
Diffuse, Adult-Onset Nesidioblastosis/Non-Insulinoma Pancreatogenous Hypoglycemia Syndrome (NIPHS): Review of the Literature of a Rare Cause of Hyperinsulinemic Hypoglycemia



 ,
,  ,
,
Abstract
1. Introduction
“…there is some evidence pointing to a diffuse or disseminated proliferation of islet cells as a possible cause of hypoglycemia. Such a diffuse proliferation of nesidioblasts would be a nesidioblastosis.”
2. Methodology of the Literature Research and Limitations
3. History, Histopathological, and Clinical Definition of Hyperinsulinemic Hypoglycemia and Nesidioblastosis/Islet Cell Hyperplasia
- (1)
- Evaluation of general hypoglycemia symptoms and their situational occurrence (i.e., postprandial, fasting, spontaneous, exercise-induced);
- (2)
- Results of a 4 h (–6 h) oral glucose tolerance test (OGTT);
- (3)
- Results of a 72 h fasting test;
- (4)
- Results of conventional imaging studies (CT, MRI);
- (5)
- Optional (might replace the next point in the future): results of functional imaging studies (where available, e.g., 68Ga-DOTA-Exendin-4 PET/CT or Somatostatin-receptor scintigraphy);
- (6)
- SACS with proof of an insulin gradient (might also be useful to define the extent of pancreatic resection if surgery is planned);
- (7)
- Exclusion of other conditions (e.g., Hirata´s disease, insulin secretagogues, etc.).
4. Nesidioblastosis and Islet Cell Hyperplasia in Other Adult Diseases
5. Etiology and Pathophysiology of NIPHS/Nesidioblastosis with Hyperinsulinism

6. Epidemiology
7. Symptoms
8. Clinical Diagnosis and Differential Diagnosis
9. Therapy
10. Conclusions and Future Perspectives
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cryer, P.E.; Axelrod, L.; Grossman, A.B.; Heller, S.R.; Montori, V.M.; Seaquist, E.R.; Service, F.J. Evaluation and Management of Adult Hypoglycemic Disorders: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2009, 94, 709–728. [Google Scholar] [CrossRef] [PubMed]
- Nadeau, A. Functional Hypoglycemia: Facts and Fancies. Can. Fam. Physician 1984, 30, 1333–1335. [Google Scholar] [PubMed]
- Gouta, E.L.; Jerraya, H.; Dougaz, W.; Chaouech, M.A.; Bouasker, I.; Nouira, R.; Dziri, C. Endogenous Hyperinsulinism: Diagnostic and Therapeutic Difficulties. Pan Afr. Med. J. 2019, 33, 57. [Google Scholar] [CrossRef] [PubMed]
- Okabayashi, T.; Shima, Y.; Sumiyoshi, T.; Kozuki, A.; Ito, S.; Ogawa, Y.; Kobayashi, M.; Hanazaki, K. Diagnosis and Management of Insulinoma. World J. Gastroenterol. 2013, 19, 829–837. [Google Scholar] [CrossRef]
- Yamada, Y.; Kitayama, K.; Oyachi, M.; Higuchi, S.; Kawakita, R.; Kanamori, Y.; Yorifuji, T. Nationwide Survey of Endogenous Hyperinsulinemic Hypoglycemia in Japan (2017–2018): Congenital Hyperinsulinism, Insulinoma, Non-Insulinoma Pancreatogenous Hypoglycemia Syndrome and Insulin Autoimmune Syndrome (Hirata’s Disease). J. Diabetes Investig. 2020, 11, 554–563. [Google Scholar] [CrossRef] [PubMed]
- Cappellani, D.; Macchia, E.; Falorni, A.; Marchetti, P. Insulin Autoimmune Syndrome (Hirata Disease): A Comprehensive Review Fifty Years after Its First Description. Diabetes Metab. Syndr. Obes. Targets Ther. 2020, 13, 963–978. [Google Scholar] [CrossRef]
- Service, G.J.; Thompson, G.B.; Service, F.J.; Andrews, J.C.; Collazo-Clavell, M.L.; Lloyd, R.V. Hyperinsulinemic Hypoglycemia with Nesidioblastosis after Gastric-Bypass Surgery. N. Engl. J. Med. 2005, 353, 249–254. [Google Scholar] [CrossRef]
- Dravecka, I.; Lazurova, I. Nesidioblastosis in Adults. Neoplasma 2014, 61, 252–256. [Google Scholar] [CrossRef]
- Laidlaw, G.F. Nesidioblastoma, the Islet Tumor of the Pancreas. Am. J. Pathol. 1938, 14, 125–134. [Google Scholar]
- Stanley, C.A. Perspective on the Genetics and Diagnosis of Congenital Hyperinsulinism Disorders. J. Clin. Endocrinol. Metab. 2016, 101, 815–826. [Google Scholar] [CrossRef]
- Anlauf, M.; Wieben, D.; Perren, A.; Sipos, B.; Komminoth, P.; Raffel, A.; Kruse, M.L.; Fottner, C.; Knoefel, W.T.; Mönig, H.; et al. Persistent Hyperinsulinemic Hypoglycemia in 15 Adults with Diffuse Nesidioblastosis: Diagnostic Criteria, Incidence, and Characterization of β-Cell Changes. Am. J. Surg. Pathol. 2005, 29, 524–533. [Google Scholar] [CrossRef] [PubMed]
- Klöppel, G.; Anlauf, M.; Raffel, A.; Perren, A.; Knoefel, W.T. Adult Diffuse Nesidioblastosis: Genetically or Environmentally Induced? Hum. Pathol. 2008, 39, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Karnauchow, P.N. Nesidioblastosis in Adults without Insular Hyperfunction. Am. J. Clin. Pathol. 1982, 78, 511–513. [Google Scholar] [CrossRef] [PubMed]
- Weidenheim, K.M.; Hinchey, W.W.; Campbell, W.G. Hyperinsulinemic Hypoglycemia in Adults with Islet-Cell Hyperplasia and Degranulation of Exocrine Cells of the Pancreas. Am. J. Clin. Pathol. 1983, 79, 14–24. [Google Scholar] [CrossRef]
- Fuller, P.J.; Ehrlich, A.R.; Susil, B.; Zeimer, H. Insulin Gene Expression in Adult-Onset Nesidioblastosis. Clin. Endocrinol. 1997, 47, 245–250. [Google Scholar] [CrossRef]
- Chen, Y.L.; Chu, J.S.; Chang, T.C.; Tai, T.Y. Nesidiodysplasia: An Unusual Cause of Hyperinsulinemic Hypoglycemia in Adults. J. Formos. Med. Assoc. 1993, 92, 1099–1103. [Google Scholar]
- Sandler, R.; Horwitz, D.L.; Rubenstein, A.H.; Kuzuya, H. Hypoglycemia and Endogenous Hyperinsulinism Complicating Diabetes Mellitus. Application of the C-Peptide Assay to Diagnosis and Therapy. Am. J. Med. 1975, 59, 730–736. [Google Scholar] [CrossRef]
- Weinstock, G.; Margulies, P.; Kahn, E.; Susin, M.; Abrams, G. Islet Cell Hyperplasia: An Unusual Cause of Hypoglycemia in an Adult. Metabolism 1986, 35, 110–117. [Google Scholar] [CrossRef]
- Gould, V.; Chejfec, G.; Shah, K.; Paloyan, E.; Lawrence, A.M. Adult Nesidiodysplasia. Semin. Diagn. Pathol. 1984, 1, 43–53. [Google Scholar]
- Vance, J.E.; Stoll, R.W.; Kitabchi, A.E.; Williams, R.H.; Wood, F.C. Nesidioblastosis in Familial Endocrine Adenomatosis. JAMA 1969, 207, 1679–1682. [Google Scholar] [CrossRef]
- Tavcar, I.; Andelković, Z.; Dragojević, R.; Duknić, M.; Ilić, S.; Novaković, O.; Tasić, G.; Lazić, R. Nesidioblastosis of the Pancreas as a Cause of Hyperinsulinemic Hypoglycemia in Adults. Vojnosanit. Pregl. 1994, 51, 73–81. [Google Scholar]
- Geoghegan, J.G.; Jackson, J.E.; Lewis, M.P.; Owen, E.R.; Bloom, S.R.; Lynn, J.A.; Williamson, R.C. Localization and Surgical Management of Insulinoma. Br. J. Surg. 1994, 81, 1025–1028. [Google Scholar] [CrossRef] [PubMed]
- Losada, J.; Sarria, R.; Fernandez Val, J.; Lopez Ariztegui, M. DNA Ploidy and PCNA Index in Pancreatic Lesions Producing Hyperinsulinemic Hypoglycemia. J. Surg. Oncol. 1995, 59, 14–17. [Google Scholar] [CrossRef] [PubMed]
- Farley, D.R.; van Heerden, J.A.; Myers, J.L. Adult Pancreatic Nesidioblastosis: Unusual Presentations of a Rare Entity. Arch. Surg. 1994, 129, 329–332. [Google Scholar] [CrossRef]
- Lechleitner, M.; Hoppichler, F.; Dzien, A.; Feichtinger, H.; Bodner, E.; Patsch, J. Nesidioblastosis in a Young Woman and the Impact of Hyperinsulinaemia on Triglyceride Metabolism. J. Intern. Med. 1995, 237, 117–118. [Google Scholar] [CrossRef]
- Walmsley, D.; Matheson, N.A.; Ewen, S.; Himsworth, R.L.; Bevan, J.S. Nesidioblastosis in an Elderly Patient. Diabet. Med. 1995, 12, 542–545. [Google Scholar] [CrossRef]
- Bell, D.S.; Grizzle, W.E.; Dunlap, E.D. Nesidioblastosis Causing Reversal of Insulin-Dependent Diabetes and Development of Hyperinsulinemic Hypoglycemia. Diabetes Care 1995, 18, 1379–1380. [Google Scholar] [CrossRef]
- Le Bodic, M.F.; Heymann, M.F.; Lecomte, M.; Berger, N.; Berger, F.; Louvel, A.; De Micco, C.; Patey, M.; De Mascarel, A.; Burtin, F.; et al. Immunohistochemical Study of 100 Pancreatic Tumors in 28 Patients with Multiple Endocrine Neoplasia, Type I. Am. J. Surg. Pathol. 1996, 20, 1378–1384. [Google Scholar] [CrossRef]
- Galizia, A.C.; Fava, S.; Foale, R. Nesidioblastosis-Associated Hypoglycaemia Presenting with Prominent Cardiac Manifestations. Postgrad. Med. J. 1996, 72, 231–232. [Google Scholar] [CrossRef][Green Version]
- Kim, H.K.; Shong, Y.K.; Han, D.J.; Cho, Y.; Lee, I.C.; Kim, G.S. Nesidioblastosis in an Adult with Hyperinsulinemic Hypoglycemia. Endocr. J. 1996, 43, 163–167. [Google Scholar] [CrossRef][Green Version]
- Frantz, V.K. Adenomatosis of Islet Cells, with Hyperinsulinism. Ann. Surg. 1944, 119, 824–844. [Google Scholar] [CrossRef]
- Martella, E.M.; Ferraro, G.; Azzoni, C.; Marignani, M.; Bordi, C. Pancreatic-Polypeptide Cell Hyperplasia Associated with Pancreatic or Duodenal Gastrinomas. Hum. Pathol. 1997, 28, 149–153. [Google Scholar] [CrossRef]
- Garcia, J.P.; Franca, T.; Pedroso, C.; Cardoso, C.; Cid, M.O. Nesidioblastosis in the Adult Surgical Management. HPB Surg. 1997, 10, 201–209. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Lee, W.L.; Won, J.G.; Chiang, J.H.; Hwang, J.I.; Lee, C.H.; Tsay, S.H. Selective Intra-Arterial Calcium Injection in the Investigation of Adult Nesidioblastosis: A Case Report. Diabet. Med. 1997, 14, 985–988. [Google Scholar] [CrossRef]
- Röher, H.D.; Simon, D.; Starke, A.; Goretzki, P.E. Spezielle Diagnostische Und Therapeutische Aspekte Beim Insulinom. Chirurg 1997, 68, 116–121. [Google Scholar] [CrossRef]
- Sanjuán Portugal, F.; Trincado Aznar, P.; Acha Pérez, J.; Velilla Marco, J. Diagnosis of Nesidioblastosis in the Adult. An. Med. Interna 1997, 14, 101. [Google Scholar] [PubMed]
- Conget, I.; Sarri, Y.; Somoza, N.; Vives, M.; Novials, A.; Ariza, A.; Fernández-Alvarez, J.; Pujol-Borrell, R.; Gomis, R. β-Cell Function Abnormalities in Islets from an Adult Subject with Nesidioblastosis and Autoantibodies against the Islet Cells. Pancreas 1997, 14, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.; Kristopaitis, T.; Yong, S.; Chejfec, G.; Pickleman, J. Cystic Glucagonoma: A Rare Variant of an Uncommon Neuroendocrine Pancreas Tumor. J. Gastrointest. Surg. 1998, 2, 533–536. [Google Scholar] [CrossRef]
- Ueda, Y.; Kurihara, K.; Kondoh, T.; Okanoue, T.; Chiba, T. Islet-Cell Hyperplasia Causing Hyperinsulinemic Hypoglycemia in an Adult. J. Gastroenterol. 1998, 33, 125–128. [Google Scholar] [CrossRef]
- Soga, J.; Yakuwa, Y.; Osaka, M. Insulinoma/Hypoglycemic Syndrome: A Statistical Evaluation of 1085 Reported Cases of a Japanese Series. J. Exp. Clin. Cancer Res. 1998, 17, 379–388. [Google Scholar]
- Pereira, P.L.; Roche, A.J.; Maier, G.W.; Huppert, P.E.; Dammann, F.; Farnsworth, C.T.; Duda, S.H.; Claussen, C.D. Insulinoma and Islet Cell Hyperplasia: Value of the Calcium Intraarterial Stimulation Test When Findings of Other Preoperative Studies Are Negative. Radiology 1998, 206, 703–709. [Google Scholar] [CrossRef] [PubMed]
- Franksson, C.; Hellstrom, J.; Hultquist, G.; Perman, G. Primary Chief-Cell Hyperplasia of the Parathyroids, and Islet Cell Hyperplasia and Adenomata of the Pancreas Associated with Gastro-Duodeno-Jejunal Ulcer. Acta Chir. Scand. 1960, 118, 270–277. [Google Scholar] [PubMed]
- Rinker, R.D.; Friday, K.; Aydin, F.; Jaffe, B.M.; Lambiase, L. Adult Nesidioblastosis: A Case Report and Review of the Literature. Dig. Dis. Sci. 1998, 43, 1784–1790. [Google Scholar] [CrossRef]
- Pasieka, J.L.; Hershfield, N. Pancreatic Polypeptide Hyperplasia Causing Watery Diarrhea Syndrome: A Case Report. Can. J. Surg. 1999, 42, 55–58. [Google Scholar] [PubMed]
- Service, F.J.; Natt, N.; Thompson, G.B.; Grant, C.S.; Van Heerden, J.A.; Andrews, J.C.; Lorenz, E.; Terzic, A.; Lloyd, R.V. Noninsulinoma Pancreatogenous Hypoglycemia: A Novel Syndrome of Hyperinsulinemic Hypoglycemia in Adults Independent of Mutations in Kir6.2 and SUR1 Genes. J. Clin. Endocrinol. Metab. 1999, 84, 1582–1589. [Google Scholar] [CrossRef]
- Eriguchi, N.; Aoyagi, S.; Hara, M.; Tanaka, E.; Hashimoto, M.; Jimi, A. Nesidioblastosis with Hyperinsulinemic Hypoglycemia in Adults: Report of Two Cases. Surg. Today 1999, 29, 361–363. [Google Scholar] [CrossRef]
- Wängberg, B.; Nilsson, O.; Grimelius, L.; Lundell, L.; Ahlman, H. Nesidiodysplasia. A Rare Cause of Hyperinsulinemia in an Adult Patient. Lakartidningen 1999, 96, 4655–4657. [Google Scholar]
- Tomaszewska, R.; Nowak, W.; Rudnicka-Sosin, L.; Stachura, J. Nesidioblastosis in an Adult Man—Case Report. Pol. J. Pathol. 1999, 50, 43–46. [Google Scholar]
- Yeh, S.P.; Wang, Y.C.; Wu, H.; Yu, M.S.; Hsueh, E.J.; Wang, Y.C. Nesidioblastosis, Myelodysplastic Syndrome and Nodular Diabetic Glomerulosclerosis in an Elderly Nondiabetic Woman: An Autopsy Report. Diabet. Med. 1999, 16, 437–441. [Google Scholar] [CrossRef]
- Hashimoto, L.A.; Walsh, R.M. Preoperative Localization of Insulinomas Is Not Necessary. J. Am. Coll. Surg. 1999, 189, 368–373. [Google Scholar] [CrossRef]
- Habanec, B.; Růzicka, M.; Dvorák, K.; Stracár, K.; Tretinová, L. Pathology of the Pancreas. Analysis of 172 Resection Specimens. Cesk. Patol. 1999, 35, 39–44. [Google Scholar] [PubMed]
- Thompson, G.B.; Service, F.J.; Andrews, J.C.; Lloyd, R.V.; Natt, N.; Van Heerden, J.A.; Grant, C.S. Noninsulinoma Pancreatogenous Hypoglycemia Syndrome: An Update in 10 Surgically Treated Patients. Surgery 2000, 128, 937–945. [Google Scholar] [CrossRef] [PubMed]
- Bloodworth, J.M.B. Morphologic Changes Associated with Sulfonylurea Therapy. Metabolism 1963, 12, 287–301. [Google Scholar]
- Kim, Y.W.; Park, Y.-K.; Park, J.H.; Lee, S.M.; Lee, J.; Ko, S.W.; Yang, M.H. Islet Cell Hyperplasia of the Pnacreas Presenting as Hyperinsulinemic Hypoglycemia in an Adult. Yonsei Med. J. 2000, 41, 426–429. [Google Scholar] [CrossRef] [PubMed]
- Van der Wal, B.C.H.; De Krijger, R.R.; De Herder, W.W.; Kwekkeboom, D.J.; Van der Ham, F.; Bonjer, H.J.; Van Eijck, C.H.J. Adult Hyperinsulinemic Hypoglycemia Not Caused by an Insulinoma: A Report of Two Cases. Virchows Arch. 2000, 436, 481–486. [Google Scholar] [CrossRef]
- White, S.A.; Sutton, C.D.; Robertson, G.S.; Furness, P.N.; Dennison, A.R. Incidental Adult Nesidioblastosis after Distal Pancreatectomy for Endocrine Microadenoma. Eur. J. Gastroenterol. Hepatol. 2000, 12, 1147–1149. [Google Scholar] [CrossRef] [PubMed]
- Kon, Y.C.; Loh, K.C.; Chew, S.P.; Wong, D.; Yap, W.M.; Lee, Y.S.; Low, C.H. Hypoglycaemia from Islet Cell Hyperplasia and Nesidioblastosis in a Patient with Type 2 Diabetes Mellitus—A Case Report. Ann. Acad. Med. Singapore 2000, 29, 682–687. [Google Scholar]
- Hellman, P.; Goretzki, P.; Simon, D.; Dotzenrath, C.; Roher, H.D. Therapeutic Experience of 65 Cases with Organic Hyperinsulinism. Langenbeck’s Arch. Surg. 2000, 385, 329–336. [Google Scholar] [CrossRef]
- Lecube, A.; Obiols, G.; Ramos, I.; Gémar, E. Hyperinsulinemic Hypoglycemia and Nesidioblastosis in Adults. An Exceptional Disease. Med. Clin. 2001, 116, 238–239. [Google Scholar] [CrossRef]
- Culberson, D.; Manci, E.; Shah, A.; Haynes, J.; Ballas, S.; Pegelow, C.; Vichinsky, E. Nesidioblastosis in Sickle Cell Disease. Pediatr. Pathol. Mol. Med. 2001, 20, 155–165. [Google Scholar] [CrossRef]
- Zhao, X.; Stabile, B.E.; Mo, J.; Wang, J.; French, S.W. Nesidioblastosis Coexisting with Islet Cell Tumor and Intraductal Papillary Mucinous Hyperplasia. Arch. Pathol. Lab. Med. 2001, 125, 1344–1347. [Google Scholar] [CrossRef] [PubMed]
- Sumarac-Dumanovic, M.; Micic, D.; Popovic, V. Noninsulinoma Pancreatogenous Hypoglycemia in Adults: Presentations of Two Cases. J. Clin. Endocrinol. Metab. 2001, 86, 2328–2329. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Witteles, R.M.; Straus, F.H.; Sugg, S.L.; Koka, M.R.; Costa, E.A.; Kaplan, E.L. Adult-Onset Nesidioblastosis Causing Hypoglycemia. Arch. Surg. 2001, 136, 656–663. [Google Scholar] [CrossRef] [PubMed]
- Zollinger, R.M. Zollinger-Ellison Syndrome: Re-Appraisal and Evaluation of 260 Registered Cases. Ann. Surg. 1964, 160, 512–528. [Google Scholar]
- Govindarajan, M.; Mohan, V.; Deepa, R.; Ashok, S.; Pitchumoni, C.S. Histopathology and Immunohistochemistry of Pancreatic Islets in Fibrocalculous Pancreatic Diabetes. Diabetes Res. Clin. Pract. 2001, 51, 29–38. [Google Scholar] [CrossRef]
- Espinosa-de-los-Monteros, A.; Robledo, F.; Cabrera, L.; Mercado, M. Nesidioblastosis as Extracolonic Manifestation Associated with Adenomatous Familial Polyposis. Rev. Gastroenterol. Mex. 2001, 66, 46–49. [Google Scholar]
- Semakula, C.; Pambuccian, S.; Gruessner, R.; Kendall, D.; Pittenger, G.; Vinik, A.; Seaquist, E.R. Hypoglycemia after Pancreas Transplantation: Association with Allograft Nesidiodysplasia and Expression of Islet Neogenesis-Associated Peptide. J. Clin. Endocrinol. Metab. 2002, 87, 3548–3554. [Google Scholar] [CrossRef]
- Matthews, B.; Smith, T.; Kercher, K.; Holder, W.; Heniford, B. Surgical Experience with Functioning Pancreatic Neuroendocrine Tumors. Am. Surg. 2002, 68, 660–665. [Google Scholar] [CrossRef]
- Carneiro, D.M.; Levi, J.U.; Irvin, G.L. Rapid Insulin Assay for Intraoperative Confirmation of Complete Resection of Insulinomas. Surgery 2002, 132, 937–943. [Google Scholar] [CrossRef]
- Lu, J.Y.; Huang, T.S.; Wu, M.Z. Hypopituitarism and Nesidioblastosis in an Elderly Patient with Orbital Lymphoma. J. Formos. Med. Assoc. 2002, 101, 68–72. [Google Scholar]
- Kaczirek, K.; Soleiman, A.; Schindl, M.; Passler, C.; Scheuba, C.; Prager, G.; Kaserer, K.; Niederle, B. Nesidioblastosis in Adults: A Challenging Cause of Organic Hyperinsulinism. Eur. J. Clin. Investig. 2003, 33, 488–492. [Google Scholar] [CrossRef] [PubMed]
- Vella, A.; Service, F.J.; O’Brien, P.C. Glucose Counterregulatory Hormones in the 72-Hour Fast. Endocr. Pract. 2003, 9, 115–118. [Google Scholar] [CrossRef]
- Branco, V.A.; Santos, R.M.; Cipriano, M.A.; Tralhão, G.; Otero, M.; Moura, J.A.; Sousa, F.C.; Porto, A. Adult Nesidioblastosis. Acta Med. Port. 2003, 16, 465–470. [Google Scholar] [PubMed]
- Martignoni, M.E.; Kated, H.; Stiegler, M.; Büchler, M.W.; Friess, H.; Zimmermann, A.; Schirp, U.; Nitzsche, E.U. Nesidioblastosis with Glucagon-Reactive Islet Cell Hyperplasia: A Case Report. Pancreas 2003, 26, 402–405. [Google Scholar] [CrossRef]
- Knight, P.O. Insulinoma and Generalized Islet Cell Hyperplasia in a Patient with Diabetes Mellitus. South. Med. J. 1967, 60, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Giorgadze, T.A.; Roy, S.; Fraker, D.L.; Brooks, J.S.J.; LiVolsi, V.A. Pathologic Quiz Case: A 49-Year-Old Woman with an Adrenal Mass. Arch. Pathol. Lab. Med. 2004, 128, 1294–1296. [Google Scholar] [CrossRef]
- Ito, K.; Takada, T.; Amano, H.; Toyota, N.; Yasuda, H.; Yoshida, M.; Takada, Y.; Takeshita, K.; Koutake, H.; Takada, K.; et al. Localization of Islet-Cell Hyperplasia: Value of Pre- and Intraoperative Arterial Stimulation and Venous Sampling. J. Hepatobiliary. Pancreat. Surg. 2004, 11, 203–206. [Google Scholar] [CrossRef]
- Wiesli, P.; Brändle, M.; Schmid, C.; Krähenbühl, L.; Furrer, J.; Keller, U.; Spinas, G.A.; Pfammatter, T. Selective Arterial Calcium Stimulation and Hepatic Venous Sampling in the Evaluation of Hyperinsulinemic Hypoglycemia: Potential and Limitations. J. Vasc. Interv. Radiol. 2004, 15, 1251–1256. [Google Scholar] [CrossRef]
- Wiesli, P.; Perren, A.; Saremaslani, P.; Pfammatter, T.; Spinas, G.A.; Schmid, C. Abnormalities of Proinsulin Processing in Functioning Insulinomas: Clinical Implications. Clin. Endocrinol. 2004, 61, 424–430. [Google Scholar] [CrossRef]
- Proye, C.; Stalnikiewicz, G.; Wemeau, J.L.; Porchet, N.; D’Herbomez, M.; Maunoury, V.; Bauters, C. Genetically-Driven or Supposed Genetic-Related Insulinomas in Adults: Validation of the Surgical Strategy Proposed by the A.F.C.E./G.E.N.E.M. Ann. Endocrinol. 2004, 65, 149–161. [Google Scholar] [CrossRef]
- Kaczirek, K.; Ba-Ssalamah, A.; Schima, W.; Niederle, B. The Importance of Preoperative Localisation Procedures in Organic Hyperinsulinism--Experience in 67 Patients. Wien. Klin. Wochenschr. 2004, 116, 373–378. [Google Scholar] [CrossRef] [PubMed]
- Boulanger, C.; Vezzosi, D.; Bennet, A.; Lorenzini, F.; Fauvel, J.; Caron, P. Normal Pregnancy in a Woman with Nesidioblastosis Treated with Somatostatin Analog Octreotide. J. Endocrinol. Investig. 2004, 27, 465–470. [Google Scholar] [CrossRef] [PubMed]
- Chetty, R.; Kennedy, M.; Ezzat, S.; Asa, S.L. Pancreatic Endocrine Pathology in von Hippel-Lindau Disease: An Expanding Spectrum of Lesions. Endocr. Pathol. 2004, 15, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Patti, M.E.; McMahon, G.; Mun, E.C.; Bitton, A.; Holst, J.J.; Goldsmith, J.; Hanto, D.W.; Callery, M.; Arky, R.; Nose, V.; et al. Severe Hypoglycaemia Post-Gastric Bypass Requiring Partial Pancreatectomy: Evidence for Inappropriate Insulin Secretion and Pancreatic Islet Hyperplasia. Diabetologia 2005, 48, 2236–2240. [Google Scholar] [CrossRef]
- Pedrazzoli, S.; Pasquali, C.; D’Andrea, A.A. Surgical Treatment of Insulinoma. Br. J. Surg. 2005, 81, 672–676. [Google Scholar] [CrossRef]
- Cavallero, C.; Solcia, E.; Sampietro, R. Cytology of Islet Tumours and Hyperplasias Associated with the Zollinger-Ellison Syndrome. Gut 1967, 8, 172–177. [Google Scholar] [CrossRef]
- Babińska, A.; Jaśkiewicz, K.; Karaszewski, B.; Łukiański, M.; Sworczak, K. Nesidioblastosis—A Rare Cause of Hypoglycaemia in Adults. Exp. Clin. Endocrinol. Diabetes 2005, 113, 350–353. [Google Scholar] [CrossRef]
- Rare Presentation of Endocrine Pancreatic Tumor: A Case of Diffuse Glucagonoma without Metastasis and Necrolytic Migratory Erythema—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/15959605/ (accessed on 7 October 2021).
- Tsujino, M.; Sugiyama, T.; Nishida, K.; Takada, Y.; Takanishi, K.; Ishizawa, M.; Hirata, Y. Noninsulinoma Pancreatogenous Hypoglycemia Syndrome: A Rare Case of Adult-Onset Nesidioblastosis. Intern. Med. 2005, 44, 843–847. [Google Scholar] [CrossRef][Green Version]
- Kondo, T.; Tomita, S.; Adachi, H.; Motoshima, H.; Taketa, K.; Matsuyoshi, A.; Tokunaga, H.; Miyamura, N.; Araki, E. A Case of Hyperinsulinemia of Undetermined Origin, Successfully Treated with Long-Acting Octreotide. Endocr. J. 2005, 52, 511–517. [Google Scholar] [CrossRef][Green Version]
- Won, J.G.S.; Tseng, H.S.; Yang, A.H.; Tang, K.T.; Jap, T.S.; Lee, C.H.; Da Lin, H.; Burcus, N.; Pittenger, G.; Vinik, A. Clinical Features and Morphological Characterization of 10 Patients with Noninsulinoma Pancreatogenous Hypoglycaemia Syndrome (NIPHS). Clin. Endocrinol. 2006, 65, 566–578. [Google Scholar] [CrossRef]
- Diaz, A.; Lucas, S.; Ferraina, P.; Ferraro, A.; Puchulu, F.; Paes De Lima, A.; Maselli Mdel, C.; Gomez, R.; Bruno, O. Clinical Experience in 37 Cases of Insulinoma. Medicina 2006, 66, 499–504. [Google Scholar]
- Raffel, A.; Krausch, M.M.; Anlauf, M.; Wieben, D.; Braunstein, S.; Klöppel, G.; Röher, H.D.; Knoefel, W.T. Diffuse Nesidioblastosis as a Cause of Hyperinsulinemic Hypoglycemia in Adults: A Diagnostic and Therapeutic Challenge. Surgery 2007, 141, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Starke, A.; Saddig, C.; Kirch, B.; Tschahargane, C.; Goretzki, P. Islet Hyperplasia in Adults: Challenge to Preoperatively Diagnose Non-Insulinoma Pancreatogenic Hypoglycemia Syndrome. World J. Surg. 2006, 30, 670–679. [Google Scholar] [CrossRef] [PubMed]
- Meier, J.J.J.; Butler, A.A.E.; Galasso, R.; Butler, P.P.C. Hyperinsulinemic Hypoglycemia after Gastric Bypass Surgery Is Not Accompanied by Islet Hyperplasia or Increased β-Cell Turnover. Diabetes Care 2006, 29, 1554–1559. [Google Scholar] [CrossRef]
- Ouyang, D.; Dhall, D.; Yu, R. Pathologic Pancreatic Endocrine Cell Hyperplasia. World J. Gastroenterol. 2011, 17, 137–143. [Google Scholar] [CrossRef]
- Wiesli, P.; Pavlicek, V.; Perren, A.; Baechli, E.; Pfammatter, T.; Krahenbuhl, L.; Schulthess, G.; Schmid, C. Recurrent Hypoglycaemia in HIV-Positive Narcotic Addicts. Swiss Med. Wkly. 2006, 136, 805–810. [Google Scholar]
- Arao, T.; Okada, Y.; Hirose, A.; Tanaka, Y. A Rare Case of Adult-Onset Nesidioblastosis Treated Successfully with Diazoxide. Endocr. J. 2006, 53, 95–100. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Clancy, T.E.; Moore, F.D.; Zinner, M.J.; TE, C.; FD, M.; MJ, Z. Post−Gastric Bypass Hyperinsulinism With Nesidioblastosis: Subtotal or Total Pancreatectomy May Be Needed to Prevent Recurrent Hypoglycemia. J. Gastrointest. Surg. 2006, 10, 1116–1119. [Google Scholar] [CrossRef]
- Albazaz, R.; Da Costa, P.E.; Verbeke, C.S. Pancreatic Polypeptide Cell Hyperplasia of the Pancreas. J. Clin. Pathol. 2006, 59, 1087–1090. [Google Scholar] [CrossRef]
- Raffel, A.; Anlauf, M.; Hosch, S.B.; Krausch, M.; Henopp, T.; Bauersfeld, J.; Klofat, R.; Bach, D.; Eisenberger, C.F.; Klöppel, G.; et al. Hyperinsulinemic Hypoglycemia Due to Adult Nesidioblastosis in Insulin-Dependent Diabetes. World J. Gastroenterol. 2006, 12, 7221–7224. [Google Scholar] [CrossRef]
- Nakagawa, A.; Ueno, K.; Ito, M.; Okamoto, S.; Uehara, K.; Ito, H.; Mishina, S.; Kinoshita, E.; Nojima, T.; Takahashi, H.; et al. Insulin Responses to Selective Arterial Calcium Infusion under Hyperinsulinemic Euglycemic Glucose Clamps: Case Studies in Adult Nesidioblastosis and Childhood Insulinoma. Endocr. J. 2007, 54, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, G.C.; Faria, E.N.; Beck, M.; Girardon, D.T.; Machado, A.C. Laparoscopic Spleen-Preserving Distal Pancreatectomy as Treatment for Nesidioblastosis after Gastric Bypass Surgery. Obes. Surg. 2007, 17, 550–552. [Google Scholar] [CrossRef] [PubMed]
- Tseng, L.M.; Chen, J.Y.; Won, J.G.S.; Tseng, H.S.; Yang, A.H.; Wang, S.E.; Lee, C.H. The Role of Intra-Arterial Calcium Stimulation Test with Hepatic Venous Sampling (IACS) in the Management of Occult Insulinomas. Ann. Surg. Oncol. 2007, 14, 2121–2127. [Google Scholar] [CrossRef] [PubMed]
- Bantle, J.P.; Ikramuddin, S.; Kellogg, T.A.; Buchwald, H. Hyperinsulinemic Hypoglycemia Developing Late after Gastric Bypass. Obes. Surg. 2007, 17, 592–594. [Google Scholar] [CrossRef] [PubMed]
- Sahloul, R.; Yaqub, N.; Driscoll, H.K.; Leidy, J.W.; Parkash, J.; Matthews, K.A.; Chertow, B.S. Noninsulinoma Pancreatogenous Hypoglycemia Syndrome: Quantitative and Immunohistochemical Analyses of Islet Cells for Insulin, Glucagon, Somatostatin, and Pancreatic and Duodenal Homeobox Protein. Endocr. Pract. 2007, 13, 187–193. [Google Scholar] [CrossRef]
- Brown, R.; Still, W. Nesidioblastosis and the Zollinger-Ellison Syndrome. Am. J. Dig. Dis. 1968, 13, 656–663. [Google Scholar] [CrossRef]
- Costa, R.; Maia, F.; Araújo, L. Endogenous Persistent Hypoglicemia of Adult: Case Report. Arq. Bras. Endocrinol. Metabol. 2007, 51, 125–130. [Google Scholar] [CrossRef]
- Rosman, J.; Bravo-Vera, R.; Sheikh, A.; Gouller, A. Metastatic Insulinoma in an Adult Patient with Underlying Nesidioblastosis. J. Endocrinol. Investig. 2007, 30, 521–524. [Google Scholar] [CrossRef]
- Kok, V.K.; Wang, T.K.; Lin, N.H.; Bei, J.J.; Huang, P.H.; Chen, Y.C. Adult Intussusception Caused by Heterotopic Pancreas. J. Formos. Med. Assoc. 2007, 106, 418–421. [Google Scholar] [CrossRef]
- Kauhanen, S.; Seppänen, M.; Minn, H.; Gullichsen, R.; Salonen, A.; Alanen, K.; Parkkola, R.; Solin, O.; Bergman, J.; Sane, T.; et al. Fluorine-18-L-Dihydroxyphenylalanine (18F-DOPA) Positron Emission Tomography as a Tool to Localize an Insulinoma or β-Cell Hyperplasia in Adult Patients. J. Clin. Endocrinol. Metab. 2007, 92, 1237–1244. [Google Scholar] [CrossRef]
- Vezzosi, D.; Bennet, A.; Fauvel, J.; Caron, P. Insulin, C-Peptide and Proinsulin for the Biochemical Diagnosis of Hypoglycaemia Related to Endogenous Hyperinsulinism. Eur. J. Endocrinol. 2007, 157, 75–83. [Google Scholar] [CrossRef]
- Bunning, J.; Merchant, S.H.; Crooks, L.A.; Hartshorne, M.F. Indium-111 Pentetreotide Uptake by Pancreatic Polypeptide Cell Hyperplasia: Potential Pitfall in Somatostatin Receptor Scintigraphy. Pancreas 2007, 35, 372–375. [Google Scholar] [CrossRef] [PubMed]
- Hong, R.; Choi, D.; Lim, S. Hyperinsulinemic Hypoglycemia Due to Diffuse Nesidioblastosis in Adults: A Case Report. World J. Gastroenterol. 2008, 14, 140–142. [Google Scholar] [CrossRef] [PubMed]
- Yu, R.; Nissen, N.N.; Dhall, Þ.D.; Heaney, A.P. Nesidioblastosis and Hyperplasia of Alpha Cells, Microglucagonoma, and Nonfunctioning Islet Cell Tumor of the Pancreas. Pancreas 2008, 36, 428–431. [Google Scholar] [CrossRef] [PubMed]
- Moreira, R.O.; Moreira, R.B.M.; Machado, N.A.M.; Gonçalves, T.B.; Coutinho, W.F. Post-Prandial Hypoglycemia after Bariatric Surgery: Pharmacological Treatment with Verapamil and Acarbose. Obes. Surg. 2008, 18, 1618–1621. [Google Scholar] [CrossRef] [PubMed]
- Kovács, E.; Németh, H.; Pásztor, E.; Pfliegler, G. Hyperinsulinemic Hypoglycemia in Adults. Case Reports and a Short Review. Orv. Hetil. 2008, 149, 1659–1664. [Google Scholar] [CrossRef] [PubMed]
- Sircus, W.; Brunt, P.W.; Walker, R.J.; Small, W.P.; Falconer, C.W.; Thomson, C.G. Two Cases of “Pancreatic Cholera” with Features of Peptide-Secreting Adenomatosis of the Pancreas. Gut 1970, 11, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Abellán, P.; Cámara, R.; Merino-Torres, J.F.; Pérez-Lazaro, A.; del Olmo, M.I.; Ponce, J.L.; Rayón, J.M.; Piñón, F. Severe Hypoglycemia after Gastric Bypass Surgery for Morbid Obesity. Diabetes Res. Clin. Pract. 2008, 79, 2007–2009. [Google Scholar] [CrossRef]
- Kellogg, T.A.; Bantle, J.P.; Leslie, D.B.; Redmond, J.B.; Slusarek, B.; Swan, T.; Buchwald, H.; Ikramuddin, S. Postgastric Bypass Hyperinsulinemic Hypoglycemia Syndrome: Characterization and Response to a Modified Diet. Surg. Obes. Relat. Dis. 2008, 4, 492–499. [Google Scholar] [CrossRef]
- Dissanayake, A.S.; Jones, V.; Fernando, D.J.S. Adult Hyperinsulinaemic Hypoglycaemia Caused by Coexisting Nesidioblastosis and Insulinoma. Eur. J. Intern. Med. 2008, 19, 303–306. [Google Scholar] [CrossRef]
- Z’graggen, K.; Guweidhi, A.; Steffen, R.; Potoczna, N.; Biral, R.; Walther, F.; Komminoth, P.; Horber, F. Severe Recurrent Hypoglycemia after Gastric Bypass Surgery. Obes. Surg. 2008, 18, 981–988. [Google Scholar] [CrossRef] [PubMed]
- Karawagh, A.; Abdullah, L.; Gasim, A.; Abdelaziz, M. Noninsulinoma Pancreatogenous Hypoglycemia Syndrome in a Saudi Male. Saudi Med. J. 2008, 29, 1654–1657. [Google Scholar] [PubMed]
- Barbour, J.; Thomas, B.; Morgan, K.; Byrne, T.; Adams, D. The Practice of Pancreatic Resection after Roux-En-Y Gastric Bypass. Am. Surg. 2008, 74, 729–734. [Google Scholar] [CrossRef] [PubMed]
- Kenney, B.; Tormey, C.A.; Qin, L.; Sosa, J.A.; Jain, D.; Neto, A. Adult Nesidioblastosis. Clinicopathologic Correlation between Pre-Operative Selective Arterial Calcium Stimulation Studies and Post-Operative Pathologic Findings. J. Pancreas 2008, 9, 504–511. [Google Scholar]
- Geraghty, M.; Draman, M.; Moran, D.; Muldoon, C.; Reynolds, J.; Cullen, M. Hypoglycaemia in an Adult Male: A Surprising Finding in Pursuit of Insulinoma. Surgeon 2008, 6, 57–60. [Google Scholar] [CrossRef] [PubMed]
- Catton, J.A.; Zaitoun, A.M.; Aithal, G.P.; Sturrock, N.D.C.; Lobo, D.N. Diffuse Nesidioblastosis Causing Hyperinsulinemic Hypoglycemia: The Importance of Pancreatic Sampling on EUS. Gastrointest. Endosc. 2008, 68, 571–572. [Google Scholar] [CrossRef] [PubMed]
- Jabri, A.L.; Bayard, C. Nesidioblastosis Associated with Hyperinsulinemic Hypoglycemia in Adults: Review of the Literature. Eur. J. Intern. Med. 2004, 15, 407–410. [Google Scholar] [CrossRef]
- Wig, J.; Nayak, N.; Kumar, S.; Buxi, T.; Nundy, S.; Mittal, K.; Gupta, P. A 20-Year-Old Man with Recurrent Abdominal Pain and Vomiting since the Age of 5 Years. Familial Chronic Pancreatitis with Nesidioblastosis and Hyperinsulinaemic Hypoglycaemia. Natl. Med. J. India 2008, 21, 307–312. [Google Scholar]
- Bright, E.; Garcea, G.; Ong, S.L.; Madira, W.; Berry, D.P.; Dennison, A.R. An Unsual Case of Concurrent Insulinoma and Nesidioblastosis. J. Pancreas 2008, 9, 649–653. [Google Scholar]
- Zhao, Y.; Xu, J.; Wu, Y.; Han, W. The Application of Intraoperative Ultrasonography in the Diagnosis and Therapy of Insulinoma. Zhonghua Wai Ke Za Zhi 2009, 47, 337–338. [Google Scholar]
- Dong, A.; Yuan, Z.; Zhang, H.; Gao, Y.; Guo, X. Nesidioblastosis in an Adult with Type 2 Diabetes Mellitus: A Case Report. Beijing Da Xue Xue Bao 2009, 41, 590–592. [Google Scholar] [PubMed]
- Carpenter, T.; Trautmann, M.E.; Baron, A.D. Hyperinsulinemic Hypoglycemia with Nesidioblastosis after Gastric-Bypass Surgery. N. Engl. J. Med. 2009, 353, 2192–2194. [Google Scholar] [CrossRef]
- Andronesi, D.; Andronesi, A.; Tonea, A.; Andrei, S.; Herlea, V.; Lupescu, I.; Ionescu-Târgovişte, C.; Coculescu, M.; Fica, S.; Ionescu, M.; et al. Insulinoma of the Pancreas: Analysis of a Clinical Series of 30 Cases. Chirurgia 2009, 104, 675–685. [Google Scholar] [PubMed]
- Ahn, J.; Lee, S.E.; Lee, E.S.; Chung, Y.J.; Oh, Y.S.; Shinn, S.H.; Kim, J. A Case of Nesidioblastosis Causing Hypoglycaemia after Delivery. Diabetes Res. Clin. Pract. 2009, 83, e5–e7. [Google Scholar] [CrossRef]
- Toyomasu, Y.; Fukuchi, M.; Yoshida, T.; Tajima, K.; Osawa, H.; Motegi, M.; Iijima, T.; Nagashima, K.; Ishizaki, M.; Mochiki, E.; et al. Treatment of Hyperinsulinemic Hypoglycemia Due to Diffuse Nesidioblastosis in Adults: A Case Report. Am. Surg. 2009, 75, 331–334. [Google Scholar] [CrossRef]
- Rumilla, K.M.; Erickson, L.A.; Service, F.J.; Vella, A.; Thompson, G.B.; Grant, C.S.; Lloyd, R.V. Hyperinsulinemic Hypoglycemia with Nesidioblastosis: Histologic Features and Growth Factor Expression. Mod. Pathol. 2009, 22, 239–245. [Google Scholar] [CrossRef]
- Francesconi, A.B.; Matos, M.; Lee, J.C.; Wyld, D.K.; Clouston, A.D.; Macfarlane, D. Nesidioblastosis as a Cause of Focal Pancreatic 111In-Pentetreotide Uptake in a Patient with Putative VIPoma: Another Differential Diagnosis. Ann. Nucl. Med. 2009, 23, 497–499. [Google Scholar] [CrossRef]
- Hight, D.; James, L.P.; Jahadi, M.R. Pancreatic Islet Hyperplasia as a Cause of a Severe Ulcer Diathesis. Arch. Surg. 1971, 103, 98–100. [Google Scholar] [CrossRef]
- Thaler, J.P.; Cummings, D.E. Minireview: Hormonal and Metabolic Mechanisms of Diabetes Remission after Gastrointestinal Surgery. Endocrinology 2009, 150, 2518–2525. [Google Scholar] [CrossRef]
- Henopp, T.; Anlauf, M.; Schmitt, A.; Schlenger, R.; Zalatnai, A.; Couvelard, A.; Ruszniewski, P.; Schaps, K.P.; Jonkers, Y.M.H.; Speel, E.J.M.; et al. Glucagon Cell Adenomatosis: A Newly Recognized Disease of the Endocrine Pancreas. J. Clin. Endocrinol. Metab. 2009, 94, 213–217. [Google Scholar] [CrossRef]
- Spanakis, E.; Gragnoli, C. Successful Medical Management of Status Post-Roux-En-y-Gastric-Bypass Hyperinsulinemic Hypoglycemia. Obes. Surg. 2009, 19, 1333–1334. [Google Scholar] [CrossRef]
- Aasheim, E.; Frigstad, S.; Søvik, T.; Birkeland, K.; Haukeland, J. Hyperinsulinemic Hypoglycemia and Liver Cirrhosis Presenting after Duodenal Switch: A Case Report. Surg. Obes. Relat. Dis. 2010, 6, 441–443. [Google Scholar] [CrossRef] [PubMed]
- Halperin, F.; Patti, M.E.; Goldfine, A.B. Glucagon Treatment for Post-Gastric Bypass Hypoglycemia. Obesity 2010, 18, 1858–1860. [Google Scholar] [CrossRef] [PubMed]
- Guseva, N.; Phillips, D.; Mordes, J.P. Successful Treatment of Persistent Hyperinsulinemic Hypoglycemia with Nifedipine in an Adult Patient. Endocr. Pract. 2010, 16, 107–111. [Google Scholar] [CrossRef] [PubMed]
- Moreno Moreno, P.; Gutiérrez Alcántara, C.; Muñoz-Villanueva Mdel, C.; Ortega, R.; Corpas Jiménez Mdel, S.; Zurera Tendero, L.; Benito López, P. Usefulness of Arterial Calcium Stimulation with Hepatic Venous Sampling in the Localization Diagnosis of Endogenous Hyperinsulinism. Endocrinol. Nutr. 2010, 57, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Goretzki, P.; Starke, A.; Lammers, B.; Schwarz, K.; Röher, H.D. Pankreatischer Hyperinsulinismus Wandel Des Krankheitsbildes Mit Spezifischen Unterschieden Auch Bei Sporadischen Erkrankungsformen (Eigene Erfahrung an 144 operierten Patienten von 19862009). Zent. Chir.-Z. Allg. Visz. Gefasschir. 2010, 135, 218–225. [Google Scholar] [CrossRef]
- Ballester, M.; Pastor, B.; Pascual, H.; Pallares, J.; Albasini, J. Nesidioblastosis as a Cause of Hyperinsulinism in the Adult. Cir. Esp. 2010, 88, 423–425. [Google Scholar] [CrossRef]
- Bränström, R.; Berglund, E.; Curman, P.; Forsberg, L.; Höög, A.; Grimelius, L.; Berggren, P.-O.; Mattsson, P.; Hellman, P.; Juntti-Berggren, L. Electrical Short-Circuit in β-Cells from a Patient with Non-Insulinoma Pancreatogenous Hypoglycemic Syndrome (NIPHS): A Case Report. J. Med. Case Rep. 2010, 4, 2–6. [Google Scholar] [CrossRef]
- Greene, C.A.; Rao, V.S.; Maragos, G.D.; Mitchell, J.R. Pancreatic Islet Cell Hyperplasia. A Case Report. Nebr. Med. J. 1972, 57, 125–126. [Google Scholar]
- McElroy, M.K.; Lowy, A.M.; Weidner, N. Case Report: Focal Nesidioblastosis (“nesidioblastoma”) in an Adult. Hum. Pathol. 2010, 41, 447–451. [Google Scholar] [CrossRef]
- Kibebew, M.; Bacha, S.; Feleke, Y.; Johnson, O. Case Reports of Insulinoma and Nesidioblastosis in Ethiopia. Ethiop. Med. J. 2010, 48, 73–79. [Google Scholar] [PubMed]
- Mathavan, V.K.; Arregui, M.; Davis, C.; Singh, K.; Patel, A.; Meacham, J. Management of Postgastric Bypass Noninsulinoma Pancreatogenous Hypoglycemia. Surg. Endosc. 2010, 24, 2547–2555. [Google Scholar] [CrossRef] [PubMed]
- Reubi, J.C.; Perren, A.; Rehmann, R.; Waser, B.; Christ, E.; Callery, M.; Goldfine, A.B.; Patti, M.E. Glucagon-like Peptide-1 (GLP-1) Receptors Are Not Overexpressed in Pancreatic Islets from Patients with Severe Hyperinsulinaemic Hypoglycaemia Following Gastric Bypass. Diabetologia 2010, 53, 2641–2645. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Vanderveen, K.A.; Grant, C.S.; Thompson, G.B.; Farley, D.R.; Richards, M.L.; Vella, A.; Vollrath, B.; Service, F.J. Outcomes and Quality of Life after Partial Pancreatectomy for Noninsulinoma Pancreatogenous Hypoglycemia from Diffuse Islet Cell Disease. Surgery 2010, 148, 1237–1246. [Google Scholar] [CrossRef]
- Bernard, B.; Kline, G.A.; Service, F.J. Hypoglycaemia Following Upper Gastrointestinal Surgery: Case Report and Review of the Literature. BMC Gastroenterol. 2010, 10, 77. [Google Scholar] [CrossRef]
- Rabiee, A.; Magruder, J.T.; Salas-Carrillo, R.; Carlson, O.; Egan, J.M.; Askin, F.B.; Elahi, D.; Andersen, D.K. Hyperinsulinemic Hypoglycemia after Roux-En-y Gastric Bypass: Unraveling the Role of Gut Hormonal and Pancreatic Endocrine Dysfunction. J. Surg. Res. 2011, 167, 199–205. [Google Scholar] [CrossRef]
- Arafah, M.; Kfoury, H.; Naseem, S. Hypoglycemia, a Rare Presentation of a Solid Pseudopapillary Neoplasm of the Pancreas: A Case Report. Turk. J. Gastroenterol. 2011, 22, 544–547. [Google Scholar] [CrossRef][Green Version]
- Nayak, H.K.; Sothwal, A.; Raizaida, N.; Daga, M.K.; Agarwal, A.K.; Durga, G. A Rare Case of Non-Insulinoma Pancreatic Hypoglycaemia Syndrome (Niphs) in an Adult Due to Localised Islet Cell Hyperplasia-Successfully Managed by Enucleation. BMJ Case Rep. 2011, 2011, bcr0720114554. [Google Scholar] [CrossRef]
- Batra, C.; Saluja, S.; Bajaj, R.; Rajshekar, U.; Thakur, V.; Gupta, V. Non-Insulinoma Pancreatogenous Hypoglycemia Syndrome. J. Assoc. Physicians India 2011, 59, 256–258. [Google Scholar]
- Jacobs, W.H.; Halperin, P.; Mantz, F.A. Watery Diarrhea and Hypokalemia Due to Nonbeta-Islet Cell Hyperplasia of the Pancreas. Am. J. Gastroenterol. 1972, 57, 333–339. [Google Scholar]
- Otto, A.I.; Marschalko, M.; Zalatnai, A.; Toth, M.; Kovacs, J.; Harsing, J.; Tulassay, Z.; Karpati, S. Glucagon Cell Adenomatosis: A New Entity Associated with Necrolytic Migratory Erythema and Glucagonoma Syndrome. J. Am. Acad. Dermatol. 2011, 65, 458–459. [Google Scholar] [CrossRef] [PubMed]
- Azemoto, N.; Kumagi, T.; Yokota, T.; Kuroda, T.; Koizumi, M.; Yamanishi, H.; Soga, Y.; Furukawa, S.; Abe, M.; Ikeda, Y.; et al. An Unusual Case of Subclinical Diffuse Glucagonoma Coexisting with Two Nodules in the Pancreas: Characteristic Features on Computed Tomography. Clin. Res. Hepatol. Gastroenterol. 2012, 36, e43–e47. [Google Scholar] [CrossRef] [PubMed]
- Roberts, R.E.; Zhao, M.; Whitelaw, B.C.; Ramage, J.; Diaz-Cano, S.; Le Roux, C.W.; Quaglia, A.; Huang, G.C.; Aylwin, S.J.B. GLP-1 and Glucagon Secretion from a Pancreatic Neuroendocrine Tumor Causing Diabetes and Hyperinsulinemic Hypoglycemia. J. Clin. Endocrinol. Metab. 2012, 97, 3039–3045. [Google Scholar] [CrossRef] [PubMed]
- Qintar, M.; Sibai, F.; Taha, M. Hypoglycemia Due to an Adult-Onset Nesidioblastosis, a Diagnostic and Management Dilemma. Avicenna J. Med. 2012, 2, 45–47. [Google Scholar] [CrossRef]
- Limongelli, P.; Belli, A.; Cioffi, L.; Russo, G.; D’Agostino, A.; Fantini, C.; Maiello, F.; Belli, G. Hepatobiliary and Pancreatic: Nesidioblastosis. J. Gastroenterol. Hepatol. 2012, 27, 1538. [Google Scholar] [CrossRef]
- De Heide, L.J.M.; Glaudemans, A.W.J.M.; Oomen, P.H.N.; Apers, J.A.; Totté, E.R.E.; Van Beek, A.P. Functional Imaging in Hyperinsulinemic Hypoglycemia after Gastric Bypass Surgery for Morbid Obesity. J. Clin. Endocrinol. Metab. 2012, 97, 963–967. [Google Scholar] [CrossRef]
- Myint, K.S.; Greenfield, J.R.; Farooqi, I.S.; Henning, E.; Holst, J.J.; Finer, N. Prolonged Successful Therapy for Hyperinsulinaemic Hypoglycaemia after Gastric Bypass: The Pathophysiological Role of GLP1 and Its Response to a Somatostatin Analogue. Eur. J. Endocrinol. 2012, 166, 951–955. [Google Scholar] [CrossRef]
- Nadelson, J.; Epstein, A. A Rare Case of Noninsulinoma Pancreatogenous Hypoglycemia Syndrome. Case Rep. Gastrointest. Med. 2012, 2012, 1–3. [Google Scholar] [CrossRef]
- Przybylik-Mazurek, E.; Pach, D.; Hubalewska-Dydejczyk, A.; Sowa-Staszczak, A.; Gilis-Januszewska, A.; Kulig, J.; Matyja, A.; Chrapczyński, P. Symptoms and Early Diagnostic Possibilities of Pancreatic Endocrine Cells Hyperplasia (Nesidioblastosis). Przegl. Lek. 2012, 69, 9–14. [Google Scholar]
- Ceppa, E.P.; Ceppa, D.P.; Omotosho, P.A.; Dickerson, J.A.; Park, C.W.; Portenier, D.D. Algorithm to Diagnose Etiology of Hypoglycemia after Roux-En-Y Gastric Bypass for Morbid Obesity: Case Series and Review of the Literature. Surg. Obes. Relat. Dis. 2012, 8, 641–647. [Google Scholar] [CrossRef]
- Vance, J.E.; Stoll, R.W.; Kitabchi, A.E.; Buchanan, K.D.; Hollander, D.; Williams, R.H. Familial Nesidioblastosis as the Predominant Manifestation of Multiple Endocrine Adenomatosis. Am. J. Med. 1972, 52, 211–227. [Google Scholar] [CrossRef]
- Ferrario, C.; Stoll, D.; Boubaker, A.; Matter, M.; Yan, P.; Puder, J.J. Diffuse Nesidioblastosis with Hypoglycemia Mimicking an Insulinoma: A Case Report. J. Med. Case Rep. 2012, 6, 332. [Google Scholar] [CrossRef]
- Lee, C.J.; Brown, T.; Magnuson, T.H.; Egan, J.M.; Carlson, O.; Elahi, D. Hormonal Response to a Mixed-Meal Challenge after Reversal of Gastric Bypass for Hypoglycemia. J. Clin. Endocrinol. Metab. 2013, 98, 1208–1212. [Google Scholar] [CrossRef]
- Christ, E.; Wild, D.; Ederer, S.; Béhé, M.; Nicolas, G.; Caplin, M.E.; Brändle, M.; Clerici, T.; Fischli, S.; Stettler, C.; et al. Glucagon-like Peptide-1 Receptor Imaging for the Localisation of Insulinomas: A Prospective Multicentre Imaging Study. Lancet Diabetes Endocrinol. 2013, 1, 115–122. [Google Scholar] [CrossRef]
- Soares, F.; Providência, R.; Pontes, M. Nesidioblastosis: An Undescribed Cause of Transient Loss of Conscience in Young Adults. Europace 2013, 15, 1506. [Google Scholar] [CrossRef] [PubMed]
- García-Santos, E.P.; Manzanares-Campillo, M.D.C.; Padilla-Valverde, D.; Villarejo-Campos, P.; Gil-Rendo, A.; Muñoz-Atienza, V.; Sánchez-García, S.; Puig-Rullán, A.M.; Rodríguez-Peralto, J.L.; Martín-Fernández, J. Nesidioblastosis. A Case of Hyperplasia of the Islets of Langerhans in the Adult. Pancreatology 2013, 13, 544–548. [Google Scholar] [CrossRef] [PubMed]
- Then, C.; Nam-Apostolopoulos, Y.; Seissler, J.; Lechner, A. Refractory Idiopathic Non-Insulinoma Pancreatogenous Hypoglycemia in an Adult: Case Report and Review of the Literature. JOP 2013, 14, 264–268. [Google Scholar] [CrossRef] [PubMed]
- Al-Sarireh, B.; Haidermota, M.; Verbeke, C.; Rees, D.A.; Yu, R.; Griffiths, A.P. Glucagon Cell Adenomatosis without Glucagon Receptor Mutation. Pancreas 2013, 42, 360–362. [Google Scholar] [CrossRef]
- Choi, J.E.; Noh, S.J.; Sung, J.J.; Moon, W.S. Nesidioblastosis and Pancreatic Non-Functioning Islet Cell Tumor in an Adult with Type 2 Diabetes Mellitus. Korean J. Pathol. 2013, 47, 489–491. [Google Scholar] [CrossRef]
- Gupta, R.; Patel, R.; Nagral, S. Adult Onset Nesidioblastosis Treated by Subtotal Pancreatectomy. JOP 2013, 14, 286–288. [Google Scholar] [CrossRef]
- Sowa-Staszczak, A.; Pach, D.; Mikołajczak, R.; Mäcke, H.; Jabrocka-Hybel, A.; Stefańska, A.; Tomaszuk, M.; Janota, B.; Gilis-Januszewska, A.; Małecki, M.; et al. Glucagon-like Peptide-1 Receptor Imaging with [Lys40(Ahx-HYNIC- 99mTc/EDDA)NH2]-Exendin-4 for the Detection of Insulinoma. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 524–531. [Google Scholar] [CrossRef] [PubMed]
- Larsson, L.I.; Ljungberg, O.; Sundler, F.; Håkanson, R.; Svensson, S.O.; Rehfeld, J.; Stadil, R.; Holst, J. Antro Pyloric Gastrinoma Associated with Pancreatic Nesidioblastosis and Proliferation of Islets. Virchows Arch. A Pathol. Pathol. Anat. 1973, 360, 305–314. [Google Scholar] [CrossRef] [PubMed]
- Pongprasobchai, S.; Lertwattanarak, R.; Pausawasdi, N.; Prachayakul, V. Diagnosis and Localization of Insulinoma in Thai Patients: Performance of Endoscopic Ultrasonography Compared to Computed Tomography and Magnetic Resonance Imaging. J. Med. Assoc. Thai. 2013, 96 (Suppl. 2), S187–S193. [Google Scholar] [PubMed]
- Maeda, Y.; Yokoyama, K.; Takeda, K.; Takada, J.; Hamada, H.; Hujioka, Y.; Kudo, S.E. Adult-Onset Diffuse Nesidioblastosis Causing Hypoglycemia. Clin. J. Gastroenterol. 2013, 6, 50–54. [Google Scholar] [CrossRef]
- Grönberg, M.; Tsolakis, A.V.; Holmbäck, U.; Stridsberg, M.; Grimelius, L.; Janson, E.T. Ghrelin and Obestatin in Human Neuroendocrine Tumors: Expression and Effect on Obestatin Levels after Food Intake. Neuroendocrinology 2013, 97, 291–299. [Google Scholar] [CrossRef]
- Challis, B.G.; Harris, J.; Sleigh, A.; Isaac, I.; Orme, S.M.; Seevaratnam, N.; Dhatariya, K.; Simpson, H.L.; Semple, R.K. Familial Adult Onset Hyperinsulinism Due to an Activating Glucokinase Mutation: Implications for Pharmacological Glucokinase Activation. Clin. Endocrinol. 2014, 81, 855–861. [Google Scholar] [CrossRef]
- Campos, G.M.; Ziemelis, M.; Paparodis, R.; Ahmed, M.; Davis, D.B. Laparoscopic Reversal of Roux-En-Y Gastric Bypass: Technique and Utility for Treatment of Endocrine Complications. Surg. Obes. Relat. Dis. 2014, 10, 36–43. [Google Scholar] [CrossRef]
- Kang, H.; Kim, S.; Lim, T.S.; Lee, H.W.; Choi, H.; Kang, C.M.; Kim, H.G.; Bang, S. A Case of Alpha-Cell Nesidioblastosis and Hyperplasia with Multiple Glucagon-Producing Endocrine Cell Tumor of the Pancreas. Korean J. Gastroenterol. 2014, 63, 253–257. [Google Scholar] [CrossRef]
- Pathak, R.; Karmacharya, P.; Salman, A.; Alweis, R. An Unusual Cause of Hypoglycemia in a Middle-Aged Female after Bariatric Surgery. J. Community Hosp. Intern. Med. Perspect. 2014, 4, 23118. [Google Scholar] [CrossRef]
- Rao, B.B.; Click, B.; Codario, R. Successful Management of Refractory Noninsulinoma Pancreatogenous Hypoglycemia Syndrome with Gastric Bypass Reversal: A Case Report. Am. J. Gastroenterol. 2014, 109, S309. [Google Scholar] [CrossRef]
- de Santibañes, M.; Cristiano, A.; Mazza, O.; Grossenbacher, L.; de Santibañes, E.; Sánchez Clariá, R.; Sivori, E.; García Mónaco, R.; Pekolj, J. Endogenous Hyperinsulinemic Hypoglycemia Syndrome: Surgical Treatment. Cir. Esp. 2014, 92, 547–552. [Google Scholar] [CrossRef] [PubMed]
- García, B.F.; Peromingo, R.; Galindo, J.; Arrieta, F.; Sánchez, J.; Vázquez, C.; Botella-Carretero, J.I. Tratamiento de Las Hipoglucemias Graves Tras Bypass Gástrico Con Pancreatectomía Subtotal: A Propósito de 2 Casos. Endocrinol. Nutr. 2014, 61, 391–393. [Google Scholar] [CrossRef] [PubMed]
- Creutzfeldt, W.; Arnold, R.; Creutzfeldt, C.; Track, N.S. Pathomorphologic, Biochemical, and Diagnostic Aspects of Gastrinomas (Zollinger-Ellison Syndrome). Hum. Pathol. 1975, 6, 47–76. [Google Scholar] [CrossRef] [PubMed]
- Woo, C.Y.; Jeong, J.Y.; Jang, J.E.; Leem, J.; Jung, C.H.; Koh, E.H.; Lee, W.J.; Kim, M.S.; Park, J.Y.; Lee, J.B.; et al. Clinical Features and Causes of Endogenous Hyperinsulinemic Hypoglycemia in Korea. Diabetes Metab. J. 2015, 39, 126–131. [Google Scholar] [CrossRef]
- Martin-Grace, J.; O’Tuathail, M.; Hannon, M.J.; Swan, N.; O’Shea, D.; Tamagno, G. Amlodipine for the Medical Treatment of Adult-Onset Diffuse Nesidioblastosis. Pancreas 2015, 44, 1162–1164. [Google Scholar] [CrossRef]
- Valli, V.; Blandamura, S.; Pastorelli, D.; Merigliano, S.; Sperti, C. Nesidioblastosis Coexisting with Non-Functioning Islet Cell Tumour in an Adult. Endokrynol. Pol. 2015, 66, 356–360. [Google Scholar] [CrossRef][Green Version]
- Ramírez-González, L.R.; Sotelo-Álvarez, J.A.; Rojas-Rubio, P.; MacÍas-Amezcua, M.D.; Orozco-Rubio, R.; Fuentes-Orozco, C. Nesidioblastosis En El Adulto: Reporte de Un Caso. Cir. Cir. 2015, 83, 324–328. [Google Scholar] [CrossRef]
- Thompson, S.M.; Vella, A.; Thompson, G.B.; Rumilla, K.M.; Service, F.J.; Grant, C.S.; Andrews, J.C. Selective Arterial Calcium Stimulation with Hepatic Venous Sampling Differentiates Insulinoma from Nesidioblastosis. J. Clin. Endocrinol. Metab. 2015, 100, 4189–4197. [Google Scholar] [CrossRef]
- Maguire, D. Lesson of the Month 2: An Unusual Presentation of Hyperinsulinaemic Hypoglycaemia with Possible Underlying Diagnosis of Glucose-Sensitive Insulinoma or Islet Cell Hyperplasia. Clin. Med. J. R. Coll. Physicians Lond. 2015, 15, 495–496. [Google Scholar] [CrossRef]
- Ünal, B.; Uzun, Ö.C.; Başsorgun, C.I.; Erdoğan, O.; Elpek, G.Ö. A Rare Complication of Gastric Bypass (Weight Loss) Surgery: Nesidioblastosis. Int. J. Surg. Pathol. 2015, 23, 68–70. [Google Scholar] [CrossRef]
- Fountoulakis, S.; Malliopoulos, D.; Papanastasiou, L.; Pappa, T.; Karydas, G.; Piaditis, G. Reversal of Impaired Counterregulatory Cortisol Response Following Diazoxide Treatment in a Patient with Non Insulinoma Pancreatogenous Hypoglycemia Syndrome: Case Report and Overview of Pathogenetic Mechanisms. Hormones 2015, 14, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Qin, H.; Li, Z.; Qu, L.; Liu, Y.; Gao, Y.; Li, F.; Wang, G. A Rare Case of Focal Nesidioblastosis Causing Adult-Onset Hypoglycemia. Exp. Ther. Med. 2015, 10, 723–726. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Sampaio-Neto, J.; Branco-Filho, A.J.; Nassif, L.S.; Nassif, A.T.; Masi, F.D.J.; Ximenez, D.R. Proposal of a Revisional Surgery to Treat Non-Insulinoma Hyperinsulinemic Hypoglicemia Postgastric Bypass. ABCD Arq. Bras. Cir. Dig. 2015, 28, 278–281. [Google Scholar] [CrossRef]
- Verner, J.V.; Morrison, A.B. Endocrine Pancreatic Islet Disease With Diarrhea: Report of a Case Due to Diffuse Hyperplasia of Nonbeta Islet Tissue with a Review of 54 Additional Cases. Arch. Intern. Med. 1974, 133, 492–500. [Google Scholar] [CrossRef] [PubMed]
- Christ, E.; Wild, D.; Antwi, K.; Waser, B.; Fani, M.; Schwanda, S.; Heye, T.; Schmid, C.; Baer, H.U.; Perren, A.; et al. Preoperative Localization of Adult Nesidioblastosis Using 68Ga-DOTA-Exendin-4-PET/CT. Endocrine 2015, 50, 821–823. [Google Scholar] [CrossRef] [PubMed]
- Mordes, J.; Alonso, L. Evaluation, Medical Therapy, and Course of Adult Persistent Hyperinsulinemic Hypoglycemia after Roux-En-Y Gastric Bypass Surgery: A Case Series. Endocr. Pract. 2015, 21, 237–246. [Google Scholar] [CrossRef]
- Mihai, B.M.; Lăcătuşu, C.M.; Arhire, L.I.; Graur, M.; Scripcariu, V.; Aniţei, M.G.; Radu, I.; Ferariu, D.; Danciu, M. Pathological Aspects Underlying Pancreatogenous Hyperinsulinemic Hypoglycemia—Report of Three Cases. Rom. J. Morphol. Embryol. 2015, 56, 251–256. [Google Scholar]
- de Vasconcellos Macedo, A.L.; Hidal, J.T.; Marcondes, W.; Mauro, F.C. Robotic Near-Total Pancreatectomy for Nesidioblastosis after Bariatric Surgery. Obes. Surg. 2016, 26, 3082–3083. [Google Scholar] [CrossRef][Green Version]
- Kim, J.R.; Jang, J.Y.; Shin, Y.C.; Cho, Y.M.; Kim, H.; Kwon, W.; Han, Y.M.; Kim, S.W. Difficult Diagnosis and Localization of Focal Nesidioblastosis: Clinical Implications of 68Gallium-DOTAD-Phe1-Tyr3-Octreotide PET Scanning. Ann. Surg. Treat. Res. 2016, 91, 51–55. [Google Scholar] [CrossRef][Green Version]
- Yang, Z.; Tan, H.; Sun, Y.; Si, S.; Xu, L.; Liu, X.; Liu, L.; Zhou, W.; Huang, J. Intraoperative Portal Vein Insulin Assay Combined with Occlusion of the Pancreas for Complex Pancreatogenous Hypoglycemia. Medicine 2016, 95, e3928. [Google Scholar] [CrossRef]
- Luo, Y.; Pan, Q.; Yao, S.; Yu, M.; Wu, W.; Xue, H.; Kiesewetter, D.O.; Zhu, Z.; Li, F.; Zhao, Y.; et al. Glucagon-like Peptide-1 Receptor PET/CT with 68Ga-NOTA-Exendin-4 for Detecting Localized Insulinoma: A Prospective Cohort Study. J. Nucl. Med. 2016, 57, 715–720. [Google Scholar] [CrossRef] [PubMed]
- Schwetz, V.; Horvath, K.; Kump, P.; Lackner, C.; Perren, A.; Forrer, F.; Pieber, T.R.; Treiber, G.; Sourij, H.; Mader, J.K. Successful Medical Treatment of Adult Nesidioblastosis with Pasireotide over 3 Years. Medicine 2016, 95, e3272. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Prasad, V.; Sainz-Esteban, A.; Arsenic, R.; Plöckinger, U.; Denecke, T.; Pape, U.F.; Pascher, A.; Kühnen, P.; Pavel, M.; Blankenstein, O. Role of 68Ga Somatostatin Receptor PET/CT in the Detection of Endogenous Hyperinsulinaemic Focus: An Explorative Study. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 1593–1600. [Google Scholar] [CrossRef]
- Krieger, A.; Smirnov, A.; Berelavichus, S.; Gorin, D.; Kaldarov, A.; Karel’skaya, N.; Vetsheva, N.; Kalinin, D.; Lebedeva, A.; Dugarova, R. Organic Hyperinsulinism: Radiological Diagnostics and Surgical Treatment. Khirurgiia 2016, 6, 14–29. [Google Scholar] [CrossRef] [PubMed]
- Stefanini, P.; Carboni, M.; Patrassi, N.; Basoli, A. Hypoglycemia and Insular Hyperplasia. Review of 148 Cases. Ann. Surg. 1974, 180, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Vilarrasa, N.; Goday, A.; Rubio, M.A.; Caixàs, A.; Pellitero, S.; Ciudin, A.; Calañas, A.; Botella, J.I.; Bretón, I.; Morales, M.J.; et al. Hyperinsulinemic Hypoglycemia after Bariatric Surgery: Diagnosis and Management Experience from a Spanish Multicenter Registry. Obes. Facts 2016, 9, 41–51. [Google Scholar] [CrossRef]
- Sowa-Staszczak, A.; Trofimiuk-Müldner, M.; Stefańska, A.; Tomaszuk, M.; Buziak-Bereza, M.; Gilis-Januszewska, A.; Jabrocka-Hybel, A.; Głowa, B.; Małecki, M.; Bednarczuk, T.; et al. 99mTc Labeled Glucagon-like Peptide-1-Analogue (99mTc-GLP1) Scintigraphy in the Management of Patients with Occult Insulinoma. PLoS ONE 2016, 11, e0160714. [Google Scholar] [CrossRef]
- Gunnarsdóttir, G.; Guðmundsdóttir, A.; Hellmanm, P.; Stålberg, P. Repeated Non-Epileptic Seizures in a Previously Healthy Young Woman—A Case Report. Laeknabladid 2016, 102, 339–342. [Google Scholar] [CrossRef]
- De Sousa, S.M.C.; Haghighi, K.S.; Qiu, M.R.; Greenfield, J.R.; Chen, D.L.T. Synchronous Nesidioblastosis, Endocrine Microadenoma, and Intraductal Papillary Mucinous Neoplasia in a Man Presenting with Hyperinsulinemic Hypoglycemia. Pancreas 2016, 45, 154–159. [Google Scholar] [CrossRef]
- Anderson, B.; Nostedt, J.; Girgis, S.; Dixon, T.; Agrawal, V.; Wiebe, E.; Senior, P.A.; Shapiro, A.M.J. Insulinoma or Non-Insulinoma Pancreatogenous Hypoglycemia? A Diagnostic Dilemma. J. Surg. Case Rep. 2016, 2016, rjw188. [Google Scholar] [CrossRef]
- Preechasuk, L.; Pongpaibul, A.; Kunavisarut, T. Non-Insulinoma Pancreatogeneous Hypoglycemia Syndrome with False-Positive Somatostatin Receptor Scintigraphy: A Case Report and Review of Literature. J. Med. Assoc. Thai. 2016, 99, 354–359. [Google Scholar] [PubMed]
- Chen, X.; Kamel, D.; Barnett, B.; Yung, E.; Quinn, A.; Nguyen, C. An Unusual Presentation of Post Gastric Bypass Hypoglycemia with Both Postprandial and Fasting Hypoglycemia. Endocrinol. Diabetes Metab. Case Rep. 2018, 2018, 18–89. [Google Scholar] [CrossRef] [PubMed]
- Dadheech, N.; Garrel, D.; Buteau, J. Evidence of Unrestrained Beta-Cell Proliferation and Neogenesis in a Patient with Hyperinsulinemic Hypoglycemia after Gastric Bypass Surgery. Islets 2018, 10, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Antwi, K.; Fani, M.; Heye, T.; Nicolas, G.; Rottenburger, C.; Kaul, F.; Merkle, E.; Zech, C.J.; Boll, D.; Vogt, D.R.; et al. Comparison of Glucagon-like Peptide-1 Receptor (GLP-1R) PET/CT, SPECT/CT and 3T MRI for the Localisation of Occult Insulinomas: Evaluation of Diagnostic Accuracy in a Prospective Crossover Imaging Study. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 2318–2327. [Google Scholar] [CrossRef]
- Luca, V.G.; Kwadwo, A.; Guillaume, N.P.; Damian, W.; Emanuel, C. Clinical Presentation of 54 Patients with Endogenous Hyperinsulinaemic Hypoglycaemia: A Neurological Chameleon (Observational Study). Swiss Med. Wkly. 2018, 148, 1–5. [Google Scholar] [CrossRef]
- Jahnke, K.; Sawitzki, E. Deafness Due to Hyperinsulinism (Author’s Transl). HNO 1975, 23, 152–155. [Google Scholar]
- Kérékou, A.; El Aziz, S.; Dédjan, A.; Chadli, A.; Farouqi, A. Hypoglycemia Controlled by Prednisone in an Occult Insulinoma or a Nesidioblastosis. Open J. Endocr. Metab. Dis. 2019, 9, 69–73. [Google Scholar] [CrossRef][Green Version]
- Wiesli, P.; Pavlicek, V.; Brändle, M.; Pfammatter, T.; Perren, A.; Schmid, C. Distinct Mechanisms of Hypoglycaemia in Patients with Somatostatin-secreting Neuroendocrine Tumours. Endocrinol. Diabetes Metab. 2019, 2, 2–5. [Google Scholar] [CrossRef]
- Lozano-Melendez, E.; Aguilar-Soto, M.; Graniel-Palafox, L.E.; Ceceña-Martínez, L.E.; Valdez-Ortiz, R.; Solis-Jimenez, F. Adult Nesidioblastosis in Chronic Kidney Disease. Case Rep. Endocrinol. 2019, 2019, 1–6. [Google Scholar] [CrossRef]
- Dauriz, M.; Maneschi, C.; Castelli, C.; Tomezzoli, A.; Fuini, A.; Landoni, L.; Malleo, G.; Ferdeghini, M.; Bonora, E.; Moghetti, P. A Case Report of Insulinoma Relapse on Background Nesidioblastosis: A Rare Cause of Adult Hypoglycemia. J. Clin. Endocrinol. Metab. 2019, 104, 773–778. [Google Scholar] [CrossRef]
- Allué, M.; Ros, S.; Lamata, F. Pancreatic Nesidioblastosis: Case Report. Med. Clin. 2019, 152, 245–246. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.; Conway, L.; Cooper, C.; Sinha, A.; Nandi, N. Nesidioblastosis in an Adult with Short Gut Syndrome and Type 2 Diabetes. AACE Clin. Case Rep. 2019, 5, e375–e379. [Google Scholar] [CrossRef] [PubMed]
- Kim, A.; Snaith, J.R.; Mahajan, H.; Holmes-Walker, D.J. Nesidioblastosis Following Laparoscopic Sleeve Gastrectomy. Clin. Endocrinol. 2019, 91, 906–908. [Google Scholar] [CrossRef]
- Orujov, M.; Lai, K.K.; Forse, C.L. Concurrent Adult-Onset Diffuse β-Cell Nesidioblastosis and Pancreatic Neuroendocrine Tumor: A Case Report and Review of the Literature. Int. J. Surg. Pathol. 2019, 27, 912–918. [Google Scholar] [CrossRef] [PubMed]
- Delbeke, D.; Newman, G.; Deppen, S.; Shah, C.; Ndolo, J.; Shi, C.; Bailey, C.E.; Jessop, A.C.; Sandler, M.P. 68Ga-DOTATATE: Significance of Uptake in the Tail of the Pancreas in Patients without Lesions. Clin. Nucl. Med. 2019, 44, 851–854. [Google Scholar] [CrossRef] [PubMed]
- Kalff, V.; Iravani, A.; Ackhurst, T.; Pattison, D.A.; Eu, P.; Hofman, M.S.; Hicks, R.J.; Akhurst, T.; Pattison, D.A.; Eu, P.; et al. Utility of 68 Ga-DOTA-Exendin-4 PET/CT Imaging in Distinguishing between Insulinoma and Nesidioblastosis in Patients with Confirmed Endogenous Hyperinsulinaemic Hypoglycaemia. Intern. Med. J. 2020, 51, 1657–1664. [Google Scholar] [CrossRef]
- Rastogi, G.K.; Sialy, R.; Sinha, M.K.; Dash, R.; Chopra, J.S.; Kataria, R.N. Serum and Pancreatic Immunoreactive Insulin (IRI) and Proinsulin-like Component (PLC), Serum IRI and PLC Response to Different Stimuli in Normal Subjects and Organic Hyperinsulinism. Acta Diabetol. Lat. 1975, 12, 309–323. [Google Scholar] [CrossRef]
- Lopes, A.A.; Miranda, A.C.; Maior, M.S.; de Mello, R.V.; Bandeira, F. Nesidioblastosis Associated with Pancreatic Heterotopia as a Differential Diagnosis of Hypoglycemia: A Literature Review and Case Report. Am. J. Case Rep. 2020, 21, e922778-1. [Google Scholar] [CrossRef]
- Antwi, K.; Hepprich, M.; Müller, N.A.; Reubi, J.C.; Fani, M.; Rottenburger, C.; Nicolas, G.; Kaul, F.; Christ, E.R.; Wild, D. Pitfalls in the Detection of Insulinomas with Glucagon-like Peptide-1 Receptor Imaging. Clin. Nucl. Med. 2020, 45, e386–e392. [Google Scholar] [CrossRef]
- Boss, M.; Buitinga, M.; Jansen, T.J.P.; Brom, M.; Visser, E.P.; Gotthardt, M. PET-Based Human Dosimetry of 68Ga-NODAGA-Exendin-4, a Tracer for β-Cell Imaging. J. Nucl. Med. 2020, 61, 112–116. [Google Scholar] [CrossRef]
- Awramiszyn-Fernández, N.; Paz-Ibarra, J.; Suárez-Rojas, J.; Rodríguez-Alegría, C.; Somocurcio-Peralta, J.; Ramírez-Delpino, E.; Teruya-Gibu, A. Hyperinsulinemic Hypoglycemia Caused by Nesidioblastosis Associated with Non-Surgical Weight Loss. Rev. Med. Inst. Mex. Seguro Soc. 2020, 58, 528–535. [Google Scholar] [CrossRef] [PubMed]
- McManus, N.M.; Margart, K.M.; Offman, R.P. Hypoglycemia Worsened by Glucose Administration: A Case of Hypoglycemia Years After Gastric Surgery. J. Emerg. Med. 2021, 60, e77–e79. [Google Scholar] [CrossRef] [PubMed]
- Kato, R.; Nishimura, A.; Matsumura, K.; Kikuno, S.; Nagasawa, K.; Mori, Y. Successful Treatment of Adult-Onset Nesidioblastosis by Continuous Subcutaneous Octreotide Infusion in a Patient on Hemodialysis. Clin. Case Rep. 2021, 9, 278–281. [Google Scholar] [CrossRef] [PubMed]
- Snaith, J.R.; McLeod, D.; Richardson, A.; Chipps, D. Multifocal Insulinoma Secondary to Insulinomatosis: Persistent Hypoglycaemia despite Total Pancreatectomy. Endocrinol. Diabetes Metab. Case Rep. 2021, 2020. [Google Scholar] [CrossRef] [PubMed]
- Torres-Arano, S.E.; Fernández-Baez, N.; Torres-González, M.G.; González-Cabrera, I.G.; López-Rosales, F. Hyperinsulinemic Hypoglycemia in Adults. Nesidioblastosis Case Report and Review of the Literature. Cir. Cir. Engl. Ed. 2021, 89, 70–75. [Google Scholar] [CrossRef]
- Castillo-López, M.G.; Fernandez, M.F.; Sforza, N.; Barbás, N.C.; Pattin, F.; Mendez, G.; Ogresta, F.; Gondolesi, I.; Barros Schelotto, P.; Musso, C.; et al. Hyperinsulinemic Hypoglycemia in Adolescents: Case Report and Systematic Review. Clin. Diabetes Endocrinol. 2022, 8, 3. [Google Scholar] [CrossRef] [PubMed]
- Koneshamoorthy, A.; Seniveratne-Epa, D.; Calder, G.; Sawyer, M.; Kay, T.W.H.; Farrell, S.; Loudovaris, T.; Mariana, L.; McCarthy, D.; Lyu, R.; et al. Case Report: Hypoglycemia Due to a Novel Activating Glucokinase Variant in an Adult—A Molecular Approach. Front. Endocrinol. 2022, 13, 842937. [Google Scholar] [CrossRef]
- Dobosz, P.; Dzieciątkowski, T. The Intriguing History of Cancer Immunotherapy. Front. Immunol. 2019, 10, 2965. [Google Scholar] [CrossRef]
- Doi, S.; Yamada, T.; Kito, Y.; Obara, S.; Fujii, Y.; Nishimura, T.; Kato, T.; Nakayama, H.; Tsutsumi, M.; Okamura, R. Adult-Onset Focal Nesidioblastosis with Nodular Formation Mimicking Insulinoma. J. Endocr. Soc. 2022, 6, bvab185. [Google Scholar] [CrossRef]
- Efendić, S.; Lins, P.E.; Sigurdsson, G.; Ivemark, B.; Granberg, P.O.; Luft, R. Effect of Somatostatin on Basal and Glucose Induced Insulin Release in Five Patients with Hyperinsulinaemia. Acta Endocrinol. 1976, 81, 525–529. [Google Scholar] [CrossRef]
- Mendelsohn, G. Multiple Tumors in a Renal Transplant Recipient. Johns Hopkins Med. J. 1976, 139, 253–256. [Google Scholar] [PubMed]
- Larsson, L.I. Two Distinct Types of Islet Abnormalities Associated with Endocrine Pancreatic Tumours. Virchows Arch. A Pathol. Anat. Histol. 1977, 376, 209–219. [Google Scholar] [CrossRef] [PubMed]
- Greider, M.H.; Lacy, P.E.; Kissane, J.M.; Rieders, E.; Thomas, G. Pancreatic Perinuclear Inclusions in Diabetes Mellitus and Other Diseases. Diabetes 1977, 26, 793–797. [Google Scholar] [CrossRef] [PubMed]
- Lesna, M.; Hamlyn, A.N.; Venables, C.W.; Record, C.O. Chronic Laxative Abuse Associated with Pancreatic Islet Cell Hyperplasia. Gut 1977, 18, 1032–1035. [Google Scholar] [CrossRef] [PubMed]
- Ingemansson, S.; Kühl, C.; Larsson, L.I.; Lunderquist, A.; Nobin, A. Islet Cell Hyperplasia Localized by Pancreatic Vein Catheterization and Insulin Radioimmunoassay. Am. J. Surg. 1977, 133, 643–645. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, M.; Floyd, J.C.; Pek, S.; Fajans, S.S. Insulin, Proinsulin, Glucagon and Gastrin in Pancreatic Tumors and in Plasma of Patients with Organic Hyperinsulinism. J. Clin. Endocrinol. Metab. 1977, 44, 681–694. [Google Scholar] [CrossRef]
- Schwartz, S.E.; Fitzgerald, M.A.; Levine, R.A.; Schwartzel, E.H. Normal Jejunal Cyclic Nucleotide Content in a Patient With Secretory Diarrhea. Arch. Intern. Med. 1978, 138, 1403–1405. [Google Scholar] [CrossRef]
- Schikman, C.H.; Chertow, B.S.; Fabris, B.L. Paradoxical Enhancement of Tolbutamide-Induced Insulin Release by Diazoxide in a Patient with Islet Cell Hyperplasia. Acta Paediatr. Scand. 1978, 67, 671–676. [Google Scholar] [CrossRef]
- Ingemansson, S.; Kühl, C.; Larsson, L.I.; Lunderquist, A.; Lundquist, I. Localization of Insulinomas and Islet Cell Hyperplasias by Pancreatic Vein Catheterization and Insulin Assay. Surg. Gynecol. Obstet. 1978, 146, 725–734. [Google Scholar]
- Kidd, G.S.; Donowitz, M.; O’Dorisio, T.; Cataland, S.; Newman, F. Mild Chronic Watery Diarrhea-Hypokalemia Syndrome Associated with Pancreatic Islet Cell Hyperplasia. Elevated Plasma and Tissue Levels of Gastric Inhibitory Polypeptide and Successful Management with Nicotinic Acid. Am. J. Med. 1979, 66, 883–888. [Google Scholar] [CrossRef]
- Varas Lorenzo, M.J.; Curto Cardús, J.A.; Sans Segarra, M.; Carrera Plans, M. Zollinger-Ellison Syndrome Type II Due to Diffuse Hyperplasia of the Pancreatic Islet Cells (Author’s Transl). Med. Clin. 1979, 73, 68–72. [Google Scholar]
- Dahms, B.B.; Landing, B.H.; Blashovics, M.; Roe, T.F. Nesidioblastosis and Other Islet Cell Abnormalities in Hyperinsulinemic Hypoglycemia of Childhood. Hum. Pathol. 1980, 11, 641–649. [Google Scholar] [CrossRef] [PubMed]
- Tomita, T.; Kimmel, J.; Friesen, S.; Mantz, F. Pancreatic Polypeptide Cell Hyperplasia with and without Watery Diarrhea Syndrome. J. Surg. Oncol. 1980, 14, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Friesen, S.R.; Kimmel, J.R.; Tomita, T. Pancreatic Polypeptide as Screening Marker for Pancreatic Polypeptide Apudomas in Multiple Endocrinopathies. Am. J. Surg. 1980, 139, 61–72. [Google Scholar] [CrossRef] [PubMed]
- Leong, A.S.; Slavotinek, A.H.; Higgins, B.A. Nesidioblastosis, Islet Cell Hyperplasia, and Adenomatosis in a Case of Metastasizing Insulinoma: Contribution to the Genesis of the Islets of Langerhans. Diabetes Care 1980, 3, 537–542. [Google Scholar] [CrossRef]
- Brennan, M.D.; Service, F.J.; Carpenter, A.M.; Rubenstein, A.H.; Edis, A.J. Diagnosis of Pancreatic Islet Hyperplasia Causing Hypoglycemia in a Patient with Portacaval Anastomosis. Am. J. Med. 1980, 68, 941–948. [Google Scholar] [CrossRef]
- Reichardt, W.; Ingemansson, S. Selective Vein Catheterization for Hormone Assay in Endocrine Tumours of the Pancreas. Technique and Results. Acta Radiol. Diagn. 1980, 21, 177–187. [Google Scholar] [CrossRef]
- Glaser, B.; Valtysson, G.; Fajans, S.S.; Vinik, A.I.; Cho, K.; Thompson, N. Gastrointestinal/Pancreatic Hormone Concentrations in the Portal Venous System of Nine Patients with Organic Hyperinsulinism. Metabolism 1981, 30, 1001–1010. [Google Scholar] [CrossRef]
- Duncan, W.E.; Duncan, T.G.; DeLaurentis, D.A.; Kryston, L.; Kaminski, K.; Paskin, D.L. Artificial Pancreas as an Aid during Insulinoma Resection. Am. J. Surg. 1981, 142, 528–531. [Google Scholar] [CrossRef]
- Bonfils, S.; Landor, J.H.; Mignon, M.; Hervoir, P. Results of Surgical Management in 92 Consecutive Patients with Zollinger Ellison Syndrome. Ann. Surg. 1981, 194, 692–697. [Google Scholar] [CrossRef]
- Nathan, D.M.; Axelrod, L.; Proppe, K.H.; Wald, R.; Hirsch, H.J.; Martin, D.B. Nesidioblastosis Associated with Insulin-Mediated Hypoglycemia in an Adult. Diabetes Care 1981, 4, 383–388. [Google Scholar] [CrossRef] [PubMed]
- Harness, J.K.; Geelhoed, G.W.; Thompson, N.W.; Nishiyama, R.H.; Fajans, S.S.; Kraft, R.O.; Howard, D.R.; Clark, K.A. Nesidioblastosis in Adults: A Surgical Dilemma. Arch. Surg. 1981, 116, 575–580. [Google Scholar] [CrossRef] [PubMed]
- Jennette, J.C.; Wilkman, A.S.; Bagnell, C.R. Insulin Receptor Autoantibody-Induced Pancreatic Islet Beta (B) Cell Hyperplasia. Arch. Pathol. Lab. Med. 1982, 106, 218–220. [Google Scholar] [PubMed]
- Cho, K.J.; Vinik, A.I.; Thompson, N.W.; Sgields, J.J.; Porter, D.J.; Brady, T.M.; Cadavid, G.; Fajans, S.S.; Shields, J.J.; Porter, D.J.; et al. Localization of the Source of Hyperinsulinism: Percutaneous Transhepatic Portal and Pancreatic Vein Catheterization with Hormone Assay. Am. J. Radiol. 1982, 139, 237–245. [Google Scholar] [CrossRef]
- Zhu, Y.; Zeng, X.J.; Zhang, J.X.; Cai, L. Reoperation for Insulinoma and Islet Hyperplasia. Chin. Med. J. 1983, 96, 525–532. [Google Scholar]
- Oliver, M.H.; Drury, P.L.; Van’t Hoff, W. A Case of Multiple Endocrine Adenomatosis (Type 1) with Nesidioblastosis, Terminating with an Exocrine Pancreatic Carcinoma. Clin. Endocrinol. 1983, 18, 495–503. [Google Scholar] [CrossRef]
- Keller, A.; Stone, A.M.; Valderrama, E.; Kolodny, H. Pancreatic Nesidioblastosis in Adults. Report of a Patient with Hyperinsulinemic Hypoglycemia. Am. J. Surg. 1983, 145, 412–416. [Google Scholar] [CrossRef]
- Rayman, G.; Santo, M.; Salomon, F.; Almog, S.; Paradinas, F.J.; Pinkhas, J.; Reynolds, K.W.; Wise, P.H. Hyperinsulinaemic Hypoglycaemia Due to Chlorpropamide-Induced Nesidioblastosis. J. Clin. Pathol. 1984, 37, 651–654. [Google Scholar] [CrossRef]
- Bauman, W.; Merkle, L.; Rachman, R.; Mitsuto, S. Hypoglycemia in a Diabetes Nurse Care Coordinator. Diabetes Care 1984, 7, 88–91. [Google Scholar] [CrossRef]
- Harrison, T.S.; Fajans, S.S.; Floyd, J.C.; Thompson, N.W.; Rasbach, D.A.; Santen, R.J.; Cohen, C. Prevalence of Diffuse Pancreatic Beta Islet Cell Disease with Hyperinsulinism: Problems in Recognition and Management. World J. Surg. 1984, 8, 583–587. [Google Scholar] [CrossRef]
- Tomita, T.; Kimmel, J.R.; Friesen, S.R.; Doull, V.; Pollock, H.G. Pancreatic Polypeptide in Islet Cell Tumors. Morphologic and Functional Correlations. Cancer 1985, 56, 1649–1657. [Google Scholar] [CrossRef] [PubMed]
- Bani, D.; Bani Sacchi, T.; Biliotti, G. Nesidioblastosis and Intermediate Cells in the Pancreas of Patients with Hyperinsulinemic Hypoglycemia. Virchows Arch. B Cell Pathol. Incl. Mol. Pathol. 1985, 48, 19–32. [Google Scholar] [CrossRef] [PubMed]
- Bani Sacchi, T.; Bani, D.; Biliotti, G. Nesidioblastosis and Islet Cell Changes Related to Endogenous Hypergastrinemia. Virchows Arch. B Cell Pathol. Incl. Mol. Pathol. 1985, 48, 261–276. [Google Scholar] [CrossRef] [PubMed]
- Campbell, I.L.; Harrison, L.C.; Ley, C.J.; Colman, P.G.; Ellis, D.W. Nesidioblastosis and Multifocal Pancreatic Islet Cell Hyperplasia in an Adult. Clinicopathologic Features and in Vitro Pancreatic Studies. Am. J. Clin. Pathol. 1985, 84, 534–541. [Google Scholar] [CrossRef]
- Madeira, M.D.; Reis, L.; Medina, J.L.; Sambade, C.; Carneiro, F.; de Oliveira, C. Nesidioblastose e Insulinoma. Uma Associação Pouco Frequente. Acta Med. Port. 1986, 7, 165–170. [Google Scholar]
- Illyés, G.; Bálint, A.; Kiss, S. Nesidioblastosis in an Adult. Orv. Hetil. 1986, 127, 2633–2636. [Google Scholar]
- Klöppel, G.; Willemer, S.; Stamm, B.; Häcki, W.H.; Heitz, P.U. Pancreatic Lesions and Hormonal Profile of Pancreatic Tumors in Multiple Endocrine Neoplasia Type I. An Immunocytochemical Study of Nine Patients. Cancer 1986, 57, 1824–1832. [Google Scholar] [CrossRef]
- Ray, M.B.; Zumwalt, R. Islet-Cell Hyperplasia in Genetic Deficiency of Alpha-1-Proteinase Inhibitor. Am. J. Clin. Pathol. 1986, 85, 681–687. [Google Scholar] [CrossRef]
- Kovacs, K.; Horvath, E.; Asa, S.L.; Murray, D.; Singer, W.; Reddy, S.S. Microscopic Peliosis of Pancreatic Islets in a Woman with MEN-1 Syndrome. Arch. Pathol. Lab. Med. 1986, 110, 607–610. [Google Scholar]
- Odaira, C.; Choux, R.; Payan, M.J.; Bockman, D.E.; Sarles, H. Chronic Obstructive Pancreatitis, Nesidioblastosis, and Small Endocrine Pancreatic Tumor. Dig. Dis. Sci. 1987, 32, 770–774. [Google Scholar] [CrossRef]
- Jerkins, T.W.; Sacks, H.S.; O’dorisio, T.M.; Tuttle, S.; Solomon, S.S. Medullary Carcinoma of the Thyroid, Pancreatic Nesidioblastosis and Microadenosis, and Pancreatic Polypeptide Hypersecretion: A New Association and Clinical and Hormonal Responses to Long-Acting Somatostatin Analog SMS 201-995*. J. Clin. Endocrinol. Metab. 1987, 64, 1313–1319. [Google Scholar] [CrossRef]
- Carlson, T.; Eckhauser, M.; DeBaz, B.; Khiyami, A.; Park, C. Nesidioblastosis in an Adult: An Illustrative Case and Collective Review. Am. J. Gastroenterol. 1987, 82, 566–571. [Google Scholar]
- Asa, S.L.; Singer, W.; Kovacs, K.; Horvath, E.; Murray, D.; Colapinto, N.; Thorner, M.O. Pancreatic Endocrine Tumour Producing Growth Hormone-Releasing Hormone Associated with Multiple Endocrine Neoplasia Type I Syndrome. Acta Endocrinol. 1987, 115, 331–337. [Google Scholar] [CrossRef]
- Glaser, B.; Shapiro, B.; Glowniak, J.; Fajans, S.S.; Vinik, A.I. Effects of Secretin on the Normal and Pathological β-Cell. J. Clin. Endocrinol. Metab. 1988, 66, 1138–1143. [Google Scholar] [CrossRef] [PubMed]
- Roncari, D.A.; Yoon, J.W.; Pak, C.Y.; Keane, P.M.; Preshaw, R.M. Excessive Growth of Cultured Beta Cells from an Adult Patient with Beta Cell Hyperplasia. Clin. Investig. Med. 1988, 11, 129–133. [Google Scholar]
- Kohnert, K.D.; Fält, K.; Odselius, R.; Ziegler, M.; Madsen, O.D.; Grimelius, L.; Falkmer, S. Production of Pro-Insulin, C-Peptide, and Insulin in Nesidioblastosis, Focal Islet-Cell Adenomatosis, and Genuine Insulomas. A Correlated Radioimmunochemical, Immunohistochemical, and Ultrastructural Investigation with Particular Regard to the Occurrence. Diabetes Res. 1988, 8, 151–163. [Google Scholar] [PubMed]
- Balas, D.; Senegas-Balas, F.; Delvaux, M.; Bertrand, C.; Fagot-Revurat, P.; Rumeau, J.L.; Ribet, A. Silent Human Pancreatic Glucagonoma and “a” Nesidioblastosis. Pancreas 1988, 3, 734–739. [Google Scholar] [CrossRef]
- Lamberts, S.W.J. Somatostatin Analogs in the Management of Gastrointestinal Tumors. Horm. Res. Paediatr. 1988, 29, 118–120. [Google Scholar] [CrossRef]
- Woltering, E.A.; Mozell, E.J.; O’Dorisio, T.M.; Fletcher, W.S.; Howe, B. Suppression of Primary and Secondary Peptides with Somatostatin Analog in the Therapy of Functional Endocrine Tumors. Surg. Gynecol. Obstet. 1988, 167, 453–462. [Google Scholar]
- Derizhanova, I.S. Clinico-Anatomical Comparisons in Duodenal Carcinoid Tumors. Arkh. Patol. 1989, 51, 53–58. [Google Scholar]
- McHenry, C.; Newell, K.; Chejfec, G.; Barbato, A.; Lawrence, A.M.; Brooks, M.; Emanuele, M.; Paloyan, E. Adult Nesidioblastosis. An Unusual Cause of Fasting Hypoglycemia. Am. Surg. 1989, 55, 366–369. [Google Scholar] [PubMed]
- Sawady, J.; Mendelsohn, G. Extrapancreatic Gastrinoma with Pancreatic Islet Cell Hyperplasia. Arch. Pathol. Lab. Med. 1989, 113, 536–538. [Google Scholar] [PubMed]
- Risaliti, A.; Pizzolitto, S. Nesidioblastosis Arising from Heterotopic Pancreas and Presenting with Hypertension. A Clinical, Immunohistochemical and Ultrastructural Study. Ann. Chir. 1989, 43, 459–464. [Google Scholar] [PubMed]
- Chines, A.; Fogelfeld, L.; Zaidel, L.; Feigl, D. Nesidioblastosis in Adults. Isr. J. Med. Sci. 1989, 25, 450–453. [Google Scholar] [PubMed]
- Albers, N.; Lohr, M.; Bogner, U.; Loy, V.; Kloppel, G.; Klöppel, G.; Kloppel, G. Nesidioblastosis of the Pancreas in an Adult with Persistent Hyperinsulinemic Hypoglycemia. Am. J. Clin. Pathol. 1989, 91, 336–340. [Google Scholar] [CrossRef][Green Version]
- Fong, T.L.; Warner, N.E.; Kumar, D. Pancreatic Nesidioblastosis in Adults. Diabetes Care 1989, 12, 108–114. [Google Scholar] [CrossRef]
- Martínez Valls, J.F.; Ascaso, J.F.; Ferrández, A.; Hernández, A.; González Bayo, E.; Carmena, R. Hyperplasia of the Pancreatic Islets or Nesidioblastosis in Adults? Apropos 2 Cases. Med. Clin. 1990, 95, 341–343. [Google Scholar]
- Mozell, E.J.; Woltering, E.A.; O’Dorisio, T.M.; Phillipson, B.E.; Fletcher, J.; Fletcher, W.S.; Howe, B.; Hill, D.; Rhea, D. Adult Onset Nesidioblastosis: Response of Glucose, Insulin, and Secondary Peptides to Therapy with Sandostatin. Am. J. Gastroenterol. 1990, 85, 181–188. [Google Scholar]
- Alhindawi, R.; Deitel, M.; Kempston, J.; Bendago, M. Severe Secretory Diarrhea with Elevated Gastrin-Releasing Peptide Controlled by Somatostatin Analogue: A Case Report. Can. J. Surg. 1990, 33, 139–142. [Google Scholar]
- Kohnert, K.; Fält, K.; Rosolski, T.; Ziegler, M.; Warzok, R.; Weirich, J.; Falkmer, S. Argyrophil and Beta-Endorphin Immunoreactive Cells in Focal Islet-Cell Adenomatosis and Insulin-Producing Islet-Cell Adenomata. Acta Histochem. 1990, 89, 57–60. [Google Scholar] [CrossRef]
- Bani, D.; Biliotti, G.; Sacchi, T.B. Morphological Changes in the Human Endocrine Pancreas Induced by Chronic Excess of Endogenous Glucagon. Virchows Arch. B Cell Pathol. Incl. Mol. Pathol. 1991, 60, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Kimura, W.; Kuroda, A.; Morioka, Y. Clinical Pathology of Endocrine Tumors of the Pancreas. Analysis of Autopsy Cases. Dig. Dis. Sci. 1991, 36, 933–942. [Google Scholar] [CrossRef] [PubMed]
- Böttger, T.; Gabbert, H.; Beyer, J.; Schweden, F.; Junginger, T. Nesidioblastosis and Adenomatosis of the Pancreas as an Unusual Cause of Organic Hyperinsulinism. Chirurg 1992, 63, 139–142. [Google Scholar] [PubMed]
- Burman, W.J.; McDermott, M.T.; Bornemann, M. Familial Hyperinsulinism Presenting in Adults. Arch. Intern. Med. 1992, 152, 2125–2127. [Google Scholar] [CrossRef]
- Andrews, R.; Balsitis, M.; Shurrock, K.; Jeffcoate, W.J. Nesidioblastosis in Adults. Postgrad. Med. J. 1992, 68, 390. [Google Scholar] [CrossRef][Green Version]
- Tibaldi, J.M.; Lorber, D.; Lomasky, S.; Steinberg, J.J.; Reisman, R.; Shamoon, H. Postprandial Hypoglycemia in Islet Beta Cell Hyperplasia with Adenomatosis of the Pancreas. J. Surg. Oncol. 1992, 50, 53–57. [Google Scholar] [CrossRef]
- Gaulier, A.; Cahen, J.; Buisson, J.L.; Périé, G.; Vacher, G.; Poulet, B. Pancreatic Insulinoma, Adenomatosis of the Wirsung’s Duct and Chronic Pancreatitis. Apropos of a Case. Arch. Anat. Cytol. Pathol. 1993, 41, 245–250. [Google Scholar]
- Weinand, J.; Kemp, W. Pancreatic Islet Hyperplasia: A Potential Marker for Anabolic-Androgenic Steroid Use. Acad. Forensic Pathol. 2018, 8, 777–785. [Google Scholar] [CrossRef]
- Weir, G.C.; Bonner-Weir, S. Islet β Cell Mass in Diabetes and How It Relates to Function, Birth, and Death. Ann. N. Y. Acad. Sci. 2013, 1281, 92–105. [Google Scholar] [CrossRef]
- Meckler, K.; Brentnall, T.; Haggitt, R.; Crispin, D.; Byrd, D.; Kimmey, M.; Bronner, M. Familial Fibrocystic Pancreatic Atrophy with Endocrine Cell Hyperplasia and Pancreatic Carcinoma. Am. J. Surg. Pathol. 2001, 25, 1047–1053. [Google Scholar] [CrossRef]
- Iannucci, A.; Mukai, K.; Johnson, D.; Burke, B. Endocrine Pancreas in Cystic Fibrosis: An Immunohistochemical Study. Hum. Pathol. 1984, 15, 278–284. [Google Scholar] [CrossRef] [PubMed]
- Schiaffino, E.; Schmid, C.; Mortara, G. Anatomopathologic Pictures of Chronic Pancreatitis. Pathologica 1990, 82, 687–693. [Google Scholar] [PubMed]
- Christ, E.; Antwi, K.; Fani, M.; Wild, D. Innovative Imaging of Insulinoma: The End of Sampling? A Review. Endocr. Relat. Cancer 2020, 27, R79–R92. [Google Scholar] [CrossRef]
- Pattison, D.A.; Hicks, R.J. Molecular Imaging in the Investigation of Hypoglycaemic Syndromes and Their Management. Endocr. Relat. Cancer 2017, 24, R203–R221. [Google Scholar] [CrossRef] [PubMed]
- Harris, S. Hyperinsulinism and Dysinsulinism. JAMA 1924, 83, 729–733. [Google Scholar] [CrossRef]
- Wilder, R.; Allan, F.; Power, M.; Robertson, H. Carcinoma of the Islands of the Pancreas: Hyperinsulinism and Hypoglycemia. J. Am. Med. Assoc. 1927, 89, 348–355. [Google Scholar] [CrossRef]
- Bartow, S.A.; Mukai, K.; Rosai, J. Pseudoneoplastic Proliferation of Endocrine Cells in Pancreatic Fibrosis. Cancer 1981, 47, 2627–2633. [Google Scholar] [CrossRef]
- Goudswaard, W.B.; Houthoff, H.J.; Koudstaal, J.; Zwierstra, R.P. Nesidioblastosis and Endocrine Hyperplasia of the Pancreas: A Secondary Phenomenon. Hum. Pathol. 1986, 17, 46–54. [Google Scholar] [CrossRef]
- Hirshberg, B.; Libutti, S.K.; Alexander, H.R.; Bartlett, D.L.; Cochran, C.; Livi, A.; Chang, R.; Shawker, T.; Skarulis, M.C.; Gorden, P. Blind Distal Pancreatectomy for Occult Insulinoma, an Inadvisable Procedure. J. Am. Coll. Surg. 2002, 194, 761–764. [Google Scholar] [CrossRef]
- Yakovac, W.C.; Baker, L.; Hummeler, K. Beta Cell Nesidioblastosis in Idiopathic Hypoglycemia of Infancy. J. Pediatr. 1971, 79, 226–231. [Google Scholar] [CrossRef]
- Bouwens, L.; Pipeleers, D.G. Extra-Insular Beta Cells Associated with Ductules Are Frequent in Adult Human Pancreas. Diabetologia 1998, 41, 629–633. [Google Scholar] [CrossRef] [PubMed]
- Ariel, I.; Kerem, E.; Bartfeld, E. Nesidiodysplasia A Histologic Entity? Hum. Pathol. 1988, 19, 1215–1218. [Google Scholar] [CrossRef] [PubMed]
- Gilbert-Barness, E.; Potter, E.L. Potter’s Pathology of the Fetus and Infant; Yearbook Publisher: Chicago, IL, USA, 1997; p. 54. [Google Scholar]
- Jiang, C.X.; Tan, Y.B. Morphogenetic Study on Hyperplastic and Neoplastic Diseases of Endocrine Pancreas. Zhonghua Bing Li Xue Za Zhi = Chin. J. Pathol. 1990, 19, 175–178. [Google Scholar]
- Yu, R. Pancreatic α-Cell Hyperplasia: Facts and Myths. J. Clin. Endocrinol. Metab. 2014, 99, 748–756. [Google Scholar] [CrossRef]
- Zhou, C.; Dhall, D.; Nissen, N.N.; Chen, C.R.; Yu, R. Homozygous P86s Mutation of the Human Glucagon Receptor Is Associated with Hyperglucagonemia, α Cell Hyperplasia, and Islet Cell Tumor. Pancreas 2009, 38, 941–946. [Google Scholar] [CrossRef] [PubMed]
- Fathia, G.; Michael, S.; Andrea, P.; Jensen, R.T. Multiple Endocrine Neoplasia Type 1 and Zollinger-Ellison Syndrome: A Prospective Study of 107 Cases and Comparison with 1009 Cases from the Literature. Medicine 2004, 83, 43–83. [Google Scholar] [CrossRef]
- Meier, J.J.; Butler, A.E.; Galasso, R.; Rizza, R.A.; Butler, P.C. Increased Islet Beta Cell Replication Adjacent to Intrapancreatic Gastrinomas in Humans. Diabetologia 2006, 49, 2689–2696. [Google Scholar] [CrossRef]
- Rosenberg, L.; Brown, R.A.; Duguid, W.P. A New Approach to the Induction of Duct Epithelial Hyperplasia and Nesidioblastosis by Cellophane Wrapping of the Hamster Pancreas. J. Surg. Res. 1983, 35, 63–72. [Google Scholar] [CrossRef]
- Rosenberg, L.; Duguid, W.; Brown, R.; Vinik, A. Induction of Nesidioblastosis Will Reverse Diabetes in Syrian Golden Hamster. Diabetes 1988, 37, 334–341. [Google Scholar] [CrossRef]
- Donev, S.; Petkov, P.; Zhablenska, R.; Katala, Z.; Bonafus, R.; Fisho, F.; Desbal, B. Morphological Changes in the Pancreas after Ligation of the Excretory Duct. Eksp. Med. Morfol. 1994, 32, 9–18. [Google Scholar]
- Meissner, H. The Islands of Langerhans in Cystic Pancreatic Fibrosis and Morphologically Related Pancreatic Conditions. Beitr. Pathol. Anat. 1954, 114, 192–211. [Google Scholar]
- Soejima, K.; Landing, B. Pancreatic Islets in Older Patients with Cystic Fibrosis with and without Diabetes Mellitus: Morphometric and Immunocytologic Studies. Pediatr. Pathol. 1986, 6, 25–46. [Google Scholar] [CrossRef] [PubMed]
- Larghi, A.; Stobinski, M.; Galasso, D.; Lecca, P.G.; Costamagna, G. Concomitant Intraductal Papillary Mucinous Neoplasm and Pancreatic Endocrine Tumour: Report of Two Cases and Review of the Literature. Dig. Liver Dis. 2009, 41, 759–761. [Google Scholar] [CrossRef] [PubMed]
- Palladino, A.A.; Stanley, C.A. Nesidioblastosis No Longer! It’s All about Genetics. J. Clin. Endocrinol. Metab. 2011, 96, 617–619. [Google Scholar] [CrossRef]
- Rosenfeld, E.; Ganguly, A.; De Leon, D.D. Congenital Hyperinsulinism Disorders: Genetic and Clinical Characteristics. Am. J. Med. Genet. Part C Semin. Med. Genet. 2019, 181, 682–692. [Google Scholar] [CrossRef] [PubMed]
- Gilis-Januszewska, A.; Piatkowski, J.; Skalniak, A.; Piwonska-Solska, B.; Nazim, J.; Pach, D.; Przybylik-Mazurek, E.; Sowa-Staszczak, A.; Starzyk, J.; Hubalewska-Dydejczyk, A. Noninsulinoma Pancreatogenous Hypoglycaemia in Adults—A Spotlight on Its Genetics. Endokrynol. Pol. 2015, 66, 344–354. [Google Scholar] [CrossRef][Green Version]
- Dunger, D.B.; Burns, C.; Ghale, G.K.; Muller, D.P.R.; Spitz, L.; Grant, D.B. Pancreatic Exocrine and Endocrine Function after Subtotal Pancreatectomy for Nesidioblastosis. J. Pediatr. Surg. 1988, 23, 112–115. [Google Scholar] [CrossRef]
- Rother, K.I.; Carney, J.A.; Couce, M.; Charlesworth, J.; Butler, P.C. Islet Amyloid Polypeptide in Pancreatic Tissue of Children with Persistent Hyperinsulinemic Hypoglycemia Caused by Primary Islet Hyperplasia and Nesidioblastosis. J. Clin. Endocrinol. Metab. 1995, 80, 1956–1959. [Google Scholar] [CrossRef]
- Leibowitz, G.; Glaser, B.; Higazi, A.A.; Salameh, M.; Cerasi, E.; Landau, H. Hyperinsulinemic Hypoglycemia of Infancy (Nesidioblastosis) in Clinical Remission: High Incidence of Diabetes Mellitus and Persistent Beta-Cell Dysfunction at Long-Term Follow-Up. J. Clin. Endocrinol. Metab. 1995, 80, 386–392. [Google Scholar] [CrossRef][Green Version]
- Dacou-Voutetakis, C.; Psychou, F.; Maniati-Christidis, M. Persistent Hyperinsulinemic Hypoglycemia of Infancy: Long-Term Results. J. Pediatr. Endocrinol. Metab. 1998, 11 (Suppl. 1), 131–141. [Google Scholar] [CrossRef]
- Martinez-Ibanez, V.; Gussinyer, M.; Toran, N.; Lloret, J.; Abad, P.; Carrascosa, A.; Boix-Ochoa, J. Pancreatectomy Extension in Persistent Hyperinsulinaemic Hypoglycaemia: A New Strategy. Eur. J. Pediatr. Surg. 2002, 12, 262–266. [Google Scholar] [CrossRef] [PubMed]
- Bin-Abbas, B.S.; Al-Ashwal, A.A. Diabetes in a Nonpancreatectomized Child with Nesidioblastosis. Diabetes Care 2004, 27, 626–627. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Restrepo, K.; Garavito, G.; Rojas, L.; Romero, A.; Neira, F.; Oliveros, R.; Abisambra, N. Nesidioblastosis Del Adulto Coexistente Con Insulinoma. Rev. Colomb. Cancerol. 2009, 13, 49–60. [Google Scholar] [CrossRef]
- De Jesús, J.; Fung, L.; Garcia, F.; Núñez, M. Nesidioblastosis En Adolescentes: A Propósito de Un Caso. Rev. Venez. Endocrinol. Metab. 2015, 13, 48–53. [Google Scholar]
- Glaser, B.; Kesavan, P.; Heyman, M.; Davis, E.; Cuesta, A.; Buchs, A.; Stanley, C.A.; Thornton, P.S.; Permutt, M.A.; Matschinsky, F.M.; et al. Familial Hyperinsulinism Caused by an Activating Glucokinase Mutation. N. Engl. J. Med. 1998, 338, 226–230. [Google Scholar] [CrossRef]
- Christesen, H.B.T.; Jacobsen, B.B.; Odili, S.; Buettger, C.; Cuesta-Munoz, A.; Hansen, T.; Brusgaard, K.; Massa, O.; Magnuson, M.A.; Shiota, C.; et al. The Second Activating Glucokinase Mutation (A456V): Implications for Glucose Homeostasis and Diabetes Therapy. Diabetes 2002, 51, 1240–1246. [Google Scholar] [CrossRef]
- Gloyn, A.L.; Noordam, K.; Willemsen, M.A.A.P.; Ellard, S.; Lam, W.W.K.; Campbell, I.W.; Midgley, P.; Shiota, C.; Buettger, C.; Magnuson, M.A.; et al. Insights into the Biochemical and Genetic Basis of Glucokinase Activation from Naturally Occurring Hypoglycemia Mutations. Diabetes 2003, 52, 2433–2440. [Google Scholar] [CrossRef]
- Heredia, V.V.; Carlson, T.J.; Garcia, E.; Sun, S. Biochemical Basis of Glucokinase Activation and the Regulation by Glucokinase Regulatory Protein in Naturally Occurring Mutations. J. Biol. Chem. 2006, 281, 40201–40207. [Google Scholar] [CrossRef]
- Gersing, S.; Cagiada, M.; Gebbia, M.; Gjesing, A.P. A Comprehensive Map of Human Glucokinase Variant Activity. Genome Biol. 2022, 24, 97. [Google Scholar] [CrossRef]
- Christesen, H.B.T.; Tribble, N.D.; Molven, A.; Siddiqui, J.; Sandal, T.; Brusgaard, K.; Ellard, S.; Njølstad, P.R.; Alm, J.; Jacobsen, B.B.; et al. Activating Glucokinase (GCK) Mutations as a Cause of Medically Responsive Congenital Hyperinsulinism: Prevalence in Children and Characterisation of a Novel GCK Mutation. Eur. J. Endocrinol. 2008, 159, 27–34. [Google Scholar] [CrossRef][Green Version]
- Labriola, L.; Peters, M.G.; Krogh, K.; Stigliano, I.; Terra, L.F.; Buchanan, C.; Machado, M.C.C.; Bal de Kier Joffé, E.; Puricelli, L.; Sogayar, M.C. Generation and Characterization of Human Insulin-Releasing Cell Lines. BMC Cell Biol. 2009, 10, 49. [Google Scholar] [CrossRef] [PubMed]
- Götz, W.; Schucht, C.; Roth, J.; Theuring, F.; Herken, R. Endocrine Pancreatic Tumors in MSV-SV40 Large T Transgenic Mice. Am. J. Pathol. 1993, 142, 1493–1503. [Google Scholar] [PubMed]
- Gacar, A.; Pekmezci, D.; Karayigit, M.O.; Kabak, Y.B.; Gulbahar, M.Y. Nesidioblastosis in a Simmental Calf. J. Comp. Pathol. 2012, 147, 491–494. [Google Scholar] [CrossRef] [PubMed]
- Son, W.C.; Faki, K.; Mowat, V.; Gopinath, C. Spontaneously Occurring Extra-Islet Endocrine Cell Proliferation in the Pancreas of Young Beagle Dogs. Toxicol. Lett. 2010, 193, 179–182. [Google Scholar] [CrossRef]
- Polansky, B.J.; Martinez, S.A.; Chalkley, M.D. Resolution of Hyperinsulinemic Hypoglycemia Following Partial Pancreatectomy in a Dog with Nesidioblastosis. J. Am. Vet. Med. Assoc. 2018, 253, 893–896. [Google Scholar] [CrossRef]
- Hawkins, K.L.; Summers, B.A.; Kuhajda, F.P.; Smith, C.A. Immunocytochemistry of Normal Pancreatic Islets and Spontaneous Islet Cell Tumors in Dogs. Vet. Pathol. 1987, 24, 170–179. [Google Scholar] [CrossRef]
- King, C.; Streett, J.; Moody, K.; Barthold, S. Nesidioblastosis Associated with Hyperglycemia in Two Squirrel Monkeys (Saimiri sciureus). J. Med. Primatol. 1996, 25, 361–366. [Google Scholar] [CrossRef]
- Hambrook, L.E.; Ciavarella, A.A.; Nimmo, J.S.; Wayne, J. Hyperinsulinaemic, Hypoglycaemic Syndrome Due to Acquired Nesidioblastosis in a Cat. J. Feline Med. Surg. Open Rep. 2016, 2, 205511691665784. [Google Scholar] [CrossRef]
- Furuoka, H.; Shirakawa, T.; Taniyama, H.; Ohishi, H.; Satoh, H.; Itakura, C. Histogenesis of Neoformation in the Endocrine Pancreas of Aging Horses. Vet. Pathol. 1989, 26, 40–46. [Google Scholar] [CrossRef]
- Novaes, G.; Chetto-de-Queiroz, A.; De-Carvalho-Cardoso, C.; Burlacchini-de-Carvalho, M.; Ribeiro-Filho, L.; Oliveira-Gonçalves, A. Nesidioblastosis Associated with Chronic Experimental Pancreatitis Produced by a Scorpion Toxin, Tityustoxin, in Rats. Braz. J. Med. Biol. Res. Rev. Bras. Pesqui. Med. Biol. 1990, 23, 1149–1151. [Google Scholar]
- Grube, D.; Jörns, A. The Endocrine Pancreas of Glucagon-and Somatostatin-Immunized Rabbits. I. Light Microscopy and Immunohistochemistry. Cell Tissue Res. 1991, 265, 251–260. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, L.; AI, V. Induction of Endocrine Cell Differentiation: A New Approach to Management of Diabetes. J. Lab. Clin. Med. 1989, 114, 75–83. [Google Scholar] [PubMed]
- Simon, B.; Merchant, J.L.; Eissele, R.; Köhler, K.; Arnold, R. Transient Transcriptional Activation of Gastrin during Sodium Butyrate-Induced Differentiation of Islet Cells. Regul. Pept. 1997, 70, 143–148. [Google Scholar] [CrossRef]
- William Traverso, L.; Bockman, D.E.; Pleis, S.K.; Dail, D.H. Nesidioblastosis as a Mechanism to Prevent Fibrosis-Induced Diabetes after Pancreatic Duct Obstruction. Pancreas 1993, 8, 325–329. [Google Scholar] [CrossRef] [PubMed]
- Gerbitz, K.; Boenke, B.; Paprotta, A.; Chemnitz, U.; Hübner, G. Human Nesidioblastosis Tissue as an Immunogen for Generation of Islet Cell Specific Monoclonal Antibodies. J. Clin. Chem. Clin. Biochem. 1988, 26, 659–666. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, L.; Dafoe, D.; Turcotte, J. Enhancing Hamster Pancreatic Islet Isolation by Induction of Nesidioblastosis. Transplant. Proc. 1987, 19, 907–908. [Google Scholar]
- Kerr-Conte, J.; Pattou, F.; Lecomte-Houcke, M.; Xia, Y.; Boilly, B.; Proye, C.; Lefebvre, J. Ductal Cyst Formation in Collagen-Embedded Adult Human Islet Preparations. A Means to the Reproduction of Nesidioblastosis in Vitro. Diabetes 1996, 45, 1108–1114. [Google Scholar] [CrossRef] [PubMed]
- Papaccio, G.; Esposito, V.; Mezzogiorno, V. Islet B Cell Neoproliferation in Early Low Dose Streptozocin Induced Diabetes in Mice: A Ducto-Endocrine Proliferation? Acta Morphol. Hung. 1991, 39, 43–52. [Google Scholar] [PubMed]
- Matsushita, K.; Okita, H.; Suzuki, A.; Shimoda, K.; Fukuma, M.; Yamada, T.; Urano, F.; Honda, T.; Sano, M.; Iwanaga, S.; et al. Islet Cell Hyperplasia in Transgenic Mice Overexpressing EAT/Mcl-1, a Bcl-2 Related Gene. Mol. Cell Endocrinol. 2003, 203, 105–116. [Google Scholar] [CrossRef]
- Pour, P.M.; Kazakoff, K. Stimulation of Islet Cell Proliferation Enhances Pancreatic Ductal Carcinogenesis in the Hamster Model. Am. J. Pathol. 1996, 149, 1017–1025. [Google Scholar]
- Pour, P. Islet Cells as a Component of Pancreatic Ductal Neoplasms. Am. J. Pathol. 1978, 90, 295–316. [Google Scholar] [PubMed]
- Luca, G.; Calvitti, M.; Basta, G.; Baroni, T.; Neri, L.M.; Becchetti, E.; Capitani, S.; Novaes, G.; Correa-Giannella, M.L.; Kalapothakis, E.; et al. Mitogenic Effects of Brazilian Arthropod Venom on Isolated Islet Beta Cells: In Vitro Morphologic Ultrastructural and Functional Studies. J. Investig. Med. 2003, 51, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Sandhyamani, S.; Vijayakumari, A.; Balaraman Nair, M. Bonnet Monkey Model for Pancreatic Changes in Induced Malnutrition. Pancreas 1999, 18, 84–95. [Google Scholar] [CrossRef]
- Rosenberg, L.; Clas, D.; Duguid, W. Trophic Stimulation of the Ductal/Islet Cell Axis: A New Approach to the Treatment of Diabetes. Surgery 1990, 108, 191–197. [Google Scholar]
- Novaes, G.; Cardozo Cde, C.; Costa, N.; de Falco, C.; de Carvalho, M.; de Queiroz, A. Experimental Chronic Interstitial Pancreatitis Induced by Scorpion Toxin in Rats. Arq. Gastroenterol. 1990, 27, 187–190. [Google Scholar]
- Young, M.T.; Phelan, M.J.; Nguyen, N.T. A Decade Analysis of Trends and Outcomes of Male vs Female Patients Who Underwent Bariatric Surgery. J. Am. Coll. Surg. 2016, 222, 226–231. [Google Scholar] [CrossRef]
- Michaels, A.D.; Hunter Mehaffey, J.; Brenton French, W.; Schirmer, B.D.; Kirby, J.L.; Hallowell, P.T. Hypoglycemia Following Bariatric Surgery: Our 31-Year Experience. Obes. Surg. 2017, 27, 3118–3123. [Google Scholar] [CrossRef]
- Singh, E.; Vella, A. Hypoglycemia after Gastric Bypass Surgery. Diabetes Spectr. 2012, 25, 217–221. [Google Scholar] [CrossRef]
- Berger, C.; Zdzieblo, D. Glucose Transporters in Pancreatic Islets. Pflug. Arch. Eur. J. Physiol. 2020, 472, 1249–1272. [Google Scholar] [CrossRef]
- Yan, H.; Yang, W.; Zhou, F.; Li, X.; Pan, Q.; Shen, Z.; Han, G.; Newell-Fugate, A.; Tian, Y.; Majeti, R.; et al. Estrogen Improves Insulin Sensitivity and Suppresses Gluconeogenesis via the Transcription Factor Foxo1. Diabetes 2019, 68, 291–304. [Google Scholar] [CrossRef]
- De Paoli, M.; Zakharia, A.; Werstuck, G.H. The Role of Estrogen in Insulin Resistance: A Review of Clinical and Preclinical Data. Am. J. Pathol. 2021, 191, 1490–1498. [Google Scholar] [CrossRef] [PubMed]
- Mathur, A.; Gorden, P.; Libutti, S. Insulinoma. Surg. Clin. N. Am. 2009, 89, 1105–1121. [Google Scholar] [CrossRef] [PubMed]
- Gill, J. Pancreatitis: A Forensic Perspective. Acad. Forensic Pathol. 2016, 6, 237–248. [Google Scholar] [CrossRef]
- Harris, J.P.; Ricker, A.T.; Gray, R.S.; Steed, R.D.; Gutal, J.J.P. Reversible Hypertrophic Cardiomyopathy Associated with Nesidioblastosis. J. Pediatr. 1992, 120, 272–275. [Google Scholar] [CrossRef] [PubMed]
- Paauw, N.D.; Stegeman, R.; de Vroede, M.A.M.J.; Termote, J.U.M.; Freund, M.W.; Breur, J.M.P.J. Neonatal Cardiac Hypertrophy: The Role of Hyperinsulinism—A Review of Literature. Eur. J. Pediatr. 2020, 179, 39–50. [Google Scholar] [CrossRef] [PubMed]
- Kaczirek, K.; Niederle, B. Nesidioblastosis: An Old Term and a New Understanding. World J. Surg. 2004, 28, 1227–1230. [Google Scholar] [CrossRef]
- Hirshberg, B.; Livi, A.; Bartlett, D.L.; Libutti, S.K.; Alexander, H.R.; Doppman, J.L.; Skarulis, M.C.; Gorden, P. Forty-Eight-Hour Fast: The Diagnostic Test for Insulinoma. J. Clin. Endocrinol. Metab. 2000, 85, 3222–3226. [Google Scholar] [CrossRef]
- Wild, D.; Mäcke, H.; Christ, E.; Gloor, B.; Reubi, J.C. Glucagon-like Peptide 1–Receptor Scans to Localize Occult Insulinomas. N. Engl. J. Med. 2009, 359, 766–768. [Google Scholar] [CrossRef]
- Hepprich, M.; Antwi, K.; Waser, B.; Reubi, J.C.; Wild, D.; Christ, E.R. Brunner’s Gland Hyperplasia in a Patient after Roux-Y Gastric Bypass: An Important Pitfall in GLP-1 Receptor Imaging. Case Rep. Endocrinol. 2020, 2020, 4510910. [Google Scholar] [CrossRef]
- Ahluwalia, N.; Attia, R.; Green, A.; Cane, P.; Routledge, T. Doege-Potter Syndrome. Ann. R. Coll. Surg. Engl. 2015, 97, e105–e107. [Google Scholar] [CrossRef]
- Schröder, G.; Blaas, V.; Boldt, R.; Schober, H.-C. Recurrent Episodes of Hypoglycaemia with Increased Production of the Tissue Hormone Adiponectin: A Case Report. Intern. Med. Care 2019, 3, 112. [Google Scholar] [CrossRef]
- Patel, A.; Daniels, G. Hypoglycemia Secondary to Factitious Hyperinsulinism in a Foster Care Adolescent—A Case Report of Munchausen Syndrome in a Community Hospital Emergency Department Setting. BMC Emerg. Med. 2018, 18, 53. [Google Scholar] [CrossRef] [PubMed]
- Douillard, C.; Mention, K.; Dobbelaere, D.; Wemeau, J.L.; Saudubray, J.M.; Vantyghem, M.C. Hypoglycaemia Related to Inherited Metabolic Diseases in Adults. Orphanet J. Rare Dis. 2012, 7, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Douillard, C.; Jannin, A.; Vantyghem, M.C. Rare Causes of Hypoglycemia in Adults. Ann. Endocrinol. 2020, 81, 110–117. [Google Scholar] [CrossRef]
- Kandaswamy, L.; Raghavan, R.; Pappachan, J.M. Spontaneous Hypoglycemia: Diagnostic Evaluation and Management. Endocrine 2016, 53, 47–57. [Google Scholar] [CrossRef]
- Daví, M.V.; Pia, A.; Guarnotta, V.; Pizza, G.; Colao, A.; Faggiano, A. The Treatment of Hyperinsulinemic Hypoglycaemia in Adults: An Update. J. Endocrinol. Investig. 2017, 40, 9–20. [Google Scholar] [CrossRef]
- Szymanowski, M.; Estebanez, M.S.; Padidela, R.; Han, B.; Mosinska, K.; Stevens, A.; Damaj, L.; Pihan-Le Bars, F.; Lascouts, E.; Reynaud, R.; et al. MTOR Inhibitors for the Treatment of Severe Congenital Hyperinsulinism: Perspectives on Limited Therapeutic Success. J. Clin. Endocrinol. Metab. 2016, 101, 4719–4729. [Google Scholar] [CrossRef]
- McLaughlin, T.; Peck, M.; Holst, J.; Deacon, C. Reversible Hyperinsulinemic Hypoglycemia after Gastric Bypass: A Consequence of Altered Nutrient Delivery. J. Clin. Endocrinol. Metab. 2010, 95, 1851–1855. [Google Scholar] [CrossRef]
- Salehi, M.; Gastaldelli, A.; D’Alessio, D. Blockade of Glucagon-like Peptide 1 Receptor Corrects Postprandial Hypoglycemia after Gastric Bypass. Gastroenterology 2014, 146, 669–680.e2. [Google Scholar] [CrossRef]
- Craig, C.M.; Liu, L.F.; Deacon, C.F.; Holst, J.J.; McLaughlin, T.L. Critical Role for GLP-1 in Symptomatic Post-Bariatric Hypoglycaemia. Diabetologia 2017, 60, 531–540. [Google Scholar] [CrossRef]
- Hackert, T.; Strobel, O.; Michalski, C.W.; Mihaljevic, A.L.; Mehrabi, A.; Müller-Stich, B.; Berchtold, C.; Ulrich, A.; Büchler, M.W. The TRIANGLE Operation—Radical Surgery after Neoadjuvant Treatment for Advanced Pancreatic Cancer: A Single Arm Observational Study. Hpb 2017, 19, 1001–1007. [Google Scholar] [CrossRef] [PubMed]
- Weitz, J.; Rahbari, N.; Koch, M.; Büchler, M.W. The “Artery First” Approach for Resection of Pancreatic Head Cancer. J. Am. Coll. Surg. 2010, 210, e1. [Google Scholar] [CrossRef] [PubMed]
- Boss, M.; Bos, D.L.; Frielink, C.; Sandker, G.; Bronkhorst, P.; van Lith, S.A.; Brom, M.; Buitinga, M.; Gotthardt, M. Receptor-Targeted Photodynamic Therapy of Glucagon-like Peptide 1 Receptor Positive Lesions. J. Nucl. Med. 2020, 61, 1588–1593. [Google Scholar] [CrossRef]
- Soldin, O.P.; Mattison, D.R. Sex Differences in Pharmacokinetics and Pharmacodynamics. Clin. Pharmacokinet. 2009, 48, 143–157. [Google Scholar] [CrossRef]
- Rentzeperi, E.; Pegiou, S.; Koufakis, T.; Grammatiki, M.; Kotsa, K. Sex Differences in Response to Treatment with Glucagon-like Peptide 1 Receptor Agonists: Opportunities for a Tailored Approach to Diabetes and Obesity Care. J. Pers. Med. 2022, 12, 454. [Google Scholar] [CrossRef]
- Gulde, S.; Wiedemann, T.; Schillmaier, M.; Valença, I.; Lupp, A.; Steiger, K.; Yen, H.Y.; Bäuerle, S.; Notni, J.; Luque, R.; et al. Gender-Specific Efficacy Revealed by Head-to-Head Comparison of Pasireotide and Octreotide in a Representative in Vivo Model of Nonfunctioning Pituitary Tumors. Cancers 2021, 13, 3097. [Google Scholar] [CrossRef] [PubMed]
- Gatto, F.; Barbieri, F.; Arvigo, M.; Thellung, S.; Amarù, J.; Albertelli, M.; Ferone, D.; Florio, T. Biological and Biochemical Basis of the Differential Efficacy of First and Second Generation Somatostatin Receptor Ligands in Neuroendocrine Neoplasms. Int. J. Mol. Sci. 2019, 20, 3940. [Google Scholar] [CrossRef]
- Rorsman, P.; Huising, M.O. The Somatostatin-Secreting Pancreatic δ-Cell in Health and Disease. Nat. Rev. Endocrinol. 2018, 14, 404–414. [Google Scholar] [CrossRef]
- Asahara, S.I.; Inoue, H.; Watanabe, H.; Kido, Y. Roles of MTOR in the Regulation of Pancreatic β-Cell Mass and Insulin Secretion. Biomolecules 2022, 12, 614. [Google Scholar] [CrossRef]


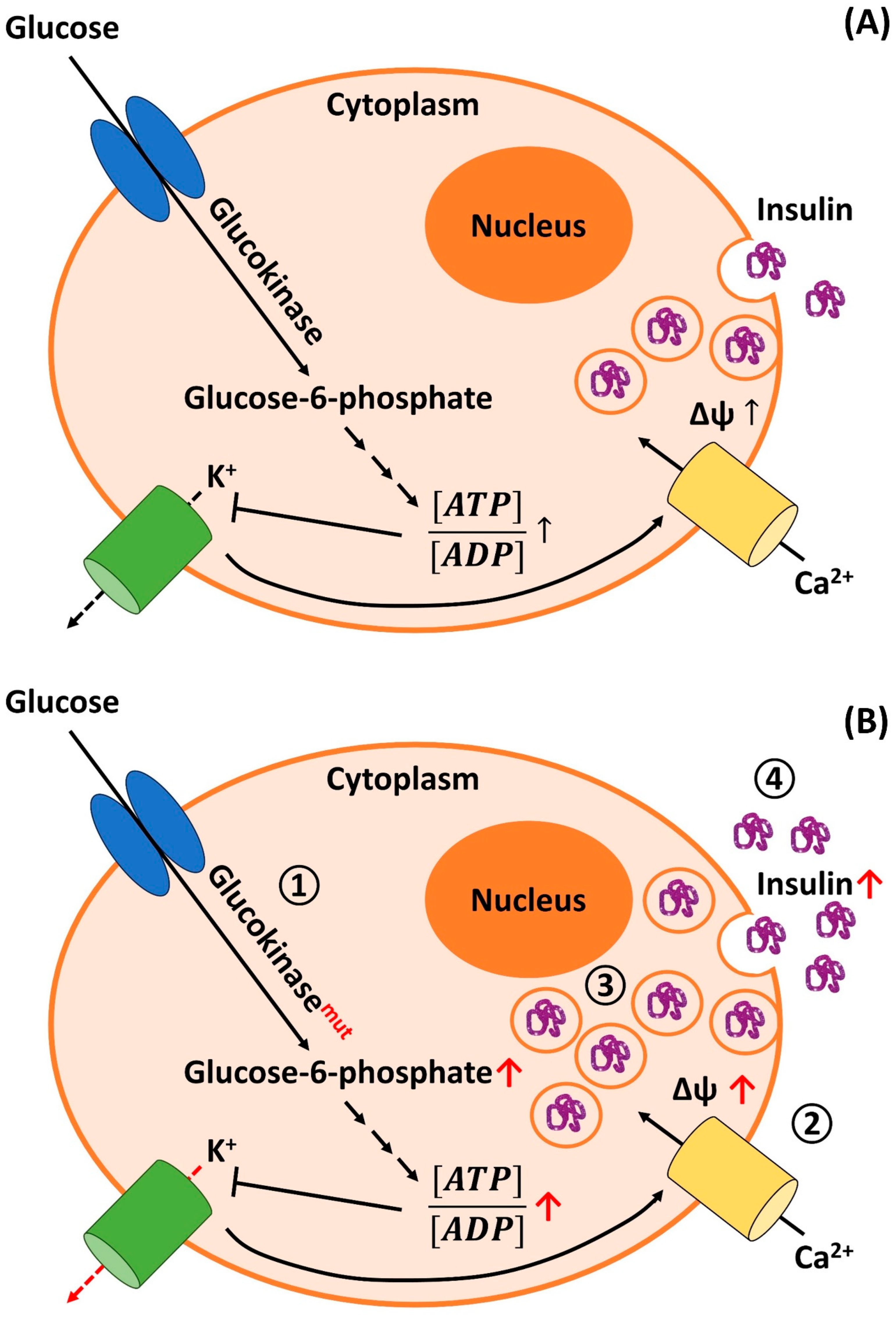{kind=link}
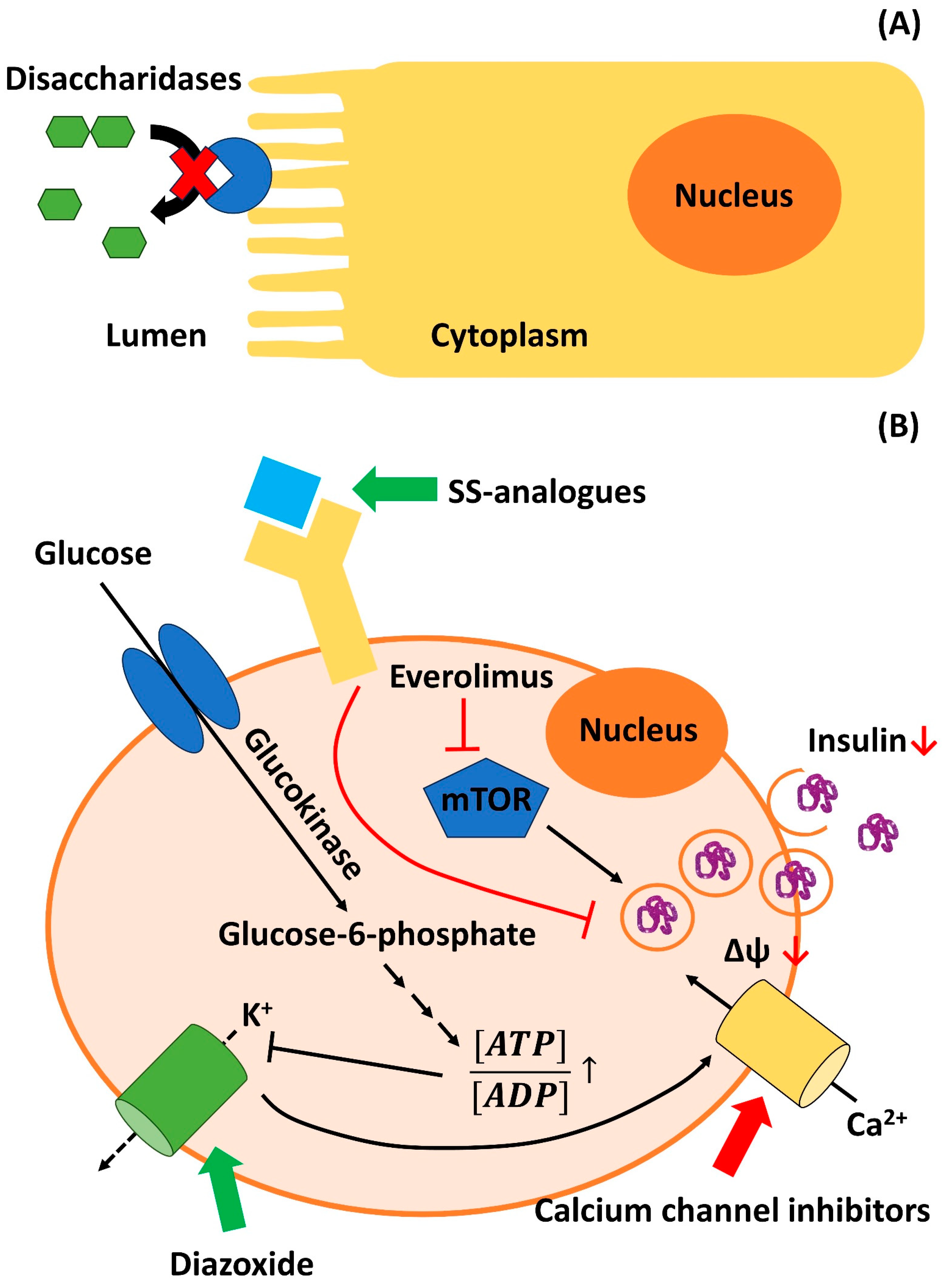{kind=link}
| Therapeutic Principle | Mechanism of Action 1 | Therapeutic Effect Based on the Current Literature 1 |
|---|---|---|
| Low carbohydrate diet/diet with low glycemic index | Limits insulin secretion postprandially due to low slope of glucose increase after food intake | Low but non-invasive |
| α-glucosidase inhibitors (Acarbose, Voglibose) | Slows down glucose resorption through inhibition of carbohydrate-digesting enzymes in the intestines | Low but non-invasive; few adverse effects |
| Diazoxide | Activates ATP-dependent potassium channels in β-cells → stabilizes resting membrane potential → inhibits insulin secretion | Sometimes effective; may have severe adverse effects (fluid retention, angina pectoris) |
| Calcium-channel antagonists (Verapamil, Amlodipine, Nifedipine) | Inhibit voltage-dependent calcium channels → inhibit depolarization of β-cells → inhibit insulin secretion | Sometimes effective; may have severe adverse effects (hypotension) |
| Somatostatin analogs (octreotide, lanreotide, pasireotide) | Stimulate somatostatin receptors (G-protein coupled receptors) on β-cells → inhibit insulin secretion | Sometimes effective; may lead to increased frequency/intensity of hypoglycemia (due to inhibition of glucagon; depends on receptor specificity) |
| Glucocorticoids | Induce gluconeogenesis and glycogenolysis in the liver; augment effects of glucagon; induce peripheral insulin resistance | Sometimes effective; long-term treatment associated with severe adverse effects |
| β-blockers (e.g., propranolol) | Mechanism not entirely clear (β1-adrenoceptor-mediated inhibition of insulin secretion?) | Rarely effective; β-blockers also tend to precipitate hypoglycemia (especially through inhibition of β2-adrenoceptor-dependent glycogenolysis) |
| Antipsychotics/Antiepileptics (e.g., phenytoin) | Probably through insulin insensitivity | Rarely effective; may have severe adverse effects |
| Everolimus | Inhibition of mammalian target of rapamycin (mTOR) signaling, which is involved in the regulation of insulin secretion | Rarely effective (more likely to be effective in the pediatric population [409]) |
| (Sub)total pancreatectomy | Surgical removal of the islets of Langerhans | Effective, if enough endocrine tissue is removed; considerable morbidity and mortality |
| Receptor-targeted photodynamic therapy | Selective destruction of GLP-1 receptor-expressing cells | Experimental treatment (animal model) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dieterle, M.P.; Husari, A.; Prozmann, S.N.; Wiethoff, H.; Stenzinger, A.; Röhrich, M.; Pfeiffer, U.; Kießling, W.R.; Engel, H.; Sourij, H.; et al. Diffuse, Adult-Onset Nesidioblastosis/Non-Insulinoma Pancreatogenous Hypoglycemia Syndrome (NIPHS): Review of the Literature of a Rare Cause of Hyperinsulinemic Hypoglycemia. Biomedicines 2023, 11, 1732. https://doi.org/10.3390/biomedicines11061732
Dieterle MP, Husari A, Prozmann SN, Wiethoff H, Stenzinger A, Röhrich M, Pfeiffer U, Kießling WR, Engel H, Sourij H, et al. Diffuse, Adult-Onset Nesidioblastosis/Non-Insulinoma Pancreatogenous Hypoglycemia Syndrome (NIPHS): Review of the Literature of a Rare Cause of Hyperinsulinemic Hypoglycemia. Biomedicines. 2023; 11(6):1732. https://doi.org/10.3390/biomedicines11061732
Chicago/Turabian StyleDieterle, Martin Philipp, Ayman Husari, Sophie Nicole Prozmann, Hendrik Wiethoff, Albrecht Stenzinger, Manuel Röhrich, Uwe Pfeiffer, Wolfgang Rüdiger Kießling, Helena Engel, Harald Sourij, and et al. 2023. "Diffuse, Adult-Onset Nesidioblastosis/Non-Insulinoma Pancreatogenous Hypoglycemia Syndrome (NIPHS): Review of the Literature of a Rare Cause of Hyperinsulinemic Hypoglycemia" Biomedicines 11, no. 6: 1732. https://doi.org/10.3390/biomedicines11061732
APA StyleDieterle, M. P., Husari, A., Prozmann, S. N., Wiethoff, H., Stenzinger, A., Röhrich, M., Pfeiffer, U., Kießling, W. R., Engel, H., Sourij, H., Steinberg, T., Tomakidi, P., Kopf, S., & Szendroedi, J. (2023). Diffuse, Adult-Onset Nesidioblastosis/Non-Insulinoma Pancreatogenous Hypoglycemia Syndrome (NIPHS): Review of the Literature of a Rare Cause of Hyperinsulinemic Hypoglycemia. Biomedicines, 11(6), 1732. https://doi.org/10.3390/biomedicines11061732