
Brain Plasticity Modulator p75 Neurotrophin Receptor in Human Urine after Different Acute Brain Injuries—A Prospective Cohort Study

 , , , and
, , , and
Abstract

1. Introduction
2. Materials and Methods
2.1. Study Methods and Participants
2.2. Study Approval and Ethics
2.3. Assessment of Biomarkers
2.4. Statistical Analysis
3. Results
3.1. Demographics and Disease Characteristics of Enrolled Patients
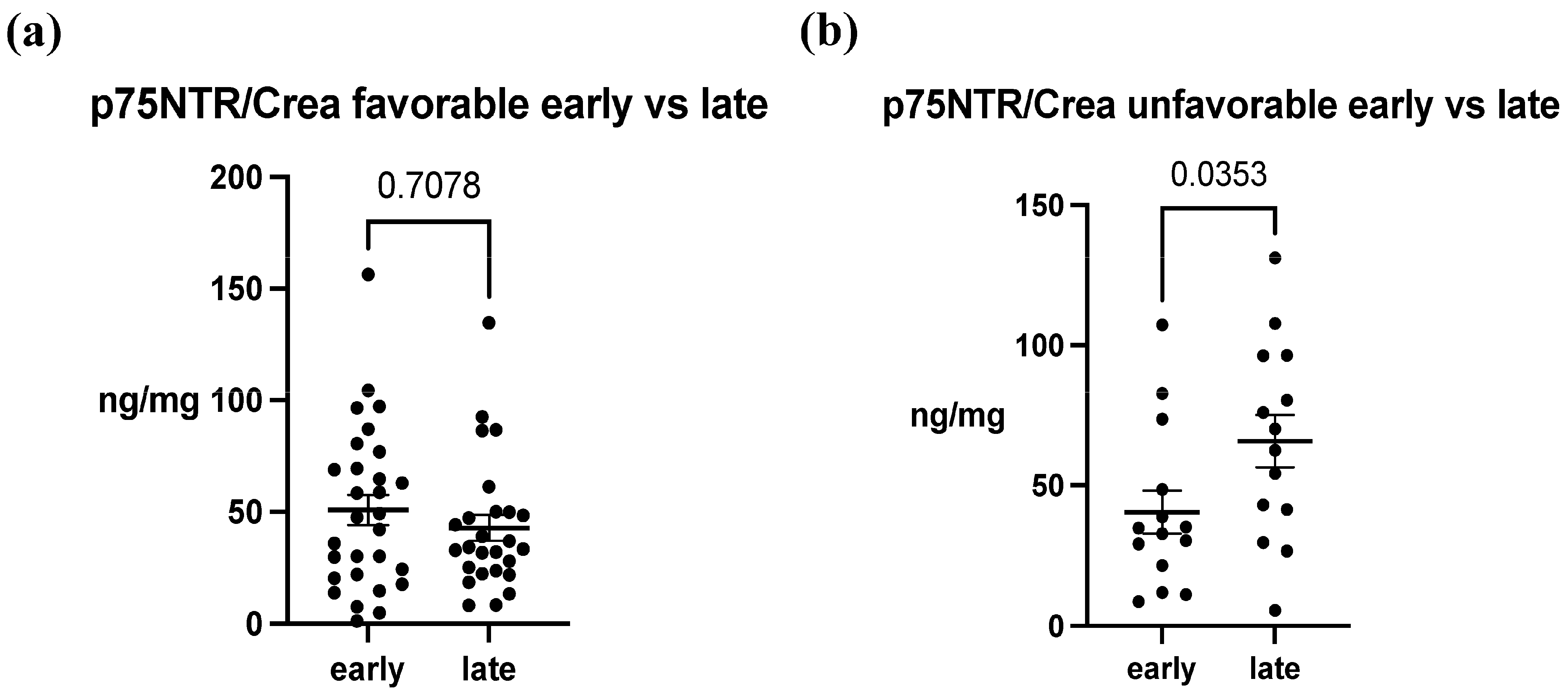
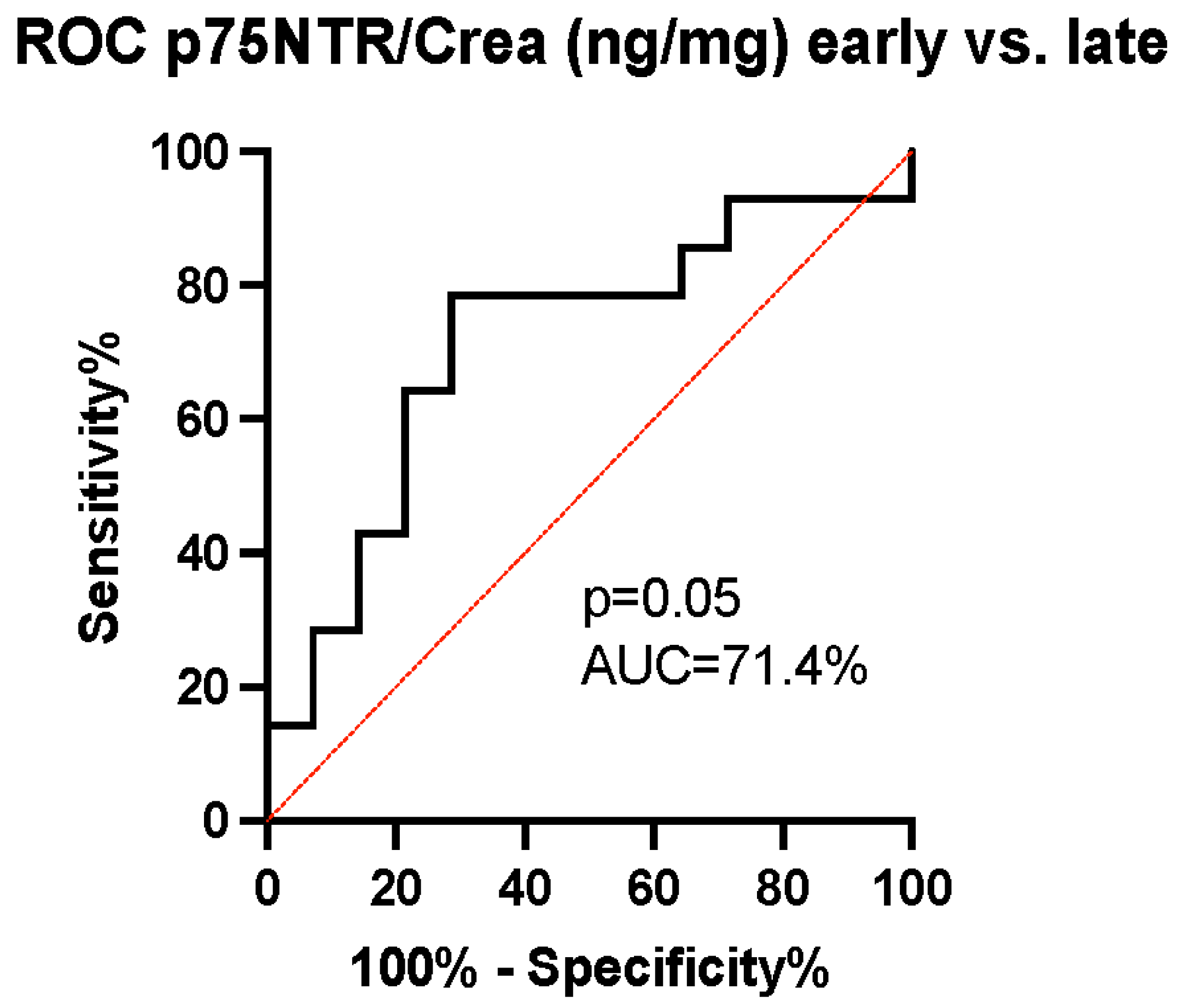
3.2. p75NTR in Urine after ABIs
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Feigin, V.L.; Brainin, M.; Norrving, B.; Martins, S.; Sacco, R.L.; Hacke, W.; Fisher, M.; Pandian, J.; Lindsay, P. World Stroke Organization (WSO): Global Stroke Fact Sheet 2022. Int. J. Stroke 2022, 17, 18–29. [Google Scholar] [CrossRef] [PubMed]
- Capizzi, A.; Woo, J.; Verduzco-Gutierrez, M. Traumatic Brain Injury: An Overview of Epidemiology, Pathophysiology, and Medical Management. Med. Clin. N. Am. 2020, 104, 213–238. [Google Scholar] [CrossRef] [PubMed]
- Galgano, M.; Toshkezi, G.; Qiu, X.; Russell, T.; Chin, L.; Zhao, L.-R. Traumatic Brain Injury: Current Treatment Strategies and Future Endeavors. Cell Transplant. 2017, 26, 1118–1130. [Google Scholar] [CrossRef] [PubMed]
- Long, B.; Koyfman, A.; Runyon, M.S. Subarachnoid Hemorrhage: Updates in Diagnosis and Management. Emerg. Med. Clin. N. Am. 2017, 35, 803–824. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.; Gao, S.; Wang, Y.; Xu, A.; Li, Y.; Wang, D. Classifying Ischemic Stroke, from TOAST to CISS. CNS Neurosci. Ther. 2012, 18, 452–456. [Google Scholar] [CrossRef] [PubMed]
- Rabinstein, A.A. Update on Treatment of Acute Ischemic Stroke. Contin. Minneap. Minn. 2020, 26, 268–286. [Google Scholar] [CrossRef] [PubMed]
- Hannah, T.C.; Kellner, R.; Kellner, C.P. Minimally Invasive Intracerebral Hemorrhage Evacuation Techniques: A Review. Diagnostics 2021, 11, 576. [Google Scholar] [CrossRef]
- van Essen, T.A.; Lingsma, H.F.; Pisică, D.; Singh, R.D.; Volovici, V.; den Boogert, H.F.; Younsi, A.; Peppel, L.D.; Heijenbrok-Kal, M.H.; Ribbers, G.M.; et al. Surgery versus conservative treatment for traumatic acute subdural haematoma: A prospective, multicentre, observational, comparative effectiveness study. Lancet Neurol. 2022, 21, 620–631. [Google Scholar] [CrossRef]
- Bendszus, M.; Fiehler, J.; Subtil, F.; Bonekamp, S.; Aamodt, A.H.; Fuentes, B.; Gizewski, E.R.; Hill, M.D.; Krajina, A.; Pierot, L.; et al. Endovascular thrombectomy for acute ischaemic stroke with established large infarct: Multicentre, open-label, randomised trial. Lancet 2023, 402, 1753–1763. [Google Scholar] [CrossRef]
- Molyneux, A.J.; Kerr, R.S.C.; Yu, L.-M.; Clarke, M.; Sneade, M.; Yarnold, J.A.; Sandercock, P. International Subarachnoid Aneurysm Trial (ISAT) Collaborative Group International subarachnoid aneurysm trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: A randomised comparison of effects on survival, dependency, seizures, rebleeding, subgroups, and aneurysm occlusion. Lancet 2005, 366, 809–817. [Google Scholar] [CrossRef]
- Pischiutta, F.; Sammali, E.; Parolini, O.; Carswell, H.V.O.; Zanier, E.R. Placenta-Derived Cells for Acute Brain Injury. Cell Transplant. 2018, 27, 151–167. [Google Scholar] [CrossRef] [PubMed]
- Coleman, E.R.; Moudgal, R.; Lang, K.; Hyacinth, H.I.; Awosika, O.O.; Kissela, B.M.; Feng, W. Early Rehabilitation After Stroke: A Narrative Review. Curr. Atheroscler. Rep. 2017, 19, 59. [Google Scholar] [CrossRef] [PubMed]
- Stewart, J.C.; Cramer, S.C. Genetic Variation and Neuroplasticity: Role in Rehabilitation After Stroke. J. Neurol. Phys. Ther. JNPT 2017, 41 (Suppl. S3), S17–S23. [Google Scholar] [CrossRef] [PubMed]
- Sr, B. Stroke Rehabilitation. Contin. Minneap. Minn. 2017, 23, 238–253. [Google Scholar] [CrossRef]
- Meeker, R.B.; Williams, K.S. The p75 neurotrophin receptor: At the crossroad of neural repair and death. Neural Regen. Res. 2015, 10, 721–725. [Google Scholar] [CrossRef] [PubMed]
- Reichardt, L.F. Neurotrophin-regulated signalling pathways. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2006, 361, 1545–1564. [Google Scholar] [CrossRef] [PubMed]
- Colucci-D’Amato, L.; Speranza, L.; Volpicelli, F. Neurotrophic Factor BDNF, Physiological Functions and Therapeutic Potential in Depression, Neurodegeneration and Brain Cancer. Int. J. Mol. Sci. 2020, 21, 7777. [Google Scholar] [CrossRef] [PubMed]
- Nykjaer, A.; Lee, R.; Teng, K.K.; Jansen, P.; Madsen, P.; Nielsen, M.S.; Jacobsen, C.; Kliemannel, M.; Schwarz, E.; Willnow, T.E.; et al. Sortilin is essential for proNGF-induced neuronal cell death. Nature 2004, 427, 843–848. [Google Scholar] [CrossRef]
- Dasgupta, S.; Montroull, L.E.; Pandya, M.A.; Zanin, J.P.; Wang, W.; Wu, Z.; Friedman, W.J. Cortical Brain Injury Causes Retrograde Degeneration of Afferent Basal Forebrain Cholinergic Neurons via the p75NTR. eNeuro 2023, 10, ENEURO.0067-23.2023. [Google Scholar] [CrossRef]
- Underwood, C.K.; Coulson, E.J. The p75 neurotrophin receptor. Int. J. Biochem. Cell Biol. 2008, 40, 1664–1668. [Google Scholar] [CrossRef]
- Knowles, J.K.; Rajadas, J.; Nguyen, T.-V.V.; Yang, T.; LeMieux, M.C.; Vander Griend, L.; Ishikawa, C.; Massa, S.M.; Wyss-Coray, T.; Longo, F.M. The p75 Neurotrophin Receptor Promotes Amyloid-β(1-42)-Induced Neuritic Dystrophy In Vitro and In Vivo. J. Neurosci. 2009, 29, 10627–10637. [Google Scholar] [CrossRef] [PubMed]
- Sebastiani, A.; Gölz, C.; Werner, C.; Schäfer, M.K.E.; Engelhard, K.; Thal, S.C. Proneurotrophin Binding to P75 Neurotrophin Receptor (P75ntr) Is Essential for Brain Lesion Formation and Functional Impairment after Experimental Traumatic Brain Injury. J. Neurotrauma 2015, 32, 1599–1607. [Google Scholar] [CrossRef] [PubMed]
- Brito, V.; Giralt, A.; Enriquez-Barreto, L.; Puigdellívol, M.; Suelves, N.; Zamora-Moratalla, A.; Ballesteros, J.J.; Martín, E.D.; Dominguez-Iturza, N.; Morales, M.; et al. Neurotrophin receptor p75NTR mediates Huntington’s disease–associated synaptic and memory dysfunction. J. Clin. Investig. 2014, 124, 4411–4428. [Google Scholar] [CrossRef] [PubMed]
- Mirzahosseini, G.; Ismael, S.; Salman, M.; Kumar, S.; Ishrat, T. Genetic and Pharmacological Modulation of P75 Neurotrophin Receptor Attenuate Brain Damage After Ischemic Stroke in Mice. Mol. Neurobiol. 2023. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Mattingly, A.; Lin, A.; Sacramento, J.; Mannent, L.; Castel, M.-N.; Canolle, B.; Delbary-Gossart, S.; Ferzaz, B.; Morganti, J.M.; et al. A novel antagonist of p75NTR reduces peripheral expansion and CNS trafficking of pro-inflammatory monocytes and spares function after traumatic brain injury. J. Neuroinflam. 2016, 13, 88. [Google Scholar] [CrossRef] [PubMed]
- Delbary-Gossart, S.; Lee, S.; Baroni, M.; Lamarche, I.; Arnone, M.; Canolle, B.; Lin, A.; Sacramento, J.; Salegio, E.A.; Castel, M.-N.; et al. A novel inhibitor of p75-neurotrophin receptor improves functional outcomes in two models of traumatic brain injury. Brain 2016, 139, 1762–1782. [Google Scholar] [CrossRef]
- Ritala, J.F.; Lyne, S.B.; Sajanti, A.; Girard, R.; Koskimäki, J. Towards a comprehensive understanding of p75 neurotrophin receptor functions and interactions in the brain. Neural Regen. Res. 2022, 17, 701–704. [Google Scholar] [CrossRef]
- Qin, X.; Wang, J.; Chen, S.; Liu, G.; Wu, C.; Lv, Q.; He, X.; Bai, X.; Huang, W.; Liao, H. Astrocytic p75NTR expression provoked by ischemic stroke exacerbates the blood-brain barrier disruption. Glia 2022, 70, 892–912. [Google Scholar] [CrossRef]
- Malik, S.C.; Sozmen, E.G.; Baeza-Raja, B.; Le Moan, N.; Akassoglou, K.; Schachtrup, C. In vivo functions of p75NTR: Challenges and opportunities for an emerging therapeutic target. Trends Pharmacol. Sci. 2021, 42, 772–788. [Google Scholar] [CrossRef]
- Nguyen, T.-V.V.; Crumpacker, R.H.; Calderon, K.E.; Garcia, F.G.; Zbesko, J.C.; Frye, J.B.; Gonzalez, S.; Becktel, D.A.; Yang, T.; Tavera-Garcia, M.A.; et al. Post-Stroke Administration of the p75 Neurotrophin Receptor Modulator, LM11A-31, Attenuates Chronic Changes in Brain Metabolism, Increases Neurotransmitter Levels, and Improves Recovery. J. Pharmacol. Exp. Ther. 2022, 380, 126–141. [Google Scholar] [CrossRef]
- Nasoohi, S.; Tayefeh Ghahremani, P.; Alehossein, P.; Elyasizadeh, S.; BaniArdalan, S.; Ismael, S.; Vatanpour, H.; Ahmadiani, A.; Ishrat, T. The p75 neurotrophin receptor inhibitor, LM11A-31, ameliorates acute stroke injury and modulates astrocytic proNGF. Exp. Neurol. 2023, 359, 114161. [Google Scholar] [CrossRef] [PubMed]
- Jia, R.; Shepheard, S.; Jin, J.; Hu, F.; Zhao, X.; Xue, L.; Xiang, L.; Qi, H.; Qu, Q.; Guo, F.; et al. Urinary Extracellular Domain of Neurotrophin Receptor p75 as a Biomarker for Amyotrophic Lateral Sclerosis in a Chinese cohort. Sci. Rep. 2017, 7, 5127. [Google Scholar] [CrossRef] [PubMed]
- Shepheard, S.R.; Wuu, J.; Cardoso, M.; Wiklendt, L.; Dinning, P.G.; Chataway, T.; Schultz, D.; Benatar, M.; Rogers, M.-L. Urinary p75ECD: A prognostic, disease progression, and pharmacodynamic biomarker in ALS. Neurology 2017, 88, 1137–1143. [Google Scholar] [CrossRef]
- Shepheard, S.R.; Chataway, T.; Schultz, D.W.; Rush, R.A.; Rogers, M.-L. The extracellular domain of neurotrophin receptor p75 as a candidate biomarker for amyotrophic lateral sclerosis. PLoS ONE 2014, 9, e87398. [Google Scholar] [CrossRef] [PubMed]
- Connolly, E.S.; Rabinstein, A.A.; Carhuapoma, J.R.; Derdeyn, C.P.; Dion, J.; Higashida, R.T.; Hoh, B.L.; Kirkness, C.J.; Naidech, A.M.; Ogilvy, C.S.; et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: A guideline for healthcare professionals from the American Heart Association/american Stroke Association. Stroke 2012, 43, 1711–1737. [Google Scholar] [CrossRef] [PubMed]
- Guidelines for the Early Management of Patients with Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association—PubMed. Available online: https://pubmed-ncbi-nlm-nih-gov.libproxy.tuni.fi/31662037/ (accessed on 4 November 2023).
- Carney, N.; Totten, A.M.; O’Reilly, C.; Ullman, J.S.; Hawryluk, G.W.J.; Bell, M.J.; Bratton, S.L.; Chesnut, R.; Harris, O.A.; Kissoon, N.; et al. Guidelines for the Management of Severe Traumatic Brain Injury, Fourth Edition. Neurosurgery 2017, 80, 6–15. [Google Scholar] [CrossRef] [PubMed]
- Motulsky, H.J.; Brown, R.E. Detecting outliers when fitting data with nonlinear regression—A new method based on robust nonlinear regression and the false discovery rate. BMC Bioinform. 2006, 7, 123. [Google Scholar] [CrossRef]
- Irmady, K.; Jackman, K.A.; Padow, V.A.; Shahani, N.; Martin, L.A.; Cerchietti, L.; Unsicker, K.; Iadecola, C.; Hempstead, B.L. MiR-592 Regulates the Induction and Cell Death-Promoting Activity of p75NTR in Neuronal Ischemic Injury. J. Neurosci. 2014, 34, 3419–3428. [Google Scholar] [CrossRef]
- Jiao, S.S.; Bu, X.L.; Liu, Y.H.; Wang, Q.H.; Liu, C.H.; Yao, X.Q.; Zhou, X.F.; Wang, Y.J. Differential levels of p75NTR ectodomain in CSF and blood in patients with Alzheimer’s disease: A novel diagnostic marker. Transl. Psychiatry 2015, 5, e650. [Google Scholar] [CrossRef]
- Kokaia, Z.; Andsberg, G.; Martinez-Serrano, A.; Lindvall, O. Focal cerebral ischemia in rats induces expression of P75 neurotrophin receptor in resistant striatal cholinergic neurons. Neuroscience 1998, 84, 1113–1125. [Google Scholar] [CrossRef]
- Kraemer, B.R.; Snow, J.P.; Vollbrecht, P.; Pathak, A.; Valentine, W.M.; Deutch, A.Y.; Carter, B.D. A role for the p75 neurotrophin receptor in axonal degeneration and apoptosis induced by oxidative stress. J. Biol. Chem. 2014, 289, 21205–21216. [Google Scholar] [CrossRef] [PubMed]
- Gaidin, S.G.; Turovskaya, M.V.; Gavrish, M.S.; Babaev, A.A.; Mal’Tseva, V.N.; Blinova, E.V.; Turovsky, E.A. The selective BDNF overexpression in neurons protects neuroglial networks against OGD and glutamate-induced excitotoxicity. Int. J. Neurosci. 2020, 130, 363–383. [Google Scholar] [CrossRef] [PubMed]
- Turovskaya, M.V.; Gaidin, S.G.; Vedunova, M.V.; Babaev, A.A.; Turovsky, E.A. BDNF Overexpression Enhances the Preconditioning Effect of Brief Episodes of Hypoxia, Promoting Survival of GABAergic Neurons. Neurosci. Bull. 2020, 36, 733–760. [Google Scholar] [CrossRef] [PubMed]
- Koskimäki, J.; Matsui, N.; Umemori, J.; Rantamäki, T.; Castrén, E. Nimodipine activates TrkB neurotrophin receptors and induces neuroplastic and neuroprotective signaling events in the mouse hippocampus and prefrontal cortex. Cell. Mol. Neurobiol. 2015, 35, 189–196. [Google Scholar] [CrossRef]
- Harpole, M.; Davis, J.; Espina, V. Current state of the art for enhancing urine biomarker discovery. Expert Rev. Proteom. 2016, 13, 609–626. [Google Scholar] [CrossRef]
- Trindade, F.; Barros, A.S.; Silva, J.; Vlahou, A.; Falcão-Pires, I.; Guedes, S.; Vitorino, C.; Ferreira, R.; Leite-Moreira, A.; Amado, F.; et al. Mining the Biomarker Potential of the Urine Peptidome: From Amino Acids Properties to Proteases. Int. J. Mol. Sci. 2021, 22, 5940. [Google Scholar] [CrossRef]
- Maier, B.; Lehnert, M.; Laurer, H.L.; Mautes, A.E.; Steudel, W.I.; Marzi, I. Delayed elevation of soluble tumor necrosis factor receptors p75 and p55 in cerebrospinal fluid and plasma after traumatic brain injury. Shock. Augusta Ga 2006, 26, 122–127. [Google Scholar] [CrossRef]
- Ertel, W.; Keel, M.; Bonaccio, M.; Steckholzer, U.; Gallati, H.; Kenney, J.S.; Trentz, O. Release of anti-inflammatory mediators after mechanical trauma correlates with severity of injury and clinical outcome. J. Trauma 1995, 39, 879–885; Discussion in 885–887. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Favorable (n = 30) | Unfavorable (n = 16) | p-Value |
|---|---|---|---|
| Age in years | 0.7283 | ||
| Mean ± SD | 57.3 ± 13.3 | 58.8 ± 13.7 | |
| Min–Max | 23.0–75.0 | 34.0–74.0 | |
| Median (IQR) | 60.0 (48.0–68.0) | 65.0 (45.0–70.0) | |
| Sex | 0.9783 | ||
| Male | 17 (56.7) | 9 (56.3) | |
| Female | 13 (43.3) | 7 (43.8) | |
| Type of brain injury | 0.0373 | ||
| aSAH | 13 (43.3) | 9 (56.3) | |
| TBI | 3 (10.0) | 5 (31.3) | |
| IS | 14 (46.7) | 2 (12.5) | |
| p75NTR/Crea Early (ng/mg) | 0.3537 | ||
| Mean ± SD | 50.86 ± 36.10 | 40.49 ± 28.83 | |
| Min–Max | 1.3–156.4 | 8.7–107.3 | |
| Median (IQR) | 47.65 (21.3–73.2) | 33.80 (19.2–54.8) | |
| p75NTR/Crea Late (ng/mg) | 0.0325 | ||
| Mean ± SD | 42.79 ± 29.24 | 65.85 ± 35.04 | |
| Min–Max | 8.3–134.7 | 5.6–131.2 | |
| Median (IQR) | 33.84 (23.4–50.0) | 66.40 (38.5–96.4) | |
| p75NTR/Crea Healthy (ng/mg) | Healthy (n = 4) | <0.0001 † | |
| Mean ± SD | 0.542 ± 0.440 0.084–1.124 0.479 (0.155–0.991) | ||
| Min–Max | |||
| Median (IQR) | |||
| Age in years | >0.05 ‡ | ||
| Mean ± SD | 44.00 ± 16.95 | ||
| Min–Max | 33.0–69.0 | ||
| Median (IQR) | 37.0 (33.3–62.8) | ||
| Sex | >0.05 ‡ | ||
| Male | 2 (50.0) | ||
| Female | 2 (50.0) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hellström, S.; Sajanti, A.; Srinath, A.; Bennett, C.; Girard, R.; Cao, Y.; Frantzén, J.; Koskimäki, F.; Falter, J.; Lyne, S.B.; et al. Brain Plasticity Modulator p75 Neurotrophin Receptor in Human Urine after Different Acute Brain Injuries—A Prospective Cohort Study. Biomedicines 2024, 12, 112. https://doi.org/10.3390/biomedicines12010112
Hellström S, Sajanti A, Srinath A, Bennett C, Girard R, Cao Y, Frantzén J, Koskimäki F, Falter J, Lyne SB, et al. Brain Plasticity Modulator p75 Neurotrophin Receptor in Human Urine after Different Acute Brain Injuries—A Prospective Cohort Study. Biomedicines. 2024; 12(1):112. https://doi.org/10.3390/biomedicines12010112
Chicago/Turabian StyleHellström, Santtu, Antti Sajanti, Abhinav Srinath, Carolyn Bennett, Romuald Girard, Ying Cao, Janek Frantzén, Fredrika Koskimäki, Johannes Falter, Seán B. Lyne, and et al. 2024. "Brain Plasticity Modulator p75 Neurotrophin Receptor in Human Urine after Different Acute Brain Injuries—A Prospective Cohort Study" Biomedicines 12, no. 1: 112. https://doi.org/10.3390/biomedicines12010112
APA StyleHellström, S., Sajanti, A., Srinath, A., Bennett, C., Girard, R., Cao, Y., Frantzén, J., Koskimäki, F., Falter, J., Lyne, S. B., Rantamäki, T., Takala, R., Posti, J. P., Roine, S., Puolitaival, J., Jänkälä, M., Kolehmainen, S., Rahi, M., Rinne, J., ... Koskimäki, J. (2024). Brain Plasticity Modulator p75 Neurotrophin Receptor in Human Urine after Different Acute Brain Injuries—A Prospective Cohort Study. Biomedicines, 12(1), 112. https://doi.org/10.3390/biomedicines12010112