
Nab-Paclitaxel and Gemcitabine as First-Line Treatment of Metastatic Ampullary Adenocarcinoma with a Novel R-Spondin2 RNA Fusion and NTRK3 Mutation
 , ,
, , 
Abstract
:1. Introduction
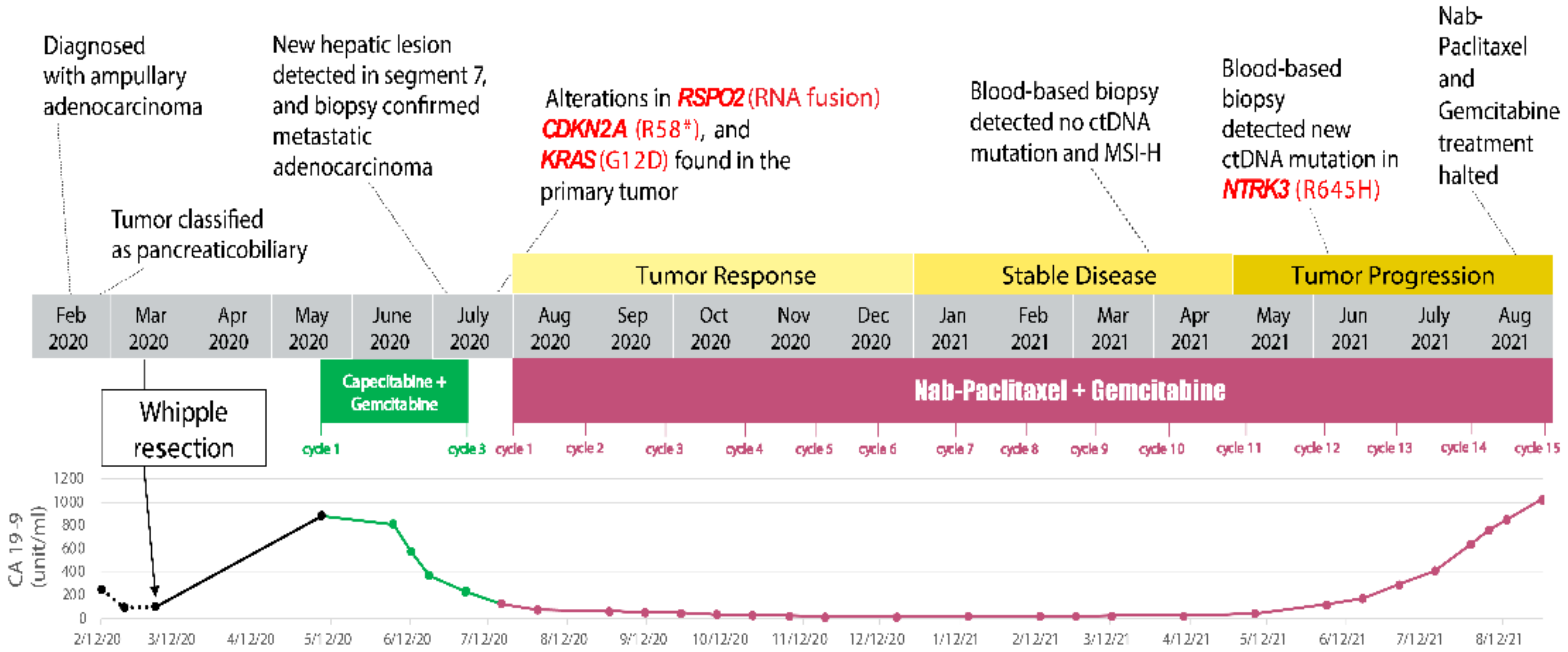
2. Case Description
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Albores-Saavedra, J.; Schwartz, A.M.; Batich, K.; Henson, D.E. Cancers of the ampulla of vater: Demographics, morphology, and survival based on 5625 cases from the SEER program. J. Surg. Oncol. 2009, 100, 598–605. [Google Scholar] [CrossRef]
- O’Connell, J.B.; Maggard, M.A.; Manunga, J.; Tomlinson, J.S.; Reber, H.A.; Ko, C.Y.; Hines, O.J. Survival After Resection of Ampullary Carcinoma: A National Population-Based Study. Ann. Surg. Oncol. 2008, 15, 1820–1827. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef] [PubMed]
- Ang, D.C.; Shia, J.; Tang, L.H.; Katabi, N.; Klimstra, D.S. The Utility of Immunohistochemistry in Subtyping Adenocarcinoma of the Ampulla of Vater. Am. J. Surg. Pathol. 2014, 38, 1371–1379. [Google Scholar] [CrossRef] [PubMed]
- Kimura, W.; Ohtsubo, K. Incidence, sites of origin, and immunohistochemical and histochemical characteristics of atypical epithelium and minute carcinoma of the papilla of vater. Cancer 1988, 61, 1394–1402. [Google Scholar] [CrossRef]
- Nappo, G.; Galvanin, J.; Gentile, D.; Capretti, G.; Pulvirenti, A.; Bozzarelli, S.; Rimassa, L.; Spaggiari, P.; Carrara, S.; Petitti, T.; et al. Long-term outcomes after pancreatoduodenectomy for ampullary cancer: The influence of the histological subtypes and comparison with the other periampullary neoplasms. Pancreatology 2021, 21, 950–956. [Google Scholar] [CrossRef]
- Kim, W.S.; Choi, D.W.; Choi, S.H.; Heo, J.S.; You, D.D.; Lee, H.G. Clinical significance of pathologic subtype in curatively resected ampulla of vater cancer. J. Surg. Oncol. 2011, 105, 266–272. [Google Scholar] [CrossRef]
- Chang, D.K.; Jamieson, N.B.; Johns, A.L.; Scarlett, C.J.; Pajic, M.; Chou, A.; Pinese, M.; Humphris, J.L.; Jones, M.D.; Toon, C.; et al. Histomolecular Phenotypes and Outcome in Adenocarcinoma of the Ampulla of Vater. J. Clin. Oncol. 2013, 31, 1348–1356. [Google Scholar] [CrossRef]
- Westgaard, A.; Pomianowska, E.; Clausen, O.P.F.; Gladhaug, I.P. Intestinal-type and pancreatobiliary-type adenocarcinomas: How does ampullary carcinoma differ from other periampullary malignancies? Ann. Surg. Oncol. 2013, 20, 430–439. [Google Scholar] [CrossRef]
- Williams, J.L.; Chan, C.K.; Toste, P.A.; Elliott, I.A.; Vasquez, C.R.; Sunjaya, D.B.; Swanson, E.A.; Koo, J.; Hines, O.J.; Reber, H.A.; et al. Association of Histopathologic Phenotype of Periampullary Adenocarcinomas with Survival. JAMA Surg. 2017, 152, 82–88. [Google Scholar] [CrossRef]
- Morris-Stiff, G.; Alabraba, E.; Tan, Y.-M.; Shapey, I.; Bhati, C.; Tanniere, P.; Mayer, D.; Buckels, J.; Bramhall, S.; Mirza, D. Assessment of survival advantage in ampullary carcinoma in relation to tumour biology and morphology. Eur. J. Surg. Oncol. 2009, 35, 746–750. [Google Scholar] [CrossRef]
- Ahn, D.H.; Bekaii-Saab, T. Ampullary Cancer: An Overview. Am. Soc. Clin. Oncol. Educ. Book 2014, 34, 112–115. [Google Scholar] [CrossRef]
- Stiles, Z.E.; Behrman, S.W.; Deneve, J.L.; Glazer, E.S.; Dong, L.; Wan, J.Y.; Martin, M.G.; Dickson, P.V. Ampullary adenocarcinoma: Defining predictors of survival and the impact of adjuvant therapy following surgical resection for stage I disease. J. Surg. Oncol. 2018, 117, 1500–1508. [Google Scholar] [CrossRef]
- Valle, J.; Wasan, H.; Palmer, D.H.; Cunningham, D.; Anthoney, A.; Maraveyas, A.; Madhusudan, S.; Iveson, T.; Hughes, S.; Pereira, S.P.; et al. Cisplatin plus Gemcitabine versus Gemcitabine for Biliary Tract Cancer. N. Engl. J. Med. 2010, 362, 1273–1281. [Google Scholar] [CrossRef] [PubMed]
- Overman, M.J.; Varadhachary, G.R.; Kopetz, S.; Adinin, R.; Lin, E.; Morris, J.S.; Eng, C.; Abbruzzese, J.L.; Wolff, R.A. Phase II Study of Capecitabine and Oxaliplatin for Advanced Adenocarcinoma of the Small Bowel and Ampulla of Vater. J. Clin. Oncol. 2009, 27, 2598–2603. [Google Scholar] [CrossRef] [PubMed]
- André, T.; Tournigand, C.; Rosmorduc, O.; Provent, S.; Maindrault-Goebel, F.; Avenin, D.; Selle, F.; Paye, F.; Hannoun, L.; Houry, S.; et al. Gemcitabine combined with oxaliplatin (GEMOX) in advanced biliary tract adenocarcinoma: A GERCOR study. Ann. Oncol. 2004, 15, 1339–1343. [Google Scholar] [CrossRef] [PubMed]
- Koprowski, M.A.; Sutton, T.L.; Brinkerhoff, B.T.; Grossberg, A.; Sheppard, B.C.; Mayo, S.C. Oncologic outcomes in resected ampullary cancer: Relevance of histologic subtype and adjuvant chemotherapy. Am. J. Surg. 2021, 221, 1128–1134. [Google Scholar] [CrossRef]
- Conti, R.M.; Bernstein, A.C.; Villaflor, V.M.; Schilsky, R.L.; Rosenthal, M.B.; Bach, P.B. Prevalence of Off-Label Use and Spending in 2010 Among Patent-Protected Chemotherapies in a Population-Based Cohort of Medical Oncologists. J. Clin. Oncol. 2013, 31, 1134–1139. [Google Scholar] [CrossRef]
- Jiang, Z.-Q.; Varadhachary, G.; Wang, X.; Kopetz, S.; Lee, J.E.; Wang, H.; Shroff, R.; Katz, M.; Wolff, R.A.; Fleming, J.; et al. A retrospective study of ampullary adenocarcinomas: Overall survival and responsiveness to fluoropyrimidine-based chemotherapy. Ann. Oncol. 2013, 24, 2349–2353. [Google Scholar] [CrossRef]
- Patel, M.; Uboha, N.V. Treatment Approach to Adenocarcinoma of the Ampulla of Vater. Curr. Treat. Options Oncol. 2021, 22, 103. [Google Scholar] [CrossRef]
- Von Hoff, D.D.; Ervin, T.; Arena, F.P.; Chiorean, E.G.; Infante, J.; Moore, M.; Seay, T.; Tjulandin, S.A.; Ma, W.W.; Saleh, M.N.; et al. Increased Survival in Pancreatic Cancer with nab-Paclitaxel plus Gemcitabine. N. Engl. J. Med. 2013, 369, 1691–1703. [Google Scholar] [CrossRef] [PubMed]
- Khorana, A.A.; Mangu, P.B.; Berlin, J.; Engebretson, A.; Hong, T.S.; Maitra, A.; Mohile, S.G.; Mumber, M.; Schulick, R.; Shapiro, M.; et al. Potentially Curable Pancreatic Cancer: American Society of Clinical Oncology Clinical Practice Guideline Update. J. Clin. Oncol. 2017, 35, 2324–2328. [Google Scholar] [CrossRef] [PubMed]
- Wong, W.; Lowery, M.A.; Berger, M.F.; Kemel, Y.; Taylor, B.; Zehir, A.; Srinivasan, P.; Bandlamudi, C.; Chou, J.; Capanu, M.; et al. Ampullary cancer: Evaluation of somatic and germline genetic alterations and association with clinical outcomes. Cancer 2019, 125, 1441–1448. [Google Scholar] [CrossRef]
- O’Hayer, K.; Farber, J.; Yeo, C.J.; Sama, A.R. HER-2-Positive Ampullary Adenocarcinoma: A Case Report. Case Rep. Pancreat. Cancer 2015, 1, 7–10. [Google Scholar] [CrossRef]
- Kapp, M.; Kosmala, A.; Kircher, S.; Luber, V.; Kunzmann, V. Exceptional Response to Nanoparticle Albumin-Bound Paclitaxel and Gemcitabine in a Patient with a Refractory Adenocarcinoma of the Ampulla of Vater. Case Rep. Oncol. 2016, 9, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Cen, P.; Wray, C.J.; Zhang, S.; Thosani, N.C.; Dinh, B.C.; Gonzalez, A.; Mohlere, V.; Bynon, J.S. Durable response for ampullary and duodenal adenocarcinoma with a nab-paclitaxel plus gemcitabine +/− cisplatin combination. Cancer Med. 2019, 8, 3464–3470. [Google Scholar] [CrossRef]
- Yachida, S.; Wood, L.D.; Suzuki, M.; Takai, E.; Totoki, Y.; Kato, M.; Luchini, C.; Arai, Y.; Nakamura, H.; Hama, N.; et al. Genomic Sequencing Identifies ELF3 as a Driver of Ampullary Carcinoma. Cancer Cell 2016, 29, 229–240. [Google Scholar] [CrossRef]
- Gingras, M.-C.; Covington, K.R.; Chang, D.K.; Donehower, L.A.; Gill, A.J.; Ittmann, M.M.; Creighton, C.J.; Johns, A.L.; Shinbrot, E.; Dewal, N.; et al. Ampullary Cancers Harbor ELF3 Tumor Suppressor Gene Mutations and Exhibit Frequent WNT Dysregulation. Cell Rep. 2016, 14, 907–919. [Google Scholar] [CrossRef]
- Ferchichi, M.; Jouini, R.; Ayari, I.; Koubaa, W.; Chadli-Debbiche, A.; BenBrahim, E. KRAS, NRAS and BRAF analysis of ampullary adenocarcinoma classified using CK7, CK20, MUC1 and MUC2. J. Gastrointest. Oncol. 2018, 9, 820–827. [Google Scholar] [CrossRef]
- A Study to Evaluate Abemaciclib in Advanced Biliary Tract Carcinoma. Available online: https://ClinicalTrials.gov/show/NCT04003896 (accessed on 1 July 2023).
- Yoon, J.K.; Lee, J.-S. Cellular signaling and biological functions of R-spondins. Cell. Signal. 2012, 24, 369–377. [Google Scholar] [CrossRef]
- Seshagiri, S.; Stawiski, E.W.; Durinck, S.; Modrusan, Z.; Storm, E.E.; Conboy, C.B.; Chaudhuri, S.; Guan, Y.; Janakiraman, V.; Jaiswal, B.S.; et al. Recurrent R-spondin fusions in colon cancer. Nature 2012, 488, 660–664. [Google Scholar] [CrossRef] [PubMed]
- Shinmura, K.; Kahyo, T.; Kato, H.; Igarashi, H.; Matsuura, S.; Nakamura, S.; Kurachi, K.; Nakamura, T.; Ogawa, H.; Funai, K.; et al. RSPO fusion transcripts in colorectal cancer in Japanese population. Mol. Biol. Rep. 2014, 41, 5375–5384. [Google Scholar] [CrossRef] [PubMed]
- AACR Project GENIE Consortium; André, F.; Arnedos, M.; Baras, A.S.; Baselga, J.; Bedard, P.L.; Berger, M.F.; Bierkens, M.; Calvo, F.; Cerami, E. AACR Project GENIE: Powering Precision Medicine through an International Consortium. Cancer Discov. 2017, 7, 818–831. [Google Scholar] [CrossRef]
- Seeber, A.; Kocher, F.; Xiu, J.; Spizzo, G.; Puccini, A.; Swensen, J.; Ellis, M.; Goldberg, R.M.; Grothey, A.; Shields, A.F.; et al. Molecular landscape of colorectal cancers harboring R-spondin fusions. J. Clin. Oncol. 2019, 37, 3588. [Google Scholar] [CrossRef]
- A Study to Evaluate the Safety and Tolerability of ETC-1922159 as a Single Agent and in Combination with Pembrolizumab in Advanced Solid Tumours. Available online: https://ClinicalTrials.gov/show/NCT02521844 (accessed on 1 July 2023).
- Study of DS-1062a in Advanced or Metastatic Non-Small Cell Lung Cancer with Actionable Genomic Alterations (TROPION-Lung05). Available online: https://ClinicalTrials.gov/show/NCT04484142 (accessed on 1 July 2023).
- Skoulidis, F.; Li, B.T.; Dy, G.K.; Price, T.J.; Falchook, G.S.; Wolf, J.; Italiano, A.; Schuler, M.; Borghaei, H.; Barlesi, F.; et al. Sotorasib for Lung Cancers with KRAS p.G12C Mutation. N. Engl. J. Med. 2021, 384, 2371–2381. [Google Scholar] [CrossRef]
- Chakraborty, S.; Ecker, B.L.; Seier, K.; Aveson, V.G.; Balachandran, V.P.; Drebin, J.A.; D’Angelica, M.I.; Kingham, T.P.; Sigel, C.S.; Soares, K.C.; et al. Genome-Derived Classification Signature for Ampullary Adenocarcinoma to Improve Clinical Cancer Care. Clin. Cancer Res. 2021, 27, 5891–5899. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| This Case Report (n = 1) | Yachida et al., 2016 [25] (n = 66) | Gingras et al., 2016 [26] (n = 71) | Ferchichi et al., 2018 [27] (n = 15) |
|---|---|---|---|
| KRAS exon 2, c.35G>A, p.G12D | KRAS (68%) | KRAS (72%) | KRAS p.G12D (27%) KRAS p.G12A (13%) NRAS p.G12D (7%) |
| CDKN2A exon 2, c.172C>T, p.R58 * | CDKN2A (9%) | CDKN2A (16%) | NR |
| RSPO2 (RNA fusion) MATN2 exon 4: RSPO2 exon 3 MATN2-RSPO2 | NR | NR | NR |
| ATM c.1009C>T p.R337C | NR | ATM (10%) | NR |
| NTRK1 Exon 6, c.640C>T, p.R214W | NR | NR | NR |
| NR | TP53 (67%) | TP53 (72%) | NR |
| NR | SMAD4 (20%) | SMAD4 (18%) | NR |
| NR | CTNNB1 (15%) | NR | NR |
| NR | ERBB3 (14%) | NR | NR |
| NR | GNAS (12%) | NR | NR |
| NR | CDH10 (12%) | NR | NR |
| NR | ELF3 (11%) | NR | NR |
| NR | NR | FBXW7 (8%) | NR |
| NR | NR | PIK3CA (13%) | NR |
| NR | NR | ARID1A (13%) | NR |
| NR | NR | APC (11%) | NR |
| NR | NR | TGFBR2 (10%) | NR |
| NR | NR | FBXW7 (8%) | NR |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Linscott, M.P.; Markus, H.; Sennett, M.; Abendroth, C.; Yee, N.S. Nab-Paclitaxel and Gemcitabine as First-Line Treatment of Metastatic Ampullary Adenocarcinoma with a Novel R-Spondin2 RNA Fusion and NTRK3 Mutation. Biomedicines 2023, 11, 2326. https://doi.org/10.3390/biomedicines11082326
Linscott MP, Markus H, Sennett M, Abendroth C, Yee NS. Nab-Paclitaxel and Gemcitabine as First-Line Treatment of Metastatic Ampullary Adenocarcinoma with a Novel R-Spondin2 RNA Fusion and NTRK3 Mutation. Biomedicines. 2023; 11(8):2326. https://doi.org/10.3390/biomedicines11082326
Chicago/Turabian StyleLinscott, Maryknoll P., Havell Markus, Mackenzie Sennett, Catherine Abendroth, and Nelson S. Yee. 2023. "Nab-Paclitaxel and Gemcitabine as First-Line Treatment of Metastatic Ampullary Adenocarcinoma with a Novel R-Spondin2 RNA Fusion and NTRK3 Mutation" Biomedicines 11, no. 8: 2326. https://doi.org/10.3390/biomedicines11082326
APA StyleLinscott, M. P., Markus, H., Sennett, M., Abendroth, C., & Yee, N. S. (2023). Nab-Paclitaxel and Gemcitabine as First-Line Treatment of Metastatic Ampullary Adenocarcinoma with a Novel R-Spondin2 RNA Fusion and NTRK3 Mutation. Biomedicines, 11(8), 2326. https://doi.org/10.3390/biomedicines11082326