

Abdominal Aortic Aneurysm Diameter versus Volume: A Systematic Review

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
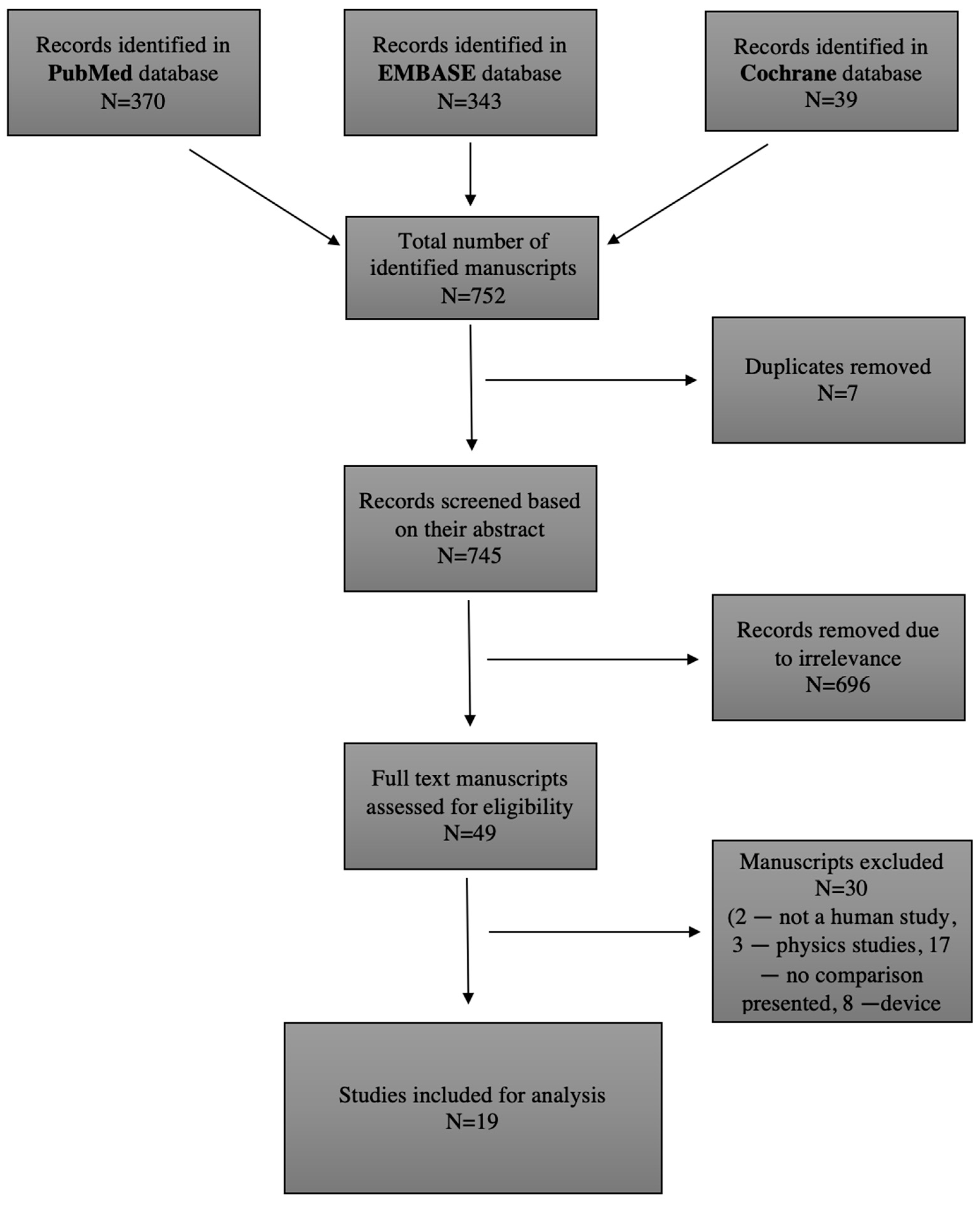
2.1. Literature Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Types of Studies
2.4. Types of Participants
2.5. Types of Outcomes
2.6. Data Extraction and Critical Appraisal
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wanhainen, A.; Verzini, F.; Van Herzeele, I.; Allaire, E.; Bown, M.; Cohnert, T.; Dick, F.; van Herwaarden, J.; Karkos, C.; Koelemay, M.; et al. Editor’s Choice—European Society for Vascular Surgery (ESVS) 2019 Clinical Practice Guidelines on the Management of Abdominal Aorto-Iliac Artery Aneurysms. Eur. J. Vasc. Endovasc. Surg. 2019, 57, 8–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Long, A.; Rouet, L.; Lindholt, J.S.; Allaire, E. Measuring the Maximum Diameter of Native Abdominal Aortic Aneurysms: Review and Critical Analysis. Eur. J. Vasc. Endovasc. Surg. 2012, 43, 515–524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaikof, E.L.; Dalman, R.L.; Eskandari, M.K.; Jackson, B.M.; Lee, W.A.; Mansour, M.A.; Mastracci, T.M.; Mell, M.; Murad, M.H.; Nguyen, L.L.; et al. The Society for Vascular Surgery Practice Guidelines on the Care of Patients with an Abdominal Aortic Aneurysm. J. Vasc. Surg. 2018, 67, 2–77.e2. [Google Scholar] [CrossRef] [Green Version]
- Ricco, J.-B.; Forbes, T.L. Trans-Atlantic Debate: External Diameter for Abdominal Aortic Aneurysm (AAA) Size versus Volume. Eur. J. Vasc. Endovasc. Surg. Off. J. Eur. Soc. Vasc. Surg. 2013, 46, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kontopodis, N.; Metaxa, E.; Papaharilaou, Y.; Georgakarakos, E.; Tsetis, D.; Ioannou, C.V. Value of Volume Measurements in Evaluating Abdominal Aortic Aneurysms Growth Rate and Need for Surgical Treatment. Eur. J. Radiol. 2014, 83, 1051–1056. [Google Scholar] [CrossRef] [PubMed]
- Spanos, K.; Nana, P.; Kouvelos, G.; Mpatzalexis, K.; Matsagkas, M.; Giannoukas, A.D. Anatomical Differences Between Intact and Ruptured Large Abdominal Aortic Aneurysms. J. Endovasc. Ther. 2020, 27, 117–123. [Google Scholar] [CrossRef]
- Singh, T.P.; Moxon, J.V.; Gasser, T.C.; Golledge, J. Systematic Review and Meta-Analysis of Peak Wall Stress and Peak Wall Rupture Index in Ruptured and Asymptomatic Intact Abdominal Aortic Aneurysms. J. Am. Heart Assoc. 2021, 10, e019772. [Google Scholar] [CrossRef]
- von Allmen, R.S.; Powell, J.T. Part Two: Against the Motion. External Diameter for AAA Size. Eur. J. Vasc. Endovasc. Surg. 2013, 46, 6–8. [Google Scholar] [CrossRef] [Green Version]
- Ghulam, Q.M.; Bredahl, K.K.; Lönn, L.; Rouet, L.; Sillesen, H.H.; Eiberg, J.P. Follow-up on Small Abdominal Aortic Aneurysms Using Three Dimensional Ultrasound: Volume Versus Diameter. Eur. J. Vasc. Endovasc. Surg. Off. J. Eur. Soc. Vasc. Surg. 2017, 54, 439–445. [Google Scholar] [CrossRef] [Green Version]
- van Keulen, J.W.; van Prehn, J.; Prokop, M.; Moll, F.L.; van Herwaarden, J.A. Potential Value of Aneurysm Sac Volume Measurements in Addition to Diameter Measurements after Endovascular Aneurysm Repair. J. Endovasc. Ther. Off. J. Int. Soc. Endovasc. Spec. 2009, 16, 506–513. [Google Scholar] [CrossRef]
- Caradu, C.; Pouncey, A.-L.; Lakhlifi, E.; Brunet, C.; Bérard, X.; Ducasse, E. Fully Automatic Volume Segmentation Using Deep Learning Approaches to Assess Aneurysmal Sac Evolution after Infrarenal Endovascular Aortic Repair. J. Vasc. Surg. 2022, 76, 620–630.E3. [Google Scholar] [CrossRef] [PubMed]
- Adam, C.; Fabre, D.; Mougin, J.; Zins, M.; Azarine, A.; Ardon, R.; d’Assignies, G.; Haulon, S. Pre-Surgical and Post-Surgical Aortic Aneurysm Maximum Diameter Measurement: Full Automation by Artificial Intelligence. Eur. J. Vasc. Endovasc. Surg. Off. J. Eur. Soc. Vasc. Surg. 2021, 62, 869–877. [Google Scholar] [CrossRef] [PubMed]
- Schiavo, J.H. PROSPERO: An International Register of Systematic Review Protocols. Med. Ref. Serv. Q. 2019, 38, 171–180. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological Index for Non-Randomized Studies ( MINORS): Development and Validation of a New Instrument: Methodological Index for Non-Randomized Studies. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef] [PubMed]
- Wolf, Y.G.; Tillich, M.; Lee, W.A.; Fogarty, T.J.; Zarins, C.K.; Rubin, G.D. Changes in Aneurysm Volume after Endovascular Repair of Abdominal Aortic Aneurysm. J. Vasc. Surg. 2002, 36, 305–309. [Google Scholar] [CrossRef] [Green Version]
- Skrebunas, A.; Lengvenis, G.; Builyte, I.; Zulpaite, R.; Bliudzius, R.; Baltrunas, T.; Misonis, N.; Marinskis, G. Aortic Sac Enlargement after Endovascular Aneurysm Repair: Volume-Related Changes and the Impact of Intraluminal Thrombus. Pol. J. Radiol. 2019, 84, 530–536. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.; Rogers, S.; Carreira, J.; Ghosh, J.; McCollum, C. Aneurysm Geometry Analyzed by the Novel Three-Dimensional Tomographic Ultrasound Relates to Abdominal Aortic Aneurysm Growth. Ann. Vasc. Surg. 2022, 87, 469–477. [Google Scholar] [CrossRef]
- Quan, C.; Oh, Y.K.; Park, S.C.; Won, Y.S.; Yun, S.S.; Suh, Y.J.; Kim, J.Y. Efficacy of Volumetric Analysis of Aorta as Surveillance Tool after EVAR. Asian J. Surg. 2019, 42, 746–754. [Google Scholar] [CrossRef]
- Bargellini, I.; Cioni, R.; Petruzzi, P.; Pratali, A.; Napoli, V.; Vignali, C.; Ferrari, M.; Bartolozzi, C. Endovascular Repair of Abdominal Aortic Aneurysms: Analysis of Aneurysm Volumetric Changes at Mid-Term Follow-Up. Cardiovasc. Intervent. Radiol. 2005, 28, 426–433. [Google Scholar] [CrossRef]
- Fillinger, M. Three-Dimensional Analysis of Enlarging Aneurysms after Endovascular Abdominal Aortic Aneurysm Repair in the Gore Excluder Pivotal Clinical Trial. J. Vasc. Surg. 2006, 43, 888–895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wever, J.J.; Blankensteijn, J.D.; Mali, W.T.M.; Eikelboom, B.C. Maximal Aneurysm Diameter Follow-up Is Inadequate after Endovascular Abdominal Aortic Aneurysm Repair. Eur. J. Vasc. Endovasc. Surg. Off. J. Eur. Soc. Vasc. Surg. 2000, 20, 177–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parr, A.; Jayaratne, C.; Buttner, P.; Golledge, J. Comparison of Volume and Diameter Measurement in Assessing Small Abdominal Aortic Aneurysm Expansion Examined Using Computed Tomographic Angiography. Eur. J. Radiol. 2011, 79, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Schnitzbauer, M.; Güntner, O.; Wohlgemuth, W.A.; Zeman, F.; Haimerl, M.; Stroszczynski, C.; Müller-Wille, R. CT after Endovascular Repair of Abdominal Aortic Aneurysms: Diagnostic Accuracy of Diameter Measurements for the Detection of Aneurysm Sac Enlargement. J. Vasc. Interv. Radiol. 2018, 29, 178–187.e3. [Google Scholar] [CrossRef]
- Olson, S.L.; Panthofer, A.M.; Blackwelder, W.; Terrin, M.L.; Curci, J.A.; Baxter, B.T.; Weaver, F.A.; Matsumura, J.S. Role of Volume in Small Abdominal Aortic Aneurysm Surveillance. J. Vasc. Surg. 2022, 75, 1260–1267.e3. [Google Scholar] [CrossRef]
- Tzirakis, K.; Kontopodis, N.; Metaxa, E.; Ioannou, C.V.; Papaharilaou, Y. Spatial Distribution of Abdominal Aortic Aneurysm Surface Expansion and Correlation With Maximum Diameter and Volume Growth. Ann. Vasc. Surg. 2019, 58, 276–288. [Google Scholar] [CrossRef]
- Lindquist Liljeqvist, M.; Hultgren, R.; Gasser, T.C.; Roy, J. Volume Growth of Abdominal Aortic Aneurysms Correlates with Baseline Volume and Increasing Finite Element Analysis-Derived Rupture Risk. J. Vasc. Surg. 2016, 63, 1434–1442.e3. [Google Scholar] [CrossRef] [Green Version]
- Renapurkar, R.D.; Setser, R.M.; O’Donnell, T.P.; Egger, J.; Lieber, M.L.; Desai, M.Y.; Stillman, A.E.; Schoenhagen, P.; Flamm, S.D. Aortic Volume as an Indicator of Disease Progression in Patients with Untreated Infrarenal Abdominal Aneurysm. Eur. J. Radiol. 2012, 81, e87–e93. [Google Scholar] [CrossRef]
- Franchin, M.; Serafini, M.; Tadiello, M.; Fontana, F.; Rivolta, N.; Venturini, M.; Curti, M.; Bush, R.L.; Dorigo, W.; Piacentino, F.; et al. A Morphovolumetric Analysis of Aneurysm Sac Evolution after Elective Endovascular Abdominal Aortic Repair. J. Vasc. Surg. 2021, 74, 1222–1231.e2. [Google Scholar] [CrossRef]
- Kritpracha, B.; Beebe, H.G.; Comerota, A.J. Aortic Diameter Is an Insensitive Measurement of Early Aneurysm Expansion After Endografting. J. Endovasc. Ther. 2004, 11, 184–190. [Google Scholar] [CrossRef]
- Raghavan, M.L.; Vorp, D.A.; Federle, M.P.; Makaroun, M.S.; Webster, M.W. Wall Stress Distribution on Three-Dimensionally Reconstructed Models of Human Abdominal Aortic Aneurysm. J. Vasc. Surg. 2000, 31, 760–769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meyrignac, O.; Bal, L.; Zadro, C.; Vavasseur, A.; Sewonu, A.; Gaudry, M.; Saint-Lebes, B.; De Masi, M.; Revel-Mouroz, P.; Sommet, A.; et al. Combining Volumetric and Wall Shear Stress Analysis from CT to Assess Risk of Abdominal Aortic Aneurysm Progression. Radiology 2020, 295, 722–729. [Google Scholar] [CrossRef] [PubMed]
- Qiu, Y.; Yuan, D.; Wen, J.; Fan, Y.; Zheng, T. Numerical Identification of the Rupture Locations in Patient-Specific Abdominal Aortic Aneurysmsusing Hemodynamic Parameters. Comput. Methods Biomech. Biomed. Eng. 2018, 21, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Boyd, A.J.; Kuhn, D.C.S.; Lozowy, R.J.; Kulbisky, G.P. Low Wall Shear Stress Predominates at Sites of Abdominal Aortic Aneurysm Rupture. J. Vasc. Surg. 2016, 63, 1613–1619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teng, B.; Zhou, Z.; Zhao, Y.; Wang, Z. Combined Curvature and Wall Shear Stress Analysis of Abdominal Aortic Aneurysm: An Analysis of Rupture Risk Factors. Cardiovasc. Intervent. Radiol. 2022, 45, 752–760. [Google Scholar] [CrossRef] [PubMed]
- Crawford, J.D.; Chivukula, V.K.; Haller, S.; Vatankhah, N.; Bohannan, C.J.; Moneta, G.L.; Rugonyi, S.; Azarbal, A.F. Aortic Outflow Occlusion Predicts Rupture of Abdominal Aortic Aneurysm. J. Vasc. Surg. 2016, 64, 1623–1628. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| 1. Publications regarding diameter and volume measurement in diagnosis and prognosis of AAA | 1. Investigation of a different morphological criteria |
| 2. Manuscripts in English, German, and Russian | 2. Only abstract available |
| 3. Human studies | 3. Physiology reviews |
| 4. Full text available | 4. Studies with the physical background |
| 5. Case series and case reports |
| Study | A Clearly Stated Aim | Inclusion of Consecutive Patients | Prospective Collection of Data | Endpoints Appropriate to the Aims of Study | Unbiased Assessment of the Study Endpoint | Follow-Up Period Appropriate to the Aim of the Study | Loss to Follow-Up Less Than 5% | Prospective Calculation of the Study Size | An Adequate Control Group | Contemporary Groups | Baseline Equivalence of Groups | Adequate Statistical Analyses | Total Max NON RCT 16, RCT 24 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Wolf et al. (2002) [16] | 2 | 2 | 1 | 2 | 2 | 1 | 1 | 0 | n/a | n/a | n/a | n/a | 11 |
| Skrebunas et al. (2019) [17] | 2 | 1 | 2 | 1 | 0 | 2 | 0 | 2 | n/a | n/a | n/a | n/a | 10 |
| Ghulam et al. (2017) [9] | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 2 | n/a | n/a | n/a | n/a | 15 |
| Khan et al. (2022) [18] | 2 | 2 | 1 | 1 | 2 | 2 | 2 | 2 | n/a | n/a | n/a | n/a | 14 |
| Quan et al. (2019) [19] | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 0 | n/a | n/a | n/a | n/a | 13 |
| Bargellini et al. (2005) [20] | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 0 | n/a | n/a | n/a | n/a | 12 |
| Fillinger et al. (2006) [21] | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 0 | n/a | n/a | n/a | n/a | 12 |
| Wever et al. (2000) [22] | 2 | 2 | 1 | 1 | 2 | 2 | 1 | 2 | n/a | n/a | n/a | n/a | 13 |
| Parr et al. (2013) [23] | 2 | 2 | 2 | 2 | 2 | 1 | 2 | 0 | n/a | n/a | n/a | n/a | 13 |
| Schnitzbauer et al. (2018) [24] | 2 | 2 | 0 | 2 | 2 | 1 | 2 | 0 | n/a | n/a | n/a | n/a | 11 |
| Olson et al. (2022) [25] | 1 | 1 | 2 | 1 | 0 | 2 | 2 | 2 | n/a | n/a | n/a | n/a | 11 |
| Tzirakis et al. (2019) [26] | 2 | 2 | 0 | 2 | 2 | 1 | 2 | 0 | n/a | n/a | n/a | n/a | 11 |
| Kontopodis et al. (2014) [5] | 2 | 2 | 0 | 2 | 2 | 1 | 2 | 0 | n/a | n/a | n/a | n/a | 11 |
| Spanos et al. (2020) [6] | 2 | 2 | 0 | 2 | 2 | 0 | 0 | 0 | 2 | 2 | 2 | 2 | 16 |
| Liljeqvist et al. (2016) [27] | 2 | 2 | 0 | 2 | 2 | 1 | 2 | 0 | n/a | n/a | n/a | n/a | 11 |
| Renapurkar et al. (2012) [28] | 2 | 1 | 0 | 2 | 2 | 1 | 2 | 0 | n/a | n/a | n/a | n/a | 10 |
| Franchin et al. (2021) [29] | 2 | 1 | 2 | 1 | 0 | 1 | 2 | 1 | n/a | n/a | n/a | n/a | 10 |
| Kritpracha et al. (2004) [30] | 2 | 0 | 0 | 2 | 2 | 1 | 1 | 0 | n/a | n/a | n/a | n/a | 8 |
| Raghavan et al. (2000) [31] | 2 | 0 | 0 | 2 | 2 | 0 | 2 | 1 | 1 | 2 | 0 | 2 | 14 |
| Study | Country | Size | Inclusion Criteria | Imaging Modality | Results | MINORS Criteria |
|---|---|---|---|---|---|---|
| Wolf et al. (2002) * [16] | USA | 154 | Patients after elective EVAR of AAA | CTA | The predictive values of changes in volume for identifying the presence or absence of endoleak were not significantly different from those associated with changes in transverse or orthogonal diameter. | 11/16 |
| Skrebunas et al. (2019) [17] | Lithuania | 39 | Patients before and after elective EVAR of AAA | CTA | Diameter increased in 11 (28.2%) of 39, but volume increased in 12 (30.8%). A moderate positive linear correlation between diameter and volume (R2 = 0.731, p < 0.0001). A clinically irrelevant AAA diameter increase after EVAR was observed in 8 (72.7%) of 11 cases. The AAA volume changes were also evaluated in those cases. There was no statistically significant difference between diameter and volumetric AAA changes in those cases (p = 0.184). | 10/16 |
| Study | Country | Size | Inclusion Criteria | Imaging Modality | Results | MINORS Criteria |
|---|---|---|---|---|---|---|
| Ghulam et al. (2017) [9] | Denmark | 179 | Patients with small (30–55 mm) AAAs | US and 3D US | Post-hoc analysis of the time period between the end of follow-up and manuscript preparation revealed that 14 patients underwent aortic repair: 13 elective repair (EVAR: n = 9; open repair: n = 4) and one subacute EVAR because of a symptomatic AAA. In this time period, more patients with a previously stable diameter and growing volume were growing in diameter, and more patients from this group than patients with a stable diameter and stable volume underwent aortic repair (20% vs. 5%). | 15/16 |
| Khan et al. (2022) [18] | UK | 128 | Patients with AAAs (30–70 mm in diameter) | 3D US | AAA growth correlated more closely with AAA volume than diameter (r 0.46, p < 0.01). Aneurysm growth is most strongly related to AAA volume and inversely to wall volume, a more reliable way to measure wall thickness. A surveillance program that incorporates aneurysm volume and wall volume rather than just diameter may better inform surveillance intervals and surgical decisions. | 14/16 |
| Quan et al. (2019) * [19] | South Korea | 82 | Patients before and after EVAR of AAA | CTA and MRA | The enlargement rate of aortic volume was significantly different from the enlargement rate of Dmax (p = 0.02 by Wilcoxon rank-sum test). The occurrence of endoleaks between the Dmax-enlargement group and the no-enlargement group was significantly different (11, 100% vs. 19, 26.76%, p < 0.001). There was a significantly different rate of occurrence of endoleaks between the aortic volume enlargement group and the no-enlargement group (20, 90.91% vs. 10, 16.67%, p < 0.001). In the aortic volume enlargement group, there were more patients with endoleaks. | 13/16 |
| Bargellini et al. (2005) * [20] | Italy | 63 | Patients after EVAR of AAA | US, CTA | Endoleaks were found in 19 patients and were more frequent (p = 0.04) in patients with higher pre-procedural Dmax. The accuracy of volume changes in predicting endoleaks ranged between 74.6% and 84.1% and was higher than those of Dmax modifications. The strongest independent predictor of endoleak was a volume change at 6 months less than 0.3% (p = 0.005), although 6 of 19 (32%) patients with endoleak showed no significant AAA enlargement, whereas in 6 of 44 (14%) patients without endoleak the aneurysm enlarged. | 12/16 |
| Fillinger et al. (2006) [21] | USA | 112 | Patients with enlarging aneurysms (5-mm increase by Core laboratory or site) and at least 4 years of follow-up in the Excluder | CTA | A total of 38 AAAs (34%) were identified as enlarging. Of the 158 scans with a prior scan for comparison, 41% demonstrated growth relative to the initial scan by diameter criteria, but 79% demonstrated growth relative to the initial scan by 3-dimensional volume criteria. This difference was most evident at early time points: at 1 year, diameter criteria indicated that 8% of these AAAs were enlarging, but 56% were already enlarging by volume criteria. On average, enlargement was detected by volume 18 months before it was detected by diameter (18 vs. 36 months, p < 0.0001) and at a smaller diameter (55.4 mm vs. 59.8 mm; p < 0.0001). | 12/16 |
| Wever et al. (2000) * [22] | USA | 35 | Patients after EVAR of AAA | CTA | There was a poor correlation between the endoleak status and aneurysm growth, but the correlation between volume increase and endoleak was stronger (r = 0.37 at 6 months, r = 0.25 at 12 months) than the correlation between Dmax and endoleak (r = −0.07 and r = 0.11, respectively). | 13/16 |
| Parr et al. (2013) [23] | Australia | 57 | Patients with AAAs (25–55 mm in diameter) | CTA | A total of 42% of patients who had increased aortic volume above the upper 95% limit of agreement had no diameter change. | 13/16 |
| Schnitzbauer et al. (2018) * [24] | Germany | 100 | Patients after elective EVAR of AAA | CTA | The use of the reporting standard showed that the diameter measurements failed to detect aneurysm volume increase in 61–72% of cases with persistent type II endoleak. | 11/16 |
| Olson et al. (2022) [25] | USA | 250 | Patients with AAAs (35 mm to 50 mm male and 35–45 mm female) | CTA | The tortuosity index is associated with volume but not Dmax (difference 32.8 cm3/year, p < 0.001). Baseline volume accounted for more volume growth than Dmax (30% vs. 13%, p < 0.001). Predictors of volume growth: high baseline volume (regression coefficient 0.2, p < 0.001), tobacco use, tortuosity index (p < 0.001), and absence of diabetes. More tortuous aneurysms at baseline had significantly larger volume growth rates (difference, 32.8 cm3/year; p < 0.0001). | 11/16 |
| Tzirakis et al. (2019) [26] | Greece | 30 | Patients with AAAs | CTA | Statistical analysis showed strong evidence of a strong correlation between Dmax and volume growth rates (rho: 0.68, p < 0.001). In addition, there was strong evidence of a moderate correlation between Dmax growth and average surface growth (rho: 0.59, p < 0.001) and a moderate correlation with maximum surface growth (rho: 0.6, p < 0.001). Finally, there was strong evidence of a very strong association of volume growth with average surface growth (rho: 0.91, p < 0.001) and a strong association between volume growth and maximum surface growth (rho: 0.7, p < 0.001). | 11/16 |
| Kontopodis et al. (2014) [5] | Greece | 34 | Patients with AAAs (initial maximum diameter 40–53 mm) | CTA | There was a strong correlation between volume and Dmax growth rates (Spearman’s rho 0.6, p = 0.002). A total of 12 of the 15 AAAs having undergone surgical correction were in the high growth rate and only 3 in the low growth rate volume group (p = 0.005). With regard to the need for surgical repair, likelihood ratios between AAAs in the high and low growth rate groups were calculated (Likelihood ratio = 10) as well as sensitivity/specificity of median growth rates (Sensitivity = 80% Specificity = 74%). | 11/16 |
| Spanos et al. (2020) [6] | Greece | 62 | Patients with large ruptured (31) and unruptured (31) AAAs | CTA | The total aneurysm volumes for elective vs. rAAAs (p = 0.014) and true lumen volumes (p = 0.022) were significantly different between the groups. Maximum diameter did not have a statistically significant difference between the groups (p = 0.150). ROC curve showed that total aneurysm volume could predict rupture (AUC 0.68, p = 0.042). A threshold value of 380 mL was fairly well associated with rupture, with 60% sensitivity and specificity. Maximum diameter was not a predictor of rupture (AUC 0.62, p = 0.151). | 16/24 |
| Liljeqvist et al. (2016) [27] | Sweden | 41 | Patients with AAAs | CTA | Diameter correlated with volume with respect to baseline value (r = 0.71, p < 0.0001) and growth rate (r = 0.55, p = 0.0002). Significant absolute volume growth rate correlated stronger than significant absolute diameter growth rate with PWS (95% CI, 0.093–1.18) and PWRI (95% CI, 0.11–1.16) change rates. | 11/16 |
| Renapurkar et al. (2012) [28] | USA | 100 | Patients with AAAs | CTA | The correlation between diameter change and volume change was modest (r2 = 0.34; p = 0.001). Most patients (n = 64) had no measurable change in maximal diameter between studies (≤2 mm), but the change in volume was found to vary widely (−2 to 69 mL). | 10/16 |
| Franchin et al. (2021) * [29] | Italy/USA | 149 | Patients before and after EVAR of AAA | CTA | Diameter shrinkage was in 27 (18.1%), and volume shrinkage in 42 (28.2%). The presence of a persistent endoleak was associated with the absence of diameter shrinkage (p = 0.045; HR, 3.49; 95% CI, 1.031–11.859) and volume shrinkage (p = 0.001; HR, 7.75; 95% CI, 2.282–26.291). The ROC analysis demonstrated fair discrimination for this multivariate model (AUROC, 0.61; 95% CI, 0.52–0.71) with a 65.8% positive predictive value of no volume change in the presence of a persistent endoleak. Although the absolute diameter decrease had similar reliability to volume decrease, the volume analysis was more sensitive in assessing sac shrinkage. | 10/16 |
| Kritpracha et al. (2004) [30] | USA | 68 | Patients of after EVAR of AAA | CTA | The majority of increased AAA size studies were not detected by diameter measurement methods. Antero–posterior diameter was the least sensitive (15%) in detecting an increase in AAA size, particularly in the later postoperative period. Of the 55 studies with unchanged Dmax, 15 (27%) studies showed significant volume increase. | 8/16 |
| Raghavan et al. (2000) [31] | USA | 7 | 6 AAA patients awaiting repair. One control subject without an aneurysm. | 3D reconstructions of CTA | Of the factors studied (diameter, height, volume, systolic pressure), AAA volume appears to have the strongest correlation with PWS. Correlation coefficient 0.7. | 14/24 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vaitėnas, G.; Mosenko, V.; Račytė, A.; Medelis, K.; Skrebūnas, A.; Baltrūnas, T. Abdominal Aortic Aneurysm Diameter versus Volume: A Systematic Review. Biomedicines 2023, 11, 941. https://doi.org/10.3390/biomedicines11030941
Vaitėnas G, Mosenko V, Račytė A, Medelis K, Skrebūnas A, Baltrūnas T. Abdominal Aortic Aneurysm Diameter versus Volume: A Systematic Review. Biomedicines. 2023; 11(3):941. https://doi.org/10.3390/biomedicines11030941
Chicago/Turabian StyleVaitėnas, Gediminas, Valerija Mosenko, Austėja Račytė, Karolis Medelis, Arminas Skrebūnas, and Tomas Baltrūnas. 2023. "Abdominal Aortic Aneurysm Diameter versus Volume: A Systematic Review" Biomedicines 11, no. 3: 941. https://doi.org/10.3390/biomedicines11030941
APA StyleVaitėnas, G., Mosenko, V., Račytė, A., Medelis, K., Skrebūnas, A., & Baltrūnas, T. (2023). Abdominal Aortic Aneurysm Diameter versus Volume: A Systematic Review. Biomedicines, 11(3), 941. https://doi.org/10.3390/biomedicines11030941