
Precision Medicine in Pancreatic Ductal Adenocarcinoma: The Impact of Targeted Therapies on Survival of Patients Harboring Actionable Mutations
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Genomic Analyses
- MOSCATO
- RAGNAR trial
- STARTRK trial
2.3. Treatment Decision
2.4. Statistical Analysis
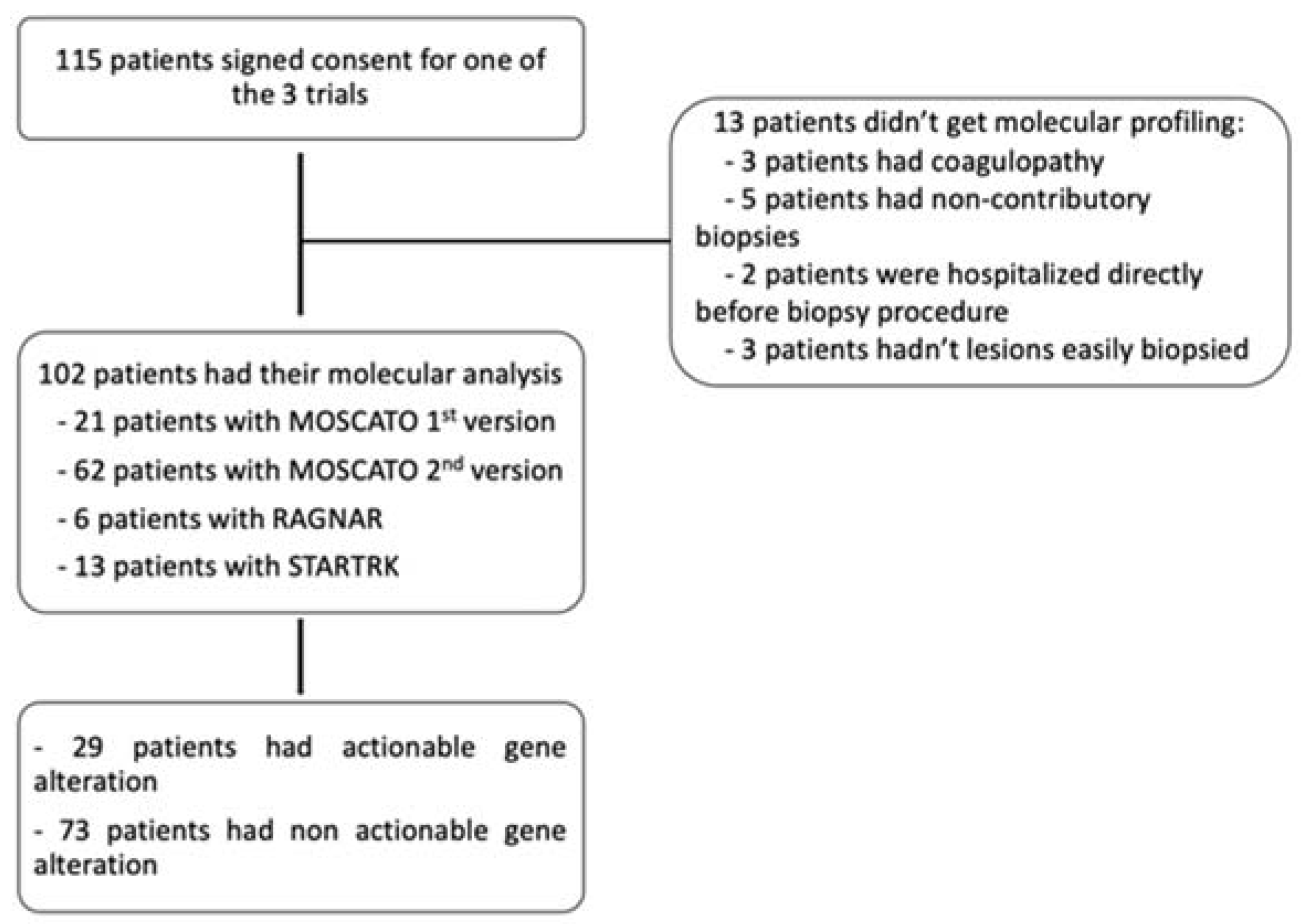
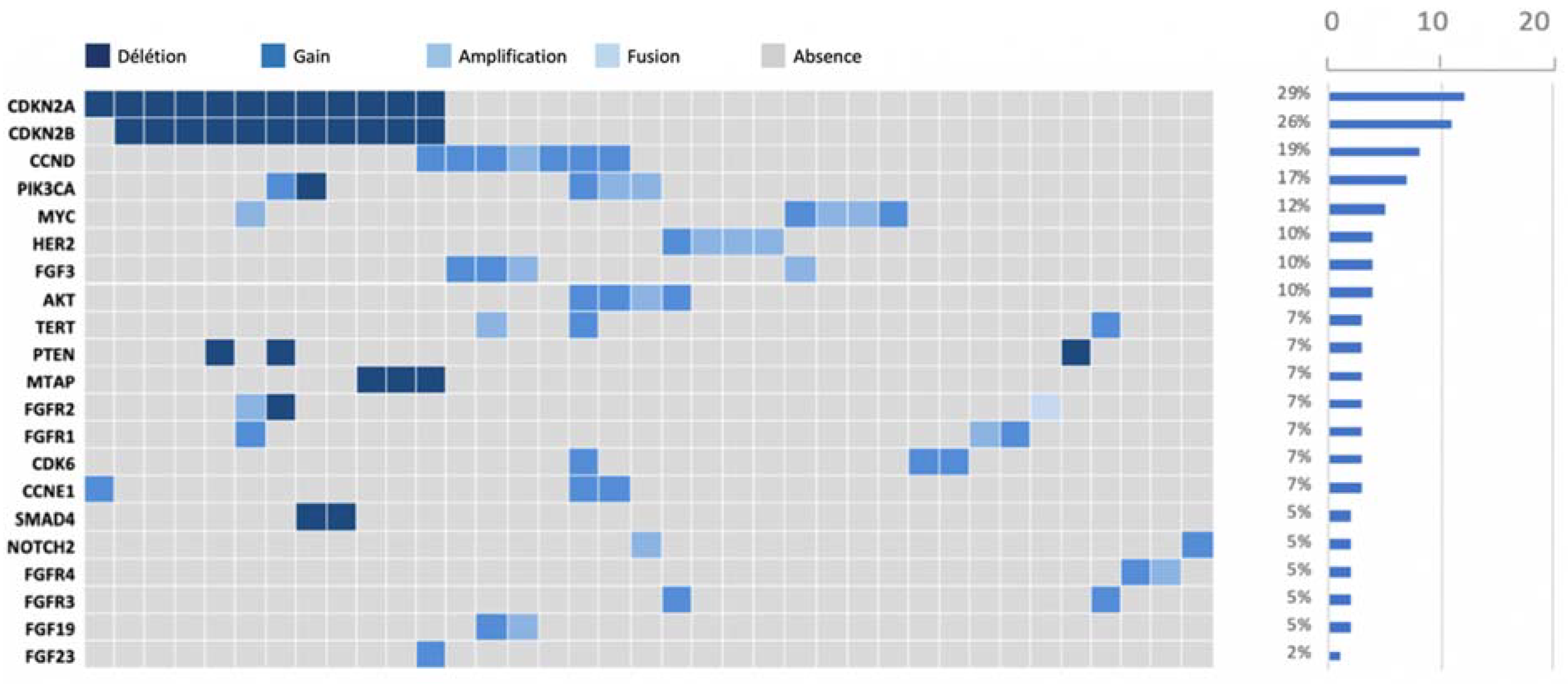
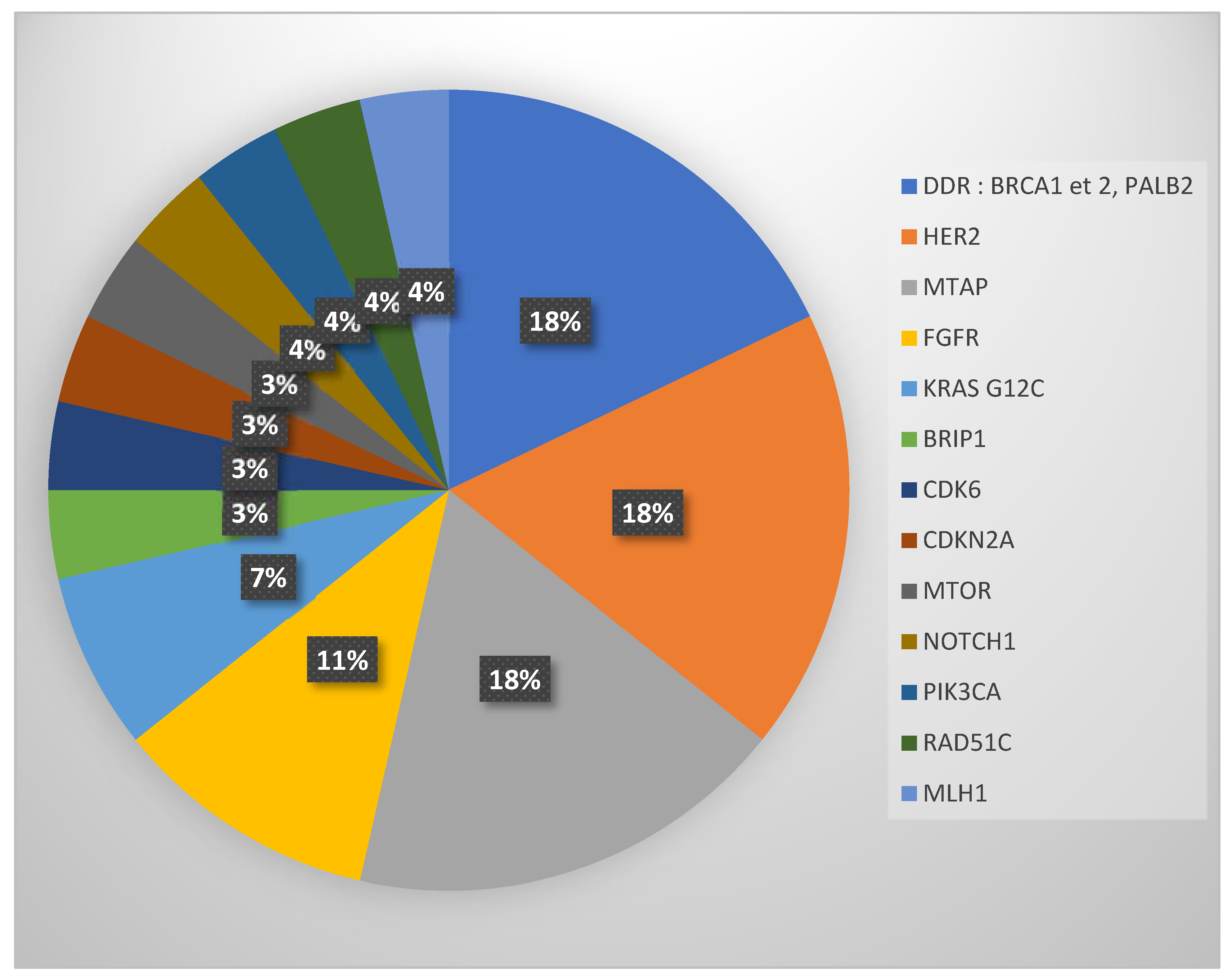
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rawla, P.; Sunkara, T.; Gaduputi, V. Epidemiology of Pancreatic Cancer: Global Trends, Etiology and Risk Factors. World J. Oncol. 2019, 10, 10–27. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Rahib, L.; Smith, B.D.; Aizenberg, R.; Rosenzweig, A.B.; Fleshman, J.M.; Matrisian, L.M. Projecting cancer incidence and deaths to 2030: The unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014, 74, 2913–2921. [Google Scholar] [CrossRef]
- Conroy, T.; Desseigne, F.; Ychou, M.; Bouché, O.; Guimbaud, R.; Bécouarn, Y.; Adenis, A.; Raoul, J.L.; Gourgou-Bourgade, S.; de la Fouchardière, C.; et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N. Engl. J. Med. 2011, 364, 1817–1825. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, D.; El-Maraghi, R.H.; Hammel, P.; Heinemann, V.; Kunzmann, V.; Sastre, J.; Scheithauer, W.; Siena, S.; Tabernero, J.; Teixeira, L.; et al. nab-Paclitaxel plus gemcitabine for metastatic pancreatic cancer: Long-term survival from a phase III trial. J. Natl. Cancer Inst. 2015, 107, dju413. [Google Scholar] [CrossRef]
- Von Hoff, D.D.; Ervin, T.; Arena, F.P.; Chiorean, E.G.; Infante, J.; Moore, M.; Seay, T.; Tjulandin, S.A.; Ma, W.W.; Saleh, M.N.; et al. Increased Survival in Pancreatic Cancer with nab-Paclitaxel plus Gemcitabine. N. Engl. J. Med. 2013, 369, 1691–1703. [Google Scholar] [CrossRef]
- Kieler, M.; Unseld, M.; Bianconi, D.; Scheithauer, W.; Prager, G.W. A real-world analysis of second-line treatment options in pancreatic cancer: Liposomal-irinotecan plus 5-fluorouracil and folinic acid. Ther. Adv. Med. Oncol. 2019, 11, 1758835919853196. [Google Scholar] [CrossRef]
- Collisson, E.A.; Bailey, P.; Chang, D.K.; Biankin, A.V. Molecular subtypes of pancreatic cancer. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 207–220. [Google Scholar] [CrossRef]
- Aguirre, A.J.; Nowak, J.A.; Camarda, N.D.; Moffitt, R.A.; Ghazani, A.A.; Hazar-Rethinam, M.; Raghavan, S.; Kim, J.; Brais, L.K.; Ragon, D.; et al. Real-time Genomic Characterization of Advanced Pancreatic Cancer to Enable Precision Medicine. Cancer Discov. 2018, 8, 1096–1111. [Google Scholar] [CrossRef]
- Pishvaian, M.J.; Blais, E.M.; Brody, J.R.; Lyons, E.; DeArbeloa, P.; Hendifar, A.; Mikhail, S.; Chung, V.; Sahai, V.; Sohal, D.P.; et al. Overall survival in patients with pancreatic cancer receiving matched therapies following molecular profiling: A retrospective analysis of the Know Your Tumor registry trial. Lancet Oncol. 2020, 21, 508–518. [Google Scholar] [CrossRef]
- Singhi, A.D.; George, B.; Greenbowe, J.R.; Chung, J.; Suh, J.; Maitra, A.; Klempner, S.J.; Hendifar, A.; Milind, J.M.; Golan, T.; et al. Real-Time Targeted Genome Profile Analysis of Pancreatic Ductal Adenocarcinomas Identifies Genetic Alterations That Might Be Targeted with Existing Drugs or Used as Biomarkers. Gastroenterology 2019, 156, 2242–2253.e4. [Google Scholar] [CrossRef] [PubMed]
- Lowery, M.A.; Jordan, E.J.; Basturk, O.; Ptashkin, R.N.; Zehir, A.; Berger, M.F.; Leach, T.; Herbst, B.; Askan, G.; Maynard, H.; et al. Real-Time Genomic Profiling of Pancreatic Ductal Adenocarcinoma: Potential Actionability and Correlation with Clinical Phenotype. Clin. Cancer Res. 2017, 23, 6094–6100. [Google Scholar] [CrossRef] [PubMed]
- Dreyer, S.B.; Chang, D.K.; Bailey, P.; Biankin, A.V. Pancreatic Cancer Genomes: Implications for Clinical Management and Therapeutic Development. Clin. Cancer Res. 2017, 23, 1638–1646. [Google Scholar] [CrossRef] [PubMed]
- Golan, T.; Hammel, P.; Reni, M.; Van Cutsem, E.; Macarulla, T.; Hall, M.J.; Park, J.O.; Hochhauser, D.; Arnold, D.; Oh, D.Y.; et al. Maintenance Olaparib for Germline BRCA-Mutated Metastatic Pancreatic Cancer. N. Engl. J. Med. 2019, 381, 317–327. [Google Scholar] [CrossRef]
- Massard, C.; Michiels, S.; Ferté, C.; Le Deley, M.C.; Lacroix, L.; Hollebecque, A.; Verlingue, L.; Ileana, E.; Rosellini, S.; Ammari, S.; et al. High-Throughput Genomics and Clinical Outcome in Hard-to-Treat Advanced Cancers: Results of the MOSCATO 01 Trial. Cancer Discov. 2017, 7, 586–595. [Google Scholar] [CrossRef]
- Le Tourneau, C.; Delord, J.P.; Gonçalves, A.; Gavoille, C.; Dubot, C.; Isambert, N.; Campone, M.; Trédan, O.; Massiani, M.A.; Mauborgne, C.; et al. Molecularly targeted therapy based on tumour molecular profiling versus conventional therapy for advanced cancer (SHIVA): A multicentre, open-label, proof-of-concept, randomised, controlled phase 2 trial. Lancet Oncol. 2015, 16, 1324–1334. [Google Scholar] [CrossRef]
- Trédan, O.; Wang, Q.; Pissaloux, D.; Cassier, P.; de la Fouchardière, A.; Fayette, J.; Desseigne, F.; Ray-Coquard, I.; de la Fouchardiere, C.; Frappaz, D.; et al. Molecular screening program to select molecular-based recommended therapies for metastatic cancer patients: Analysis from the ProfiLER trial. Ann. Oncol. 2019, 30, 757–765. [Google Scholar] [CrossRef]
- Andre, F.; Filleron, T.; Kamal, M.; Mosele, F.; Arnedos, M.; Dalenc, F.; Sablin, M.-P.; Campone, M.; Bonnefoi, H.; Lefeuvre-Plesse, C.; et al. Genomics to select treatment for patients with metastatic breast cancer. Nature 2022, 610, 343–348. [Google Scholar] [CrossRef]
- Zehir, A.; Benayed, R.; Shah, R.H.; Syed, A.; Middha, S.; Kim, H.R.; Srinivasan, P.; Gao, J.; Chakravarty, D.; Devlin, S.M.; et al. Mutational landscape of metastatic cancer revealed from prospective clinical sequencing of 10,000 patients. Nat. Med. 2017, 23, 703–713. [Google Scholar] [CrossRef]
- Tuxen, I.V.; Rohrberg, K.S.; Oestrup, O.; Ahlborn, L.B.; Schmidt, A.Y.; Spanggaard, I.; Hasselby, J.P.; Santoni-Rugiu, E.; Yde, C.W.; Mau-Sørensen, M.; et al. Copenhagen Prospective Personalized Oncology (CoPPO)-Clinical Utility of Using Molecular Profiling to Select Patients to Phase I Trials. Clin. Cancer Res. 2019, 25, 1239–1247. [Google Scholar] [CrossRef]
- Martin-Romano, P.; Mezquita, L.; Hollebecque, A.; Lacroix, L.; Rouleau, E.; Gazzah, A.; Bahleda, R.; Planchard, D.; Varga, A.; Baldini, C.; et al. Implementing the European Society for Medical Oncology Scale for Clinical Actionability of Molecular Targets in a Comprehensive Profiling Program: Impact on Precision Medicine Oncology. JCO Precis. Oncol. 2022, 6, e2100484. [Google Scholar] [CrossRef] [PubMed]
- Tsimberidou, A.-M.; Hong, D.S.; Ye, Y.; Cartwright, C.; Wheler, J.J.; Falchook, G.S.; Naing, A.; Fu, S.; Piha-Paul, S.; Janku, F.; et al. Initiative for Molecular Profiling and Advanced Cancer Therapy (IMPACT): An MD Anderson Precision Medicine Study. JCO Precis. Oncol. 2017, 2017, 1–18. [Google Scholar]
- Schwaederle, M.; Zhao, M.; Lee, J.J.; Eggermont, A.M.; Schilsky, R.L.; Mendelsohn, J.; Lazar, V.; Kurzrock, R. Impact of Precision Medicine in Diverse Cancers: A Meta-Analysis of Phase II Clinical Trials. J. Clin. Oncol. 2015, 33, 3817–3825. [Google Scholar] [CrossRef] [PubMed]
- Mateo, J.; Chakravarty, D.; Dienstmann, R.; Jezdic, S.; Gonzalez-Perez, A.; Lopez-Bigas, N.; Ng, C.; Bedard, P.; Tortora, G.; Douillard, J.-Y.; et al. A framework to rank genomic alterations as targets for cancer precision medicine: The ESMO Scale for Clinical Actionability of molecular Targets (ESCAT). Ann. Oncol. 2018, 29, 1895–1902. [Google Scholar] [CrossRef]
- Cobain, E.F.; Wu, Y.-M.; Vats, P.; Chugh, R.; Worden, F.; Smith, D.C.; Schuetze, S.M.; Zalupski, M.M.; Sahai, V.; Alva, A.; et al. Assessment of Clinical Benefit of Integrative Genomic Profiling in Advanced Solid Tumors. JAMA Oncol. 2021, 7, 525–533. [Google Scholar] [CrossRef]
- Hong, D.S.; Fakih, M.G.; Strickler, J.H.; Desai, J.; Durm, G.A.; Shapiro, G.I.; Falchook, G.S.; Price, T.J.; Sacher, A.; Denlinger, C.S.; et al. KRASG12C Inhibition with Sotorasib in Advanced Solid Tumors. N. Engl. J. Med. 2020, 383, 1207–1217. [Google Scholar] [CrossRef]
- Ou, S.H.I.; Jänne, P.A.; Leal, T.A.; Rybkin, I.I.; Sabari, J.K.; Barve, M.A.; Bazhenova, L.; Johnson, M.L.; Velastegui, K.L.; Cilliers, C.; et al. First-in-Human Phase I/IB Dose-Finding Study of Adagrasib (MRTX849) in Patients with Advanced KRASG12C Solid Tumors (KRYSTAL-1). J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2022, 40, 2530. [Google Scholar] [CrossRef]
- Waters, A.M.; Der, C.J. KRAS: The Critical Driver and Therapeutic Target for Pancreatic Cancer. Cold Spring Harb Perspect. Med. 2018, 8, a031435. [Google Scholar] [CrossRef]
- Shah, S.; Rana, T.; Kancharla, P.; Monga, D. Targeted Therapy for BRAF V600E Positive Pancreatic Adenocarcinoma: Two Case Reports. Cancer Genom. Proteom. 2023, 20, 398–403. [Google Scholar] [CrossRef]
- Wang, Z.; He, D.; Chen, C.; Liu, X.; Ke, N. Vemurafenib Combined with Trametinib Significantly Benefits the Survival of a Patient with Stage IV Pancreatic Ductal Adenocarcinoma with BRAF V600E Mutation: A Case Report. Front. Oncol. 2022, 11, 801320. [Google Scholar] [CrossRef]
- Bayle, A.; Peyraud, F.; Belcaid, L.; Brunet, M.; Aldea, M.; Clodion, R.; Dubos, P.; Vasseur, D.; Nicotra, C.; Geraud, A.; et al. Liquid versus tissue biopsy for detecting actionable alterations according to ESCAT in patients with advanced cancer: A study from the French National Center for Precision Medicine (PRISM). Ann. Oncol. 2022, 33, 1328–1331. [Google Scholar] [CrossRef] [PubMed]

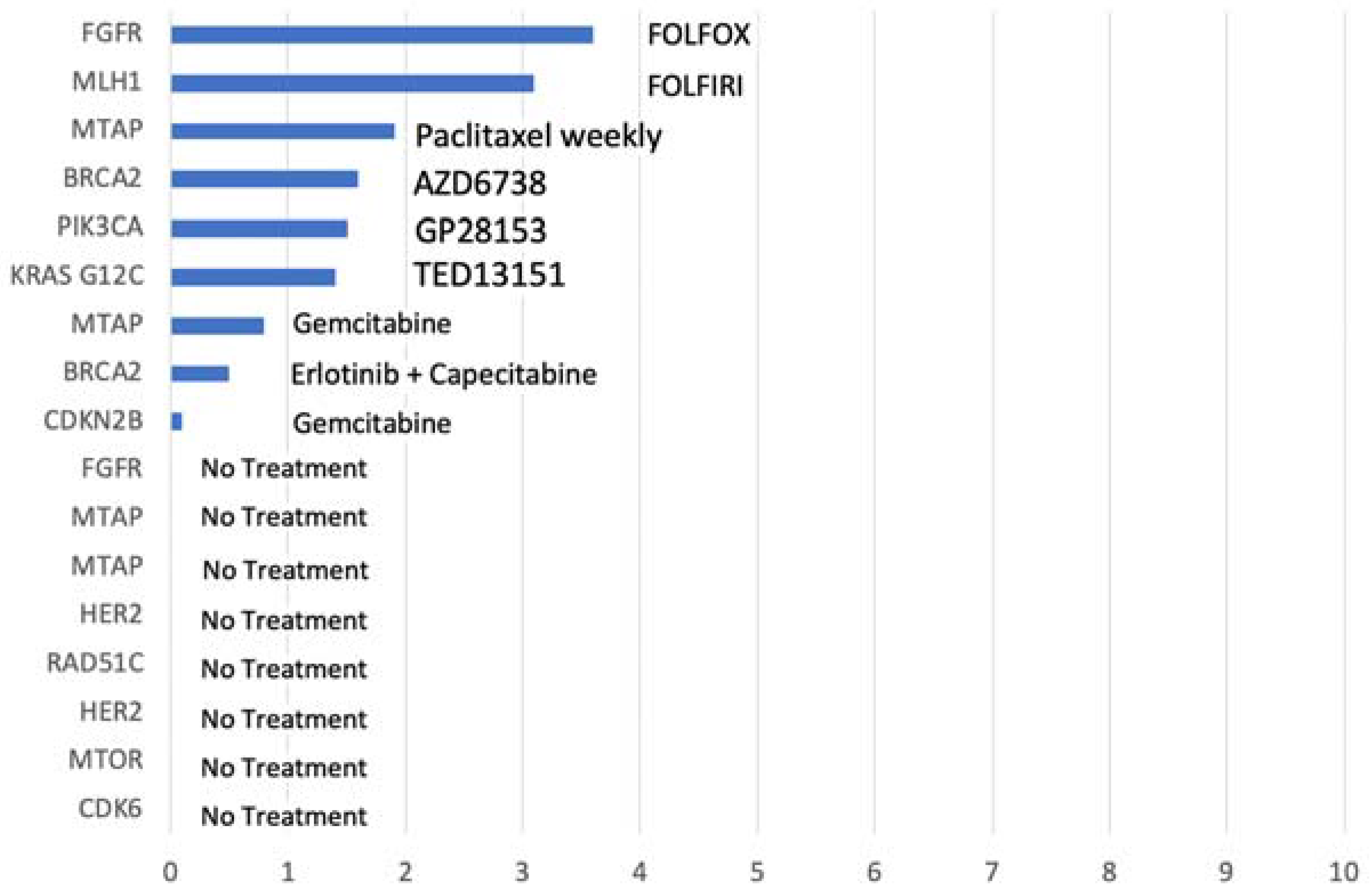
 ongoing treatment; † dead). Better PFS is seen in patients with BRCA2 mutations that were treated with olaparib.
ongoing treatment; † dead). Better PFS is seen in patients with BRCA2 mutations that were treated with olaparib.
ongoing treatment; † dead). Better PFS is seen in patients with BRCA2 mutations that were treated with olaparib.
ongoing treatment; † dead). Better PFS is seen in patients with BRCA2 mutations that were treated with olaparib.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | Group A | Group B | Group C | p | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Sex | n (%) | 102 | 12 | 17 | 73 | |||||
| Male | 57 | (55.9) | 6 | (50.0) | 13 | (76.5) | 38 | (52.1) | 0.1716 | |
| Female | 45 | (44.1) | 6 | (50.0) | 4 | (23.5) | 35 | (47.9) | ||
| Age at diagnosis | n | 102 | 12 | 17 | 73 | |||||
| Mean | 57.8 | 58.3 | 58.3 | 57.9 | ||||||
| Median | 59 | 60 | 60 | 59 | ||||||
| Min; Max | 30; 75 | 30; 68 | 40; 75 | 30; 75 | ||||||
| Age at molecular profiling | n | 102 | 12 | 17 | 73 | |||||
| Mean (sd) | 59.8 | (10.7) | 58.1 | (11.5) | 63.0 | (11.3) | 59.4 | (10.5) | 0.3322 | |
| Median | 61 (52; 68) | 63 (52; 67) | 64 (54; 72) | 60 (51; 68) | ||||||
| (Q1; Q3) | ||||||||||
| Min; Max | 31; 78 | 31; 69 | 41; 77 | 32; 78 | ||||||
| Stage at molecular profiling | n (%) | 102 | 12 | 17 | 73 | |||||
| Stage I–III | 2 | (2.0) | 2 | (2.7) | 0.6668 | |||||
| Stage IV | 100 | (98.0) | 12 | (100.0) | 17 | (100.0) | 71 | (97.3) | ||
| Nb of prior treatments | n (%) | 102 | 12 | 17 | 73 | |||||
| ≤ 1 line | 27 | (26.5) | 4 | (33.3) | 5 | (29.4) | 18 | (24.7) | 0.7260 | |
| >1 line | 75 | (73.5) | 8 | (66.7) | 12 | (70.6) | 55 | (75.3) | ||
| Nb of metastatic sites | n (%) | 100 | 12 | 17 | 71 | |||||
| 1 site | 78 | (78.0) | 9 | (75.0) | 12 | (70.6) | 57 | (80.3) | 0.8340 | |
| > 1 site | 22 | (22.0) | 3 | (25.0) | 5 | (29.4) | 14 | (19.7) | ||
| Liver metastasis | n (%) | 100 | 12 | 17 | 71 | |||||
| No | 24 | (24.0) | 3 | (25.0) | 3 | (17.6) | 18 | (25.4) | 0.9314 | |
| Yes | 76 | (76.0) | 9 | (75.0) | 14 | (82.4) | 53 | (74.6) | ||
| Lung metastasis | n (%) | 100 | 12 | 17 | 71 | |||||
| No | 85 | (85.0) | 9 | (75.0) | 15 | (88.2) | 61 | (85.9) | ||
| Yes | 15 | (15.0) | 3 | (25.0) | 2 | (11.8) | 10 | (14.1) | ||
| Peritoneal carcinosis | n (%) | 100 | 12 | 17 | 71 | |||||
| No | 88 | (88.0) | 10 | (83.3) | 15 | (88.2) | 63 | (88.7) | ||
| Yes | 12 | (12.0) | 2 | (16.7) | 2 | (11.8) | 8 | (11.3) | ||
| Reasons for Not Receiving Molecular Target Therapies (MTTs) | Number (%) |
|---|---|
| Poor performance status at progression | 9 (53.0) |
| Patients having some of the exclusion criteria of the trial offering the MTT | 4 (23.6) |
| Patients refusing consent | 2 (11.7) |
| Other causes | 2 (11.7) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tarabay, A.; Boileve, A.; Smolenschi, C.; Antoun, L.; Valery, M.; Fuerea, A.; Perret, A.; Burtin, P.; Cosconea, S.; Belkhodja, H.; et al. Precision Medicine in Pancreatic Ductal Adenocarcinoma: The Impact of Targeted Therapies on Survival of Patients Harboring Actionable Mutations. Biomedicines 2023, 11, 2569. https://doi.org/10.3390/biomedicines11092569
Tarabay A, Boileve A, Smolenschi C, Antoun L, Valery M, Fuerea A, Perret A, Burtin P, Cosconea S, Belkhodja H, et al. Precision Medicine in Pancreatic Ductal Adenocarcinoma: The Impact of Targeted Therapies on Survival of Patients Harboring Actionable Mutations. Biomedicines. 2023; 11(9):2569. https://doi.org/10.3390/biomedicines11092569
Chicago/Turabian StyleTarabay, Anthony, Alice Boileve, Cristina Smolenschi, Leony Antoun, Marine Valery, Alina Fuerea, Audrey Perret, Pascal Burtin, Simona Cosconea, Hichem Belkhodja, and et al. 2023. "Precision Medicine in Pancreatic Ductal Adenocarcinoma: The Impact of Targeted Therapies on Survival of Patients Harboring Actionable Mutations" Biomedicines 11, no. 9: 2569. https://doi.org/10.3390/biomedicines11092569
APA StyleTarabay, A., Boileve, A., Smolenschi, C., Antoun, L., Valery, M., Fuerea, A., Perret, A., Burtin, P., Cosconea, S., Belkhodja, H., Malka, D., Boige, V., Hollebecque, A., & Ducreux, M. (2023). Precision Medicine in Pancreatic Ductal Adenocarcinoma: The Impact of Targeted Therapies on Survival of Patients Harboring Actionable Mutations. Biomedicines, 11(9), 2569. https://doi.org/10.3390/biomedicines11092569