Abstract
Background: Acute kidney injury (AKI) is a common complication in patients with severe COVID-19. Methods: We retrospectively reviewed 249 patients admitted to an intensive care unit (ICU) during the first wave of the pandemic to determine risk factors for AKI. Demographics, comorbidities, and clinical and outcome variables were obtained from electronic medical records. Results: Univariate analysis revealed older age, higher admission serum creatinine, elevated Sequential Organ Failure Assessment (SOFA) score, elevated admission D-Dimer, elevated CRP on day 2, mechanical ventilation, vasopressor requirement, and azithromycin usage as significant risk factors for AKI. Multivariate analysis demonstrated that higher admission creatinine (p = 0.0001, OR = 2.41, 95% CI = 1.56–3.70), vasopressor requirement (p = 0.0001, OR = 3.20, 95% CI = 1.69–5.98), elevated admission D-Dimer (p = 0.008, OR = 1.0001, 95% CI = 1.000–1.001), and elevated C-reactive protein (CRP) on day 2 (p = 0.033, OR = 1.0001, 95% CI = 1.004–1.009) were independent risk factors. Conversely, the combined use of Tocilizumab and corticosteroids was independently associated with reduced AKI risk (p = 0.0009, OR = 0.437, 95% CI = 0.23–0.81). Conclusion: This study confirms the high rate of AKI and associated mortality among COVID-19 patients admitted to ICUs and suggests a role for inflammation and/or coagulopathy in AKI development. One should consider the possibility that early administration of anti-inflammatory agents, as is now routinely conducted in the management of COVID-19-associated acute respiratory distress syndrome, may improve clinical outcomes in patients with AKI.
1. Introduction
Severe COVID-19 disease, as caused by SARS-CoV-2 infection, results in a wide variety of renal injuries, manifesting as hematuria, proteinuria, tubular dysfunction, acute tubular necrosis, thrombotic microangiopathy (TMA), and/or collapsing glomerulopathy [1,2,3]. The incidence of acute kidney injury (AKI) with COVID-19 disease ranges from 0.5% to 36% among all infected patients and is much higher in patients requiring intensive care management [4,5,6,7,8,9,10]. The reasons for the variability in the development of AKI are not completely clear, and may be related to timing of diagnosis, severity of illness, differences in demographics, and definitions of AKI [10,11]. Aside from the development of COVID-19-associated respiratory distress syndrome (C19-ARDS), AKI in the setting of COVID-19 disease is the second most common cause of morbidity and mortality [5,12,13]. The prevalence of AKI in non-survivors of COVID-19 having C19-ARDS and infected with the Wuhan strain of the virus during the first wave of the pandemic was increased 2.5-fold compared to survivors of COVID-19 with C19-ARDS [12].
Although COVID-19 disease primarily impacts the respiratory tract, the enzyme angiotensin converting enzyme-2 (ACE-2), the primary receptor for SARS-CoV-2, is expressed by the endothelium of almost all extra-pulmonary organs, including the reproductive tract. Interaction of SARS-CoV-2 with the ACE-2 receptor leads to a pro-thrombotic hyper-inflammatory state as well as maladaptive hyper-activation of the innate immune system resulting in cytokine storm. In this respect, COVID-19 disease can be viewed as a multisystem disease, with both acute and chronic multiorgan dysfunction, including myocarditis, myocardial infarction, macrophage activation syndrome, arterial and venous thrombosis, encephalitis, stroke, thyroiditis, adrenal insufficiency, hepatitis, hepatic failure, preeclampsia, and sterility [14,15,16,17,18].
Moreover, infection with COVID-19 is associated with several pathophysiologic phases: an incubation phase, an early viremic phase (which may or may not be symptomatic), and an early inflammatory pulmonary phase occurring between seven and fourteen days after infection [19]. In some patients, this is followed by a progressive inflammatory pulmonary phase leading to the development of C19-ARDS and multiorgan dysfunction [19]. An imbalance among pro- and anti-anticoagulant factors, in part a result of hyper-inflammation and cytokine storm, produces a pro-thrombotic state characterized by disseminated intravascular coagulation, macro- and microvascular thrombotic events, and multiorgan failure [19].
A myriad of insults, each capable of causing AKI, can occur during severe COVID-19 infection. These include hyper-inflammation as a part of cytokine storm, septic-shock-associated hypoperfusion, ischemia, C19-ARDS-associated hypoxia, and vascular thrombosis [1,2,20,21,22]. Previous studies of COVID-19 patients found that the risk factors for developing AKI were similar to those identified in other groups of patients with critical illness, such as comorbidities, age, vasopressor requirement, and respiratory failure requiring mechanical ventilation [2,3,21,22,23]. What remains unclear is the impact and interaction of inflammatory-coagulopathic biomarkers and other clinical and laboratory variables on the development and mortality of COVID-19-associated AKI. In addition, few studies have included therapeutic agents among the variables examined. With this in mind, we evaluated the incidence, risk factors, and medical therapy associated with the development and outcome of AKI in patients with severe COVID-19 disease admitted to an intensive care unit (ICU).
2. Materials and Methods
To determine risk factors for the development of AKI in patients with severe COVID-19 infection, and to compare risk factors for mortality between patients with and without AKI, we conducted a retrospective analysis of 249 consecutive patients either admitted or transferred to the ICU of two community hospitals between 12 March 2020 and 17 June 2020. At the time of ICU entry, all patients manifested severe difficulty in breathing as evidenced by one or more of the following: respiratory rate greater than 30 breaths per minute, blood oxygen saturation of 93% or less on room air, PAO2/FIO2 ratio less than 300, and presence of lung infiltrates in more than half of the lung fields [24,25].
Inclusion criteria were age greater than 18, confirmed diagnosis of COVID-19 by a positive PCR test, and signs and symptoms of COVID-19 infection. Study baseline was the time of hospital admission. Patients with end-stage renal disease (ESRD) were excluded from the analysis. All patients received standard-of-care therapy. Management and timing of ventilator support, employment of C19-ARDS ventilator strategies, antibiotic use, antiviral therapy, anticoagulation, initiation of vasopressors, use of convalescent plasma, corticosteroid (CC) therapy, and Tocilizumab therapy were determined by the ICU physician and consultants.
All standard laboratory results were extracted from the electronic medical record and were performed according to standardized laboratory practices. D-Dimer levels were obtained using a latex agglutination photo-optical assay from a sample of citrated whole blood. C-reactive protein (CRP) levels were obtained from serum samples and analyzed incorporating a laser-nephelometric method. Missing values in the case of standard laboratory results were not imputed and accounted for less than 1% of all measurements. Missing biomarker data, including CRP, D-Dimer, and ferritin, were found to be missing completely at random (MCAR) by Little’s MCAR test. Substituted values were inserted using an expectation maximization algorithm [26,27]. Missing biomarker data are reported in Supplementary Table S1.
Demographics, comorbidities, and clinical outcome variables were obtained from the electronic medical record or the patient’s history and physical exam and entered into a de-identified database. Measurements obtained on admission included arterial blood gas (ABG), routine metabolic chemistries, CRP, D-Dimer, ferritin, WBC and differential, and all variables necessary to calculate a Sequential Organ Failure Assessment (SOFA) score on admission. Other collected data included the dates of admission, ICU transfer, and death; need for vasopressor therapy; need for mechanical ventilation; PAO2/FIO2 ratio; use of corticosteroid (CC) therapy; and use of azithromycin, hydroxychloroquine (HCQ), convalescent plasma, Tocilizumab, or heparin (low molecular weight or unfractionated) either as deep vein thrombosis (DVT) prophylaxis or anticoagulant therapy. If patients received both anticoagulant doses and thrombo-prophylactic doses of heparin, they were analyzed in the anticoagulant group.
AKI was defined according to Kidney Disease: Improving Global Outcomes (KDIGO) criteria, namely, an increase in serum creatinine value (SCr) by ≥0.3 mg/dL (≥26.5 μMol/L) within 48 h. Urine output was not considered. SCr on admission was used to assess the change in SCr [28,29,30]. For this study, AKI associated with COVID-19 is defined as AKI occurring during the first 7 days of admission. The consulting nephrologist determined the timing and indication for the initiation of renal replacement therapy (RRT).
All statistical analyses were performed with IBM SPSS 28 software (IBM SPSS Inc., Chicago, IL, USA). We performed both univariate and multivariate analyses. The primary outcome was development of AKI for patients admitted or transferred to the ICU during the index admission. Summary statistics were computed for patients who did or did not develop AKI and for survivors vs. non-survivors, as well as for various subgroups of those who did and did not develop AKI. Continuous variables were expressed as median with interquartile ranges (IQR) and compared by the Student’s t-test or the Wilcoxon rank-sum test, as appropriate. Categorical variables were compared with Pearson’s chi-squared test. Fisher’s exact test was employed when indicated. Variables that were significant by univariate analysis at p < 0.05 were candidates for multivariate analysis. To determine risk factors that were independently associated with the outcome of AKI, we performed multivariate analysis by logistic regression with stepwise forward variable selection. Goodness of fit was determined by the Hosmer–Lameshow test. For continuous variables, the odds ratio (OR) represents the relative amount by which the odds ratio for the outcome variable increases or decreases when the independent variable is changed by exactly one unit. ORs and their 95% confidence intervals (95% CI) were determined by exponentiation of the beta coefficient and its upper and lower CI, respectively. If variables included imputed values for missing measurements, we performed multivariate analysis with and without these variables. Cox proportional hazards with forward variable selection was performed to determine variables independently predictive of the outcome of survival among all patients, and in those who did or did not develop AKI. For continuous variables, the hazard ratio (HR) represents the relative amount by which the probability of obtaining the outcome variable increases or decreases when the independent variable is changed by exactly one unit. HRs and their 95% CIs were determined by exponentiation of the regression coefficient and its upper and lower CI, respectively.
3. Results
3.1. Patient Characteristics
To evaluate risk factors for the development of AKI and its associated mortality, we retrospectively evaluated severe COVID-19 admissions (those patients requiring ICU admission or transfer). From 12 March 2020 to 17 June 2020, a total of 249 patients met the definition of severe COVID-19 infection; 90 (36%) were admitted directly to the ICU, and 159 (64%) were admitted to COVID-19 units and subsequently transferred to the ICU. The median age was 70 years (IQR 61, 80). There were 148 males (59%), and 177 patients were Caucasian (71%). The majority of patients had severe respiratory failure requiring mechanical ventilation (n = 173, 69%).
The mortality rate among these patients was 65% (162 patients). There was no significant difference in mortality between those directly admitted to the ICU (n = 56, 62%) vs. those transferred to the ICU (n = 106, 66%) (p = 0.48, OR = 0.82, 95% CI = 0.48–1.40). Likewise, there was no significant difference in the development of AKI between those directly admitted to the ICU (n = 40, 44%) and those transferred later (n = 79, 50%) (p = 0.43, OR = 0.8, 95% CI = 0.48–1.36). The median time to ICU transfer was three days (IQR 1, 5). For those patients not initially admitted to an ICU, there was no statistically significant difference in median time to ICU transfer between survivors and non-survivors (2 days (IQR 1, 4) vs. 3 days (IQR 1, 6), p = 0.1). Similarly, there was no significant difference in median time to ICU transfer between those who did and did not develop AKI (3 days (IQR 1, 6) vs. 3 days (IQR 1, 5), p = 0.17). As expected, patients directly admitted to the ICU had higher SOFA scores (6, IQR 3, 19) compared to those initially admitted to COVID-19 units (3, IQR 2, 5) (p = 0.00001).
3.2. Univariate Analysis of Risk Factors for AKI
Overall, 119 (48%) patients developed AKI, and 23 (19%) of these required RRT by the 7th day following hospital admission. Four additional patients developed AKI and required RRT later during their hospitalization (10–15 days). As the later development of AKI suggested an etiologic role for hospital-related factors distinct from initial COVID-19 infection, these patients were included in the non-AKI group. However, the inclusion of these late AKI patients in either group had no effect on the study’s results. The admission characteristics of the entire group of patients with severe COVID-19 infection are given in Table 1. Univariate analysis revealed that older age, the need for mechanical ventilation, elevated SCr, and higher SOFA score were associated with the development of AKI (Table 1).

Table 1.
COVID-19 ICU patients: characteristics of individuals with and without AKI.
Therapeutic and pharmacologic interventions are given in Table 2 and Figure 1. In general, information on the timing, rationale, and route of administration of agents was available only for CC and Tocilizumab and is therefore not a part of the analysis. Among all severe COVID-19 patients, 152 (61%) required vasopressor support, 192 (77%) received HCQ, 87 (35%) received azithromycin, 26 (10%) received Tocilizumab alone without CC, 69 (27%) received CC alone without Tocilizumab, 92 (37%) received combination therapy with both Tocilizumab and CC, and 65 (26%) received convalescent plasma. Consistent with admission during the first wave of the pandemic, only six patients (2.4%) received Remdesivir. Full-dose heparin was administered in 126 (50%) patients, and thrombo-prophylactic doses were administered in 85 (34%) patients. By univariate analysis, the need for vasopressors (p = 0.009, OR = 2.58, 95% CI = 1.25–5.31) and the use of azithromycin (p = 0.04, OR = 1.74, 95% CI = 1.03–2.95) were associated with the development of AKI. Conversely, patients who received combination therapy with Tocilizumab and CC were less likely to develop AKI (p = 0.018, OR = 0.53, 95% CI = 0.31–0.90). The use of either Tocilizumab alone or CC alone as monotherapy was not associated with a reduced risk of AKI. Only the combination predicted a lower risk of AKI. There was no difference in the time of initiation of CC among patients with and without AKI (4 days (IQR 1, 14) versus 3 days (IQR 1, 8), p = 0.56). Similarly, there was no difference in the time of initiation of Tocilizumab among patients with and without AKI (4 days (IQR 2, 6) versus 3 days (IQR 1.5, 7), p = 0.96).
Table 2.
Pharmacological interventions in COVID-19 ICU patients with and without AKI.
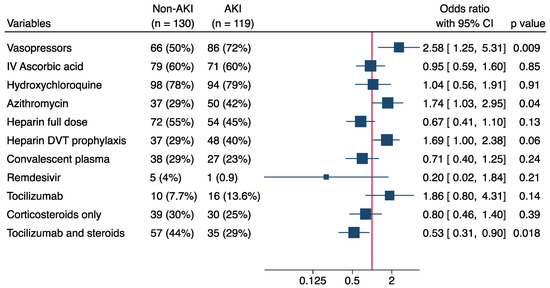
Figure 1.
Forest plot depicting the effect of the indicated pharmacologic interventions on the odds ratio (OR) for developing AKI as determined by univariate analysis.
Finally, since endothelial dysfunction, thrombosis, and inflammation are common features of COVID-19 disease, we examined the levels of inflammatory and coagulopathic markers in these patients [31,32]. These data were available from the electronic record, as it was common practice during the first wave of the pandemic to obtain serial inflammatory and thrombotic biomarkers in patients with COVID-19. Patients who developed AKI were noted to have significantly higher levels of D-Dimer on day 1 (hospital admission) and of CRP on day 2 (Table 3). These results are consistent with the interaction of SARS-CoV-2 with ACE2 on vascular endothelial cells in nearly all organs of the body, leading to excessive circulating levels of angiotensin 2, a pro-inflammatory, pro-thrombotic, and vasoconstrictive molecule [31,32,33].
Table 3.
Inflammatory and thrombotic markers in COVID-19 patients with and without AKI.
3.3. Multivariate Analysis of Risk Factors for the Development of AKI
Independent predictors of AKI development were identified by stepwise logistic regression with forward variable selection for all predictive variables identified by univariate analysis (Table 4 and Figure 2). Increased risk of AKI was associated with elevated admission SCr (p = 0.0001, OR = 2.406, 95% CI= 1.56–3.70), vasopressor requirement (p = 0.0001, OR = 3.188, 95% CI = 1.69–5.98), elevated D-Dimer on day 1 (p = 0.008, OR = 1.0001, 95% CI = 1.000–1.0010), and elevated CRP on day 2 (p = 0.033, OR = 1.004, 95% CI = 1.0001–1.009). In contrast, co-administration of Tocilizumab and CC was independently associated with a lower risk for development of AKI (p = 0.009, OR = 0.437, 95% CI = 0.23–0.81). Elevated SCr, vasopressor requirement, and lack of co-administration of Tocilizumab and CC remained significant independent risk factors for AKI development even when the biomarker variables with missing and imputed values were removed from the analysis.
Table 4.
Multivariate analysis of risk factors for AKI.
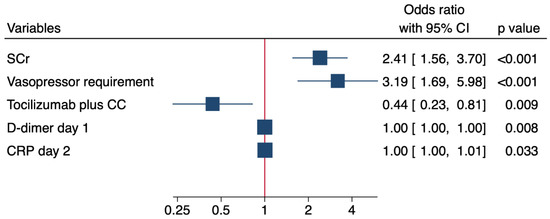
Figure 2.
Forest plot depicting the impact of the indicated risk factors on the odds ratio (OR) for developing AKI as determined by logistic regression with stepwise forward variable selection. For continuous variables, the odds ratio (OR) represents the relative amount by which the odds ratio for the outcome variable increases or decreases when the independent variable is increased by exactly one unit.
3.4. Univariate Analysis of Risk Factors for In-Hospital Mortality
We next examined the risk factors for in-hospital mortality among patients with severe COVID-19 infection. AKI development was associated with a 73% mortality, in contrast to a 56% mortality in patients not developing AKI. By univariate analysis, increased mortality was associated with older age, Caucasian race, presence of diabetes mellitus, presence of hypertension, development of AKI, requirement for RRT, need for mechanical ventilation, lower absolute lymphocyte count, elevated neutrophil to lymphocyte ratio, lower absolute platelet count, and elevated total bilirubin (Table 5).
Table 5.
COVID-19 ICU patients: characteristics of survivors and non-survivors.
To determine the effect of AKI on mortality, we compared the risk factors for mortality between patients who did and did not develop AKI. For patients with AKI, an increase in mortality was associated with need for mechanical ventilation, lower absolute lymphocyte counts, elevated absolute neutrophil count, elevated neutrophil to lymphocyte ratio, lower admission SCr, and lower absolute platelet count (Table 6). For those not developing AKI, increased mortality was associated with increased age, need for mechanical ventilation, presence of several co-morbidities (diabetes mellitus, hypertension, coronary artery disease, and chronic kidney disease (CKD)), increased admission SCr, and increased total bilirubin (Table 7).
Table 6.
Risk factors for mortality among COVID-19 ICU patients with AKI.
Table 7.
Risk factors for mortality among COVID-19 ICU patients without AKI.
The only pharmacologic intervention associated with increased mortality was the need for vasopressor support. This was true for the entire cohort (Table 8), as well as the subgroups with AKI (Table 9) and without AKI (Table 10). No inflammatory or thrombotic markers were associated with increased mortality (Table 11).
Table 8.
Pharmacologic interventions in COVID-19 ICU survivors and non-survivors.
Table 9.
Pharmacologic interventions in COVID-19 ICU survivors and non-survivors with AKI.
Table 10.
Pharmacologic interventions in COVID-19 ICU survivors and non-survivors without AKI.
Table 11.
Inflammatory and thrombotic markers in COVID-19 ICU survivors and non-survivors.
3.5. Multivariate Analysis of Risk Factors Associated with Mortality
Finally, to determine independent risk factors associated with mortality, we performed Cox proportional hazards analysis with forward variable selection (Table 12 and Figure 3). For the entire cohort of COVID-19 patients admitted to the ICU, only advanced age was independently associated with decreased survival (p = 0.00001, HR = 1.028, 95% CI = 1.016–1.041). For patients not developing AKI, increased age (p = 0.00001, HR = 1.044, 95% CI = 1.024–1.065) and CKD (p = 0.004, HR = 2.65, 95% CI = 1.37–5.1) were independently associated with decreased survival. For patients who developed AKI, surprisingly, the only independent risk factor was a lower SCr on admission (p = 0.011, HR = 0.79, 95% CI = 0.66–0.95).
Table 12.
Multivariate Cox proportional hazards analysis of risk factors for mortality.
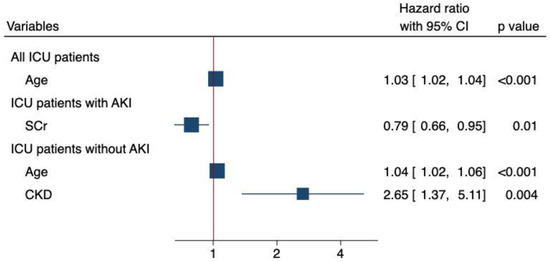
Figure 3.
Forest plot depicting the impact of the indicated risk factors on the hazard ratio (HR) for mortality as determined by Cox proportional hazards with stepwise forward variable selection. For continuous variables, the hazard ratio (HR) represents the relative amount by which the probability of obtaining the outcome increases or decreases when the independent variable is changed by exactly one unit.
4. Discussion
Clinical experience with patients hospitalized from COVID-19 has demonstrated significant heterogeneity in the development of AKI [10,34]. Chinese and Italian studies reported the development of AKI in 0.5–29% of patients [1,2,6,11]. In contrast, data from the United States and other developed nations have demonstrated a much higher incidence of this complication [9,12,35,36]. In a large cohort of COVID-19 patients, Fisher et al. found that COVID-19 patients developed AKI at twice the rate of historical controls [12]. The same investigators observed a similarly increased rate of AKI over the same timeframe when COVID-19 patients were compared to those admitted without COVID-19 [12]. Moreover, AKI in the setting of COVID-19 tends to be more severe. As compared to historical controls, COVID-19 patients had a 2.6-fold higher mortality and an increased requirement for RRT [37,38]. A recent meta-analysis involving over 25,000 COVID-19 patients found a pooled incidence of AKI of 53% in those with severe disease [39]. Schaubroeck et al., in a multi-center study involving 1286 critically ill patients, observed the development of AKI in 85% of patients [7]. In an ICU cohort of 313 ICU patients, Lumlertgul et al. observed the development of AKI in 76% of patients [40]. The results of our retrospective study are in accord with these data. AKI occurred in 119 of 249 (48%) of COVID-19 patients requiring ICU admission. Of these 119 patients, 23 (19%) required RRT, and 88 died (74%). These findings are consistent with previous studies from the US and other developed nations demonstrating an incidence of AKI in 40–80% of patients admitted to the ICU [5,7,12,40,41].
Despite these differences in incidence and severity, no risk factors have been consistently identified that discriminate between AKI developing in the presence or absence of COVID-19 infection. Traditional risk factors for AKI have included older age, elevated SCr on admission, requirement for vasopressors, thrombo-inflammatory biomarkers, and comorbidities such as diabetes and hypertension. By univariate analysis, in agreement with past studies, we found that the development of AKI was associated older age, the need for mechanical ventilation, elevated admission SCr, higher SOFA score, vasopressor requirement, and elevated inflammatory and thrombotic biomarkers (Table 1, Table 2 and Table 3). Of these, an elevated SCr, vasopressor requirement, and elevated inflammatory and thrombotic biomarkers were independent predictors (Table 4 and Figure 2). The lack of influence of comorbidities on the development of AKI may be a consequence of the advanced age of patients in our study (median age of 70), for whom comorbidities were similarly common in both AKI and non-AKI patients. In their studies of ICU patients with C19-ARDS, Wang et al. and Piniero et al. also found that the presence of multiple co-morbidities was not associated with the development of AKI [42,43].
A critical question is whether COVID-19-associated AKI is a separate clinical entity from other causes of AKI [44,45,46]. Investigations into this question have yielded conflicting results. Autopsy and biopsy series of COVID-19 patients with AKI have demonstrated a wide variety of glomerular and tubular injuries [44,46,47,48,49]. The prominence of glomerular and thrombotic injury, including collapsing glomerulopathy and TMA, is striking, and typically absent in sepsis-mediated AKI [46,47,49,50]. Nonetheless, notably, for both septic and COVID-19-associated AKI, morphologic and molecular evidence implicates inflammation as the primary driver of injury [51]. Thus, postmortem pathologic and molecular gene expression analyses have revealed that tubular injury occurring during the course of COVID-19 infection bears many similarities to sepsis-mediated acute tubular necrosis (ATN) [47,51]. Similarities include mitochondrial injury and dysregulation, increased autophagy, increased ceramide signaling, abnormalities in oxidative phosphorylation, up-regulation of apoptotic and necroptotic pathways, and increased endothelial and microvascular inflammation [51]. In addition, proteomic and genomic evidence indicates that a large number of genes involved in immune and metabolic counter-regulatory pathways, such as Treg differentiation and Sirtuin signaling, are expressed in both septic ATN and COVID-19-associated AKI [51].
In contrast, Volbeda and colleagues evaluated non-autolytic post mortem biopsies of patients with severe COVID-19 infection and observed morphologically more severe tubular injury, significant thrombosis of peritubular capillaries, and a less intense inflammatory response [52]. In fact, transcript levels for the pro-inflammatory cytokines TNF-α, IL-6, and MMP8 in biopsies from COVID-19-associated AKI patients were comparable to those found in normal controls [47,52]. In addition, the transcript levels of several genes, normally down-regulated during states of decreased renal perfusion, were also down-regulated in biopsies of COVID-19-associated AKI. Taken together, these differences suggest that decreased renal perfusion, rather than intense inflammatory state, may be the driver in some cases of COVID-19-associated AKI [52].
Such heterogeneity of pathologic and molecular findings may be due to differences in the timing of biopsies or possibly the existence of different endotypes within COVID-19-associated AKI. Certainly, the existence of an inflammatory phenotype is supported by the Recovery trial, which showed that the administration of Tocilizumab, a monoclonal antibody directed against the IL-6 receptor, led to a decrease in severe AKI requiring RRT [53]. Additional studies have demonstrated that the use of CC decreases the incidence of severe AKI [54,55,56]. Our own data also favor a role for inflammation in the pathophysiology of COVID-19-associated AKI. In the multivariate analysis, not only was increased CRP on day 2 independently predictive of AKI, but also combined treatment with Tocilizumab and CC was associated with decreased development of AKI. Our data further suggest a role for thrombosis, as an elevated level of D-Dimer on day 1 was also an independent predictor of AKI. In accord with this finding, Jewell et al. observed in a large UK cohort that patients who developed AKI had a statistically significant increase in thromboembolic complications [13]. Moreover, a systematic review has shown the risk of both venous and arterial thromboembolism to be statistically significantly higher in those with COVID-19 infection relative to those without [57].
With regard to mortality, although a large number of patient characteristics and interventions were associated with increased mortality, including the development of AKI, the only independent predictor for the entire cohort was advanced age. The impact of age is especially noteworthy, given that the median age of both survivors and non-survivors was greater than 65 and the difference in their median ages was less than 10 years (66 and 73, respectively). It is pertinent to note that the independent effect of older age on mortality is an almost universal finding. While one may associate increasing age with frailty and increased comorbidities, this may not be the entire explanation. For example, cellular expression of ACE-2, the putative receptor for the COVID-19 virus, decreases with age. As ACE-2 is capable of cleaving the pro-inflammatory peptide angiotensin 2 into the anti-inflammatory and anti-oxidant peptide angiotensin (1–7), aging may be associated with an increased tendency for inflammation [58,59,60,61]. Similar changes in ACE-2 expression have been observed in patients with cardiovascular disease [59,62,63,64,65]. Thus, aging and underlying cardiovascular disease may represent pro-inflammatory conditions predisposing patients to increased complications during the clinical course of COVID-19 disease.
Among patients without AKI, CKD was an additional independent predictor of mortality. Surprisingly, among patients with AKI, the only independent predictor of mortality was a lower SCr on admission. We can only speculate on the reasons for this anomalous finding. For example, a lower SCr on admission may have masked recognition of AKI and led to later renal consultation, resuscitative efforts, and use of RRT. Alternatively, a lower SCr might have been a surrogate for wasting or poorer nutritional status.
The retrospective and observational nature of our study necessarily entails several weaknesses. First, its retrospective nature limited our ability to determine and adjust for all differences in baseline characteristics and comorbidities. Second, we were unable to obtain information on such important potential risk factors as urinary output, urinary sediment, or proteinuria. Third, there were insufficient data to adjust for titration or timing and dose of pharmacologic interventions and therapies. Fourth, the diagnosis of comorbidities such as CKD or coronary artery disease were based on ICD coding rather than independent assessment by a non-involved clinician. Fifth, our retrospective analysis poses the usual limitations of selection and introduction bias. Thus, the benefits of anti-inflammatory therapy with Tocilizumab and CC in preventing AKI are associational and need to be confirmed in prospective trials. Sixth, there were many missing data points for the biomarkers D-Dimer, CRP, and ferritin, thus making it difficult to draw robust conclusions regarding their role as risk factors in the development of AKI. As a result, we had to rely on imputed data. Employing the imputed values into the multivariate analysis should therefore be considered exploratory. Nonetheless, removing the imputed biomarker data from the multivariate analysis did not alter the remaining risk factors. Further studies are needed to elucidate the role of biomarkers as predictors of AKI in patients with COVID-19 disease. Finally, our study was conducted during the first wave of the pandemic, before vaccinations were available, and extrapolation of our data to current patients may not necessarily be possible.
Despite these limitations, a major strength of our study is its study population, which comes from a large community hospital and is thus clinically and demographically similar to elderly COVID-19 patients in the general population.
5. Conclusions
The current study confirms the high rates of AKI and mortality among COVID-19 patients admitted to an ICU. As seen with other causes of AKI, multivariate analysis demonstrated that an elevated SCr on admission and the need for vasopressors were independent predictors of the development of AKI in patients with severe COVID-19. In addition, elevations of CRP and D-Dimer, biomarkers for inflammation and thrombosis, respectively, were also associated with an increased risk for AKI, albeit the effect was of small magnitude. Notably, patients who received both CC and Tocilizumab, but not either alone, were less likely to develop AKI. As has been shown for the development of C-19 ARDS in severely ill COVID-19 patients, our data suggest a potential role for inflammation in the development of COVID-19-associated AKI. One should consider the possibility that early administration of anti-inflammatory agents, just as one performs in the management of C-19 ARDS, may improve clinical outcomes in patients with AKI.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/biomedicines11030845/s1, Table S1. Missing values of biomarkers.
Author Contributions
Conceptualization, J.I. (Jose Iglesias), A.V., J.S.L., J.I. (Justin Ilagan), N.U. and A.M.; methodology, J.I. (Jose Iglesias), J.S.L. and A.V.; data curation, J.I. (Jose Iglesias), A.V. and Y.E.; validation, J.I. (Jose Iglesias), J.S.L. and AV.; formal analysis, S.P.A., J.I. (Jose Iglesias), A.V., J.S.L., J.I. (Justin Ilagan) and A.A.; investigation, J.I. (Jose Iglesias), A.V., J.S.L., J.I. (Justin Ilagan), N.U. and A.M.; data curation, J.I. (Jose Iglesias); writing—original draft preparation, J.I. (Jose Iglesias) and J.S.L.; writing—reviewing, J.I. (Jose Iglesias), J.S.L., A.V., S.P.A., D.P. and Y.E,. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by Medical Center Institutional Review Board (IRB # 20-005).
Informed Consent Statement
Informed consent was waived by the Community Medical Center Institutional Review Board as the study was deemed minimal risk to participants due to its retrospective nature and de-identified results.
Data Availability Statement
The data used in this study are protected under HIPPA and were not intended or allowed to be shared publicly, so due to the sensitive nature of the research supporting data are not available.
Acknowledgments
Jerrold S. Levine is employed by the Department of Veteran Affairs as a Staff Physician, Medical Service, Jesse Brown Veterans Affairs Medical Center, Chicago, IL. The views expressed in this manuscript are those of the author and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States government.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Chávez-Valencia, V.; Orizaga-de-la-Cruz, C.; Lagunas-Rangel, F.A. Acute Kidney Injury in COVID-19 Patients: Pathogenesis, Clinical Characteristics, Therapy, and Mortality. Diseases 2022, 10, 53. [Google Scholar] [CrossRef]
- Ahmadian, E.; Hosseiniyan Khatibi, S.M.; Razi Soofiyani, S.; Abediazar, S.; Shoja, M.M.; Ardalan, M.; Zununi Vahed, S. COVID-19 and Kidney Injury: Pathophysiology and Molecular Mechanisms. Rev. Med. Virol. 2021, 31, e2176. [Google Scholar] [CrossRef]
- Ahmed, A.R.; Ebad, C.A.; Stoneman, S.; Satti, M.M.; Conlon, P.J. Kidney Injury in COVID-19. World J. Nephrol. 2020, 9, 18–32. [Google Scholar] [CrossRef] [PubMed]
- El-Sayed, E.E.; Allayeh, A.K.; Salem, A.A.; Omar, S.M.; Zaghlol, S.M.; Abd-Elmaguid, H.M.; Abdul-Ghaffar, M.M.; ElSharkawy, M.M. Incidence of Acute Kidney Injury among COVID-19 Patients in Egypt. Ren. Replace Ther. 2021, 7, 32. [Google Scholar] [CrossRef]
- Hirsch, J.S.; Ng, J.H.; Ross, D.W.; Sharma, P.; Shah, H.H.; Barnett, R.L.; Hazzan, A.D.; Fishbane, S.; Jhaveri, K.D. Acute Kidney Injury in Patients Hospitalized with COVID-19. Kidney Int. 2020, 98, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Schaubroeck, H.; Vandenberghe, W.; Boer, W.; Boonen, E.; Dewulf, B.; Bourgeois, C.; Dubois, J.; Dumoulin, A.; Fivez, T.; Gunst, J.; et al. Acute Kidney Injury in Critical COVID-19: A Multicenter Cohort Analysis in Seven Large Hospitals in Belgium. Crit. Care 2022, 26, 225. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, M.M.B.; Lukitsch, I.; Torres-Ortiz, A.E.; Walker, J.B.; Varghese, V.; Hernandez-Arroyo, C.F.; Alqudsi, M.; LeDoux, J.R.; Velez, J.C.Q. Acute Kidney Injury Associated with Coronavirus Disease 2019 in Urban New Orleans. Kidney360 2020, 1, 614–622. [Google Scholar] [CrossRef] [PubMed]
- Rubin, S.; Orieux, A.; Prevel, R.; Garric, A.; Bats, M.-L.; Dabernat, S.; Camou, F.; Guisset, O.; Issa, N.; Mourissoux, G.; et al. Characterization of Acute Kidney Injury in Critically Ill Patients with Severe Coronavirus Disease 2019. Clin. Kidney J. 2020, 13, 354–361. [Google Scholar] [CrossRef]
- Sabaghian, T.; Kharazmi, A.B.; Ansari, A.; Omidi, F.; Kazemi, S.N.; Hajikhani, B.; Vaziri-Harami, R.; Tajbakhsh, A.; Omidi, S.; Haddadi, S.; et al. COVID-19 and Acute Kidney Injury: A Systematic Review. Front. Med. 2022, 9, 705908. [Google Scholar] [CrossRef]
- Gameiro, J.; Fonseca, J.A.; Oliveira, J.; Marques, F.; Bernardo, J.; Costa, C.; Carreiro, C.; Braz, S.; Lopes, J.A. Acute Kidney Injury in Hospitalized Patients with COVID-19: A Portuguese Cohort. Nefrología 2021, 41, 689–698. [Google Scholar] [CrossRef]
- Fisher, M.; Neugarten, J.; Bellin, E.; Yunes, M.; Stahl, L.; Johns, T.S.; Abramowitz, M.K.; Levy, R.; Kumar, N.; Mokrzycki, M.H.; et al. AKI in Hospitalized Patients with and without COVID-19: A Comparison Study. J. Am. Soc. Nephrol. 2020, 31, 2145–2157. [Google Scholar] [CrossRef] [PubMed]
- Jewell, P.D.; Bramham, K.; Galloway, J.; Post, F.; Norton, S.; Teo, J.; Fisher, R.; Saha, R.; Hutchings, S.; Hopkins, P.; et al. COVID-19-Related Acute Kidney Injury; Incidence, Risk Factors and Outcomes in a Large UK Cohort. BMC Nephrol. 2021, 22, 359. [Google Scholar] [CrossRef]
- Elrobaa, I.H.; New, K.J. COVID-19: Pulmonary and Extra Pulmonary Manifestations. Front. Public Health 2021, 9, 711616. [Google Scholar] [CrossRef]
- Gulati, A.; Pomeranz, C.; Qamar, Z.; Thomas, S.; Frisch, D.; George, G.; Summer, R.; DeSimone, J.; Sundaram, B. A Comprehensive Review of Manifestations of Novel Coronaviruses in the Context of Deadly COVID-19 Global Pandemic. Am. J. Med. Sci. 2020, 360, 5–34. [Google Scholar] [CrossRef]
- Tossetta, G.; Fantone, S.; Delli Muti, N.; Balercia, G.; Ciavattini, A.; Giannubilo, S.R.; Marzioni, D. Preeclampsia and Severe Acute Respiratory Syndrome Coronavirus 2 Infection: A Systematic Review. J. Hypertens. 2022, 40, 1629–1638. [Google Scholar] [CrossRef]
- Dale, L. Neurological Complications of COVID-19: A Review of the Literature. Cureus 2022, 14, e27633. [Google Scholar] [CrossRef]
- Delli Muti, N.; Finocchi, F.; Tossetta, G.; Salvio, G.; Cutini, M.; Marzioni, D.; Balercia, G. Could SARS-CoV-2 Infection Affect Male Fertility and Sexuality? APMIS 2022, 130, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Griffin, D.O.; Brennan-Rieder, D.; Ngo, B.; Kory, P.; Confalonieri, M.; Shapiro, L.; Iglesias, J.; Dube, M.; Nanda, N.; In, G.K.; et al. The Importance of Understanding the Stages of COVID-19 in Treatment and Trials. AIDS Rev. 2021, 23, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Chaibi, K.; Dao, M.; Pham, T.; Gumucio-Sanguino, V.D.; Di Paolo, F.A.; Pavot, A.; Cohen, Y.; Dreyfuss, D.; Pérez-Fernandez, X.; Gaudry, S. Severe Acute Kidney Injury in Patients with COVID-19 and Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2020, 202, 1299–1301. [Google Scholar] [CrossRef]
- Del Vecchio, L.; Locatelli, F. Hypoxia Response and Acute Lung and Kidney Injury: Possible Implications for Therapy of COVID-19. Clin. Kidney J. 2020, 13, 494–499. [Google Scholar] [CrossRef] [PubMed]
- Diebold, M.; Zimmermann, T.; Dickenmann, M.; Schaub, S.; Bassetti, S.; Tschudin-Sutter, S.; Bingisser, R.; Heim, C.; Siegemund, M.; Osswald, S.; et al. Comparison of Acute Kidney Injury in Patients with COVID-19 and Other Respiratory Infections: A Prospective Cohort Study. J. Clin. Med. 2021, 10, 2288. [Google Scholar] [CrossRef]
- Nardo, A.D.; Schneeweiss-Gleixner, M.; Bakail, M.; Dixon, E.D.; Lax, S.F.; Trauner, M. Pathophysiological Mechanisms of Liver Injury in COVID-19. Liver Int. 2021, 41, 20–32. [Google Scholar] [CrossRef]
- Berlin, D.A.; Gulick, R.M.; Martinez, F.J. Severe COVID-19. N. Engl. J. Med. 2020, 383, 2451–2460. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72,314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Li, C. Little’s Test of Missing Completely at Random. Stata J. 2013, 13, 795–809. [Google Scholar] [CrossRef]
- Do, C.B.; Batzoglou, S. What Is the Expectation Maximization Algorithm? Nat. Biotechnol. 2008, 26, 897–899. [Google Scholar] [CrossRef]
- Bernier-Jean, A.; Beaubien-Souligny, W.; Goupil, R.; Madore, F.; Paquette, F.; Troyanov, S.; Bouchard, J. Diagnosis and Outcomes of Acute Kidney Injury Using Surrogate and Imputation Methods for Missing Preadmission Creatinine Values. BMC Nephrol. 2017, 18, 141. [Google Scholar] [CrossRef]
- Kellum, J.A.; Lameire, N. Diagnosis, Evaluation, and Management of Acute Kidney Injury: A KDIGO Summary (Part 1). Crit. Care 2013, 17, 204. [Google Scholar] [CrossRef] [PubMed]
- Singbartl, K.; Kellum, J.A. AKI in the ICU: Definition, Epidemiology, Risk Stratification, and Outcomes. Kidney Int. 2012, 81, 819–825. [Google Scholar] [CrossRef]
- Gómez-Mesa, J.E.; Galindo-Coral, S.; Montes, M.C.; Muñoz Martin, A.J. Thrombosis and Coagulopathy in COVID-19. Curr. Probl. Cardiol. 2021, 46, 100742. [Google Scholar] [CrossRef]
- Asakura, H.; Ogawa, H. COVID-19-Associated Coagulopathy and Disseminated Intravascular Coagulation. Int. J. Hematol. 2021, 113, 45–57. [Google Scholar] [CrossRef] [PubMed]
- Amraei, R.; Rahimi, N. COVID-19, Renin-Angiotensin System and Endothelial Dysfunction. Cells 2020, 9, 1652. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-T.; Shao, S.-C.; Hsu, C.-K.; Wu, I.-W.; Hung, M.-J.; Chen, Y.-C. Incidence of Acute Kidney Injury in COVID-19 Infection: A Systematic Review and Meta-Analysis. Crit. Care 2020, 24, 346. [Google Scholar] [CrossRef]
- Hardenberg, J.-H.B.; Stockmann, H.; Eckardt, K.-U.; Schmidt-Ott, K.M. COVID-19 and acute kidney injury in the intensive care unit. Nephrologe 2021, 16, 20–25.e1. [Google Scholar] [CrossRef]
- Ng, J.H.; Hirsch, J.S.; Hazzan, A.; Wanchoo, R.; Shah, H.H.; Malieckal, D.A.; Ross, D.W.; Sharma, P.; Sakhiya, V.; Fishbane, S.; et al. Outcomes Among Patients Hospitalized with COVID-19 and Acute Kidney Injury. Am. J. Kidney Dis. 2021, 77, 204–215.e1. [Google Scholar] [CrossRef]
- Kolhe, N.V.; Fluck, R.J.; Selby, N.M.; Taal, M.W. Acute Kidney Injury Associated with COVID-19: A Retrospective Cohort Study. PLOS Med. 2020, 17, e1003406. [Google Scholar] [CrossRef] [PubMed]
- McNicholas, B.A.; Rezoagli, E.; Simpkin, A.J.; Khanna, S.; Suen, J.Y.; Yeung, P.; Brodie, D.; Li Bassi, G.; Pham, T.; Bellani, G.; et al. Epidemiology and Outcomes of Early-Onset AKI in COVID-19-Related ARDS in Comparison with Non-COVID-19-Related ARDS: Insights from Two Prospective Global Cohort Studies. Critical. Care 2023, 27, 3. [Google Scholar] [CrossRef]
- Fabrizi, F.; Alfieri, C.M.; Cerutti, R.; Lunghi, G.; Messa, P. COVID-19 and Acute Kidney Injury: A Systematic Review and Meta-Analysis. Pathogens 2020, 9, 1052. [Google Scholar] [CrossRef]
- Lumlertgul, N.; Pirondini, L.; Cooney, E.; Kok, W.; Gregson, J.; Camporota, L.; Lane, K.; Leach, R.; Ostermann, M. Acute Kidney Injury Prevalence, Progression and Long-Term Outcomes in Critically Ill Patients with COVID-19: A Cohort Study. Ann. Intensive Care 2021, 11, 123. [Google Scholar] [CrossRef]
- Flythe, J.E.; Assimon, M.M.; Tugman, M.J.; Chang, E.H.; Gupta, S.; Shah, J.; Sosa, M.A.; Renaghan, A.D.; Melamed, M.L.; Wilson, F.P.; et al. Characteristics and Outcomes of Individuals with Pre-Existing Kidney Disease and COVID-19 Admitted to Intensive Care Units in the United States. Am. J. Kidney Dis. 2021, 77, 190–203.e1. [Google Scholar] [CrossRef]
- Piñeiro, G.J.; Molina-Andújar, A.; Hermida, E.; Blasco, M.; Quintana, L.F.; Rojas, G.M.; Mercadal, J.; Castro, P.; Sandoval, E.; Andrea, R.; et al. Severe Acute Kidney Injury in Critically Ill COVID-19 Patients. J. Nephrol. 2021, 34, 285–293. [Google Scholar] [CrossRef]
- Wang, F.; Ran, L.; Qian, C.; Hua, J.; Luo, Z.; Ding, M.; Zhang, X.; Guo, W.; Gao, S.; Gao, W.; et al. Epidemiology and Outcomes of Acute Kidney Injury in COVID-19 Patients with Acute Respiratory Distress Syndrome: A Multicenter Retrospective Study. Blood Purif. 2021, 50, 499–505. [Google Scholar] [CrossRef]
- Golmai, P.; Larsen, C.P.; DeVita, M.V.; Wahl, S.J.; Weins, A.; Rennke, H.G.; Bijol, V.; Rosenstock, J.L. Histopathologic and Ultrastructural Findings in Postmortem Kidney Biopsy Material in 12 Patients with AKI and COVID-19. J. Am. Soc. Nephrol. 2020, 31, 1944–1947. [Google Scholar] [CrossRef] [PubMed]
- Shetty, A.A.; Tawhari, I.; Safar-Boueri, L.; Seif, N.; Alahmadi, A.; Gargiulo, R.; Aggarwal, V.; Usman, I.; Kisselev, S.; Gharavi, A.G.; et al. COVID-19-Associated Glomerular Disease. J. Am. Soc. Nephrol. 2021, 32, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Volbeda, M.; Jou-Valencia, D.; van den Heuvel, M.C.; Zijlstra, J.G.; Franssen, C.F.M.; van der Voort, P.H.J.; Moser, J.; van Meurs, M. Acute and Chronic Histopathological Findings in Renal Biopsies in COVID-19. Clin. Exp. Med. 2022, 1–12. [Google Scholar] [CrossRef]
- Ng, J.H.; Bijol, V.; Sparks, M.A.; Sise, M.E.; Izzedine, H.; Jhaveri, K.D. Pathophysiology and Pathology of Acute Kidney Injury in Patients With COVID-19. Adv. Chronic Kidney Dis. 2020, 27, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Santoriello, D.; Khairallah, P.; Bomback, A.S.; Xu, K.; Kudose, S.; Batal, I.; Barasch, J.; Radhakrishnan, J.; D’Agati, V.; Markowitz, G. Postmortem Kidney Pathology Findings in Patients with COVID-19. J. Am. Soc. Nephrol. 2020, 31, 2158–2167. [Google Scholar] [CrossRef] [PubMed]
- Tang, N.; Li, D.; Wang, X.; Sun, Z. Abnormal Coagulation Parameters Are Associated with Poor Prognosis in Patients with Novel Coronavirus Pneumonia. J. Thromb. Haemost. 2020, 18, 844–847. [Google Scholar] [CrossRef]
- Wu, H.; Larsen, C.P.; Hernandez-Arroyo, C.F.; Mohamed, M.M.B.; Caza, T.; Sharshir, M.; Chughtai, A.; Xie, L.; Gimenez, J.M.; Sandow, T.A.; et al. AKI and Collapsing Glomerulopathy Associated with COVID-19 and APOL 1 High-Risk Genotype. J. Am. Soc. Nephrol. 2020, 31, 1688–1695. [Google Scholar] [CrossRef]
- Alexander, M.P.; Mangalaparthi, K.K.; Madugundu, A.K.; Madugundu, A.K.; Moyer, A.M.; Adam, B.; Mengel, M.; Smrita, S.; Singh, S.; Singh, S.K.; et al. Acute Kidney Injury in Severe COVID-19 Has Similarities to Sepsis-Associated Kidney Injury: A Multi-Omics Study. Mayo Clinic Proc. 2021, 96, 2561–2575. [Google Scholar] [CrossRef]
- Volbeda, M.; Jou-Valencia, D.; van den Heuvel, M.C.; Knoester, M.; Zwiers, P.J.; Pillay, J.; Berger, S.P.; van der Voort, P.H.J.; Zijlstra, J.G.; van Meurs, M.; et al. Comparison of Renal Histopathology and Gene Expression Profiles between Severe COVID-19 and Bacterial Sepsis in Critically Ill Patients. Crit. Care 2021, 25, 202. [Google Scholar] [CrossRef]
- Tocilizumab in Patients Admitted to Hospital with COVID-19 (RECOVERY): A Randomised, Controlled, Open-Label, Platform Trial. Lancet 2021, 397, 1637–1645. [CrossRef]
- Orieux, A.; Khan, P.; Prevel, R.; Gruson, D.; Rubin, S.; Boyer, A. Impact of Dexamethasone Use to Prevent from Severe COVID-19-Induced Acute Kidney Injury. Crit. Care 2021, 25, 249. [Google Scholar] [CrossRef] [PubMed]
- Saggi, S.J.; Nath, S.; Culas, R.; Chittalae, S.; Burza, A.; Srinivasan, M.; Abdul, R.; Silver, B.; Lora, A.; Ibtida, I.; et al. Early Experience with Methylprednisolone on SARS-CoV-2 Infection in the African American Population, a Retrospective Analysis. Clin. Med. Insights Circ. Respir. Pulm. Med. 2020, 14, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Dexamethasone in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [CrossRef] [PubMed]
- Malas, M.B.; Naazie, I.N.; Elsayed, N.; Mathlouthi, A.; Marmor, R.; Clary, B. Thromboembolism Risk of COVID-19 Is High and Associated with a Higher Risk of Mortality: A Systematic Review and Meta-Analysis. EClinicalMedicine 2020, 29, 100639. [Google Scholar] [CrossRef]
- Chen, J.; Jiang, Q.; Xia, X.; Liu, K.; Yu, Z.; Tao, W.; Gong, W.; Han, J.-D.J. Individual Variation of the SARS-CoV-2 Receptor ACE2 Gene Expression and Regulation. Aging Cell 2020, 19, e13168. [Google Scholar] [CrossRef]
- Monteonofrio, L.; Florio, M.C.; AlGhatrif, M.; Lakatta, E.G.; Capogrossi, M.C. Aging- and Gender-Related Modulation of RAAS: Potential Implications in COVID-19 Disease. Vasc. Biol. 2021, 3, R1–R14. [Google Scholar] [CrossRef]
- Zhu, H.; Zhang, L.; Ma, Y.; Zhai, M.; Xia, L.; Liu, J.; Yu, S.; Duan, W. The Role of SARS-CoV-2 Target ACE2 in Cardiovascular Diseases. J. Cell. Mol. Med. 2021, 25, 1342–1349. [Google Scholar] [CrossRef]
- Baker, S.A.; Kwok, S.; Berry, G.J.; Montine, T.J. Angiotensin-Converting Enzyme 2 (ACE2) Expression Increases with Age in Patients Requiring Mechanical Ventilation. PLoS ONE 2021, 16, e0247060. [Google Scholar] [CrossRef]
- Tikellis, C.; Thomas, M.C. Angiotensin-Converting Enzyme 2 (ACE2) Is a Key Modulator of the Renin Angiotensin System in Health and Disease. Int. J. Pept. 2012, 2012, 256294. [Google Scholar] [CrossRef]
- Bartleson, J.M.; Radenkovic, D.; Covarrubias, A.J.; Furman, D.; Winer, D.A.; Verdin, E. SARS-CoV-2, COVID-19 and the Aging Immune System. Nat. Aging 2021, 1, 769–782. [Google Scholar] [CrossRef] [PubMed]
- Keidar, S.; Kaplan, M.; Gamliel-Lazarovich, A. ACE2 of the Heart: From Angiotensin I to Angiotensin (1–7). Cardiovasc. Res. 2007, 73, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Oudit, G.Y.; Kassiri, Z.; Patel, M.P.; Chappell, M.; Butany, J.; Backx, P.H.; Tsushima, R.G.; Scholey, J.W.; Khokha, R.; Penninger, J.M. Angiotensin II-Mediated Oxidative Stress and Inflammation Mediate the Age-Dependent Cardiomyopathy in ACE2 Null Mice. Cardiovasc. Res. 2007, 75, 29–39. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).