
Prevalence of Unfavorable Video-Urodynamic Findings and Clinical Implications in Patients with Minimally Conscious State/Unresponsive Wakefulness Syndrome: A Retrospective Descriptive Analysis

 , , , , , , and
, , , , , , and
Abstract
1. Introduction
2. Materials and Methods
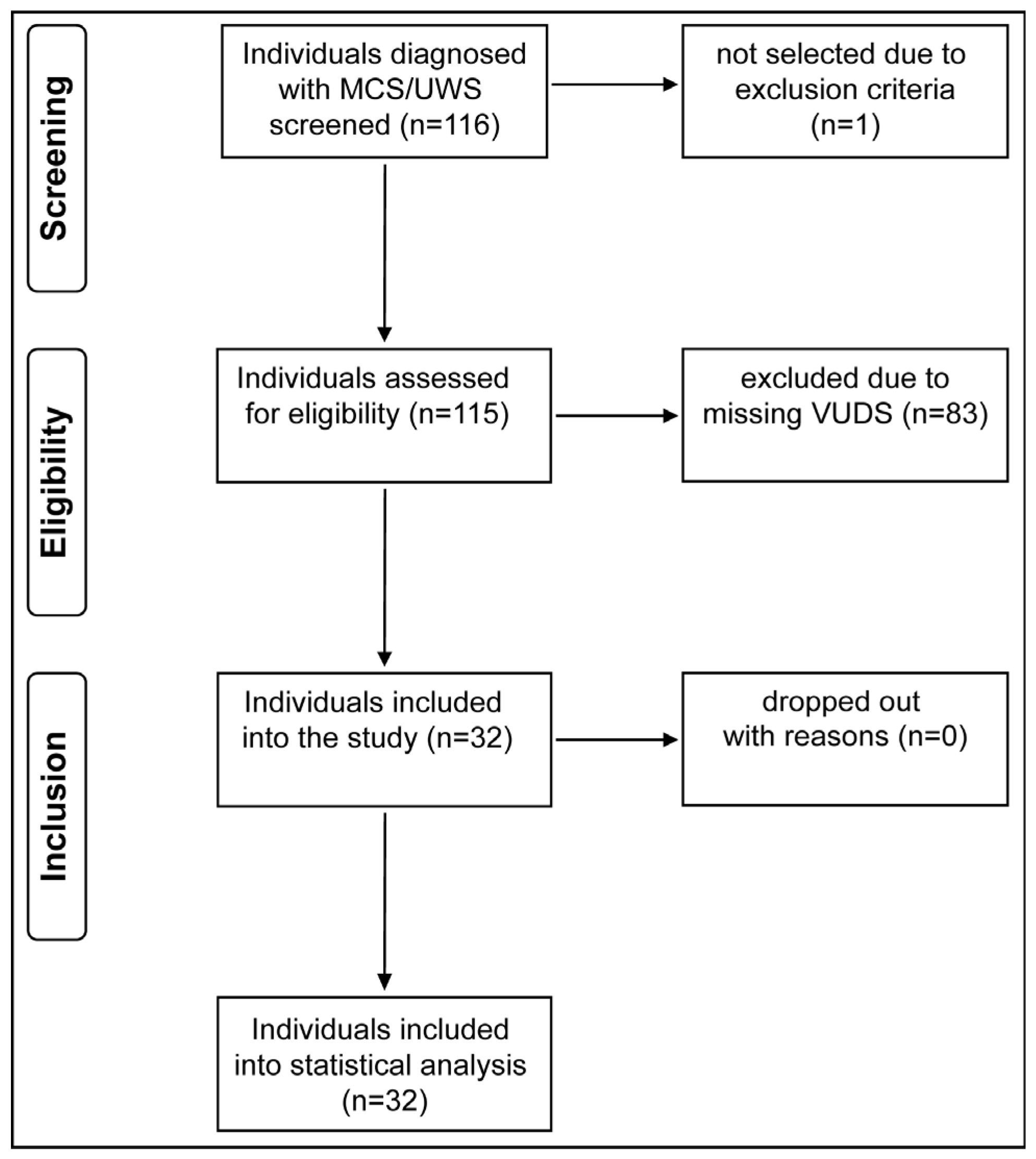
2.1. Population
2.2. Objectives
2.3. Outcome Variables
2.4. Data Source and Collection
2.5. Bias
2.6. Statistical Methods
3. Results
4. Discussion
4.1. Main Findings
4.2. Findings of Unfavorable Urodynamic Parameters
4.3. LUT Management before and after VUDS
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jennett, B.; Plum, F. Persistent vegetative state after brain damage: A syndrome in search of a name. Lancet 1972, 299, 734–737. [Google Scholar] [CrossRef]
- Laureys, S.; Celesia, G.G.; Cohadon, F.; Lavrijsen, J.; León-Carrión, J.; Sannita, W.G.; Sazbon, L.; Schmutzhard, E.; Von Wild, K.R.; Zeman, A.; et al. Unresponsive wakefulness syndrome: A new name for the vegetative state or apallic syndrome. BMC Med. 2010, 8, 68. [Google Scholar] [CrossRef]
- Giacino, J.T.; Katz, D.I.; Schiff, N.D.; Whyte, J.; Ashman, E.J.; Ashwal, S.; Barbano, R.; Hammond, F.M.; Laureys, S.; Ling, G.S.F.; et al. Practice guideline update recommendations summary: Disorders of consciousness. Neurology 2018, 91, 450–460. [Google Scholar] [CrossRef]
- College of Physicians, R. Prolonged Disorders of Consciousness Following Sudden Onset Brain Injury: National Clinical Guidelines. 2009. Available online: https://www.rcplondon.ac.uk/guidelines-policy/prolonged-disorders-consciousness-following-sudden-onset-brain-injury-national-clinical-guidelines (accessed on 27 July 2023).
- Magnani, F.G.; Leonardi, M.; Sattin, D. Caregivers of people with disorders of consciousness: Which burden predictors? Neurol. Sci. 2020, 41, 2773–2779. [Google Scholar] [CrossRef] [PubMed]
- Naro, A.; Calabrò, R.S. Towards New Diagnostic Approaches in Disorders of Consciousness: A Proof of Concept Study on the Promising Use of Imagery Visuomotor Task. Brain Sci. 2020, 10, 746. [Google Scholar] [CrossRef] [PubMed]
- Berrol, S. Evolution and the persistent vegetative state. J. Head Trauma Rehabil. 1986, 1, 7–13. [Google Scholar] [CrossRef]
- Levin, H.S.; Saydjari, C.; Eisenberg, H.M.; Foulkes, M.; Marshall, L.F.; Ruff, R.M.; Jane, J.A.; Marmarou, A. Vegetative State after Closed-Head Injury. A Traumatic Coma Data Bank Report. Arch. Neurol. 1991, 48, 580–585. [Google Scholar] [CrossRef]
- Wales, L.R.; Bernhardt, J.A. A case for slow to recover rehabilitation services following severe acquired brain injury. Aust. J. Physiother. 2000, 46, 143–146. [Google Scholar] [CrossRef]
- Cope, D.N.; Hall, K. Head injury rehabilitation: Benefit of early intervention. Arch. Phys. Med. Rehabil. 1982, 63, 433–437. [Google Scholar]
- Mackay, L.E.; Bernstein, B.A.; Chapman, P.E.; Morgan, A.S.; Milazzo, L.S. Early intervention in severe head injury: Long-term benefits of a formalized program. Arch. Phys. Med. Rehabil. 1992, 73, 635–641. [Google Scholar]
- Krimchansky, B.-Z.; Sazbon, L.; Heller, L.; Kosteff, H.; ZLuttwak, Z. Bladder tone in patients in post-traumatic vegetative state. Brain Inj. 1999, 13, 899–903. [Google Scholar] [CrossRef] [PubMed]
- Giraudo, D.; Gozzerino, F.; Lamberti, G.; Antoniono, E.; Califano, C.; Filocamo, M.; Massazza, G. Urodynamic evaluation before and after continuous intrathecal Baclofen infusion (ITB) in patients unresponsive wakefulness syndrome and minimally conscious state. Pelviperineology 2017, 36, 60–62. [Google Scholar]
- Benecchi, L.; Caldera, G.; Cavestro, C.; Bordinazzo, R.; Privitera, O.; Feller, S. Post-comatose cystomanometric peculiarities. Urol. J. 1996, 63 (Suppl. S1), 99–104. [Google Scholar] [CrossRef]
- Nardulli, R.; Monitillo, V.; Losavio, E.; Megna, M.; Megna, G. Urodynamic evaluation in the apallic syndrome. Urodinamica 1992, 2, 180–182. [Google Scholar]
- Wyndaele, J.J. Urodynamics in comatose patients. Neurourol. Urodyn. 1990, 9, 43–52. [Google Scholar] [CrossRef]
- Satar, N.; Bauer, S.B.; Shefner, J.; Kelly, M.D.; Darbey, M.M. The Effects of Delayed Diagnosis and Treatment in Patients with an Occult Spinal Dysraphism. J. Urol. 1995, 154 2 Pt 2, 754–758. [Google Scholar] [CrossRef]
- Çetinel, B.; Önal, B.; Can, G.; Talat, Z.; Erhan, B.; Gündüz, B. Risk factors predicting upper urinary tract deterioration in patients with spinal cord injury: A retrospective study. Neurourol. Urodyn. 2017, 36, 653–658. [Google Scholar] [CrossRef]
- Blok, B.; Castro-Diaz, D.; Del Popolo, G.; Groen, J.; Hamid, R.; Karsenty, G.; Kessler, T.M.; Pannek, J. EAU Guidelines on Neuro-Urology. 2023. Available online: https://uroweb.org/guidelines/neuro-urology (accessed on 27 July 2023).
- Welk, B.; Schneider, M.P.; Thavaseelan, J.; Traini, L.R.; Curt, A.; Kessler, T.M. Early urological care of patients with spinal cord injury. World J. Urol. 2018, 36, 1537–1544. [Google Scholar] [CrossRef] [PubMed]
- Giacino, J.T.; Kalmar, K.; Whyte, J. The JFK Coma Recovery Scale-Revised: Measurement characteristics and diagnostic utility. Arch. Phys. Med. Rehabil. 2004, 85, 2020–2029. [Google Scholar] [CrossRef]
- Teasdale, G.; Jennett, B. Assessment of coma and impaired consciousness: A practical scale. Lancet 1974, 2, 81–84. [Google Scholar] [CrossRef]
- Huber, M.; Koch, S.; Hund-Georgiadis, M.; Mäder, M.; Borgwardt, S.; Stieglitz, R.-D. Diagnostic Validity of the Basler Vegetative State Assessment-BAVESTA/Diagnostische Validität des Basler Vegetative State Assessments-BAVESTA. Int. J. Health Prof. 2014, 1, 50–60. [Google Scholar] [CrossRef]
- Schäfer, W.; Abrams, P.; Liao, L.; Mattiasson, A.; Pesce, F.; Spangberg, A.; Sterling, A.M.; Zinner, N.R.; van Kerrebroeck, P. Good urodynamic practices: Uroflowmetry, filling cystometry, and pressure-flow studies. Neurourol. Urodyn. 2002, 21, 261–274. [Google Scholar] [CrossRef] [PubMed]
- Huber, M.; Koch, S.; Mäder, M.; Hund-Georgiadis, M.; Borgwardt, S.; Stieglitz, R.D. Verlaufsbeobachtung von Wachkomapatienten-Validierung des Basler Vegetative State Assessments (BAVESTA). Neurol. Rehabil. 2014, 20, 123–132. [Google Scholar]
- Hooton, T.M.; Bradley, S.F.; Cardenas, D.D.; Colgan, R.; Geerlings, S.E.; Rice, J.C.; Saint, S.; Schaeffer, A.J.; Tambayh, P.A.; Tenke, P.; et al. Diagnosis, Prevention, and Treatment of Catheter-Associated Urinary Tract Infection in Adults: 2009 International Clinical Practice Guidelines from the Infectious Diseases Society of America. Clin. Infect. Dis. 2010, 50, 625–663. [Google Scholar] [CrossRef] [PubMed]
- Kozomara, M.; Birkhäuser, V.; Anderson, C.E.; Bywater, M.; Gross, O.; Kiss, S.; Knüpfer, S.C.; Koschorke, M.; Leitner, L.; Mehnert, U.; et al. Neurogenic Lower Urinary Tract Dysfunction in the First Year After Spinal Cord Injury: A Descriptive Study of Urodynamic Findings. J. Urol. 2023, 209, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Weld, K.J.; Dmochowski, R.R. Association of level of injury and bladder behavior in patients with post-traumatic spinal cord injury. Urology 2000, 55, 490–494. [Google Scholar] [CrossRef] [PubMed]
- Al Dandan, H.B.; Coote, S.; McClurg, D. Prevalence of Lower Urinary Tract Symptoms in People with Multiple Sclerosis: A systematic review and meta-analysis. Int. J. MS Care 2020, 22, 91–99. [Google Scholar] [CrossRef]
- Yu, W.-R.; Kuo, H.-C. Usefulness of videourodynamic study in the decision-making of surgical intervention and bladder management for neurogenic lower urinary tract dysfunction among patients with myelomeningocele. Int. Urol. Nephrol. 2022, 54, 1815–1824. [Google Scholar] [CrossRef]
- Blaivas, J.G.; Sinha, H.P.; Zayed, A.A.H.; Labib, K.B. Detrusor-external Sphincter Dyssynergia: A Detailed Electromyographic Study. J. Urol. 1981, 125, 545–548. [Google Scholar] [CrossRef]
- Abrams, P.; Cardozo, L.; Fall, M.; Griffiths, D.; Rosier, P.; Ulmsten, U.; Van Kerrebroeck, P.; Victor, A.; Wein, A.; Standardisation Sub-committee of the International Continence Society. The standardisation of terminology of lower urinary tract function: Report from the standardisation sub-committee of the International Continence Society. Neurourol. Urodyn. 2002, 21, 167–178. [Google Scholar]
- Gormley, E.A. Urologic Complications of the Neurogenic Bladder. Urol. Clin. N. Am. 2010, 37, 601–607. [Google Scholar] [CrossRef]
- Bywater, M.; Tornic, J.; Mehnert, U.; Kessler, T.M. Detrusor Acontractility after Acute Spinal Cord Injury—Myth or Reality? J. Urol. 2018, 199, 1565–1570. [Google Scholar] [CrossRef] [PubMed]
- Sirasaporn, P.; Saengsuwan, J. Incidence and predictive factors for developing vesicouretericreflux in individuals with suprasarcral spinal cord injury: A historical cohort study. Spinal Cord 2021, 59, 753–760. [Google Scholar]
- Piquet, V.; Turmel, N.; Chesnel, C.; Haddad, R.; Lebreton, F.; Amarenco, G.; Hentzen, C. Upper urinary tract function of patients with multiple sclerosis. Neurourol. Urodyn. 2022, 41, 498–505. [Google Scholar] [CrossRef] [PubMed]
- Hackler, R.H.; Hall, M.K.; Zampieri, T.A. Bladder Hypocompliance in the Spinal Cord Injury Population. J. Urol. 1989, 141, 1390–1393. [Google Scholar] [CrossRef]
- Igawa, Y.; Wyndaele, J.-J.; Nishizawa, O. Catheterization: Possible complications and their prevention and treatment. Int. J. Urol. 2008, 15, 481–485. [Google Scholar] [CrossRef] [PubMed]
- Jamison, J.; Maguire, S.; McCann, J. Catheter policies for management of long term voiding problems in adults with neurogenic bladder disorders. Cochrane Database Syst. Rev. 2013, 11, CD004375. [Google Scholar] [CrossRef]
- Jiang, H.-H.; Kokiko-Cochran, O.N.; Li, K.; Balog, B.; Lin, C.-Y.; Damaser, M.S.; Lin, V.; Cheng, J.Y.; Lee, Y.-S. Bladder dysfunction changes from underactive to overactive after experimental traumatic brain injury. Exp. Neurol. 2013, 240, 57–63. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kavanagh, A.; Akhavizadegan, H.; Walter, M.; Stothers, L.; Welk, B.; Boone, T.B. Surveillance urodynamics for neurogenic lower urinary tract dysfunction: A systematic review. Can. Urol. Assoc. J. 2019, 13, 133–141. [Google Scholar] [CrossRef]


{kind=link}
| Demographics | All Patients (n = 32) | Early VUDS (n = 26) | Late VUDS (n = 6) | p Value $ |
|---|---|---|---|---|
| Age [years] | 37 [28; 52], 20–74 | 37 [28; 51], 20–69 | 36 [28; 58], 23–74 | 1.0 |
| Time from diagnosis to VUDS [months] | 4 [2; 6], 1–93 | 2.5 [2; 4], 1–7 | 32 [28; 74], 25–93 | 0.03 |
| Sex (female/male) | 7 (21.9%)/25 (78.1%) | 7 (26.9%)/19 (73.1%) | 0/6 | 0.3 |
| Injury characteristics | ||||
| Type of brain injury | 0.8 | |||
| Traumatic | 18 (56.3%) | 15 (57.7%) | 3 (50%) | |
| Hypoxic | 13 (40.6%) | 10 (38.5%) | 3 (50%) | |
| Hemorrhagic | 1 (3.1%) | 1 (3.8%) | 0 | |
| Coma Recovery Scale-revised (n = 19) * | 16 [7.5; 21.5], 3–24 | 9 [6; 22.2], 3–24 | 15 [10; 16], 8–17 | 0.1 |
| Glasgow Coma Scale (n = 26) * | 9.5 [6.2; 10.8], 3–15 | 8 [6; 10.8], 3–15 | 10 [9.2; 10], 8–11 | 0.3 |
| Bavesta Score (n = 19) * | 2.8 [1.5; 3.6], 0.8–5.0 | 3 [1.5; 3.7], 0.8–5.0 | 2.2 [1.6; 3.1], 1.2–3.6 | 0.2 |
| Pharmaceutical LUT Treatment | All Patients (n = 32) | Early VUDS (n = 26) | Late VUDS (n = 6) | |||
|---|---|---|---|---|---|---|
| Before | After | Before | After | Before | After | |
| No. of patients on LUT treatment | 7 (21.9%) | 24 (75%) * | 7 (26.9%) | 19 (73.1%) ** | 0 | 5 (83.3%) *** |
| Antimuscarinics | 4 | 10 | 4 | 8 | 0 | 2 |
| Alpha-blockers | 3 | 11 | 3 | 8 | 0 | 3 |
| Mirabegron | 0 | 1 | 0 | 1 | 0 | 0 |
| Intradetrusor botulinum toxin-A | 0 | 2 | 0 | 2 | 0 | 0 |
| Intrasphincteric botulinum toxin-A | 0 | 6 | 0 | 3 | 0 | 3 |
| Bladder-emptying methods | ||||||
| Indwelling catheters | 25 (78.1%) | 12 (37.5%) | 21 (80.8%) | 10 (38.5%) | 4 (66.7%) | 2 (33.3%) |
| Transurethral | 7 | 2 | 7 | 2 | 0 | 0 |
| Suprapubic | 18 | 10 | 14 | 8 | 4 | 2 |
| Intermittent catheterization | 0 | 0 | 0 | 0 | 0 | 0 |
| NDO incontinence | 6 (18.8%) | 19 (59.4%) | 4 (15.4%) | 15 (57.7%) | 2 (33.3%) | 4 (66.7%) |
| with condom catheter | 5 | 18 | 0 | 14 | 2 | 4 |
| without condom catheter | 1 | 1 | 0 | 1 | 0 | 0 |
| Volitional voiding | 1 (3.1%) | 1 (3.1%) | 1 (3.8%) | 1 (3.8%) | 0 | 0 |
| Video-Urodynamic Parameters | All Patients (n = 32) | Early VUDS (n = 26) | Late VUDS (n = 6) | p Value $ |
|---|---|---|---|---|
| NDO * [yes/no] | 25 (78.1%)/7 (21.9%) | 19 (78.1%)/7 (26.9%) | 6/0 | 0.3 |
| Pdetmax storage [cmH2O] | 52 [21; 76], 5–272 | 49 [15; 62], 5–190 | 91 [81; 186], 51–272 | 0.3 |
| Pdetmax storage > 40 cmH2O * [yes or no] | 21 (65.6%)/11 (34.4%) | 15 (57.7%)/11 (42.3%) | 6/0 | 0.07 |
| DOLPP [cmH2O] | 42 [33; 52], 12–95 | 39 [30; 51], 12–95 | 43 [42; 61], 38–90 | 0.6 |
| DOLV [mL] | 98 [22; 241], 0–450 | 78 [0; 219], 0–450 | 185 [88; 290], 65–320 | 0.6 |
| Compliance [mL/H2O] | 29 [21; 44], 4–116 | 36 [24; 45], 5–116 | 18 [12; 28], 4–55 | 0.8 |
| Low-compliance bladder * [yes or no] | 8 (25.0%)/24 (75.0%) | 5 (19.2%)/21 (80.8%) | 3 (50.0%)/3 (50.0%) | |
| MCC [mL] | 238 [140; 351], 60–600 | 238 [150; 359], 60–600 | 215 [95; 331], 65–350 | 0.8 |
| PVR urine [yes/no] | 20 (62.5%)/12 (37.5%) | 16 (61.5%)/10 (38.5%) | 4 (66.7%)/2 (33.3%) | |
| PVR urine [mL] | 35 [0; 116], 0–530 | 45 [0; 120], 0–530 | 30 [8; 30], 0–45 | 0.09 |
| DSD * [yes/no] | 22 (68.8%)/10 (31.2%) | 17 (65.4%)/9 (34.6%) | 5 (83.3%)/1 (16.7%) | 0.6 |
| VUR * [yes/no] | 1 (3.1%)/31 (96.9%) | 0/26 | 1 (16.7%)/5 (83.3%) | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leboutte, F.; Engesser, C.; Zahiti, L.; Rentsch, C.A.; Seifert, H.; Anding, R.; Hund-Georgiadis, M.; Möhr, S.; Walter, M. Prevalence of Unfavorable Video-Urodynamic Findings and Clinical Implications in Patients with Minimally Conscious State/Unresponsive Wakefulness Syndrome: A Retrospective Descriptive Analysis. Biomedicines 2023, 11, 2432. https://doi.org/10.3390/biomedicines11092432
Leboutte F, Engesser C, Zahiti L, Rentsch CA, Seifert H, Anding R, Hund-Georgiadis M, Möhr S, Walter M. Prevalence of Unfavorable Video-Urodynamic Findings and Clinical Implications in Patients with Minimally Conscious State/Unresponsive Wakefulness Syndrome: A Retrospective Descriptive Analysis. Biomedicines. 2023; 11(9):2432. https://doi.org/10.3390/biomedicines11092432
Chicago/Turabian StyleLeboutte, Francois, Christian Engesser, Leutrim Zahiti, Cyrill A. Rentsch, Helge Seifert, Ralf Anding, Margret Hund-Georgiadis, Sandra Möhr, and Matthias Walter. 2023. "Prevalence of Unfavorable Video-Urodynamic Findings and Clinical Implications in Patients with Minimally Conscious State/Unresponsive Wakefulness Syndrome: A Retrospective Descriptive Analysis" Biomedicines 11, no. 9: 2432. https://doi.org/10.3390/biomedicines11092432
APA StyleLeboutte, F., Engesser, C., Zahiti, L., Rentsch, C. A., Seifert, H., Anding, R., Hund-Georgiadis, M., Möhr, S., & Walter, M. (2023). Prevalence of Unfavorable Video-Urodynamic Findings and Clinical Implications in Patients with Minimally Conscious State/Unresponsive Wakefulness Syndrome: A Retrospective Descriptive Analysis. Biomedicines, 11(9), 2432. https://doi.org/10.3390/biomedicines11092432