

IKs Activator ML277 Mildly Affects Repolarization and Arrhythmic Outcome in the CAVB Dog Model
 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Preparation
2.3. Compounds
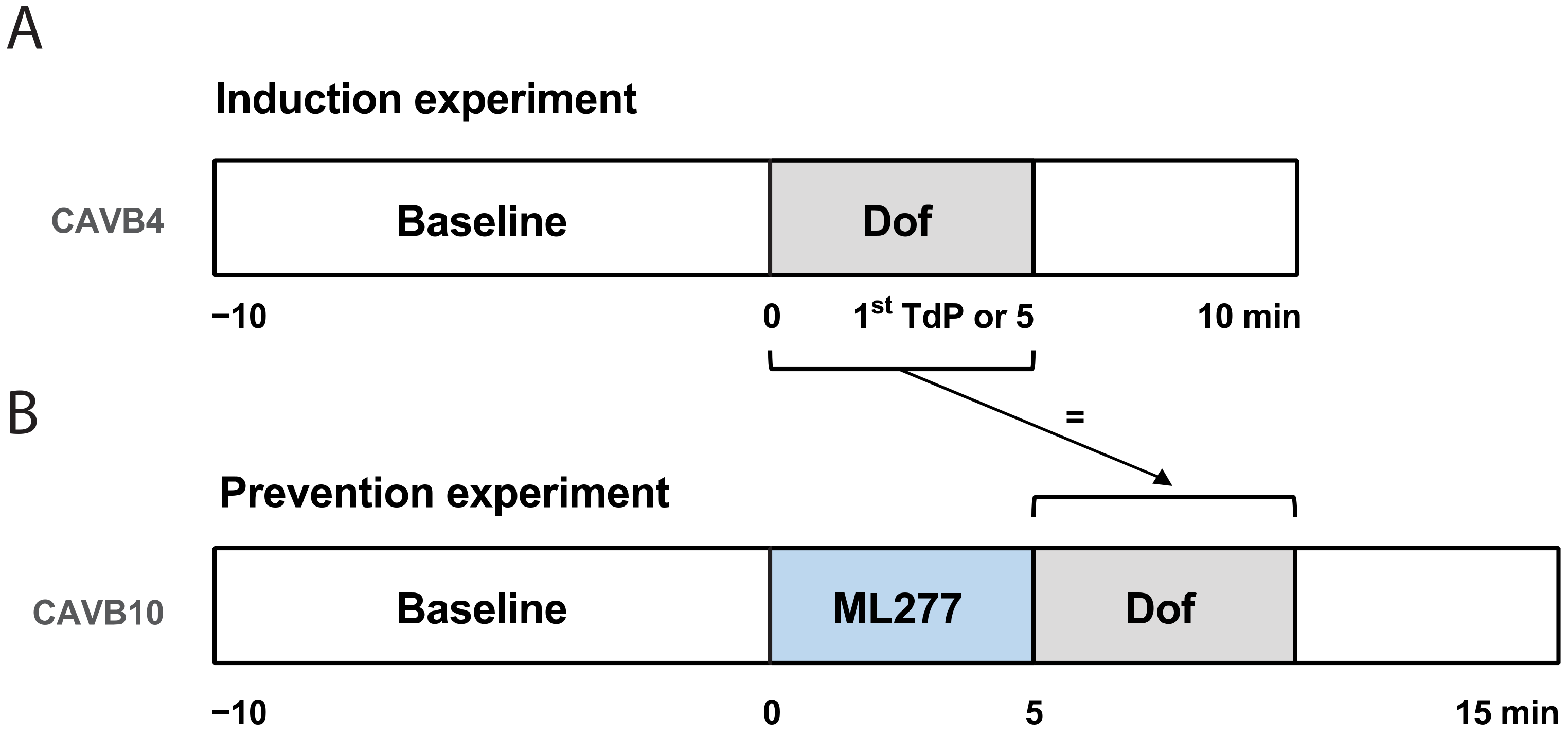
2.4. Induction Experiment
2.5. Prevention Experiment
2.6. Data Analysis
2.7. Statistical Analysis
3. Results
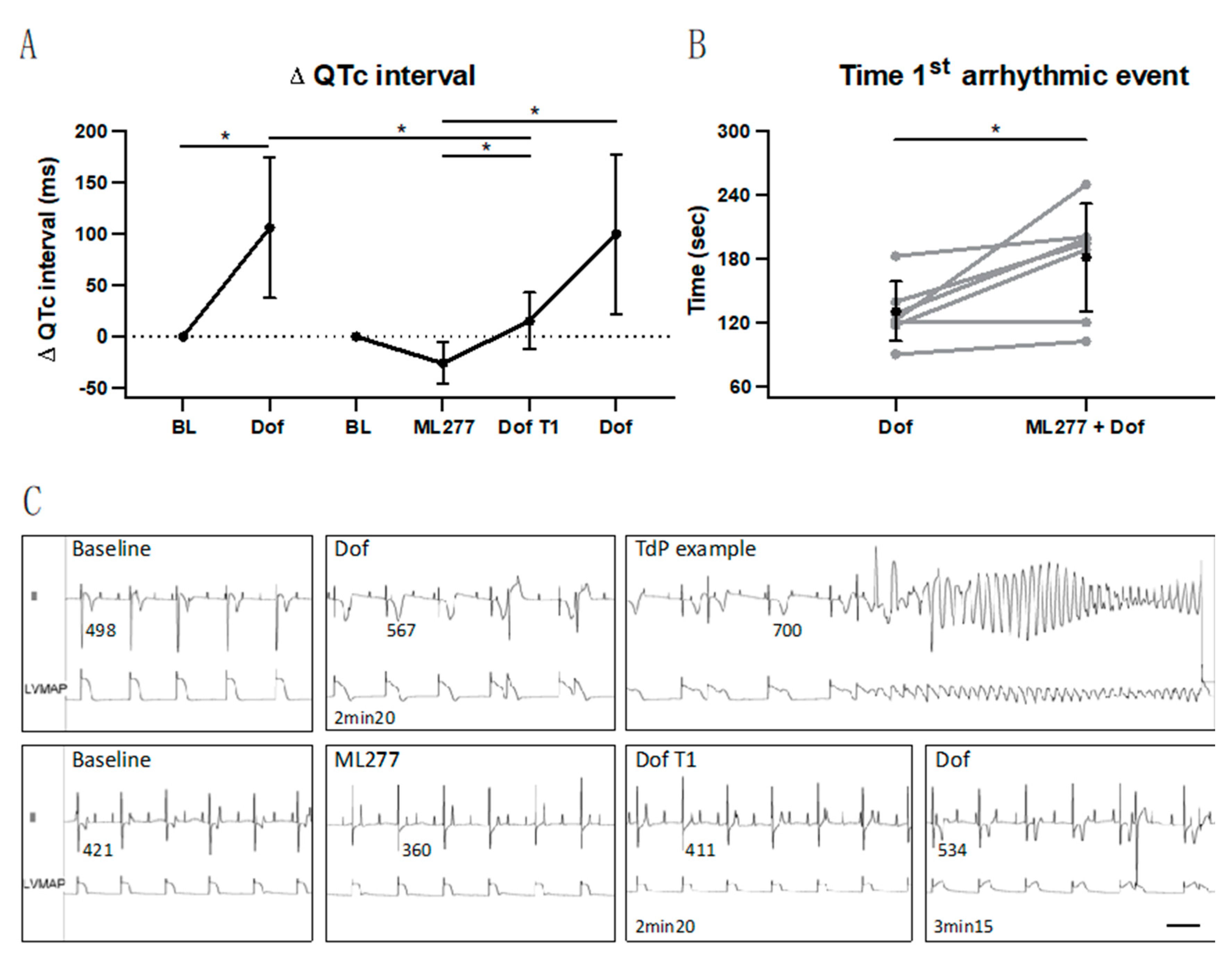
3.1. Temporary Suppression of Repolarization Prolongation
3.2. Delay in Occurrence of First Arrhythmic Event
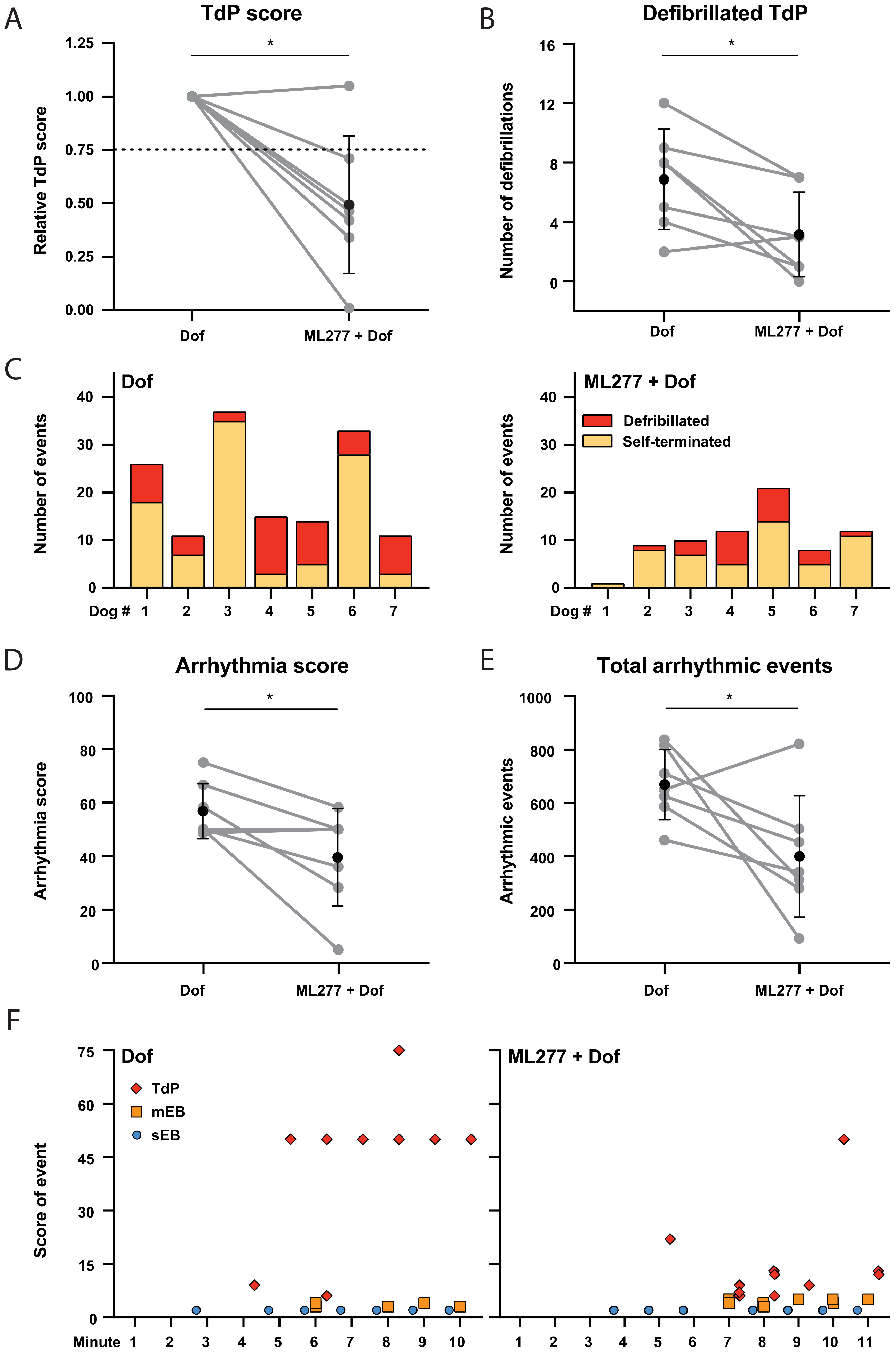
3.3. Mild Antiarrhythmic Effect: Occurrence of TdP Arrhythmias
4. Discussion
4.1. Targeting IKs in the CAVB Dog Model
4.2. Reproducibility of Dofetilide-Induced Arrhythmias
4.3. (Pre)Clinical Implications
4.4. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Napolitano, C.; Priori, S.G.; Schwartz, P.J.; Bloise, R.; Ronchetti, E.; Nastoli, J.; Bottelli, G.; Cerrone, M.; Leonardi, S. Genetic testing in the long QT syndrome: Development and validation of an efficient approach to genotyping in clinical practice. JAMA 2005, 294, 2975–2980. [Google Scholar] [CrossRef]
- Kapplinger, J.D.; Tester, D.J.; Salisbury, B.A.; Carr, J.L.; Harris-Kerr, C.; Pollevick, G.D.; Wilde, A.A.; Ackerman, M.J. Spectrum and prevalence of mutations from the first 2500 consecutive unrelated patients referred for the FAMILION long QT syndrome genetic test. Heart Rhythm 2009, 6, 1297–1303. [Google Scholar] [CrossRef]
- Banyasz, T.; Jian, Z.; Horvath, B.; Khabbaz, S.; Izu, L.T.; Chen-Izu, Y. Beta-adrenergic stimulation reverses the IKr-IKs dominant pattern during cardiac action potential. Pflug. Arch. 2014, 466, 2067–2076. [Google Scholar] [CrossRef]
- Volders, P.G.; Stengl, M.; Van Opstal, J.M.; Gerlach, U.; Spätjens, R.L.; Beekman, J.D.; Sipido, K.R.; Vos, M.A. Probing the contribution of IKs to canine ventricular repolarization: Key role for beta-adrenergic receptor stimulation. Circulation 2003, 107, 2753–2760. [Google Scholar] [CrossRef]
- Dvir, M.; Peretz, A.; Haitin, Y.; Attali, B. Recent molecular insights from mutated IKs channels in cardiac arrhythmia. Curr. Opin. Pharmacol. 2014, 15, 74–82. [Google Scholar] [CrossRef]
- Chen, S.; Zhang, L.; Bryant, R.; Vincent, G.; Flippin, M.; Lee, J.; Brown, E.; Zimmerman, F.; Rozich, R.; Szafranski, P.; et al. KCNQ1 mutations in patients with a family history of lethal cardiac arrhythmias and sudden death. Clin. Genet. 2003, 63, 273–282. [Google Scholar] [CrossRef]
- Zheng, Y.; Zhu, X.; Zhou, P.; Lan, X.; Xu, H.; Li, M.; Gao, Z. Hexachlorophene is a potent KCNQ1/KCNE1 potassium channel activator which rescues LQTs mutants. PLoS ONE 2012, 7, e51820. [Google Scholar] [CrossRef]
- Gao, Z.; Xiong, Q.; Sun, H.; Li, M. Desensitization of chemical activation by auxiliary subunits: Convergence of molecular determinants critical for augmenting KCNQ1 potassium channels. J. Biol. Chem. 2008, 283, 22649–22658. [Google Scholar] [CrossRef]
- Nissen, J.D.; Diness, J.G.; Diness, T.G.; Hansen, R.S.; Grunnet, M.; Jespersen, T. Pharmacologically induced long QT type 2 can be rescued by activation of IKs with benzodiazepine R-L3 in isolated guinea pig cardiomyocytes. J. Cardiovasc. Pharmacol. 2009, 54, 169–177. [Google Scholar] [CrossRef]
- Wu, X.; Larsson, H.P. Insights into cardiac IKs (KCNQ1/KCNE1) channels regulation. Int. J. Mol. Sci. 2020, 21, 9440. [Google Scholar] [CrossRef]
- Mattmann, M.E.; Yu, H.; Lin, Z.; Xu, K.; Huang, X.; Long, S.; Wu, M.; McManus, O.B.; Engers, D.W.; Le, U.M.; et al. Identification of (R)-N-(4-(4-methoxyphenyl)thiazol-2-yl)-1-tosylpiperidine-2-carboxamide, ML277, as a novel, potent and selective K(v)7.1 (KCNQ1) potassium channel activator. Bioorg. Med. Chem. Lett. 2012, 22, 5936–5941. [Google Scholar] [CrossRef]
- Xu, Y.; Wang, Y.; Zhang, M.; Jiang, M.; Rosenhouse-Dantsker, A.; Wassenaar, T.; Tseng, G.-N. Probing binding sites and mechanisms of action of an I(Ks) activator by computations and experiments. Biophys. J. 2015, 108, 62–75. [Google Scholar] [CrossRef]
- Hou, P.; Shi, J.; White, K.M.; Gao, Y.; Cui, J. ML277 specifically enhances the fully activated open state of KCNQ1 by modulating VSD-pore coupling. Elife 2019, 8, e48576. [Google Scholar] [CrossRef]
- Willegems, K.; Eldstrom, J.; Kyriakis, E.; Ataei, F.; Sahakyan, H.; Dou, Y.; Russo, S.; Van Petegem, F.; Fedida, D. Structural and electrophysiological basis for the modulation of KCNQ1 channel currents by ML277. Nat. Commun. 2022, 13, 3760. [Google Scholar] [CrossRef]
- Yu, H.; Lin, Z.; Mattmann, M.E.; Zou, B.; Terrenoire, C.; Zhang, H.; Wu, M.; McManus, O.B.; Kass, R.S.; Lindsley, C.W.; et al. Dynamic subunit stoichiometry confers a progressive continuum of pharmacological sensitivity by KCNQ potassium channels. Proc. Natl. Acad. Sci. USA 2013, 110, 8732–8737. [Google Scholar] [CrossRef]
- Ma, D.; Wei, H.; Lu, J.; Huang, D.; Liu, Z.; Loh, L.J.; Islam, O.; Liew, R.; Shim, W.; Cook, S.A. Characterization of a novel KCNQ1 mutation for type 1 long QT syndrome and assessment of the therapeutic potential of a novel IKs activator using patient-specific induced pluripotent stem cell-derived cardiomyocytes. Stem Cell Res. Ther. 2015, 6, 39. [Google Scholar] [CrossRef]
- Kuusela, J.; Kim, J.; Rasanen, E.; Aalto-Setala, K. The effects of pharmacological compounds on beat rate variations in human long QT-syndrome cardiomyocytes. Stem Cell Rev. Rep. 2016, 12, 698–707. [Google Scholar] [CrossRef]
- Loen, V.; Vos, M.A.; Van der Heyden, M.A.G. The canine chronic atrioventricular block model in cardiovascular preclinical drug research. Br. J. Pharmacol. 2022, 179, 859–881. [Google Scholar] [CrossRef]
- Vos, M.A.; De Groot, S.H.M.; Verduyn, S.C.; Van Der Zande, J.; Leunissen, H.D.M.; Cleutjens, J.P.M.; Van Bilsen, M.; Daemen, M.J.A.P.; Schreuder, J.J.; Allessie, M.A.; et al. Enhanced susceptibility for acquired torsade de pointes arrhythmias in the dog with chronic, complete AV block is related to cardiac hypertrophy and electrical remodeling. Circulation 1998, 98, 1125–1135. [Google Scholar] [CrossRef]
- Bourgonje, V.J.A.; Van Veen, T.A.B.; Vos, M.A. Ventricular electrical remodeling in compensated cardiac hypertrophy. In Electrical Diseases of the Heart; Gussak, I., Antzelevitch, C., Eds.; Springer: London, UK, 2013; pp. 387–398. [Google Scholar]
- Timmermans, C.; Rodriguez, L.M.; Van Suylen, R.J.; Leunissen, J.; Vos, M.; Ayers, G.M.; Crijns, H.J.; Wellens, H.J. Catheter-based cryoablation produces permanent bidirectional cavotricuspid isthmus conduction block in dogs. J. Interv. Card. Electrophysiol. 2002, 7, 149–155. [Google Scholar] [CrossRef]
- Van de Water, A.; Verheyen, J.; Xhonneux, R.; Reneman, R.S. An improved method to correct the QT interval of the electrocardiogram for changes in heart rate. J. Pharmacol. Methods 1989, 22, 207–217. [Google Scholar] [CrossRef]
- Thomsen, M.B.; Verduyn, S.C.; Stengl, M.; Beekman, J.D.; de Pater, G.; Van Opstal, J.; Volders, P.G.; Vos, M.A. Increased short-term variability of repolarization predicts d-sotalol-induced torsades de pointes in dogs. Circulation 2004, 110, 2453–2459. [Google Scholar] [CrossRef]
- Stams, T.R.G.; Winckels, S.K.G.; Oros, A.; Varkevisser, R.; Oosterhoff, P.; Van der Nagel, R.; Beekman, H.D.M.; Vos, M.A. Novel parameters to improve quantification of repolarization reserve and arrhythmogenesis using a dofetilide challenge. Heart Rhythm 2013, 10, 1745–1746. [Google Scholar] [CrossRef]
- Jost, N.; Virág, L.; Comtois, P.; Ördög, B.; Szuts, V.; Seprényi, G.; Bitay, M.; Kohajda, Z.; Koncz, I.; Nagy, N.; et al. Ionic mechanisms limiting cardiac repolarization reserve in humans compared to dogs. J. Physiol. 2013, 591, 4189–4206. [Google Scholar] [CrossRef]
- Volders, P.G.; Sipido, K.R.; Vos, M.A.; Spätjens, R.L.; Leunissen, J.D.; Carmeliet, E.; Wellens, H.J. Downregulation of delayed rectifier K+ currents in dogs with chronic complete atrioventricular block and acquired torsades de pointes. Circulation 1999, 100, 2455–2461. [Google Scholar] [CrossRef] [PubMed]
- Van Bavel, J.J.A.; Beekman, H.D.M.; Van Weperen, V.Y.H.; Van der Linde, H.J.; Van der Heyden, M.A.G.; Vos, M.A. I(Ks) inhibitor JNJ303 prolongs the QT interval and perpetuates arrhythmia when combined with enhanced inotropy in the CAVB dog. Eur. J. Pharmacol. 2022, 932, 175218. [Google Scholar] [CrossRef]
- Suzuki, A.; Bosnjak, Z.J.; Kwok, W.M. The effects of isoflurane on the cardiac slowly activating delayed-rectifier potassium channel in Guinea pig ventricular myocytes. Anesth. Analg. 2003, 96, 1308–1315. [Google Scholar] [CrossRef]
- Bossu, A.; Varkevisser, R.; Beekman, H.D.M.; Houtman, M.J.C.; Van der Heyden, M.A.G.; Vos, M.A. Short-term variability of repolarization is superior to other repolarization parameters in the evaluation of diverse antiarrhythmic interventions in the chronic atrioventricular block dog. J. Cardiovasc. Pharmacol. 2017, 69, 398–407. [Google Scholar] [CrossRef] [PubMed]
- Oros, A.; Beekman, J.D.; Vos, M.A. The canine model with chronic, complete atrio-ventricular block. Pharmacol. Ther. 2008, 119, 168–178. [Google Scholar] [CrossRef]
- Stengl, M.; Ramakers, C.; Donker, D.W.; Nabar, A.; Rybin, A.V.; Spätjens, R.L.; Van der Nagel, T.; Wodzig, W.K.; Sipido, K.R.; Antoons, G.; et al. Temporal patterns of electrical remodeling in canine ventricular hypertrophy: Focus on IKs downregulation and blunted beta-adrenergic activation. Cardiovasc. Res. 2006, 72, 90–100. [Google Scholar] [CrossRef] [PubMed]
- Dunnink, A.; Sharif, S.; Oosterhoff, P.; Winckels, S.; Montagne, D.; Beekman, J.; Van der Nagel, R.; Van der Heyden, M.; A Vos, M. Anesthesia and arrhythmogenesis in the chronic atrioventricular block dog model. J. Cardiovasc. Pharmacol. 2010, 55, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Van Weperen, V.Y.H.; Bossu, A.; Vos, M.A. Point of View: Electrophysiological endpoints differ when comparing the mode of action of highly successful anti-arrhythmic drugs in the CAVB dog model with TdP. J. Cardiovasc. Pharmacol. 2019, 74, 499–507. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Induction | Prevention | |||||
|---|---|---|---|---|---|---|
| BL | Dof | BL | ML277 | Dof T1 | Dof | |
| RR | 1275 ± 190 | 1285 ± 180 | 1322 ± 242 | 1399 ± 299 | 1398 ± 301 | 1432 ± 290 |
| PP | 583 ± 113 | 638 ± 101 | 577 ± 101 | 596 ± 114 | 611 ± 102 | 672 ± 143 * |
| QRS | 104 ± 21 | 102 ± 27 | 107 ± 24 | 107 ± 25 | 104 ± 27 | 103 ± 29 |
| QT | 456 ± 93 | 563 ± 70 * | 406 ± 40 | 387 ± 36 | 428 ± 27 # | 516 ± 77 *&% |
| QTc | 432 ± 84 | 538 ± 65 * | 378 ± 26 | 352 ± 31 | 393 ± 18 # | 479 ± 82 *&% |
| JTc | 327 ± 74 | 436 ± 47 * | 272 ± 40 | 245 ± 34 | 289 ± 19 # | 376 ± 59 *&% |
| LV MAPD | 308 ± 41 | 399 ± 77 * | 278 ± 20 | 274 ± 26 | 315 ± 24 # | 389 ± 53 *&% |
| STV | 1.63 ± 0.50 | 2.97 ± 0.91 | 0.78 ± 0.56 | 0.73 ± 0.33 | 0.85 ± 0.41 | 2.31 ± 1.44 *& |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Bavel, J.J.A.; Beekman, H.D.M.; Smoczyńska, A.; van der Heyden, M.A.G.; Vos, M.A. IKs Activator ML277 Mildly Affects Repolarization and Arrhythmic Outcome in the CAVB Dog Model. Biomedicines 2023, 11, 1147. https://doi.org/10.3390/biomedicines11041147
van Bavel JJA, Beekman HDM, Smoczyńska A, van der Heyden MAG, Vos MA. IKs Activator ML277 Mildly Affects Repolarization and Arrhythmic Outcome in the CAVB Dog Model. Biomedicines. 2023; 11(4):1147. https://doi.org/10.3390/biomedicines11041147
Chicago/Turabian Stylevan Bavel, Joanne J. A., Henriëtte D. M. Beekman, Agnieszka Smoczyńska, Marcel A. G. van der Heyden, and Marc A. Vos. 2023. "IKs Activator ML277 Mildly Affects Repolarization and Arrhythmic Outcome in the CAVB Dog Model" Biomedicines 11, no. 4: 1147. https://doi.org/10.3390/biomedicines11041147
APA Stylevan Bavel, J. J. A., Beekman, H. D. M., Smoczyńska, A., van der Heyden, M. A. G., & Vos, M. A. (2023). IKs Activator ML277 Mildly Affects Repolarization and Arrhythmic Outcome in the CAVB Dog Model. Biomedicines, 11(4), 1147. https://doi.org/10.3390/biomedicines11041147