
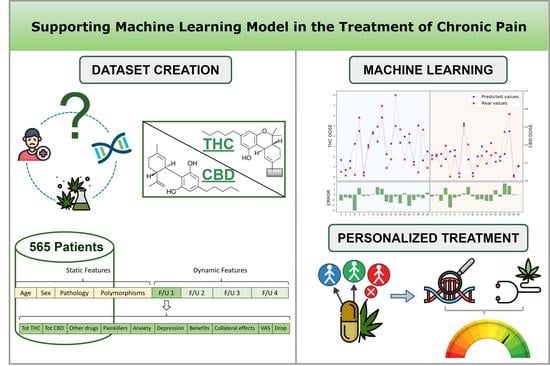
Supporting Machine Learning Model in the Treatment of Chronic Pain
 , , and
, , and 
Abstract
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Gene Analysis
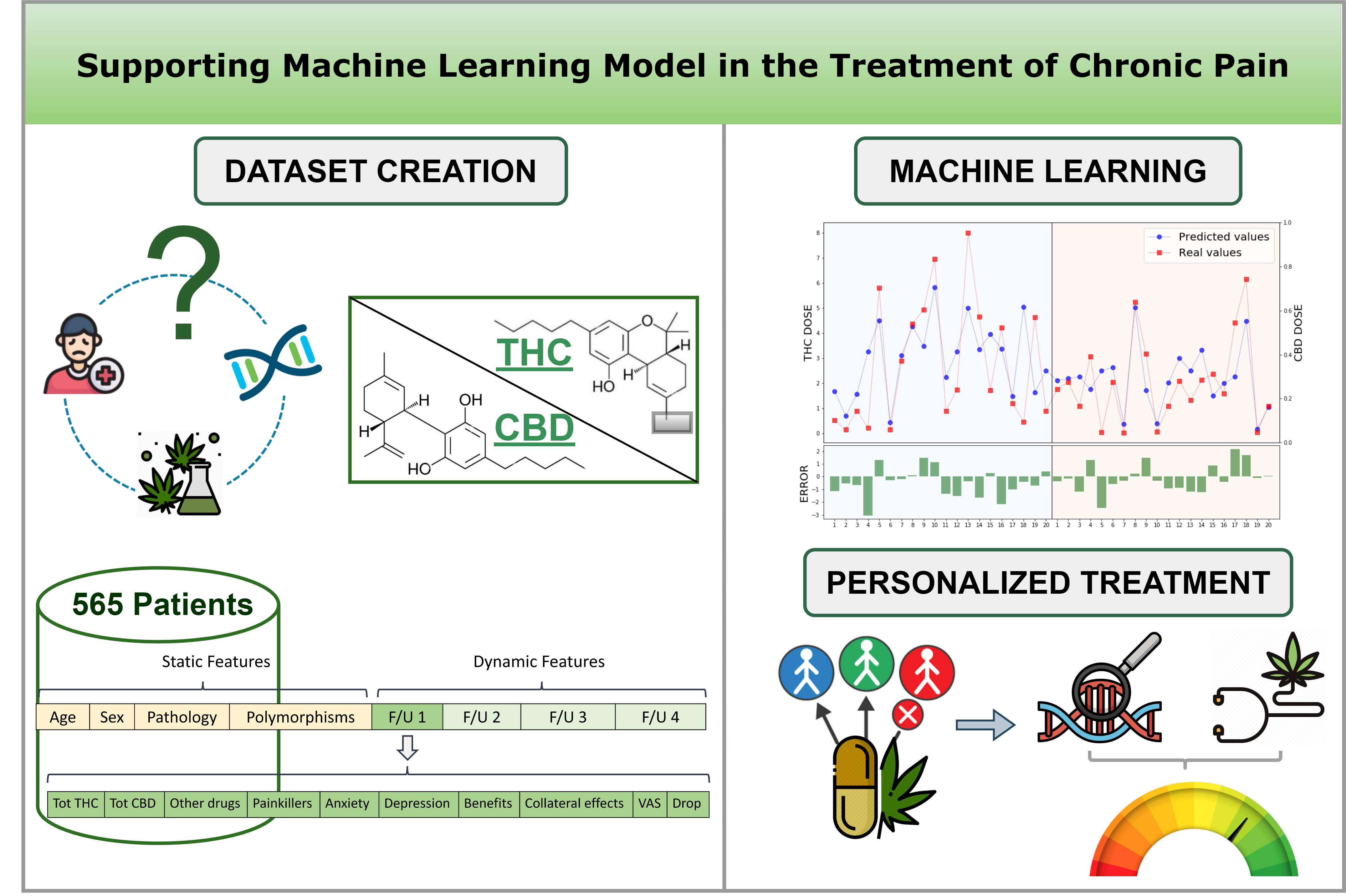
2.3. Clinical Dataset
2.4. Machine Learning Method
3. Results
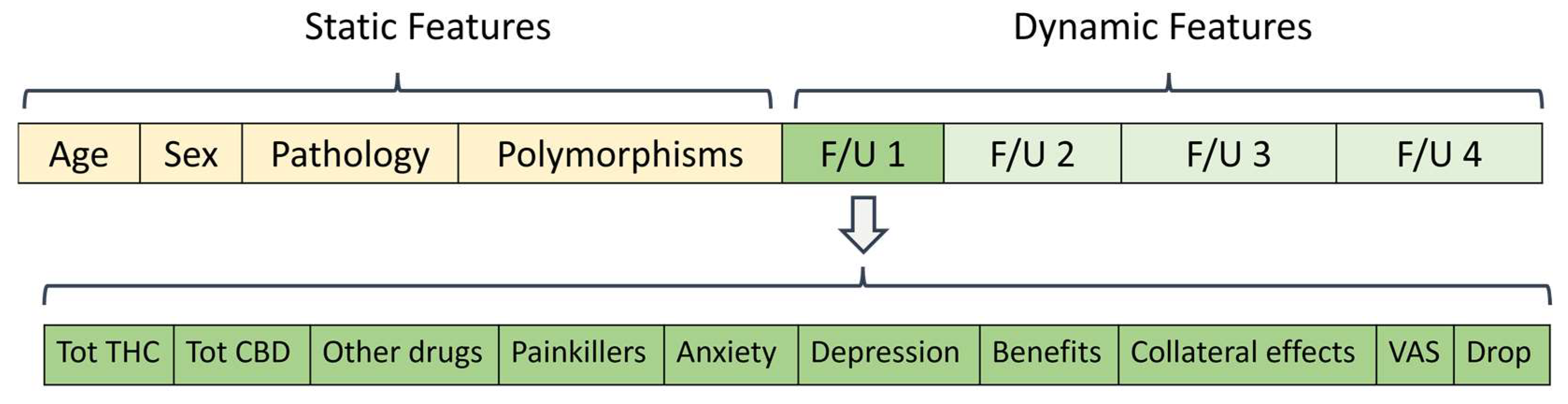
3.1. Data Pre-Processing
3.2. XGBoost Prediction
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dahlhamer, J.; Lucas, J.; Zelaya, C.; Nahin, R.; Mackey, S.; DeBar, L.; Kerns, R.; Korff, M.; Porter, L.; Helmick, C. Prevalence of Chronic Pain and High-Impact Chronic Pain Among Adults—United States, 2016. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 1001–1006. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare. Chronic Pain in Australia; Cat. no. PHE 267; Australian Institute of Health and Welfare: Canberra, Australia, 2020.
- Breivik, H.; Collett, B.; Ventafridda, V.; Cohen, R.; Gallacher, D. Survey of Chronic Pain in Europe: Prevalence, Impact on Daily Life, and Treatment. Eur. J. Pain 2006, 10, 287–333. [Google Scholar] [CrossRef]
- Fillingim, R.B. Chapter 49—Sex, Gender, and Pain. In Principles of Gender-Specific Medicine, 4th ed.; Legato, M.J., Ed.; Academic Press: Cambridge, MA, USA, 2023; pp. 769–792. ISBN 978-0-323-88534-8. [Google Scholar]
- Reid, M.C.; Eccleston, C.; Pillemer, K. Management of Chronic Pain in Older Adults. BMJ 2015, 350, h532. [Google Scholar] [CrossRef]
- Jackson, T.; Thomas, S.; Stabile, V.; Han, X.; Shotwell, M.; McQueen, K. Prevalence of Chronic Pain in Low-Income and Middle-Income Countries: A Systematic Review and Meta-Analysis. Lancet 2015, 385, S10. [Google Scholar] [CrossRef]
- Hadi, M.A.; McHugh, G.A.; Closs, S.J. Impact of Chronic Pain on Patients’ Quality of Life: A Comparative Mixed-Methods Study. J. Patient Exp. 2019, 6, 133–141. [Google Scholar] [CrossRef]
- Mathias, J.L.; Cant, M.L.; Burke, A.L.J. Sleep Disturbances and Sleep Disorders in Adults Living with Chronic Pain: A Meta-Analysis. Sleep Med. 2018, 52, 198–210. [Google Scholar] [CrossRef]
- Institute of Medicine (US) Committee on Advancing Pain Research, Care, and Education. Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research; The National Academies Press: Washington, DC, USA, 2011; ISBN 978-0-309-25627-8. [Google Scholar]
- Tang, N.; Crane, C. Suicidality in Chronic Pain: A Review of the Prevalence, Risk Factors and Psychological Links. Psychol. Med. 2006, 36, 575–586. [Google Scholar] [CrossRef]
- Hoehe, M.R.; Caenazzo, L.; Martinez, M.M.; Hsieh, W.T.; Modi, W.S.; Gershon, E.S.; Bonner, T.I. Genetic and Physical Mapping of the Human Cannabinoid Receptor Gene to Chromosome 6q14-Q15. New Biol. 1991, 3, 880–885. [Google Scholar]
- Gérard, C.; Mollereau, C.; Vassart, G.; Parmentier, M. Nucleotide Sequence of a Human Cannabinoid Receptor CDNA. Nucleic Acids Res. 1990, 18, 7142. [Google Scholar] [CrossRef]
- Galiègue, S.; Mary, S.; Marchand, J.; Dussossoy, D.; Carrière, D.; Carayon, P.; Bouaboula, M.; Shire, D.; LE Fur, G.; Casellas, P. Expression of Central and Peripheral Cannabinoid Receptors in Human Immune Tissues and Leukocyte Subpopulations. Eur. J. Biochem. 1995, 232, 54–61. [Google Scholar] [CrossRef]
- Pattnaik, F.; Nanda, S.; Mohanty, S.; Dalai, A.K.; Kumar, V.; Ponnusamy, S.K.; Naik, S. Cannabis: Chemistry, Extraction and Therapeutic Applications. Chemosphere 2022, 289, 133012. [Google Scholar] [CrossRef]
- Russo, E. Cannabis Therapeutics and the Future of Neurology. Front. Integr. Neurosci. 2018, 12, 51. [Google Scholar] [CrossRef]
- Billnitzer, A.; Jankovic, J. Current Management of Tics and Tourette Syndrome: Behavioral, Pharmacologic, and Surgical Treatments. Neurotherapeutics 2020, 17, 1681–1693. [Google Scholar] [CrossRef]
- Fitzcharles, M.-A.; Baerwald, C.; Ablin, J.; Häuser, W. Efficacy, Tolerability and Safety of Cannabinoids in Chronic Pain Associated with Rheumatic Diseases (Fibromyalgia Syndrome, Back Pain, Osteoarthritis, Rheumatoid Arthritis). Der. Schmerz. 2016, 30, 47–61. [Google Scholar] [CrossRef]
- Scicluna, J.C.; Giovanni, G. Di Cannabinoids for Fibromyalgia: An Updated Systematic Review. medRxiv 2022. [Google Scholar] [CrossRef]
- Passani, A.; Posarelli, C.; Sframeli, A.T.; Perciballi, L.; Pellegrini, M.; Guidi, G.; Figus, M. Cannabinoids in Glaucoma Patients: The Never-Ending Story. J. Clin. Med. 2020, 9, 3978. [Google Scholar] [CrossRef]
- Dalavaye, N.; Erridge, S.; Nicholas, M.; Pillai, M.; Bapir, L.; Holvey, C.; Coomber, R.; Rucker, J.J.; Hoare, J.; Sodergren, M.H. The Effect of Medical Cannabis in Inflammatory Bowel Disease: Analysis from the UK Medical Cannabis Registry. Expert Rev. Gastroenterol. Hepatol. 2023, 17, 85–98. [Google Scholar] [CrossRef]
- Mucke, M.; Phillips, T.; Radbruch, L.; Petzke, F.; Hauser, W. Cannabis Based Medicines for Chronic Neuropathic Pain in Adults. Cochrane Database Syst. Rev. 2018, 3, CD012182. [Google Scholar] [CrossRef]
- Chung, M.; Kim, H.K.; Abdi, S. Update on Cannabis and Cannabinoids for Cancer Pain. Curr. Opin. Anaesthesiol. 2020, 33, 825–831. [Google Scholar] [CrossRef]
- ElSohly, M.A. Marijuana and the Cannabinoids; Humana: Totowa, NJ, USA, 2006. [Google Scholar]
- Demuth, D.G.; Molleman, A. Cannabinoid Signalling. Life Sci. 2006, 78, 549–563. [Google Scholar] [CrossRef]
- National Academies of Sciences, Engineering, and Medicine. The Health Effects of Cannabis and Cannabinoids: The Current State of Evidence and Recommendations for Research; National Academies Press (US): Washington, DC, USA, 2017. [Google Scholar]
- Babayeva, M.; Loewy, Z.G. Cannabis Pharmacogenomics: A Path to Personalized Medicine. Curr. Issues Mol. Biol. 2023, 45, 3479–3514. [Google Scholar] [CrossRef] [PubMed]
- Hryhorowicz, S.; Walczak, M.; Zakerska-Banaszak, O.; Słomski, R.; Skrzypczak-Zielińska, M. Pharmacogenetics of Cannabinoids. Eur. J. Drug Metab. Pharmacokinet. 2018, 43, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Delgado, D.A.; Lambert, B.S.; Boutris Nickolas and McCulloch, P.C.; Robbins, A.B.; Moreno Michael, R.; Harris, J.D. Validation of Digital Visual Analog Scale Pain Scoring With a Traditional Paper-Based Visual Analog Scale in Adults. JAAOS Glob. Res. Rev. 2018, 2, e088. [Google Scholar] [CrossRef] [PubMed]
- Poli, P.; Peruzzi, L.; Maurizi, P.; Mencucci, A.; Scocca, A.; Carnevale, S.; Spiga, O.; Santucci, A. The Pharmacogenetics of Cannabis in the Treatment of Chronic Pain. Genes 2022, 13, 1832. [Google Scholar] [CrossRef]
- Cilluffo, G.; Fasola, S.; Ferrante, G.; Malizia, V.; Montalbano, L. Machine Learning: An Overview and Applications in Pharmacogenetics. Genes 2021, 12, 1511. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Guestrin, C. XGBoost: A Scalable Tree Boosting System. In Proceedings of the 22nd ACM SIGKDD International Conference on Knowledge Discovery and Data Mining, San Francisco, CA, USA, 13–17 August 2016; Association for Computing Machinery: New York, NY, USA, 2016; p. 10. [Google Scholar]
- Romero-Sandoval, E.A.; Fincham, J.E.; Kolano, A.L.; Sharpe, B.N.; Alvarado-Vázquez, P.A. Cannabis for Chronic Pain: Challenges and Considerations. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2018, 38, 651–662. [Google Scholar] [CrossRef]
- Harris, M.; Erridge, S.; Ergisi, M.; Nimalan, D.; Kawka, M.; Salazar, O.; Ali, R.; Loupasaki, K.; Holvey, C.; Coomber, R.; et al. UK Medical Cannabis Registry: An Analysis of Clinical Outcomes of Medicinal Cannabis Therapy for Chronic Pain Conditions. Expert Rev. Clin. Pharmacol. 2022, 15, 473–485. [Google Scholar] [CrossRef]
- Blanton, H.L.; Barnes, R.C.; McHann, M.C.; Bilbrey, J.A.; Wilkerson, J.L.; Guindon, J. Sex Differences and the Endocannabinoid System in Pain. Pharmacol. Biochem. Behav. 2021, 202, 173107. [Google Scholar] [CrossRef]
- Fattore, L.; Fratta, W. How Important Are Sex Differences in Cannabinoid Action? Br. J. Pharmacol. 2010, 160, 544–548. [Google Scholar] [CrossRef]
- Nowell, W.B.; Gavigan, K.; Silverman, S.L. Cannabis for Rheumatic Disease Pain: A Review of Current Literature. Curr. Rheumatol. Rep. 2022, 24, 119–131. [Google Scholar] [CrossRef] [PubMed]
- Ortiz, Y.T.; McMahon, L.R.; Wilkerson, J.L. Medicinal Cannabis and Central Nervous System Disorders. Front. Pharmacol. 2022, 13, 881810. [Google Scholar] [CrossRef] [PubMed]
- Shah, R.M.; Saklecha, A.; Patel, A.A.; Divi, S.N. Analyzing the Impact of Cannabinoids on the Treatment of Spinal Disorders. Curr. Rev. Musculoskelet. Med. 2022, 15, 133–142. [Google Scholar] [CrossRef]
- Chayasirisobhon, S. Cannabis and Neuropsychiatric Disorders: An Updated Review. Acta Neurol Taiwan 2019, 28, 27–39. [Google Scholar]
- EI-Mallakh, R.S. Marijuana and Migraine. Headache J. Head Face Pain 1987, 27, 442–443. [Google Scholar] [CrossRef]
- Chen, Q.; Lin, W.; Yang, J.; Lin, M.; Lin, X.; Weng, Y.; Chen, Y. Prognostic Value of Two Polymorphisms, Rs1045642 and Rs1128503, in ABCB1 Following Taxane-Based Chemotherapy: A Meta-Analysis. Asian Pac. J. Cancer Prev. 2021, 22, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Rao, Q.; Lin, K.; He, Y.; Cai, J.; Yang, M.; Xu, Y.; Hou, L.; Lin, Y.; Liu, H. CYP2C19-Rs4986893 Confers Risk to Major Depressive Disorder and Bipolar Disorder in the Han Chinese Population Whereas ABCB1-Rs1045642 Acts as a Protective Factor. BMC Psychiatry 2023, 23, 69. [Google Scholar] [CrossRef]
- Benyamina, A.; Bonhomme-Faivre, L.; Picard, V.; Sabbagh, A.; Richard, D.; Blecha, L.; Rahioui, H.; Karila, L.; Lukasiewicz, M.; Farinotti, R.; et al. Association between ABCB1 C3435T Polymorphism and Increased Risk of Cannabis Dependence. Prog. Neuropsychopharmacol. Biol. Psychiatry 2009, 33, 1270–1274. [Google Scholar] [CrossRef]
- Aziz, M.A.; Islam, M.S. The Role of ABCB1 Gene Polymorphisms in Steroid-Resistant Nephrotic Syndrome: Evidence from a Meta-Analysis of Steroid-Receiving Patients. J. Gene Med. 2022, 24, e3436. [Google Scholar] [CrossRef]
- Tapanee, P.; Tidwell, D.K.; Schilling, M.W.; Peterson, D.G.; Tolar-Peterson, T. Genetic Variation in Taste Receptor Genes (SCNN1B, TRPV1) and Its Correlation with the Perception of Saltiness in Normotensive and Hypertensive Adults. Int. J. Hypertens 2021, 2021, 5559831. [Google Scholar] [CrossRef]
- Dias, A.G.; Rousseau, D.; Duizer, L.; Cockburn, M.; Chiu, W.; Nielsen, D.; El-Sohemy, A. Genetic Variation in Putative Salt Taste Receptors and Salt Taste Perception in Humans. Chem. Senses 2013, 38, 137–145. [Google Scholar] [CrossRef]
- Binder, A.; May, D.; Baron, R.; Maier, C.; Tölle, T.R.; Treede, R.-D.; Berthele, A.; Faltraco, F.; Flor, H.; Gierthmühlen, J.; et al. Transient Receptor Potential Channel Polymorphisms Are Associated with the Somatosensory Function in Neuropathic Pain Patients. PLoS ONE 2011, 6, e17387. [Google Scholar] [CrossRef] [PubMed]
- Tian, J.-N.; Ho, I.-K.; Tsou, H.-H.; Fang, C.-P.; Hsiao, C.-F.; Chen, C.-H.; Tan, H.K.-L.; Lin, L.; Wu, C.-S.; Su, L.-W.; et al. UGT2B7 Genetic Polymorphisms Are Associated with the Withdrawal Symptoms in Methadone Maintenance Patients. Pharmacogenomics 2012, 13, 879–888. [Google Scholar] [CrossRef] [PubMed]
- Verdejo-García, A.; Fagundo, A.B.; Cuenca, A.; Rodriguez, J.; Cuyás, E.; Langohr, K.; de Sola Llopis, S.; Civit, E.; Farré, M.; Peña-Casanova, J.; et al. COMT Val158met and 5-HTTLPR Genetic Polymorphisms Moderate Executive Control in Cannabis Users. Neuropsychopharmacology 2013, 38, 1598–1606. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, C.; Vieira-Coelho, M.A. Cannabis Induced Psychosis: A Systematic Review on the Role of Genetic Polymorphisms. Pharmacol. Res. 2022, 181, 106258. [Google Scholar] [CrossRef] [PubMed]
- Gerra, M.C.; Manfredini, M.; Cortese, E.; Antonioni, M.C.; Leonardi, C.; Magnelli, F.; Somaini, L.; Jayanthi, S.; Cadet, J.L.; Donnini, C. Genetic and Environmental Risk Factors for Cannabis Use: Preliminary Results for the Role of Parental Care Perception. Subst. Use Misuse 2019, 54, 670–680. [Google Scholar] [CrossRef]
- Wang, L.; Bai, M.; Jin, T.; Zheng, J.; Wang, Y.; He, Y.; Yuan, D.; He, X. Effects of CYP3A4 Polymorphisms on Drug Addiction Risk Among the Chinese Han Population. Front. Public Health 2019, 7, 315. [Google Scholar] [CrossRef]
- Chen, C.-H.; Wang, S.-C.; Tsou, H.-H.; Ho, I.-K.; Tian, J.-N.; Yu, C.-J.; Hsiao, C.-F.; Chou, S.-Y.; Lin, Y.-F.; Fang, K.-C.; et al. Genetic Polymorphisms in CYP3A4 Are Associated with Withdrawal Symptoms and Adverse Reactions in Methadone Maintenance Patients. Pharmacogenomics 2011, 12, 1397–1406. [Google Scholar] [CrossRef]
- Wang, D.; Sadee, W. CYP3A4 Intronic SNP Rs35599367 (CYP3A4*22) Alters RNA Splicing. Pharmacogenet. Genom. 2016, 26, 40–43. [Google Scholar] [CrossRef]
- Kitzmiller, J.; (Talameh) Luzum, J.; Baldassarre, D.; Krauss, R.; Medina, M. CYP3A4z.Ast22 and CYP3A5z.Ast3 Are Associated with Increased Levels of Plasma Simvastatin Concentrations in the Cholesterol and Pharmacogenetics Study Cohort. Pharmacogenet. Genom. 2014, 24, 486–491. [Google Scholar] [CrossRef]
- Hopfer, C.; Young, S.; Purcell, S.; Crowley, T.; Stallings, M.; Corley, R.; Rhee, S.; Smolen, A.; Krauter, K.; Hewitt, J.; et al. Cannabis Receptor Haplotype Associated With Fewer Cannabis Dependence Symptoms In Adolescents. Am. J. Med. Genet. B Neuropsychiatr. Genet. 2006, 141B, 895–901. [Google Scholar] [CrossRef]
- Zhang, P.-W.; Ishiguro, H.; Ohtsuki, T.; Hess, J.; Carillo, F.; Walther, D.; Onaivi, E.S.; Arinami, T.; Uhl, G.R. Human Cannabinoid Receptor 1: 5′ Exons, Candidate Regulatory Regions, Polymorphisms, Haplotypes and Association with Polysubstance Abuse. Mol. Psychiatry 2004, 9, 916–931. [Google Scholar] [CrossRef]
- Pabalan, N.; Chaweeborisuit, P.; Tharabenjasin, P.; Tasanarong, A.; Jarjanazi, H.; Eiamsitrakoon, T.; Tapanadechopone, P. Associations of CB1 Cannabinoid Receptor (CNR1) Gene Polymorphisms with Risk for Alcohol Dependence. Medicine 2021, 100, e27343. [Google Scholar] [CrossRef]
- Tyndale, R.; Payne, J.; Gerber, A.; Sipe, J. The Fatty Acid Amide Hydrolase C385A (P129T) Missense Variant in Cannabis Users: Studies of Drug Use and Dependence in Caucasians. Am. J. Med. Genet. B Neuropsychiatr. Genet. 2007, 144B, 660–666. [Google Scholar] [CrossRef] [PubMed]
- Hosseinzadeh Anvar, L.; Ahmadalipour, A. Fatty Acid Amide Hydrolase C385A Polymorphism Affects Susceptibility to Various Diseases. BioFactors 2023, 49, 62–78. [Google Scholar] [CrossRef] [PubMed]
- Myers, J.L.; Xia, H.; Caballero, M.Y.; Valtier, S.; Chaudry, G.J. A Military Community Cohort Study Reveals Single Nucleotide Polymorphisms in Inflammation Mediator Genes That Associate With Type 2 Diabetes. Mil. Med. 2022. online ahead of print. [Google Scholar] [CrossRef]
- Lucas, C.J.; Galettis, P.; Schneider, J. The Pharmacokinetics and the Pharmacodynamics of Cannabinoids. Br. J. Clin. Pharmacol. 2018, 84, 2477–2482. [Google Scholar] [CrossRef]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Visibelli, A.; Peruzzi, L.; Poli, P.; Scocca, A.; Carnevale, S.; Spiga, O.; Santucci, A. Supporting Machine Learning Model in the Treatment of Chronic Pain. Biomedicines 2023, 11, 1776. https://doi.org/10.3390/biomedicines11071776
Visibelli A, Peruzzi L, Poli P, Scocca A, Carnevale S, Spiga O, Santucci A. Supporting Machine Learning Model in the Treatment of Chronic Pain. Biomedicines. 2023; 11(7):1776. https://doi.org/10.3390/biomedicines11071776
Chicago/Turabian StyleVisibelli, Anna, Luana Peruzzi, Paolo Poli, Antonella Scocca, Simona Carnevale, Ottavia Spiga, and Annalisa Santucci. 2023. "Supporting Machine Learning Model in the Treatment of Chronic Pain" Biomedicines 11, no. 7: 1776. https://doi.org/10.3390/biomedicines11071776
APA StyleVisibelli, A., Peruzzi, L., Poli, P., Scocca, A., Carnevale, S., Spiga, O., & Santucci, A. (2023). Supporting Machine Learning Model in the Treatment of Chronic Pain. Biomedicines, 11(7), 1776. https://doi.org/10.3390/biomedicines11071776