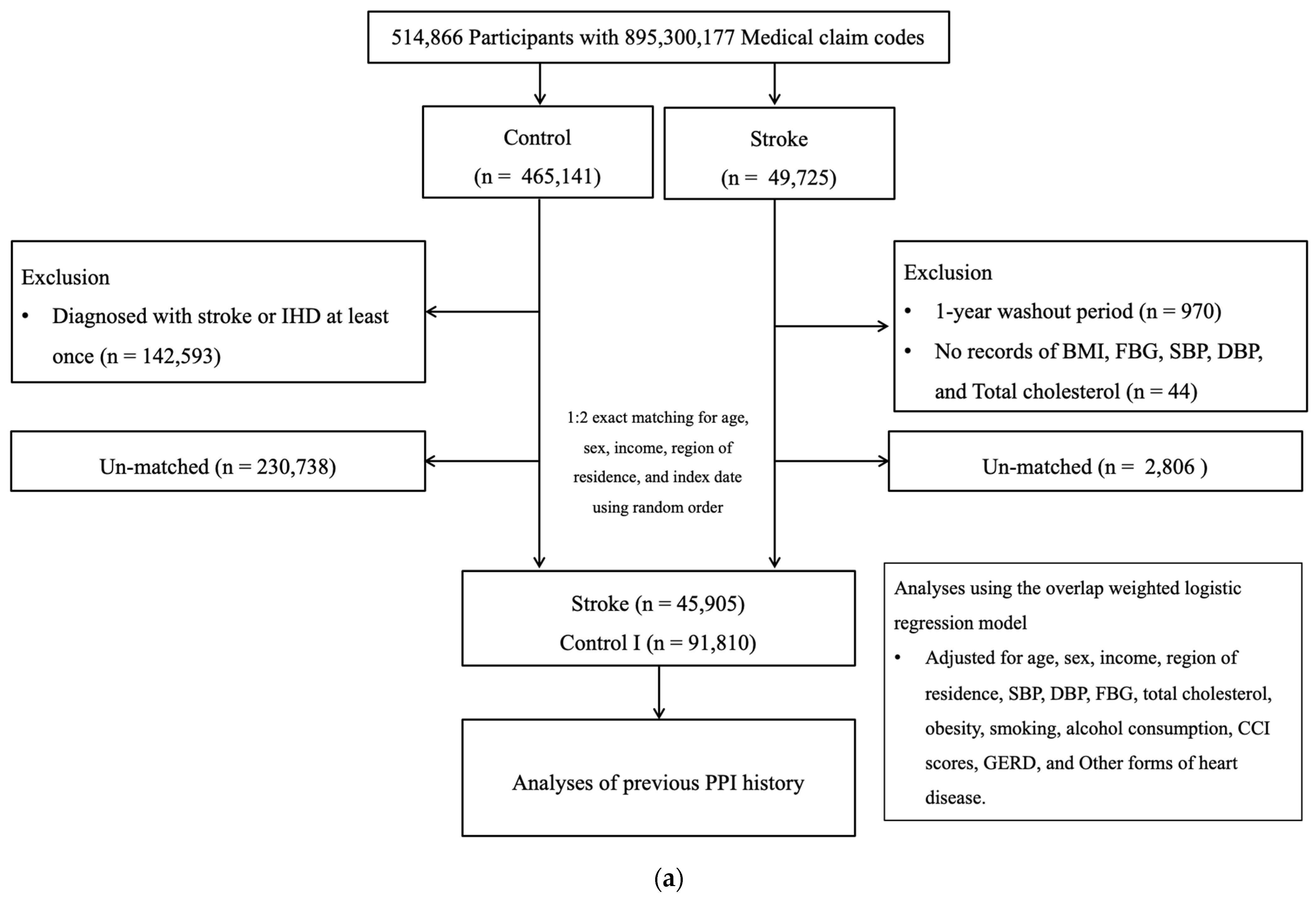
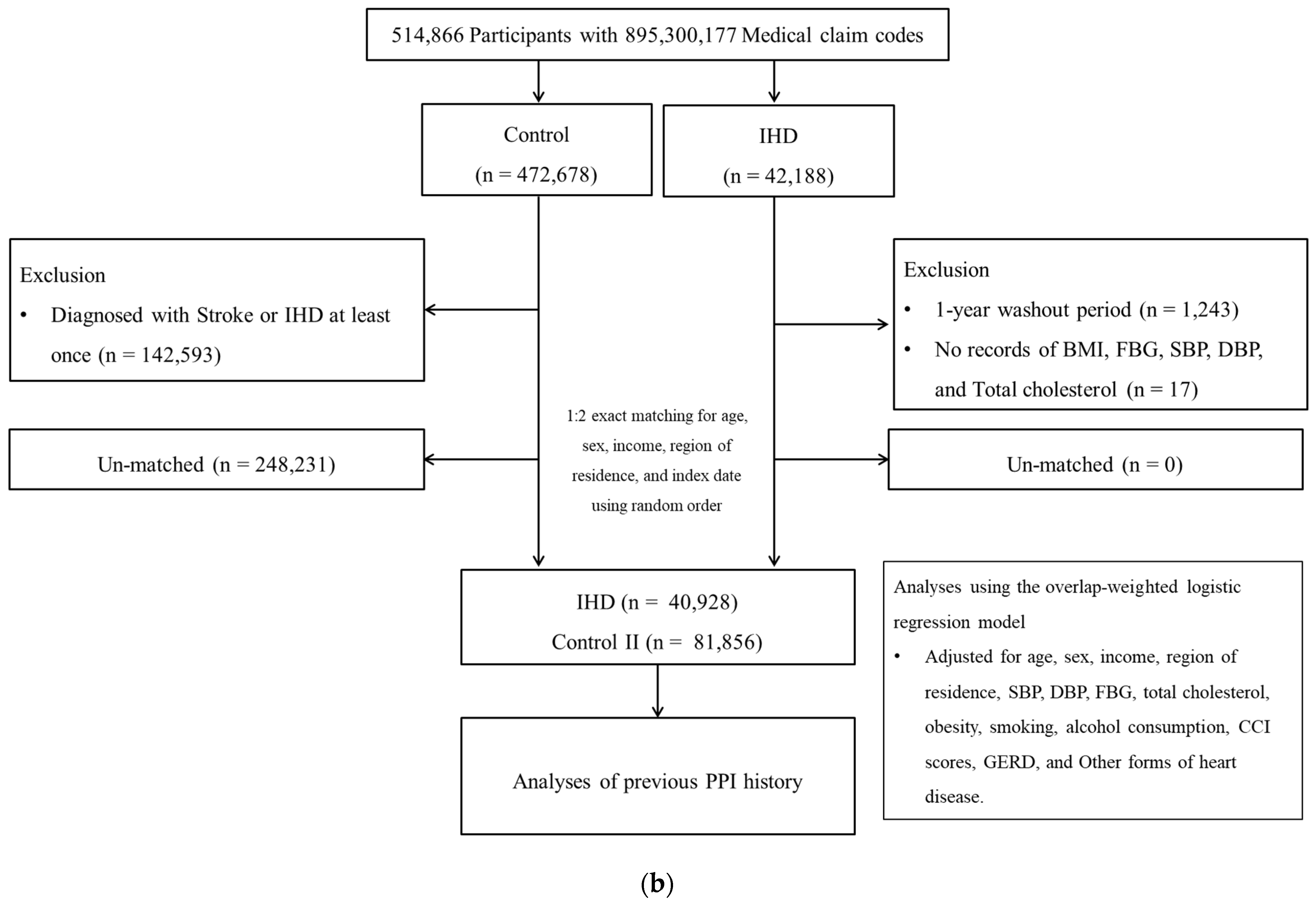
2.3. Participant Selection
2.3.1. Study I
2.3.2. Study II
2.4. Covariates
2.5. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schnoll-Sussman, F.; Niec, R.; Katz, P.O. Proton Pump Inhibitors: The Good, Bad, and Ugly. Gastrointest. Endosc. Clin. N. Am. 2020, 30, 239–251. [Google Scholar] [CrossRef] [PubMed]
- Katz, P.O.; Gerson, L.B.; Vela, M.F. Guidelines for the diagnosis and management of gastroesophageal reflux disease. Am. J. Gastroenterol. 2013, 108, 308–328. [Google Scholar] [CrossRef] [PubMed]
- Savarino, V.; Marabotto, E.; Zentilin, P.; Furnari, M.; Bodini, G.; De Maria, C.; Pellegatta, G.; Coppo, C.; Savarino, E. Proton pump inhibitors: Use and misuse in the clinical setting. Expert Rev. Clin. Pharmacol. 2018, 11, 1123–1134. [Google Scholar] [CrossRef]
- Koyyada, A. Long-term use of proton pump inhibitors as a risk factor for various adverse manifestations. Therapie 2021, 76, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Fossmark, R.; Martinsen, T.C.; Waldum, H.L. Adverse Effects of Proton Pump Inhibitors-Evidence and Plausibility. Int. J. Mol. Sci. 2019, 20, 5203. [Google Scholar] [CrossRef]
- Malfertheiner, P.; Kandulski, A.; Venerito, M. Proton-pump inhibitors: Understanding the complications and risks. Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 697–710. [Google Scholar] [CrossRef] [PubMed]
- Ariel, H.; Cooke, J.P. Cardiovascular Risk of Proton Pump Inhibitors. Methodist. Debakey Cardiovasc. J. 2019, 15, 214–219. [Google Scholar] [CrossRef] [PubMed]
- Hu, W.; Tong, J.; Kuang, X.; Chen, W.; Liu, Z. Influence of proton pump inhibitors on clinical outcomes in coronary heart disease patients receiving aspirin and clopidogrel: A meta-analysis. Medicine 2018, 97, e9638. [Google Scholar] [CrossRef]
- Cardoso, R.N.; Benjo, A.M.; DiNicolantonio, J.J.; Garcia, D.C.; Macedo, F.Y.B.; El-Hayek, G.; Nadkarni, G.N.; Gili, S.; Iannaccone, M.; Konstantinidis, I.; et al. Incidence of cardiovascular events and gastrointestinal bleeding in patients receiving clopidogrel with and without proton pump inhibitors: An updated meta-analysis. Open Heart 2015, 2, e000248. [Google Scholar] [CrossRef]
- Ghebremariam, Y.T.; LePendu, P.; Lee, J.C.; Erlanson, D.A.; Slaviero, A.; Shah, N.H.; Leiper, J.; Cooke, J.P. Unexpected effect of proton pump inhibitors: Elevation of the cardiovascular risk factor asymmetric dimethylarginine. Circulation 2013, 128, 845–853. [Google Scholar] [CrossRef]
- Batchelor, R.; Kumar, R.; Gilmartin-Thomas, J.F.M.; Hopper, I.; Kemp, W.; Liew, D. Systematic review with meta-analysis: Risk of adverse cardiovascular events with proton pump inhibitors independent of clopidogrel. Aliment. Pharmacol. Ther. 2018, 48, 780–796. [Google Scholar] [CrossRef] [PubMed]
- Shiraev, T.P.; Bullen, A. Proton Pump Inhibitors and Cardiovascular Events: A Systematic Review. Heart Lung Circ. 2018, 27, 443–450. [Google Scholar] [CrossRef]
- Choi, S.; Kim, K.; Kim, S.M.; Lee, G.; Jeong, S.-M.; Park, S.Y.; Kim, Y.-Y.; Son, J.S.; Yun, J.-M.; Park, S.M. Association of Obesity or Weight Change with Coronary Heart Disease Among Young Adults in South Korea. JAMA Intern. Med. 2018, 178, 1060–1068. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Park, S.M.; Lee, K. Weight gain after smoking cessation does not modify its protective effect on myocardial infarction and stroke: Evidence from a cohort study of men. Eur. Heart J. 2018, 39, 1523–1531. [Google Scholar] [CrossRef]
- Service, W.N.H.I.; National Health Insurance Service. National Health Insurance Sharing Service 2019. Available online: https://nhiss.nhis.or.kr/bd/ab/bdaba002cv.do (accessed on 1 December 2019).
- Seong, S.C.; Kim, Y.-Y.; Park, S.K.; Khang, Y.H.; Kim, H.C.; Park, J.H.; Kang, H.-J.; Do, C.-H.; Song, J.-S.; Lee, E.-J.; et al. Cohort profile: The National Health Insurance Service-National Health Screening Cohort (NHIS-HEALS) in Korea. BMJ Open. 2017, 7, e016640. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Lee, J.S.; Park, S.H.; Shin, S.A.; Kim, K. Cohort Profile: The National Health Insurance Service-National Sample Cohort (NHIS-NSC), South Korea. Int. J. Epidemiol. 2017, 46, e15. [Google Scholar] [CrossRef]
- Kim, S.Y.; Min, C.; Oh, D.J.; Choi, H.G. Bidirectional Association Between GERD and Asthma: Two Longitudinal Follow-Up Studies Using a National Sample Cohort. J. Allergy Clin. Immunol. Pract. 2020, 8, 1005–1013.e9. [Google Scholar] [CrossRef]
- Kim, S.Y.; Oh, D.J.; Park, B.; Choi, H.G. Bell’s palsy and obesity, alcohol consumption and smoking: A nested case-control study using a national health screening cohort. Sci. Rep. 2020, 10, 4248. [Google Scholar] [CrossRef]
- Quan, H.; Li, B.; Couris, C.M.; Fushimi, K.; Graham, P.; Hider, P.; Januel, J.-M.; Sundararajan, V. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.-C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med. Care. 2005, 43, 1130–1139. [Google Scholar] [CrossRef]
- Li, F.; Thomas, L.E.; Li, F. Addressing Extreme Propensity Scores via the Overlap Weights. Am. J. Epidemiol. 2019, 188, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Thomas, L.E.; Li, F.; Pencina, M.J. Overlap Weighting: A Propensity Score Method That Mimics Attributes of a Randomized Clinical Trial. JAMA 2020, 323, 2417–2418. [Google Scholar] [CrossRef] [PubMed]
- Teperikidis, E.; Boulmpou, A.; Potoupni, V.; Kundu, S.; Singh, B.; Papadopoulos, C. Does the long-term administration of proton pump inhibitors increase the risk of adverse cardiovascular outcomes? A ChatGPT powered umbrella review. Acta Cardiol. 2023, 78, 980–988. [Google Scholar] [CrossRef] [PubMed]
- Sehested, T.S.G.; Gerds, T.A.; Fosbøl, E.L.; Hansen, P.W.; Charlot, M.G.; Carlson, N.; Hlatky, M.A.; Torp-Pedersen, C.; Gislason, G.H. Long-term use of proton pump inhibitors, dose-response relationship and associated risk of ischemic stroke and myocardial infarction. J. Intern. Med. 2018, 283, 268–281. [Google Scholar] [CrossRef]
- Yang, M.; He, Q.; Gao, F.; Nirantharakumar, K.; Veenith, T.; Qin, X.; Page, A.T.; Wong, M.C.S.; Huang, J.; Kuo, Z.C.; et al. Regular use of proton-pump inhibitors and risk of stroke: A population-based cohort study and meta-analysis of randomized-controlled trials. BMC Med. 2021, 19, 316. [Google Scholar] [CrossRef] [PubMed]
- Chui, C.S.L.; Cheung, K.S.; Brown, J.P.; Douglas, I.J.; Wong, I.C.K.; Chan, E.W.; Wong, A.Y.S. Proton pump inhibitors and myocardial infarction: An application of active comparators in a self-controlled case series. Int. J. Epidemiol. 2023, 52, 899–907. [Google Scholar] [CrossRef]
- Lam, J.R.; Schneider, J.L.; Zhao, W.; Corley, D.A. Proton pump inhibitor and histamine 2 receptor antagonist use and vitamin B12 deficiency. JAMA 2013, 310, 2435–2442. [Google Scholar] [CrossRef]
- Imperatore, N.; Tortora, R.; Testa, A.; Gerbino, N.; Caporaso, N.; Rispo, A. Proton pump inhibitors as risk factor for metabolic syndrome and hepatic steatosis in coeliac disease patients on gluten-free diet. J. Gastroenterol. 2018, 53, 507–516. [Google Scholar] [CrossRef]
- Yuan, J.; He, Q.; Nguyen, L.H.; Wong, M.C.S.; Huang, J.; Yu, Y.; Xia, B.; Tang, Y.; He, Y.; Zhang, C. Regular use of proton pump inhibitors and risk of type 2 diabetes: Results from three prospective cohort studies. Gut 2021, 70, 1070–1077. [Google Scholar] [CrossRef]
- Shin, J.M.; Kim, N. Pharmacokinetics and pharmacodynamics of the proton pump inhibitors. J. Neurogastroenterol. Motil. 2013, 19, 25–35. [Google Scholar] [CrossRef]
- Min, Y.W.; Lim, S.W.; Lee, J.H.; Lee, H.L.; Lee, O.Y.; Park, J.M.; Choi, M.-G.; Rhee, P.-L. Prevalence of Extraesophageal Symptoms in Patients with Gastroesophageal Reflux Disease: A Multicenter Questionnaire-based Study in Korea. J. Neurogastroenterol. Motil. 2014, 20, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Horwitz, R.I.; Feinstein, A.R. The problem of “protopathic bias” in case-control studies. Am. J. Med. 1980, 68, 255–258. [Google Scholar] [CrossRef] [PubMed]
- Shanika, L.G.T.; Reynolds, A.; Pattison, S.; Braund, R. Proton pump inhibitor use: Systematic review of global trends and practices. Eur. J. Clin. Pharmacol. 2023, 79, 1159–1172. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | After PS Overlap Weighting Adjustment | After PS Overlap Weighting Adjustment | ||||
|---|---|---|---|---|---|---|
| Stroke | Control I | Standardized Difference | IHD | Control II | Standardized Difference | |
| Age (%) | 0.00 | 0.00 | ||||
| 40–44 | 43 (0.16) | 43 (0.16) | 140 (0.59) | 140 (0.59) | ||
| 45–49 | 553 (2.13) | 553 (2.13) | 871 (3.68) | 871 (3.68) | ||
| 50–54 | 1621 (6.24) | 1621 (6.24) | 1945 (8.23) | 1945 (8.23) | ||
| 55–59 | 3084 (11.87) | 3084 (11.87) | 3409 (14.41) | 3409 (14.41) | ||
| 60–64 | 3630 (13.97) | 3630 (13.97) | 3884 (16.42) | 3884 (16.42) | ||
| 65–69 | 4226 (16.26) | 4226 (16.26) | 4094 (17.31) | 4094 (17.31) | ||
| 70–74 | 4878 (18.77) | 4878 (18.77) | 3795 (16.05) | 3795 (16.05) | ||
| 75–79 | 4893 (18.83) | 4893 (18.83) | 3000 (12.69) | 3000 (12.69) | ||
| 80–84 | 2843 (10.94) | 2843 (10.94) | 1742 (7.37) | 1742 (7.37) | ||
| 85+ | 216 (0.83) | 216 (0.83) | 770 (3.26) | 770 (3.26) | ||
| Sex (%) | 0.00 | 0.00 | ||||
| Male | 14,005 (53.90) | 14,005 (53.90) | 14,538 (61.47) | 14,538 (61.47) | ||
| Female | 11,979 (46.10) | 11,979 (46.10) | 9113 (38.53) | 9113 (38.53) | ||
| Income (%) | 0.00 | 0.00 | ||||
| 1 (lowest) | 4718 (18.16) | 4718 (18.16) | 4009 (16.95) | 4009 (16.95) | ||
| 2 | 3211 (12.36) | 3211 (12.36) | 2848 (12.04) | 2848 (12.04) | ||
| 3 | 3976 (15.30) | 3976 (15.30) | 3517 (14.87) | 3517 (14.87) | ||
| 4 | 5480 (21.09) | 5480 (21.09) | 4922 (20.81) | 4922 (20.81) | ||
| 5 (highest) | 8600 (33.10) | 8600 (33.10) | 8356 (35.33) | 8356 (35.33) | ||
| Region of residence (%) | 0.00 | 0.00 | ||||
| Urban | 9945 (38.27) | 9945 (38.27) | 9917 (41.93) | 9917 (41.93) | ||
| Rural | 16,039 (61.73) | 16,039 (61.73) | 13,734 (58.07) | 13,734 (58.07) | ||
| Obesity † (%) | 0.00 | 0.00 | ||||
| Underweight | 883 (3.40) | 883 (3.40) | 662 (2.80) | 662 (2.80) | ||
| Normal | 9023 (34.72) | 9023 (34.72) | 7481 (31.63) | 7481 (31.63) | ||
| Overweight | 6865 (26.42) | 6865 (26.42) | 6426 (27.17) | 6426 (27.17) | ||
| Obese I | 8366 (32.20) | 8366 (32.20) | 8252 (34.89) | 8252 (34.89) | ||
| Obese II | 847 (3.26) | 847 (3.26) | 830 (3.51) | 830 (3.51) | ||
| Smoking status (%) | 0.00 | 0.00 | ||||
| Non-smoker | 17,625 (67.83) | 17,625 (67.83) | 14,996 (63.40) | 14,996 (63.40) | ||
| Past smoker | 2132 (8.21) | 2132 (8.21) | 2349 (9.93) | 2349 (9.93) | ||
| Current smoker | 6226 (23.96) | 6226 (23.96) | 6307 (26.67) | 6307 (26.67) | ||
| Alcohol consumption (%) | 0.00 | 0.00 | ||||
| <1 time a week | 19,021 (73.20) | 19,021 (73.20) | 17,040 (72.05) | 17,040 (72.05) | ||
| ≥1 time a week | 6963 (26.80) | 6963 (26.80) | 6611 (27.95) | 6611 (27.95) | ||
| SBP (Mean, SD) | 130.85 (13.71) | 130.85 (9.59) | 0.00 | 130.12 (12.97) | 130.12 (9.24) | 0.00 |
| DBP (Mean, SD) | 79.39 (8.61) | 79.39 (5.96) | 0.00 | 79.24 (8.25) | 79.24 (5.76) | 0.00 |
| FBG (Mean, SD) | 105.74 (25.97) | 105.74 (19.58) | 0.00 | 106.02 (25.14) | 106.02 (19.84) | 0.00 |
| Total cholesterol (Mean, SD) | 197.50 (31.58) | 197.50 (22.27) | 0.00 | 199.03 (31.41) | 199.03 (20.87) | 0.00 |
| CCI score (Mean, SD) | 1.36 (1.29) | 1.36 (1.14) | 0.00 | 1.21 (1.28) | 1.21 (1.01) | 0.00 |
| GERD for 1 year before index date (Mean, SD) | 0.62 (1.57) | 0.62 (1.26) | 0.00 | 0.66 (1.41) | 0.66 (1.41) | 0.00 |
| Other forms of heart disease (n, %) | 8151 (31.37) | 8151 (31.37) | 0.00 | 8769 (37.08) | 8769 (37.08) | 0.00 |
| Duration of PPI use (n, %) | 0.22 | 0.37 | ||||
| Non-user | 3434 (13.21) | 4677 (18.00) | 2377 (10.05) | 4392 (18.57) | ||
| <30 days | 2979 (11.47) | 4228 (16.27) | 2790 (11.80) | 4558 (19.27) | ||
| 30 to 180 days | 5747 (22.12) | 5081 (19.56) | 5454 (23.06) | 4855 (20.53) | ||
| ≥180 days | 13,824 (53.20) | 11,998 (46.17) | 13,029 (55.09) | 9845 (41.63) | ||
| Characteristics | N of Stroke | N of Control I | Odd Ratios for Stroke (95% Confidence Interval) | |||
|---|---|---|---|---|---|---|
| (Exposure/Total, %) | (Exposure/Total, %) | Crude | p-Value | Overlap-Weighted Model † | p-Value | |
| Duration of PPI use | ||||||
| Non-user | 5197/42,048 (12.4) | 16,893/84,096 (20.1) | 1 | 1 | ||
| <30 days | 4619/42,048 (11.0) | 14,852/84,096 (17.7) | 1.01 (0.97–1.06) | 0.639 | 0.96 (0.92–1.00) | 0.031 * |
| 30 to 180 days | 9052/42,048 (21.5) | 17,001/84,096 (20.2) | 1.73 (1.66–1.80) | <0.001 * | 1.55 (1.50–1.61) | <0.001 * |
| ≥180 days | 23,180/42,048 (55.1) | 35,350/84,096 (42.0) | 2.13 (2.06–2.21) | <0.001 * | 1.62 (1.57–1.68) | <0.001 * |
| Characteristics | N of IHD | N of Control II | Odd Ratios for IHD (95% Confidence Interval) | |||
|---|---|---|---|---|---|---|
| (Exposure/Total, %) | (Exposure/Total, %) | Crude | p-Value | Overlap-Weighted Model † | p-Value | |
| Duration of PPI use | ||||||
| Non-user | 3795/40,928 (9.3) | 16,917/81,856 (20.7) | 1 | 1 | ||
| <30 days | 4551/40,928 (11.1) | 17,202/81,856 (21.0) | 1.18 (1.12–1.24) | <0.001 * | 1.13 (1.08–1.18) | <0.001 * |
| 30 to 180 days | 9157/40,928 (22.4) | 17,124/81,856 (20.9) | 2.38 (2.28–2.49) | <0.001 * | 2.12 (2.04–2.21) | <0.001 * |
| ≥180 days | 23,425/40,928 (57.2) | 30,613/81,856 (37.4 | 3.41 (3.28–3.55) | <0.001 * | 2.60 (2.51–2.69) | <0.001 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jang, S.; Choi, H.G.; Kwon, M.J.; Kim, J.H.; Kim, J.-H.; Kim, Y.; Kim, S.Y. Association between the Use of Proton Pump Inhibitors and Cardiovascular Diseases: A Nested Case-Control Study Using a National Health Screening Cohort. Biomedicines 2024, 12, 170. https://doi.org/10.3390/biomedicines12010170
Jang S, Choi HG, Kwon MJ, Kim JH, Kim J-H, Kim Y, Kim SY. Association between the Use of Proton Pump Inhibitors and Cardiovascular Diseases: A Nested Case-Control Study Using a National Health Screening Cohort. Biomedicines. 2024; 12(1):170. https://doi.org/10.3390/biomedicines12010170
Chicago/Turabian StyleJang, Sarang, Hyo Geun Choi, Mi Jung Kwon, Ji Hee Kim, Joo-Hee Kim, Yoonjoong Kim, and So Young Kim. 2024. "Association between the Use of Proton Pump Inhibitors and Cardiovascular Diseases: A Nested Case-Control Study Using a National Health Screening Cohort" Biomedicines 12, no. 1: 170. https://doi.org/10.3390/biomedicines12010170
APA StyleJang, S., Choi, H. G., Kwon, M. J., Kim, J. H., Kim, J.-H., Kim, Y., & Kim, S. Y. (2024). Association between the Use of Proton Pump Inhibitors and Cardiovascular Diseases: A Nested Case-Control Study Using a National Health Screening Cohort. Biomedicines, 12(1), 170. https://doi.org/10.3390/biomedicines12010170