

Trends in Dual Antiplatelet Therapy Use for Neurointerventional Procedures for the Management of Intracranial Aneurysms
Abstract
1. Introduction
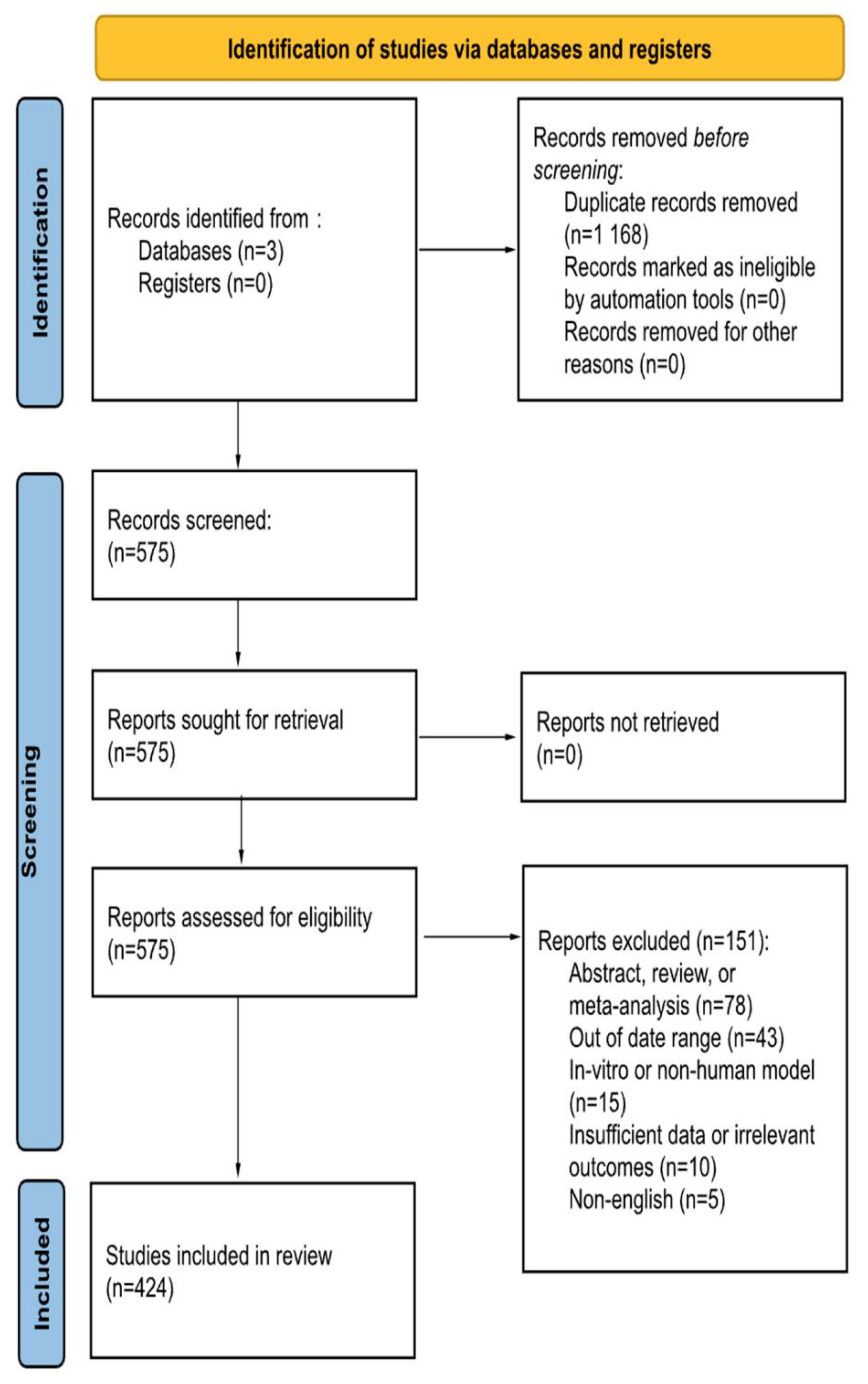
2. Methods
3. Results
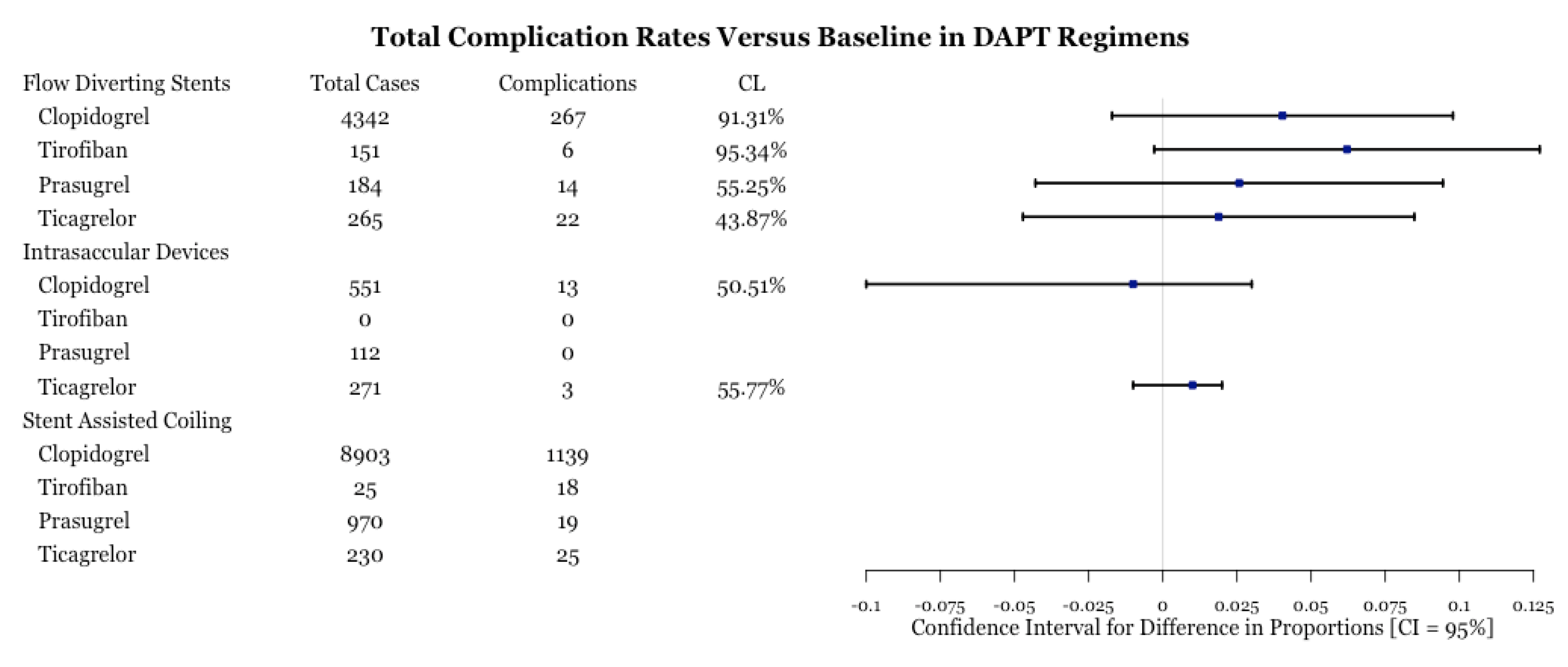
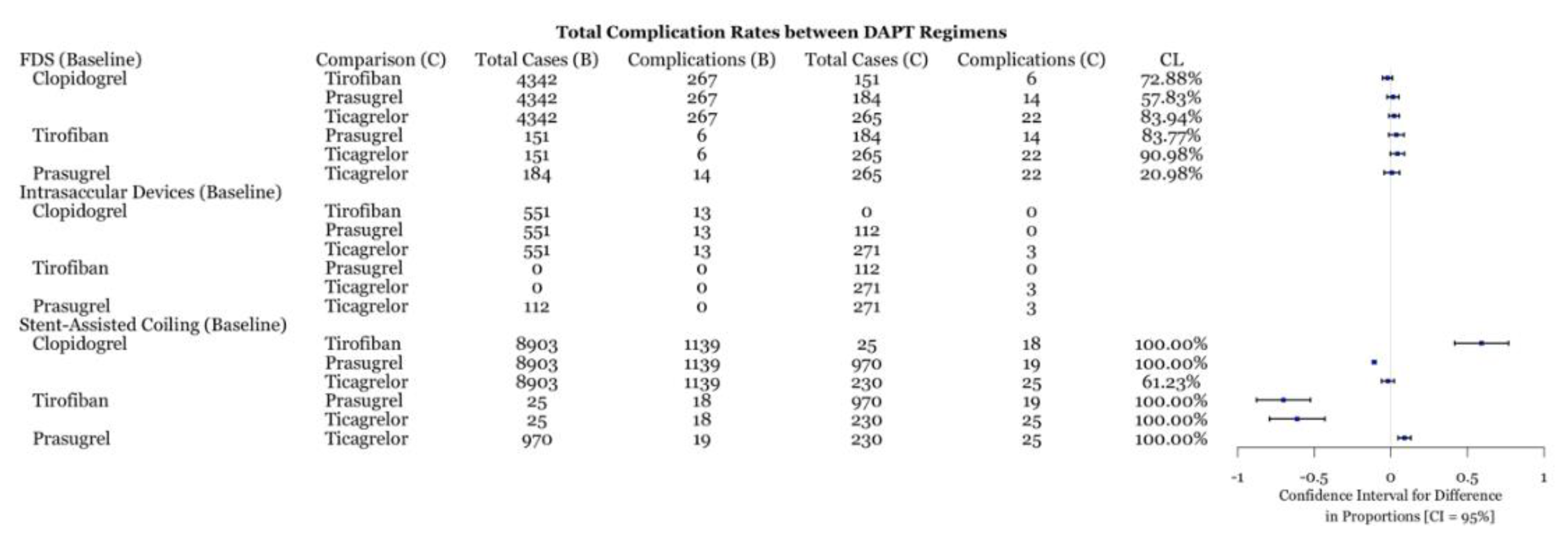
3.1. Total Complications
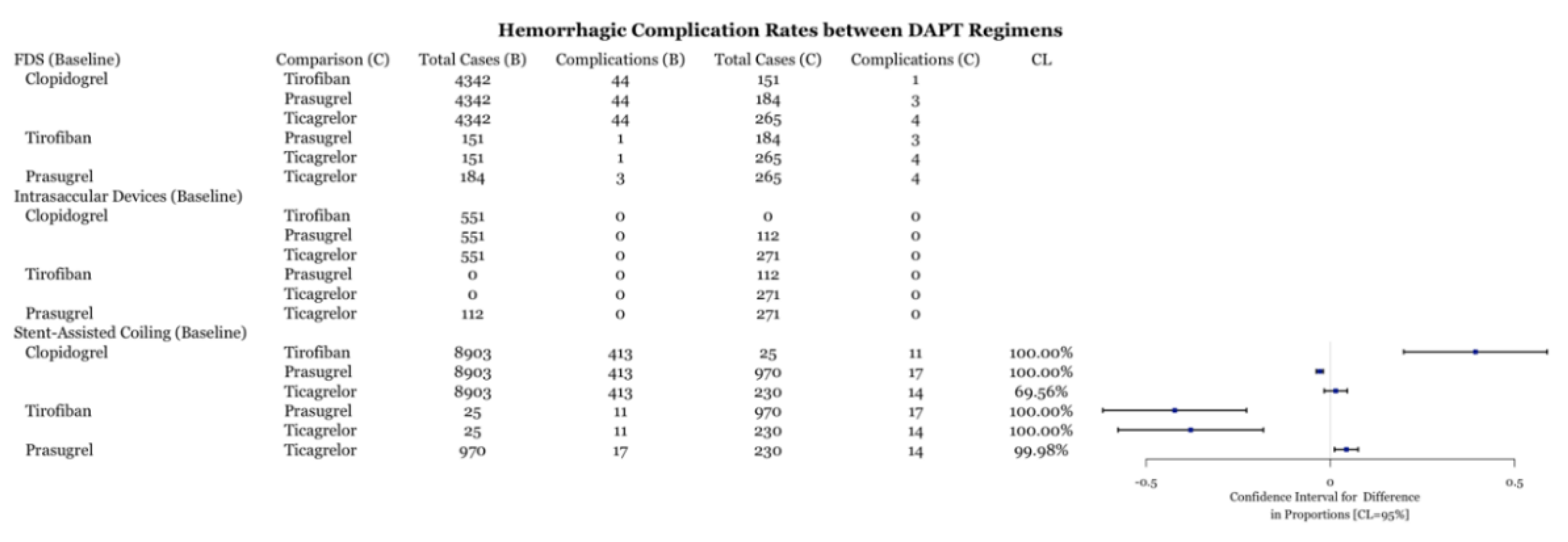
3.2. Hemorrhagic Complications
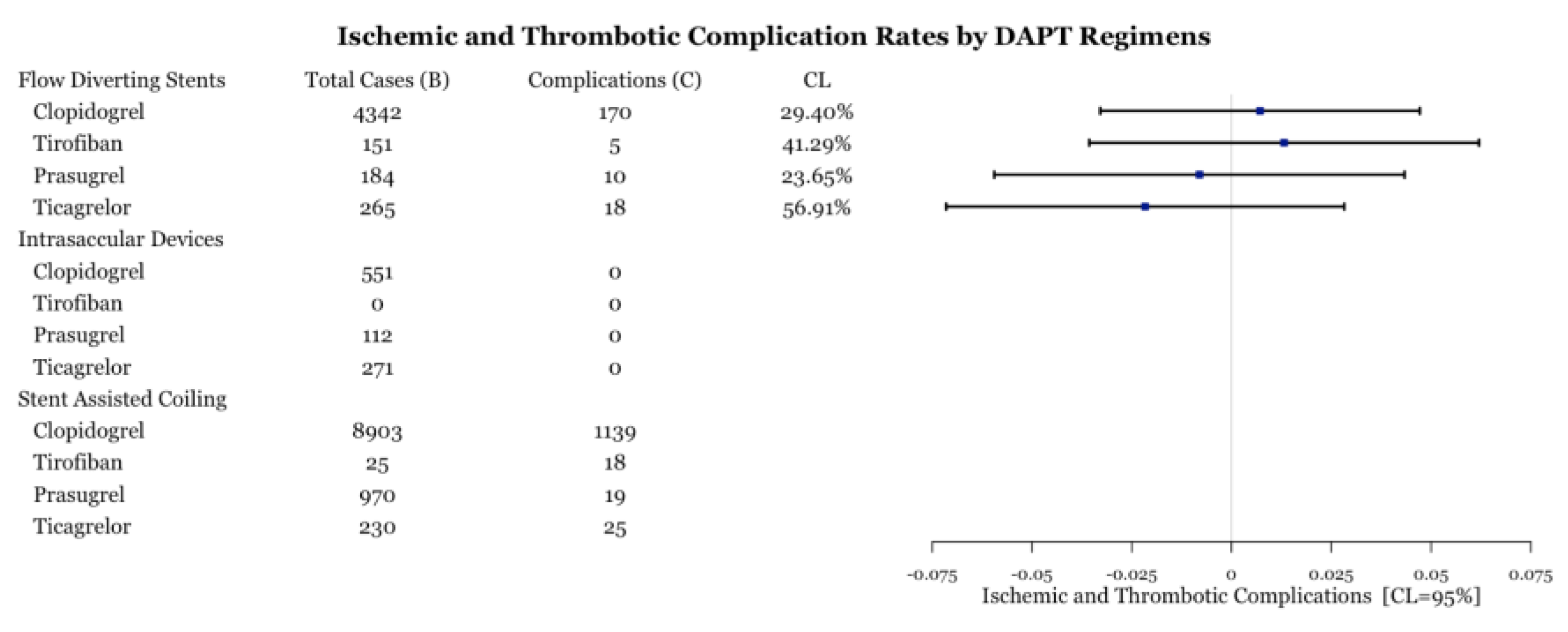
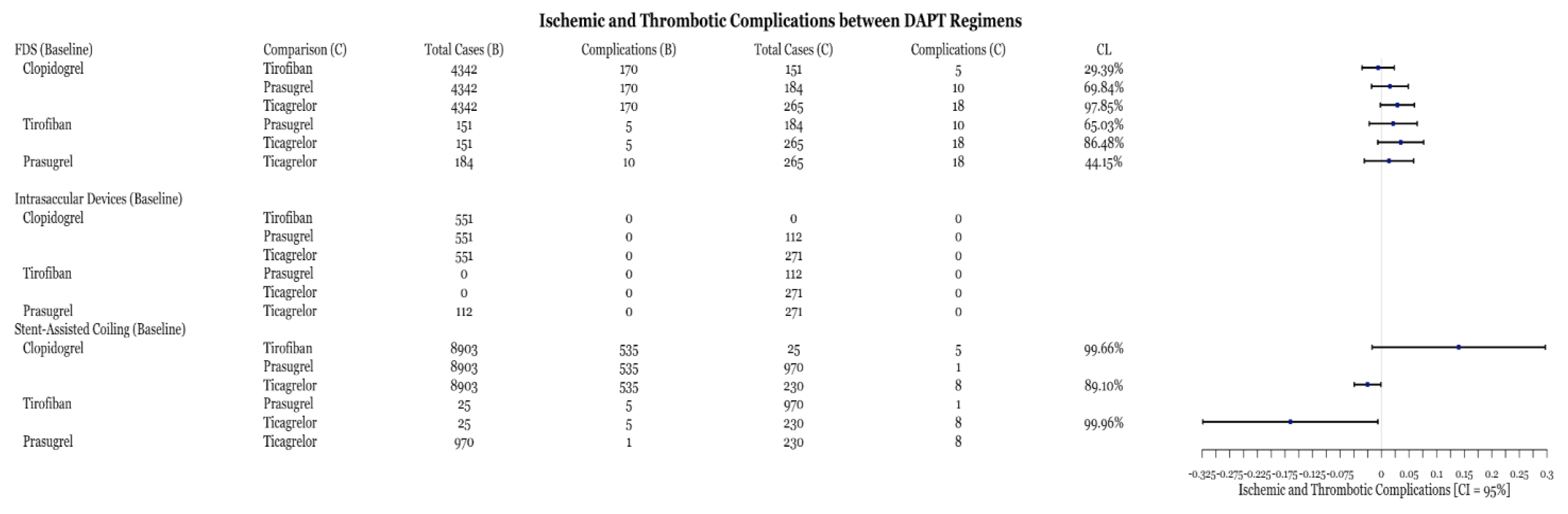
3.3. Ischemic and Thrombotic Complications
4. Discussion
4.1. General DAPT Use for Aneurysm Treatment
4.2. DAPT Use in Stent-Assisted Coiling
4.3. DAPT with FDS and Aneurysm Treatment
4.4. DAPT with Intrasaccular Devices and Aneurysms
4.5. Limitations
4.6. Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kamal, H.; Fine, E.J.; Shakibajahromi, B.; Mowla, A. A history of the path towards imaging of the brain: From skull radiography through cerebral angiography. Curr. J. Neurol. 2021, 19, 131–137. [Google Scholar] [CrossRef]
- Phan, K.; Huo, Y.R.; Jia, F.; Phan, S.; Rao, P.J.; Mobbs, R.J.; Mortimer, A.M. Meta-analysis of stent-assisted coiling versus coiling-only for the treatment of intracranial aneurysms. J. Clin. Neurosci. 2016, 31, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Campos, J.K.; Lien, B.; Wang, A.S.; Lin, L.-M. Advances in endovascular aneurysm management: Coiling and adjunctive devices. Stroke Vasc. Neurol. 2020, 5, 14–21. [Google Scholar] [CrossRef]
- Campos, J.K.; Ii, B.C.; Lien, B.V.; Zarrin, D.A.; Vo, C.D.; Colby, G.P.; Lin, L.-M.; Coon, A.L. Advances in endovascular aneurysm management: Flow modulation techniques with braided mesh devices. Stroke Vasc. Neurol. 2020, 5, 1–13. [Google Scholar] [CrossRef]
- Steinhubl, S.R.; Berger, P.B.; Iii, J.T.M.; Fry, E.T.A.; Delago, A.; Wilmer, C.; Topol, E.; CREDO Investigators. Early and Sustained Dual Oral Antiplatelet Therapy Following Percutaneous Coronary Intervention: A Randomized Controlled Trial. JAMA 2002, 288, 2411–2420, Erratum in JAMA 2003, 289, 987. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, S.; Zhao, F.; Mehta, S.R.; Chrolavicius, S.; Tognoni, G.; Fox, K.K. Clopidogrel in Unstable Angina to Prevent Recurrent Events Trial Investigators. Effects of Clopidogrel in Addition to Aspirin in Patients with Acute Coronary Syndromes without ST-Segment Elevation. N. Engl. J. Med. 2001, 345, 494–502, Erratum in N. Engl. J. Med. 2001, 345, 1506; Erratum in N. Engl. J. Med. 2001, 345, 1716. [Google Scholar]
- Wiviott, S.D.; Braunwald, E.; McCabe, C.H.; Montalescot, G.; Ruzyllo, W.; Gottlieb, S.; Neumann, F.-J.; Ardissino, D.; De Servi, S.; Murphy, S.A.; et al. Prasugrel versus Clopidogrel in Patients with Acute Coronary Syndromes. N. Engl. J. Med. 2007, 357, 2001–2015. [Google Scholar] [CrossRef] [PubMed]
- James, S.; Åkerblom, A.; Cannon, C.P.; Emanuelsson, H.; Husted, S.; Katus, H.; Skene, A.; Steg, P.G.; Storey, R.F.; Harrington, R.; et al. Comparison of ticagrelor, the first reversible oral P2Y12 receptor antagonist, with clopidogrel in patients with acute coronary syndromes: Rationale, design, and baseline characteristics of the PLATelet inhibition and patient Outcomes (PLATO) trial. Am. Heart J. 2009, 157, 599–605. [Google Scholar] [CrossRef]
- Mauri, L.; Kereiakes, D.J.; Normand, S.-L.T.; Wiviott, S.D.; Cohen, D.J.; Holmes, D.R.; Bangalore, S.; Cutlip, D.E.; Pencina, M.; Massaro, J.M. Rationale and design of the dual antiplatelet therapy study, a prospective, multicenter, randomized, double-blind trial to assess the effectiveness and safety of 12 versus 30 months of dual antiplatelet therapy in subjects undergoing percutaneous coronary intervention with either drug-eluting stent or bare metal stent placement for the treatment of coronary artery lesions. Am. Heart J. 2010, 160, 1035–1041.e1. [Google Scholar] [CrossRef]
- Nagahama, Y.; Allan, L.; Nakagawa, D.; Zanaty, M.; Starke, R.M.; Chalouhi, N.; Jabbour, P.; Brown, R.D.; Derdeyn, C.P.; Leira, E.C.; et al. Dual antiplatelet therapy in aneurysmal subarachnoid hemorrhage: Association with reduced risk of clinical vasospasm and delayed cerebral ischemia. J. Neurosurg. 2018, 129, 702–710. [Google Scholar] [CrossRef]
- Mauri, L.; Kereiakes, D.J.; Yeh, R.W.; Driscoll-Shempp, P.; Cutlip, D.E.; Steg, P.G.; Normand, S.-L.T.; Braunwald, E.; Wiviott, S.D.; Cohen, D.J.; et al. Twelve or 30 Months of Dual Antiplatelet Therapy after Drug-Eluting Stents. N. Engl. J. Med. 2014, 371, 2155–2166. [Google Scholar] [CrossRef]
- Quinn, M.J.; Fitzgerald, D.J. Ticlopidine and Clopidogrel. Circulation 1999, 100, 1667–1672. [Google Scholar] [CrossRef]
- Brandt, J.T.; Close, S.L.; Iturria, S.J.; Payne, C.D.; Farid, N.A.; Ernest, C.S.; Lachno, D.R.; Salazar, D.; Winters, K.J. Common polymorphisms of CYP2C19 and CYP2C9 affect the pharmacokinetic and pharmacodynamic response to clopidogrel but not prasugrel. J. Thromb. Haemost. 2007, 5, 2429–2436. [Google Scholar] [CrossRef] [PubMed]
- Sangkuhl, K.; Klein, T.E.; Altman, R.B. Clopidogrel pathway. Pharmacogenet. Genomics 2010, 20, 463–465. [Google Scholar] [CrossRef] [PubMed]
- Norgard, N.B.; Abu-Fadel, M. Comparison of prasugrel and clopidogrel in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Vasc. Health Risk Manag. 2009, 5, 873–882. [Google Scholar] [CrossRef]
- Mobley, J.E.; Bresee, S.J.; Wortham, D.C.; Craft, R.M.; Snider, C.C.; Carroll, R.C. Frequency of nonresponse antiplatelet activity of clopidogrel during pretreatment for cardiac catheterization. Am. J. Cardiol. 2004, 93, 456–458. [Google Scholar] [CrossRef] [PubMed]
- Dean, L. Prasugrel Therapy and CYP Genotype. In Medical Genetics Summaries; Pratt, V.M., Scott, S.A., Pirmohamed, M., Esquivel, B., Kattman, B.L., Malheiro, A.J., Eds.; National Center for Biotechnology Information: Bethesda, MD, USA, 2017. [Google Scholar]
- Xia, P.; Huang, Y.; Chen, G. The Effect of Ticagrelor for Endovascular Intervention of Intracranial Aneurysm Patients with or without Clopidogrel Resistant: A Meta-Analysis. Brain Sci. 2022, 12, 1077. [Google Scholar] [CrossRef] [PubMed]
- Hiatt, W.R.; Fowkes, F.G.R.; Heizer, G.; Berger, J.S.; Baumgartner, I.; Held, P.; Katona, B.G.; Mahaffey, K.W.; Norgren, L.; Jones, W.S.; et al. Ticagrelor versus Clopidogrel in Symptomatic Peripheral Artery Disease. N. Engl. J. Med. 2017, 376, 32–40. [Google Scholar] [CrossRef]
- Vranckx, P.; Valgimigli, M.; Jüni, P.; Hamm, C.; Steg, P.G.; Heg, D.; van Es, G.A.; McFadden, E.P.; Onuma, Y.; van Meijeren, C.; et al. Ticagrelor plus aspirin for 1 month, followed by ticagrelor monotherapy for 23 months vs aspirin plus clopidogrel or ticagrelor for 12 months, followed by aspirin monotherapy for 12 months after implantation of a drug-eluting stent: A multicentre, open-label, randomised superiority trial. Lancet 2018, 392, 940–949. [Google Scholar] [CrossRef]
- Wallentin, L.; Becker, R.C.; Budaj, A.; Cannon, C.P.; Emanuelsson, H.; Held, C.; Horrow, J.; Husted, S.; James, S.; Katus, H.; et al. Ticagrelor versus Clopidogrel in Patients with Acute Coronary Syndromes. N. Engl. J. Med. 2009, 361, 1045–1057. [Google Scholar] [CrossRef]
- Yang, M.; Huo, X.; Miao, Z.; Wang, Y. Platelet Glycoprotein IIb/IIIa Receptor Inhibitor Tirofiban in Acute Ischemic Stroke. Drugs 2019, 79, 515–529. [Google Scholar] [CrossRef]
- Kondo, K.; Umemura, K. Clinical Pharmacokinetics of Tirofiban, a Nonpeptide Glycoprotein IIb/IIIa Receptor Antagonist: Comparison with the monoclonal antibody abciximab. Clin. Pharmacokinet. 2002, 41, 187–195. [Google Scholar] [CrossRef]
- Topol, E.J.; Moliterno, D.J.; Herrmann, H.C.; Powers, E.R.; Grines, C.L.; Cohen, D.J.; Cohen, E.A.; Bertrand, M.; Neumann, F.-J.; Stone, G.W.; et al. Comparison of Two Platelet Glycoprotein IIb/IIIa Inhibitors, Tirofiban and Abciximab, for the Prevention of Ischemic Events with Percutaneous Coronary Revascularization. N. Engl. J. Med. 2001, 344, 1888–1894. [Google Scholar] [CrossRef]
- The RESTORE Investigators. Effects of Platelet Glycoprotein IIb/IIIa Blockade with Tirofiban on Adverse Cardiac Events in Patients with Unstable Angina or Acute Myocardial Infarction Undergoing Coronary Angioplasty. Circulation 1997, 96, 1445–1453. [Google Scholar] [CrossRef] [PubMed]
- Xiang, Y.; Zhao, H.; Ding, C.; Chen, H.; Wang, D.; Liu, A. The Prophylactic Use of Tirofiban versus Oral Antiplatelet Medications in Stent-Assisted Coiling of Intracranial Aneurysms: A Meta-analysis. Am. J. Neuroradiol. 2021, 42, 713–719. [Google Scholar] [CrossRef] [PubMed]
- Samaniego, E.A.; Gibson, E.; Nakagawa, D.; Ortega-Gutierrez, S.; Zanaty, M.; Roa, J.A.; Jabbour, P.; Hasan, D.M. Safety of tirofiban and dual antiplatelet therapy in treating intracranial aneurysms. Stroke Vasc. Neurol. 2019, 4, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Verdoia, M.; Pergolini, P.; Barbieri, L.; Rolla, R.; Nardin, M.; Negro, F.; Suryapranata, H.; De Luca, G. Impact of pre-procedural dual antiplatelet therapy on periprocedural myocardial infarction in patients undergoing percutaneous coronary interventions with adjunctive tirofiban. Thromb. Res. 2018, 164, 17–23. [Google Scholar] [CrossRef]
- Brack, M.J.; Hubner, P.J.; Gershlick, A.H. Anticoagulation after intracoronary stent insertion. Br. Heart J. 1994, 72, 294–296. [Google Scholar] [CrossRef][Green Version]
- Horowitz, M.B.; Pride, G.L.; Graybeal, D.F.; Purdy, P.D. Percutaneous Transluminal Angioplasty and Stenting of Midbasilar Stenoses: Three Technical Case Reports and Literature Review. Neurosurgery 1999, 45, 925–931. [Google Scholar] [CrossRef]
- Schirmer, C.M.; Bulsara, K.R.; Al-Mufti, F.; Haranhalli, N.; Thibault, L.; Hetts, S.W. Antiplatelets and antithrombotics in neurointerventional procedures: Guideline update. J. NeuroInterventional Surg. 2023. [Google Scholar] [CrossRef]
- Maree, A.O.; Curtin, R.J.; Dooley, M.; Conroy, R.M.; Crean, P.; Cox, D.; Fitzgerald, D.J. Platelet Response to Low-Dose Enteric-Coated Aspirin in Patients with Stable Cardiovascular Disease. J. Am. Coll. Cardiol. 2005, 46, 1258–1263. [Google Scholar] [CrossRef] [PubMed]
- Wijeyeratne, Y.D.; Heptinstall, S. Anti-platelet therapy: ADP receptor antagonists. Br. J. Clin. Pharmacol. 2011, 72, 647–657. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, Y.; Kondo, R.; Matsumori, Y.; Shimizu, H.; Takahashi, A.; Tominaga, T. Antiplatelet Therapy for Prevention of Thromboembolic Complications Associated with Coil Embolization of Unruptured Cerebral Aneurysms. Drugs R&D 2012, 12, 1–7. [Google Scholar] [CrossRef]
- Angiolillo, D.J.; Fernandez-Ortiz, A.; Bernardo, E.; Alfonso, F.; Macaya, C.; Bass, T.A.; Costa, M.A. Variability in Individual Responsiveness to Clopidogrel: Clinical Implications, Management, and Future Perspectives. J. Am. Coll. Cardiol. 2007, 49, 1505–1516. [Google Scholar] [CrossRef] [PubMed]
- Rosengart, A.; Collins, M.K.; Hendrix, P.; Uber, R.; Sartori, M.; Jain, A.; Mao, J.; Goren, O.; Schirmer, C.M.; Griessenauer, C.J. P2Y12inhibitors in neuroendovascular surgery: An opportunity for precision medicine. Interv. Neuroradiol. 2021, 27, 682–694. [Google Scholar] [CrossRef]
- Bender, M.T.; Zarrin, D.A.; Campos, J.K.; Jiang, B.; Chandra, A.; Vo, C.D.; Caplan, J.M.; Huang, J.; Tamargo, R.J.; Lin, L.-M.; et al. Precision of VerifyNow P2Y12 Assessment of Clopidogrel Response in Patients Undergoing Cerebral Aneurysm Flow Diversion. Neurosurgery 2018, 85, 543–549. [Google Scholar] [CrossRef]
- Kim, K.S.; Fraser, J.F.; Grupke, S.; Cook, A.M. Management of antiplatelet therapy in patients undergoing neuroendovascular procedures. J. Neurosurg. 2018, 129, 890–905. [Google Scholar] [CrossRef]
- Ma, Y.; Zhang, X.; Zhang, T.; Feng, Y.; Zhao, W.; Chen, X. Safety and efficacy of dual antiplatelet therapy combining aspirin and ticagrelor in patients with undergoing intracranial stenting procedures. J. Neurosurg. Sci. 2022. [Google Scholar] [CrossRef]
- Teng, R. Ticagrelor: Pharmacokinetic, Pharmacodynamic and Pharmacogenetic Profile: An Update. Clin. Pharmacokinet. 2015, 54, 1125–1138. [Google Scholar] [CrossRef]
- Gurbel, P.A.; Bliden, K.P.; Butler, K.; Antonino, M.J.; Wei, C.; Teng, R.; Rasmussen, L.; Storey, R.F.; Nielsen, T.; Eikelboom, J.W.; et al. Response to Ticagrelor in Clopidogrel Nonresponders and Responders and Effect of Switching Therapies. Circulation 2010, 121, 1188–1199. [Google Scholar] [CrossRef]
- Narata, A.P.; Amelot, A.; Bibi, R.; Herbreteau, D.; Angoulvant, D.; Gruel, Y.; Janot, K. Dual Antiplatelet Therapy Combining Aspirin and Ticagrelor for Intracranial Stenting Procedures: A Retrospective Single Center Study of 154 Consecutive Patients with Unruptured Aneurysms. Neurosurgery 2018, 84, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Yi, M.-M.; Do, H.P.; Li, Y.-C.; Wang, R.; Zhuang, Z.; Xu, M.-M.; Liu, T.; Shao, T.-F.; Ding, L.-P.; Ge, W.-H. Ticagrelor versus Clopidogrel in the Dual Antiplatelet Regimen for Unruptured Intracranial Aneurysm Treated with Stent-Assisted Coil Embolization: A Single-Center Cohort Study. World Neurosurg. 2023, 170, e755–e765. [Google Scholar] [CrossRef] [PubMed]
- Vrijens, B.; Claeys, M.J.; Legrand, V.; Vandendriessche, E.; Van de Werf, F. Projected inhibition of platelet aggregation with ticagrelor twice daily vs. clopidogrel once daily based on patient adherence data (the TWICE project). Br. J. Clin. Pharmacol. 2014, 77, 746–755. [Google Scholar] [CrossRef][Green Version]
- Roffman, D.S. Developments in Oral Antiplatelet Agents for the Treatment of Acute Coronary Syndromes: Clopidogrel, Prasugrel, and Ticagrelor. J. Pharm. Pract. 2015, 29, 239–249. [Google Scholar] [CrossRef] [PubMed]
- Sedat, J.; Chau, Y.; Gaudart, J.; Sachet, M.; Beuil, S.; Lonjon, M. Prasugrel versus clopidogrel in stent-assisted coil embolization of unruptured intracranial aneurysms. Interv. Neuroradiol. 2016, 23, 52–59. [Google Scholar] [CrossRef]
- Russo, R.; Bradac, G.B.; Castellan, L.; Gallesio, I.; Garbossa, D.; Iannucci, G.; Mardighian, D.; Menozzi, R.; Pitrone, A.; Romano, G.; et al. Neuroform Atlas stent-assisted coiling of ruptured intracranial aneurysms: A multicenter study. J. Neuroradiol. 2020, 48, 479–485. [Google Scholar] [CrossRef]
- Finneran, M.M.; Young, M.; Farhat, H. Antiplatelet Therapy for Stent-Assisted Coil of Ruptured Middle Cerebral Artery Bifurcation Aneurysm: Is There a Right Answer? Cureus 2020, 12, e11612. [Google Scholar] [CrossRef]
- Zi-Liang, W.; Xiao-Dong, L.; Tian-Xiao, L.; Liang-Fu, Z.; Jiang-Yu, X.; Wei-Xing, B.; Ying-Kun, H.; Gang-Qin, X.; Qiu-Ji, S.; Li, L.; et al. Intravenous administration of tirofiban versus loading dose of oral clopidogrel for preventing thromboembolism in stent-assisted coiling of intracranial aneurysms. Int. J. Stroke 2016, 12, 553–559. [Google Scholar] [CrossRef]
- Ospel, J.; Brouwer, P.; Dorn, F.; Arthur, A.; Jensen, M.; Nogueira, R.; Chapot, R.; Albuquerque, F.; Majoie, C.; Jayaraman, M.; et al. Antiplatelet Management for Stent-Assisted Coiling and Flow Diversion of Ruptured Intracranial Aneurysms: A DELPHI Consensus Statement. Am. J. Neuroradiol. 2020, 41, 1856–1862, Erratum in Am. J. Neuroradiol. 2021, 42, E76. [Google Scholar] [CrossRef]
- Ma, Y.; Jia, C.; Zhang, T.; Feng, Y.; Chen, X.; Zhao, W. Safety and efficacy of intravenous tirofiban for stent-assisted coiling in acutely ruptured intracranial aneurysms: A single center experience. Interv. Neuroradiol. 2021, 28, 476–481. [Google Scholar] [CrossRef]
- Shen, G.; Jia, Z.; Zhao, L.; Lu, G.; Liu, S.; Shi, H. The safety and efficacy of a low dose of tirofiban for early complications during and after stent-assisted coiling of ruptured intracranial aneurysms: A propensity matching study. Clin. Neurol. Neurosurg. 2022, 214, 107132. [Google Scholar] [CrossRef]
- Kim, S.; Choi, J.-H.; Kang, M.; Cha, J.-K.; Huh, J.-T. Safety and Efficacy of Intravenous Tirofiban as Antiplatelet Premedication for Stent-Assisted Coiling in Acutely Ruptured Intracranial Aneurysms. Am. J. Neuroradiol. 2015, 37, 508–514. [Google Scholar] [CrossRef] [PubMed]
- Bilgin, C.; Ghozy, S.; Shehata, M.; Ibrahim, M.; Jabal, M.S.; Kobeissi, H.; Gerberi, D.J.; Kadirvel, R.; Kallmes, D.F. The Prophylactic Use of Glycoprotein 2b/3a Inhibitors in the Endovascular Treatment of Intracranial Aneurysms: A Systematic Review and Meta-Analysis. World Neurosurg. 2022, 168, e50–e66. [Google Scholar] [CrossRef] [PubMed]
- Siebler, M.; Hennerici, M.G.; Schneider, D.; von Reutern, G.M.; Seitz, R.J.; Röther, J.; Witte, O.W.; Hamann, G.; Junghans, U.; Villringer, A.; et al. Safety of Tirofiban in Acute Ischemic Stroke. Stroke 2011, 42, 2388–2392. [Google Scholar] [CrossRef] [PubMed]
- McClellan, K.J.; Goa, K.L. Tirofiban. A review of its use in acute coronary syndromes. Drugs 1998, 56, 1067–1080. [Google Scholar] [CrossRef]
- Li, Y.; Zhang, X.; Guo, Z.; Zhu, J.; Xu, R.; He, Z.; Sun, X. Standard vs. Modified Antiplatelet Therapy Based on Thromboelastography With Platelet Mapping for Preventing Bleeding Events in Patients Undergoing Stent-Assisted Coil for a Ruptured Intracranial Aneurysm. Front. Neurol. 2021, 11, 615829. [Google Scholar] [CrossRef] [PubMed]
- Xian, E.; Morrison, T.; Wong, J. Hyperacute in-Stent Thrombosis Causing Large Vessel Occlusion after Stent-Assisted Aneurysm Coiling Secondary to Complete Clopidogrel and Prasugrel Resistance: A Case Report. J. Neurol. Surg. Part A Cent. Eur. Neurosurg. 2022. [Google Scholar] [CrossRef]
- Tonetti, D.A.; Jankowitz, B.T.; Gross, B.A. Antiplatelet Therapy in Flow Diversion. Neurosurgery 2019, 86, S47–S52. [Google Scholar] [CrossRef] [PubMed]
- Becske, T.; Kallmes, D.F.; Saatci, I.; McDougall, C.G.; Szikora, I.; Lanzino, G.; Moran, C.J.; Woo, H.H.; Lopes, D.K.; Berez, A.L.; et al. Pipeline for Uncoilable or Failed Aneurysms: Results from a Multicenter Clinical Trial. Radiology 2013, 267, 858–868. [Google Scholar] [CrossRef]
- Brown, S.-A.; Pereira, N. Pharmacogenomic Impact of CYP2C19 Variation on Clopidogrel Therapy in Precision Cardiovascular Medicine. J. Pers. Med. 2018, 8, 8. [Google Scholar] [CrossRef]
- Park, K.; Ozaki, T.; Kostynskyy, A.; Kortman, H.; Hilario, A.; Nicholson, P.; Agid, R.; Krings, T.; Pereira, V. Ticagrelor versus Clopidogrel in the Dual Antiplatelet Regimen for Intracranial Stenting or Flow-Diverter Treatment for Unruptured Cerebral Aneurysms: A Single-Center Cohort Study. Am. J. Neuroradiol. 2021, 42, 1638–1644. [Google Scholar] [CrossRef]
- Podlasek, A.; Al Sultan, A.A.; Assis, Z.; Kashani, N.; Goyal, M.; Almekhlafi, M.A. Outcome of intracranial flow diversion according to the antiplatelet regimen used: A systematic review and meta-analysis. J. NeuroInterventional Surg. 2019, 12, 148–155. [Google Scholar] [CrossRef]
- Wu, Q.; Shao, Q.; Li, L.; Liang, X.; Chang, K.; Li, T.; He, Y. Prophylactic administration of tirofiban for preventing thromboembolic events in flow diversion treatment of intracranial aneurysms. J. NeuroInterventional Surg. 2020, 13, 835–840. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, A.H.; Monteiro, A.; Hanel, R.A.; Kan, P.; Mohanty, A.; Cortez, G.M.; Rabinovich, M.; Matouk, C.; Sujijantarat, N.; Romero, C.; et al. Triple therapy versus dual-antiplatelet therapy for dolichoectatic vertebrobasilar fusiform aneurysms treated with flow diverters. J. NeuroInterventional Surg. 2022, 15, 655–663. [Google Scholar] [CrossRef] [PubMed]
- Geisbush, T.R.; Pulli, B.; Wolman, D.N.; Pendharkar, A.V.; Telischak, N.A. A case of recurrent aneurysm resulting from dual antiplatelet plus anticoagulation after confirmed aneurysm closure following coil-assisted flow diversion. Radiol. Case Rep. 2022, 17, 4075–4078. [Google Scholar] [CrossRef] [PubMed]
- Luo, C.; Jin, L.; Dong, J.; Fu, Z.; Liu, E.; Yin, S.; Jian, L.; Luo, P.; Liu, B.; Huang, W.; et al. Clinical outcomes of pipeline embolization devices with shield technology for treating intracranial aneurysms. Front. Neurol. 2022, 13, 971664. [Google Scholar] [CrossRef] [PubMed]
- Lobsien, D.; Clajus, C.; Behme, D.; Ernst, M.; Riedel, C.; Abu-Fares, O.; Götz, F.; Fiorella, D.; Klisch, J. Aneurysm Treatment in Acute SAH with Hydrophilic-Coated Flow Diverters under Single-Antiplatelet Therapy: A 3-Center Experience. Am. J. Neuroradiol. 2021, 42, 508–515. [Google Scholar] [CrossRef]
- Aguilar-Perez, M.; Hellstern, V.; AlMatter, M.; Wendl, C.; Bäzner, H.; Ganslandt, O.; Henkes, H. The p48 Flow Modulation Device with Hydrophilic Polymer Coating (HPC) for the Treatment of Acutely Ruptured Aneurysms: Early Clinical Experience Using Single Antiplatelet Therapy. Cardiovasc. Interv. Radiol. 2020, 43, 740–748. [Google Scholar] [CrossRef]
- Matsuda, Y.; Jang, D.-K.; Chung, J.; Wainwright, J.M.; Lopes, D. Preliminary outcomes of single antiplatelet therapy for surface-modified flow diverters in an animal model: Analysis of neointimal development and thrombus formation using OCT. J. NeuroInterventional Surg. 2018, 11, 74–79. [Google Scholar] [CrossRef]
- Senol, Y.C.; Orscelik, A.; Ghozy, S.; Kobeissi, H.; Arul, S.; Bilgin, C.; Kadirvel, R.; Kallmes, D.F. The safety profile of single antiplatelet therapy with flow diverters: Systematic review and meta-analysis. Interv. Neuroradiol. 2023, 15910199231168669. [Google Scholar] [CrossRef]
- Bender, M.T.; Zarrin, D.A.; Jiang, B.; Campos, J.K.; Lin, L.-M.; Young, R.W.; Colby, G.P.; Coon, A.L. Aspirin Monotherapy in Flow Diversion of Selected Internal Carotid Artery Aneurysms. World Neurosurg. 2019, 134, 580–583. [Google Scholar] [CrossRef] [PubMed]
- Goyal, N.; Hoit, D.; DiNitto, J.; Elijovich, L.; Fiorella, D.; Pierot, L.; Lamin, S.; Spelle, L.; Saatci, I.; Cekirge, S.; et al. How to WEB: A practical review of methodology for the use of the Woven EndoBridge. J. NeuroInterventional Surg. 2020, 12, 512–520. [Google Scholar] [CrossRef]
- Narsinh, K.H.; Caton, M.T.; Mahmood, N.F.; Higashida, R.T.; Halbach, V.V.; Hetts, S.W.; Amans, M.R.; Dowd, C.F.; Cooke, D.L. Intrasaccular flow disruption (WEB) of a large wide-necked basilar apex aneurysm using PulseRider-assistance. Interdiscip. Neurosurg. 2020, 24, 101072. [Google Scholar] [CrossRef] [PubMed]
- Sirakov, A.; Bhogal, P.; Sirakova, K.; Penkov, M.; Minkin, K.; Ninov, K.; Hristov, H.; Hadzhiyanev, A.; Karakostov, V.; Sirakov, S. Endovascular treatment of wide-necked intracranial aneurysms using the Nautilus Intrasaccular System: Initial case series of 41 patients at a single center. J. NeuroInterventional Surg. 2022. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Tian, H.; Xiang, B.; Liu, J.; Xiang, H. Woven EndoBridge device for the treatment of ruptured intracranial aneurysms: A systematic review of clinical and angiographic results. Interv. Neuroradiol. 2021, 28, 240–249. [Google Scholar] [CrossRef]
- Piotin, M.; Fahed, R.; Redjem, H.; Smajda, S.; Desilles, J.P.; Escalard, S.; Maïer, B.; Hebert, S.; Delvoye, F.; Mazighi, M.; et al. The ARTISSE intrasaccular device for intracranial aneurysm treatment: Short-term, mid-term and long-term clinical and angiographic results. J. NeuroInterventional Surg. 2021, 14, 957–961. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Search Phrase | PubMed | Embase | Scopus |
|---|---|---|---|
| (dual antiplatelet therapy) AND (flow diversion) | 95 | 220 | 197 |
| (dual antiplatelet therapy) AND (pipeline embolization device) | 70 | 230 | 184 |
| (dual antiplatelet therapy) AND (fred) | 7 | 47 | 32 |
| (dual antiplatelet therapy) AND (p64) | 3 | 8 | 6 |
| (dual antiplatelet therapy) AND (silk) | 2 | 29 | 24 |
| (dual antiplatelet therapy) AND (surpass) | 6 | 31 | 32 |
| (dual antiplatelet therapy) AND (stent-assisted coiling) | 59 | 174 | 158 |
| (dual antiplatelet therapy) AND (intrasaccular device) | 3 | 15 | 9 |
| (dual antiplatelet therapy) AND (WEB) | 8 | 51 | 43 |
| Total | 253 | 805 | 685 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meyer, B.M.; Campos, J.K.; Collard de Beaufort, J.C.; Chen, I.; Khan, M.W.; Amin, G.; Zarrin, D.A.; Lien, B.V.; Coon, A.L. Trends in Dual Antiplatelet Therapy Use for Neurointerventional Procedures for the Management of Intracranial Aneurysms. Biomedicines 2023, 11, 2234. https://doi.org/10.3390/biomedicines11082234
Meyer BM, Campos JK, Collard de Beaufort JC, Chen I, Khan MW, Amin G, Zarrin DA, Lien BV, Coon AL. Trends in Dual Antiplatelet Therapy Use for Neurointerventional Procedures for the Management of Intracranial Aneurysms. Biomedicines. 2023; 11(8):2234. https://doi.org/10.3390/biomedicines11082234
Chicago/Turabian StyleMeyer, Benjamen M., Jessica K. Campos, Jonathan C. Collard de Beaufort, Ivette Chen, Muhammad Waqas Khan, Gizal Amin, David A. Zarrin, Brian V. Lien, and Alexander L. Coon. 2023. "Trends in Dual Antiplatelet Therapy Use for Neurointerventional Procedures for the Management of Intracranial Aneurysms" Biomedicines 11, no. 8: 2234. https://doi.org/10.3390/biomedicines11082234
APA StyleMeyer, B. M., Campos, J. K., Collard de Beaufort, J. C., Chen, I., Khan, M. W., Amin, G., Zarrin, D. A., Lien, B. V., & Coon, A. L. (2023). Trends in Dual Antiplatelet Therapy Use for Neurointerventional Procedures for the Management of Intracranial Aneurysms. Biomedicines, 11(8), 2234. https://doi.org/10.3390/biomedicines11082234