

Advanced Graft Development Approaches for ACL Reconstruction or Regeneration


 ,
, 
Abstract
1. Introduction
2. ACL Morphology and Mechanical Properties
3. ACL Healing Using Both Classical Methods and a Tissue Engineering Approach
- -
- Artificial grafts based on non-resorbable polymers (e.g., Jewel ACL, Lars);
- -
- Artificial non-resorbable tapes used as a bridge for ligament repairs (e.g., Internal Brace, Poly-tape);
- -
- Bio-based and synthetic membranes/meshes used as a bandage for ligament healing.
4. ACL Artificial Graft Development in the Tissue Engineering Approach
4.1. Essential Requirements of ACL Artificial Grafts
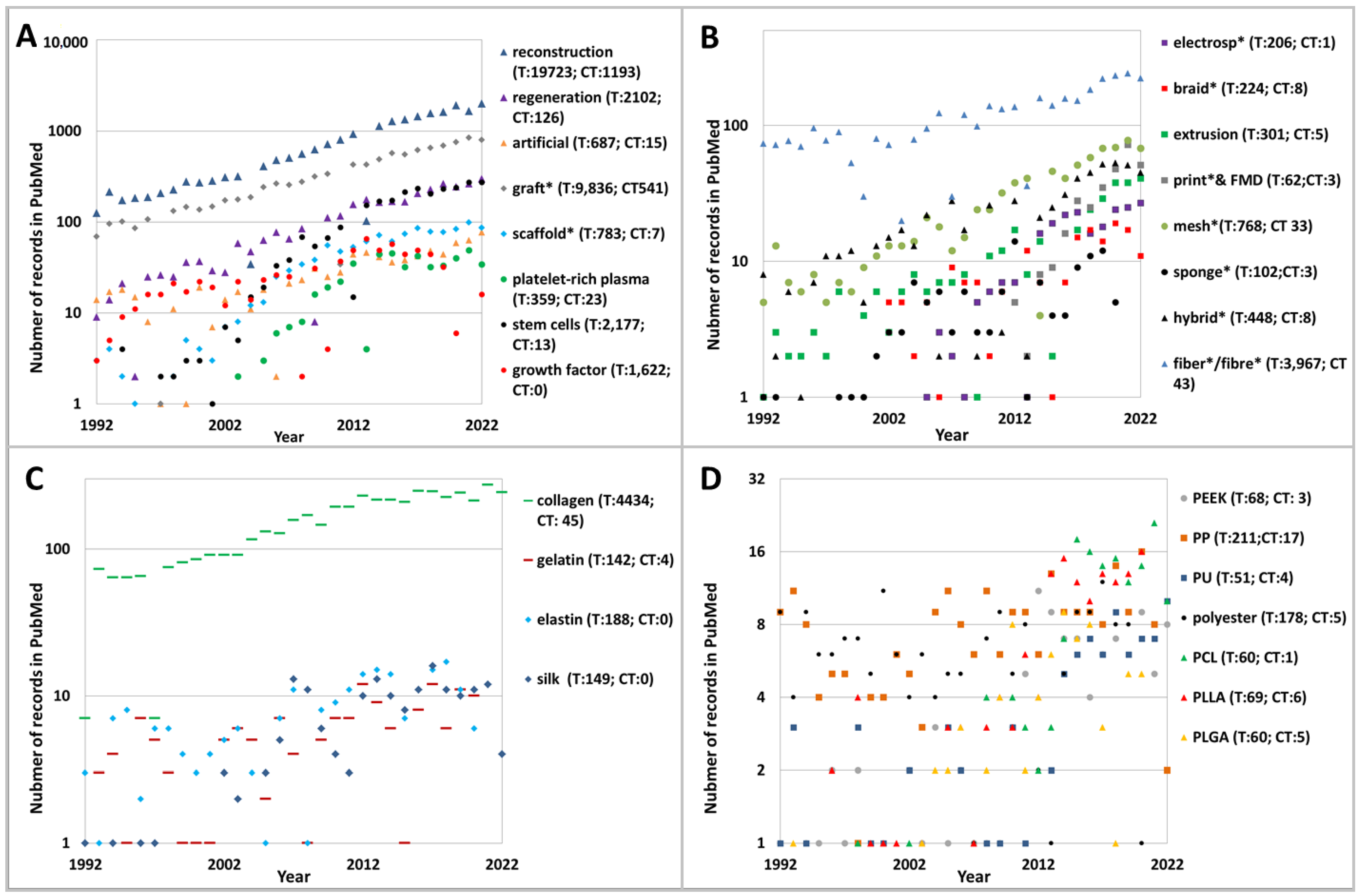
4.2. Summary of Records from PubMed
- (a)
- Treatment methods: reconstruction, regeneration, artificial, graft, scaffold, stem cells, growth factors, platelet-rich plasma;
- (b)
- Scaffold forms and fabrication methods: electrospun, extruded, printed, fiber, braid, mesh, sponge, hybrid;
- (c)
- Natural polymers: collagen, gelatin, silk, elastin;
- (d)
- Synthetic polymers: polyester, polyether ether ketone (PEEK), poly (ethylene terephthalate) (PET), polypropylene (PP), polyurethane (PU), poly(lactic-co-glycolic acid) (PLGA), poly(L-lactide-co-ε-caprolactone) (PLCL), poly(L-lactide) (PLLA), polycaprolactone (PCL).
4.3. Techniques in Artificial Graft Development
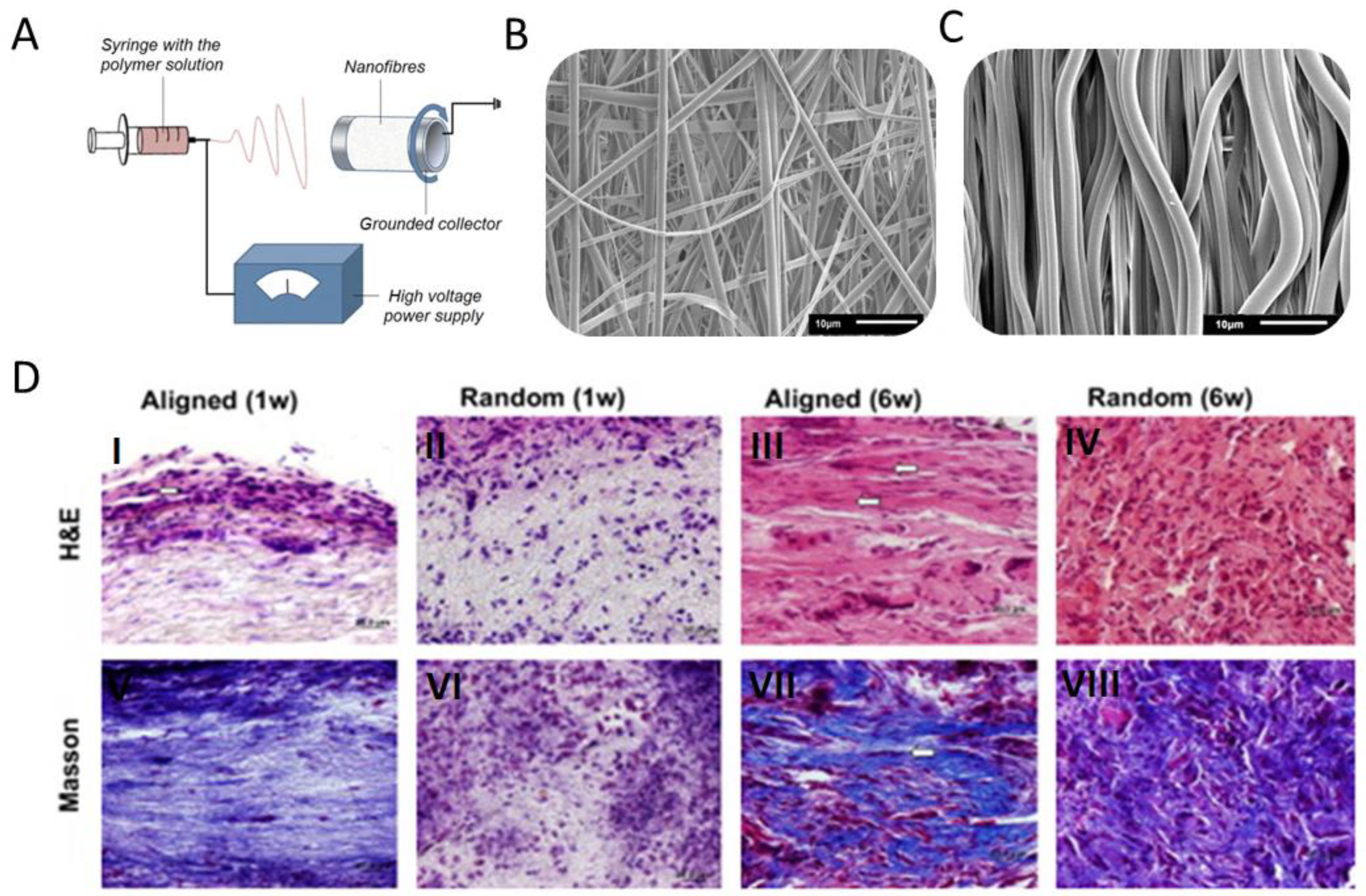
4.3.1. Fibers
4.3.2. 3D Braid
4.3.3. Other Techniques
4.4. ACL Scaffold/Graft-Bone Fixation
5. Discussion
- There is a significantly strong interest in collagen for the purpose of ACL regeneration;
- The interest in hybrid grafts is growing due to their greater capacity for mimicking graft morphology, mechanical properties, and biological functionality;
- There is a balance between the number of biodegradable and nonbiodegradable scaffolds in scientific literature, suggesting that both approaches to ACL healing are still needed;
- Many publications describe in vitro studies, but only a small percentage of them arrive at the level of clinical trials;
- The development of biodegradable scaffolds for ACL reconstruction is still an unattained goal;
- Increasing attention is being focused on the graft implantation technique, the support of the torn ACL using a sponge scaffold, and the injection of stem cell plasma or the patient’s blood;
- In most cases, scaffold fabrication techniques are easy to upscale to reach mass production, which is an undeniable advantage.
6. Conclusions and Future Approaches
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Oryan, A.; Moshiri, A.; Meimandi-Parizi, A. Graft Selection in ACL Reconstructive Surgery: Past, Present, and Future. Curr. Orthop. Pract. 2013, 24, 321–333. [Google Scholar] [CrossRef]
- Oryan, A.; Moshiri, A.; Meimandiparizi, A.-H. Effects of Sodium-Hyaluronate and Glucosamine-Chondroitin Sulfate on Remodeling Stage of Tenotomized Superficial Digital Flexor Tendon in Rabbits: A Clinical, Histopathological, Ultrastructural, and Biomechanical Study. Connect. Tissue Res. 2011, 52, 329–339. [Google Scholar] [CrossRef] [PubMed]
- Moshiri, A.; Oryan, A. Structural and Functional Modulation of Early Healing of Full-Thickness Superficial Digital Flexor Tendon Rupture in Rabbits by Repeated Subcutaneous Administration of Exogenous Human Recombinant Basic Fibroblast Growth Factor. J. Foot Ankle Surg. 2011, 50, 654–662. [Google Scholar] [CrossRef]
- Oryan, A.; Kamali, A.; Moshiri, A.; Eslaminejad, M.B. Role of Mesenchymal Stem Cells in Bone Regenerative Medicine: What Is the Evidence? Cell. Tissues Organs 2017, 204, 59–83. [Google Scholar] [CrossRef] [PubMed]
- Cheung, S.; Ma, C.B. Clinical Aspects: An Orthopedic Surgeon’s Perspective. In Cartilage Imaging: Significance, Techniques, and New Developments; Link, T.M., Ed.; Springer: New York, NY, USA, 2011; pp. 19–26. ISBN 978-1-4419-8438-8. [Google Scholar]
- Cięszczyk, P.; Willard, K.; Gronek, P.; Zmijewski, P.; Trybek, G.; Gronek, J.; Weber-Rajek, M.; Stastny, P.; Petr, M.; Lulińska-Kuklik, E.; et al. Are Genes Encoding Proteoglycans Really Associated with the Risk of Anterior Cruciate Ligament Rupture? Biol. Sport 2017, 34, 97–103. [Google Scholar] [CrossRef]
- Hunter, D.J. Clinical Aspects: A Rheumatologist’s Perspective. In Cartilage Imaging: Significance, Techniques, and New Developments; Link, T.M., Ed.; Springer: New York, NY, USA, 2011; pp. 11–18. ISBN 978-1-4419-8438-8. [Google Scholar]
- Artificial Tendons and Ligaments Market by Application (Knee Injuries, Shoulder Injuries, Foot and Ankle Injuries, Others), by End users (Hospitals and Clinics, ASCs): Global Opportunity Analysis and Industry Forecast, 2021–2031. Available online: https://www.alliedmarketresearch.com/artificial-tendons-and-ligaments-market-A10245 (accessed on 30 December 2022).
- Zbrojkiewicz, D.; Vertullo, C.; Grayson, J.E. Increasing Rates of Anterior Cruciate Ligament Reconstruction in Young Australians, 2000–2015. Med. J. Aust. 2018, 208, 354–358. [Google Scholar] [CrossRef]
- Abram, S.G.F.; Price, A.J.; Judge, A.; Beard, D.J. Anterior Cruciate Ligament (ACL) Reconstruction and Meniscal Repair Rates Have Both Increased in the Past 20 Years in England: Hospital Statistics from 1997 to 2017. Br. J. Sport. Med. 2020, 54, 286–291. [Google Scholar] [CrossRef]
- Herzog, M.M.; Marshall, S.W.; Lund, J.L.; Pate, V.; Mack, C.D.; Spang, J.T. Incidence of Anterior Cruciate Ligament Reconstruction among Adolescent Females in the United States, 2002 through 2014. JAMA Pediatr. 2017, 171, 808–810. [Google Scholar] [CrossRef]
- Hunsberger, J.; Harrysson, O.; Shirwaiker, R.; Starly, B.; Wysk, R.; Cohen, P.; Allickson, J.; Yoo, J.; Atala, A. Manufacturing Road Map for Tissue Engineering and Regenerative Medicine Technologies. Stem Cell. Transl. Med. 2015, 4, 130–135. [Google Scholar] [CrossRef]
- Lin, X.; Huang, J.; Shi, Y.; Liu, W. Tissue Engineering and Regenerative Medicine in Applied Research: A Year in Review of 2014. Tissue Eng. Part B Rev. 2015, 21, 177–186. [Google Scholar] [CrossRef]
- Butler, D.L.; Kay, M.D.; Stouffer, D.C. Comparison of Material Properties in Fascicle-Bone Units from Human Patellar Tendon and Knee Ligaments. J. Biomech. 1986, 19, 425–432. [Google Scholar] [CrossRef] [PubMed]
- CNOS Health Improving. Available online: http://www.cnos.net/totalmobility/knee-joint-replacement/knee-conditions/anterior-cruciate-ligament-acl-injury (accessed on 1 January 2022).
- Clifford, R. Wheeless Anatomy of ACL. In Wheeless’ Textbook of Orthopaedics; Data Trace Publishing Company: Towson, MD, USA, 2020. [Google Scholar]
- Woo, S.L.-Y.; Hollis, J.M.; Adams, D.J.; Lyon, R.M.; Takai, S. Tensile Properties of the Human Femur-Anterior Cruciate Ligament-Tibia Complex: The Effects of Specimen Age and Orientation. Am. J. Sport. Med. 1991, 19, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Proffen, B.L.; Sieker, J.T.; Murray, M.M. Bio-Enhanced Repair of the Anterior Cruciate Ligament. Arthrosc. J. Arthrosc. Relat. Surg. 2015, 31, 990–997. [Google Scholar] [CrossRef]
- Spector, M. Decellularized Tissues and Organs: An Historical Perspective and Prospects for the Future. Biomed. Mater. 2016, 11, 020201. [Google Scholar] [CrossRef] [PubMed]
- Lovati, A.B.; Bottagisio, M.; Moretti, M. Decellularized and Engineered Tendons as Biological Substitutes: A Critical Review. Stem Cell. Int. 2016, 2016, e7276150. [Google Scholar] [CrossRef] [PubMed]
- Parmaksiz, M.; Dogan, A.; Odabas, S.; Elçin, A.E.; Elçin, Y.M. Clinical Applications of Decellularized Extracellular Matrices for Tissue Engineering and Regenerative Medicine. Biomed. Mater. 2016, 11, 022003. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Xu, J.; Wang, A.; Zheng, M. Scaffolds for Tendon and Ligament Repair: Review of the Efficacy of Commercial Products. Expert Rev. Med. Devices 2009, 6, 61–73. [Google Scholar] [CrossRef]
- Rodrigues, M.T.; Reis, R.L.; Gomes, M.E. Engineering Tendon and Ligament Tissues: Present Developments towards Successful Clinical Products. J. Tissue Eng. Regen. Med. 2013, 7, 673–686. [Google Scholar] [CrossRef]
- Legnani, C.; Ventura, A.; Terzaghi, C.; Borgo, E.; Albisetti, W. Anterior Cruciate Ligament Reconstruction with Synthetic Grafts. A Review of Literature. Int. Orthop. SICOT 2010, 34, 465–471. [Google Scholar] [CrossRef]
- Matteo, B.D.; Loibl, M.; Andriolo, L.; Filardo, G.; Zellner, J.; Koch, M.; Angele, P. Biologic Agents for Anterior Cruciate Ligament Healing: A Systematic Review. World J. Orthop. 2016, 7, 592–603. [Google Scholar] [CrossRef]
- Von Porat, A.; Roos, E.M.; Roos, H. High Prevalence of Osteoarthritis 14 Years after an Anterior Cruciate Ligament Tear in Male Soccer Players: A Study of Radiographic and Patient Relevant Outcomes. Ann. Rheum. Dis. 2004, 63, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Fabricant, P.D.; Lakomkin, N.; Cruz, A.I.; Spitzer, E.; Lawrence, J.T.R.; Marx, R.G. Early ACL Reconstruction in Children Leads to Less Meniscal and Articular Cartilage Damage When Compared with Conservative or Delayed Treatment. J. ISAKOS 2016, 1, 10–15. [Google Scholar] [CrossRef]
- Wasilko, S.M.; Tourville, T.W.; DeSarno, M.J.; Slauterbeck, J.R.; Johnson, R.J.; Struglics, A.; Beynnon, B.D. Relationship between Synovial Fluid Biomarkers of Articular Cartilage Metabolism and the Patient’s Perspective of Outcome Depends on the Severity of Articular Cartilage Damage Following ACL Trauma. J. Orthop. Res. 2016, 34, 820–827. [Google Scholar] [CrossRef] [PubMed]
- Murray, M.M.; Fleming, B.C. Use of a Bioactive Scaffold to Stimulate Anterior Cruciate Ligament Healing Also Minimizes Posttraumatic Osteoarthritis after Surgery. Am. J. Sport. Med. 2013, 41, 1762–1770. [Google Scholar] [CrossRef] [PubMed]
- Role of Scaffolds in the Reconstruction of Anterior Cruciate Ligament of Knee-Systematic Review|Nellaiyappan|International Journal of Orthopaedics. Available online: http://www.ghrnet.org/index.php/ijo/article/view/1292/2016 (accessed on 30 December 2022).
- Rana, D.; Arulkumar, S.; Vishwakarma, A.; Ramalingam, M. Chapter 10—Considerations on Designing Scaffold for Tissue Engineering. In Stem Cell Biology and Tissue Engineering in Dental Sciences; Vishwakarma, A., Sharpe, P., Shi, S., Ramalingam, M., Eds.; Academic Press: Boston, MA, USA, 2015; pp. 133–148. ISBN 978-0-12-397157-9. [Google Scholar]
- Langer, R.; Vacanti, J.P. Tissue Engineering. Science 1993, 260, 920–926. [Google Scholar] [CrossRef] [PubMed]
- Yin, Z.; Chen, X.; Chen, J.L.; Shen, W.L.; Nguyen, T.M.H.; Gao, L.; Ouyang, H.W. The Regulation of Tendon Stem Cell Differentiation by the Alignment of Nanofibers. Biomaterials 2010, 31, 2163–2175. [Google Scholar] [CrossRef] [PubMed]
- Sahoo, S.; Ang, L.-T.; Goh, J.C.-H.; Toh, S.-L. Bioactive Nanofibers for Fibroblastic Differentiation of Mesenchymal Precursor Cells for Ligament/Tendon Tissue Engineering Applications. Differentiation 2010, 79, 102–110. [Google Scholar] [CrossRef] [PubMed]
- Samavedi, S.; Vaidya, P.; Gaddam, P.; Whittington, A.R.; Goldstein, A.S. Electrospun Meshes Possessing Region-Wise Differences in Fiber Orientation, Diameter, Chemistry and Mechanical Properties for Engineering Bone-Ligament-Bone Tissues. Biotechnol. Bioeng. 2014, 111, 2549–2559. [Google Scholar] [CrossRef]
- Bosworth, L.A.; Alam, N.; Wong, J.K.; Downes, S. Investigation of 2D and 3D Electrospun Scaffolds Intended for Tendon Repair. J. Mater. Sci. Mater. Med. 2013, 24, 1605–1614. [Google Scholar] [CrossRef]
- Said, S.S.; Pickering, J.G.; Mequanint, K. Controlled Delivery of Fibroblast Growth Factor-9 from Biodegradable Poly(Ester Amide) Fibers for Building Functional Neovasculature. Pharm. Res. 2014, 31, 3335–3347. [Google Scholar] [CrossRef]
- Plencner, M.; East, B.; Tonar, Z.; Otáhal, M.; Prosecká, E.; Rampichová, M.; Krejčí, T.; Litvinec, A.; Buzgo, M.; Míčková, A.; et al. Abdominal Closure Reinforcement by Using Polypropylene Mesh Functionalized with Poly-Ԑ-Caprolactone Nanofibers and Growth Factors for Prevention of Incisional Hernia Formation. IJN 2014, 9, 3263–3277. [Google Scholar] [CrossRef]
- Han, F.; Zhang, P.; Sun, Y.; Lin, C.; Zhao, P.; Chen, J. Hydroxyapatite-Doped Polycaprolactone Nanofiber Membrane Improves Tendon-Bone Interface Healing for Anterior Cruciate Ligament Reconstruction. IJN 2015, 10, 7333–7343. [Google Scholar] [CrossRef]
- Manning, C.N.; Schwartz, A.G.; Liu, W.; Xie, J.; Havlioglu, N.; Sakiyama-Elbert, S.E.; Silva, M.J.; Xia, Y.; Gelberman, R.H.; Thomopoulos, S. Controlled Delivery of Mesenchymal Stem Cells and Growth Factors Using a Nanofiber Scaffold for Tendon Repair. Acta Biomater. 2013, 9, 6905–6914. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Deng, G.; Chen, W.; Ye, X.; Mo, X. A Novel Electrospun-Aligned Nanoyarn-Reinforced Nanofibrous Scaffold for Tendon Tissue Engineering. Colloids Surf. B Biointerfaces 2014, 122, 270–276. [Google Scholar] [CrossRef]
- Bosworth, L.A.; Rathbone, S.R.; Bradley, R.S.; Cartmell, S.H. Dynamic Loading of Electrospun Yarns Guides Mesenchymal Stem Cells towards a Tendon Lineage. J. Mech. Behav. Biomed. Mater. 2014, 39, 175–183. [Google Scholar] [CrossRef]
- Laranjeira, M.; Domingues, R.M.A.; Costa-Almeida, R.; Reis, R.L.; Gomes, M.E. 3D Mimicry of Native-Tissue-Fiber Architecture Guides Tendon-Derived Cells and Adipose Stem Cells into Artificial Tendon Constructs. Small 2017, 13, 1700689. [Google Scholar] [CrossRef]
- Cooper, J.A.; Lu, H.H.; Ko, F.K.; Freeman, J.W.; Laurencin, C.T. Fiber-Based Tissue-Engineered Scaffold for Ligament Replacement: Design Considerations and in Vitro Evaluation. Biomaterials 2005, 26, 1523–1532. [Google Scholar] [CrossRef]
- Li, X.; Snedeker, J.G. Wired Silk Architectures Provide a Biomimetic ACL Tissue Engineering Scaffold. J. Mech. Behav. Biomed. Mater. 2013, 22, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; He, J.; Bian, W.; Li, Z.; Zhang, W.; Li, D.; Snedeker, J.G. A Novel Silk-Based Artificial Ligament and Tricalcium Phosphate/Polyether Ether Ketone Anchor for Anterior Cruciate Ligament Reconstruction—Safety and Efficacy in a Porcine Model. Acta Biomater. 2014, 10, 3696–3704. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.H.; Cooper, J.A.; Manuel, S.; Freeman, J.W.; Attawia, M.A.; Ko, F.K.; Laurencin, C.T. Anterior Cruciate Ligament Regeneration Using Braided Biodegradable Scaffolds: In Vitro Optimization Studies. Biomaterials 2005, 26, 4805–4816. [Google Scholar] [CrossRef] [PubMed]
- Laurencin, C.T.; Aronson, M.T.; Nair, L.S. Mechanically Competent Scaffold for Ligament and Tendon Regeneration. U.S. Patent US2013/0096679, 16 July 2013. Available online: https://patentcenter.uspto.gov/applications/13693878 (accessed on 30 December 2022).
- Teuschl, A.; Heimel, P.; Nürnberger, S.; van Griensven, M.; Redl, H.; Nau, T. A Novel Silk Fiber–Based Scaffold for Regeneration of the Anterior Cruciate Ligament: Histological Results from a Study in Sheep. Am. J. Sports Med. 2016, 44, 1547–1557. [Google Scholar] [CrossRef] [PubMed]
- Cai, C.; Chen, C.; Chen, G.; Wang, F.; Guo, L.; Yin, L.; Feng, D.; Yang, L. Type I Collagen and Polyvinyl Alcohol Blend Fiber Scaffold for Anterior Cruciate Ligament Reconstruction. Biomed. Mater. 2013, 8, 035001. [Google Scholar] [CrossRef]
- Faia-Torres, A.B.; Guimond-Lischer, S.; Rottmar, M.; Charnley, M.; Goren, T.; Maniura-Weber, K.; Spencer, N.D.; Reis, R.L.; Textor, M.; Neves, N.M. Differential Regulation of Osteogenic Differentiation of Stem Cells on Surface Roughness Gradients. Biomaterials 2014, 35, 9023–9032. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Fan, H.; Wong, E.J.W.; Toh, S.L.; Goh, J.C.H. Silk-Based Scaffold for Ligament Tissue Engineering. In Proceedings of the 14th Nordic-Baltic Conference on Biomedical Engineering and Medical Physics, Riga, Latvia, 16–20 June 2008; Katashev, A., Dekhtyar, Y., Spigulis, J., Eds.; Springer: Berlin/Heidelberg, Germany, 2008; pp. 34–37. [Google Scholar]
- Smith, S.E.; White, R.A.; Grant, D.A.; Grant, S.A. Gold and Hydroxyapatite Nano-Composite Scaffolds for Anterior Cruciate Ligament Reconstruction: In Vitro Characterization. J. Nanosci. Nanotechnol. 2016, 16, 1160–1169. [Google Scholar] [CrossRef] [PubMed]
- Spalazzi, J.P.; Dagher, E.; Doty, S.B.; Guo, X.E.; Rodeo, S.A.; Lu, H.H. In Vivo Evaluation of a Multiphased Scaffold Designed for Orthopaedic Interface Tissue Engineering and Soft Tissue-to-Bone Integration. J. Biomed. Mater. Res. Part A 2008, 86A, 1–12. [Google Scholar] [CrossRef]
- Chung, E.J.; Sugimoto, M.J.; Koh, J.L.; Ameer, G.A. A Biodegradable Tri-Component Graft for Anterior Cruciate Ligament Reconstruction. J. Tissue Eng. Regen. Med. 2017, 11, 704–712. [Google Scholar] [CrossRef]
- Naghashzargar, E.; Farè, S.; Catto, V.; Bertoldi, S.; Semnani, D.; Karbasi, S.; Tanzi, M.C. Nano/Micro Hybrid Scaffold of PCL or P3HB Nanofibers Combined with Silk Fibroin for Tendon and Ligament Tissue Engineering. J. Appl. Biomater. Funct. Mater. 2015, 13, 156–168. [Google Scholar] [CrossRef]
- Font Tellado, S.; Bonani, W.; Balmayor, E.R.; Foehr, P.; Motta, A.; Migliaresi, C.; van Griensven, M. Fabrication and Characterization of Biphasic Silk Fibroin Scaffolds for Tendon/Ligament-to-Bone Tissue Engineering. Tissue Eng. Part A 2017, 23, 859–872. [Google Scholar] [CrossRef]
- Murray, M.M.; Magarian, E.M.; Harrison, S.L.; Mastrangelo, A.N.; Zurakowski, D.; Fleming, B.C. The Effect of Skeletal Maturity on Functional Healing of the Anterior Cruciate Ligament. JBJS 2010, 92, 2039. [Google Scholar] [CrossRef]
- Persano, L.; Camposeo, A.; Tekmen, C.; Pisignano, D. Industrial Upscaling of Electrospinning and Applications of Polymer Nanofibers: A Review. Macromol. Mater. Eng. 2013, 298, 504–520. [Google Scholar] [CrossRef]
- Tang, Y.; Tian, J.; Li, L.; Huang, L.; Shen, Q.; Guo, S.; Jiang, Y. Biomimetic Biphasic Electrospun Scaffold for Anterior Cruciate Ligament Tissue Engineering. Tissue Eng. Regen. Med. 2021, 18, 819–830. [Google Scholar] [CrossRef] [PubMed]
- Uehlin, A.F.; Vines, J.B.; Feldman, D.S.; Nyairo, E.; Dean, D.R.; Thomas, V. Uni-Directionally Oriented Fibro-Porous PLLA/Fibrin Bio-Hybrid Scaffold: Mechano-Morphological and Cell Studies. Pharmaceutics 2022, 14, 277. [Google Scholar] [CrossRef] [PubMed]
- Barber, J.G.; Handorf, A.M.; Allee, T.J.; Li, W.-J. Braided Nanofibrous Scaffold for Tendon and Ligament Tissue Engineering. Tissue Eng. Part A 2013, 19, 1265–1274. [Google Scholar] [CrossRef] [PubMed]
- Rothrauff, B.B.; Lauro, B.B.; Yang, G.; Debski, R.E.; Musahl, V.; Tuan, R.S. Braided and Stacked Electrospun Nanofibrous Scaffolds for Tendon and Ligament Tissue Engineering. Tissue Eng. Part A 2017, 23, 378–389. [Google Scholar] [CrossRef]
- Gouveia, P.J.; Hodgkinson, T.; Amado, I.; Sadowska, J.M.; Ryan, A.J.; Romanazzo, S.; Carroll, S.; Cryan, S.-A.; Kelly, D.J.; O’Brien, F.J. Development of Collagen-Poly(Caprolactone)-Based Core-Shell Scaffolds Supplemented with Proteoglycans and Glycosaminoglycans for Ligament Repair. Mater. Sci. Eng. C 2021, 120, 111657. [Google Scholar] [CrossRef]
- Ross, T.M.; Moubaraki, B.; Turner, D.R.; Halder, G.J.; Chastanet, G.; Neville, S.M.; Cashion, J.D.; Létard, J.; Batten, S.R.; Murray, K.S. Spin Crossover and Solvate Effects in 1D FeII Chain Compounds Containing Bis(dipyridylamine)-Linked Triazine Ligands. Eur. J. Inorg. Chem. 2011, 2011, 1395–1417. [Google Scholar] [CrossRef]
- Rinoldi, C.; Fallahi, A.; Yazdi, I.K.; Paras, J.C.; Kijeńska-Gawrońska, E.; Trujillo-de Santiago, G.; Tuoheti, A.; Demarchi, D.; Annabi, N.; Khademhosseini, A.; et al. Mechanical and Biochemical Stimulation of 3D Multilayered Scaffolds for Tendon Tissue Engineering. ACS Biomater. Sci. Eng. 2019, 5, 2953–2964. [Google Scholar] [CrossRef]
- Rinoldi, C.; Costantini, M.; Kijeńska-Gawrońska, E.; Testa, S.; Fornetti, E.; Heljak, M.; Ćwiklińska, M.; Buda, R.; Baldi, J.; Cannata, S.; et al. Tendon Tissue Engineering: Effects of Mechanical and Biochemical Stimulation on Stem Cell Alignment on Cell-Laden Hydrogel Yarns. Adv. Healthc. Mater. 2019, 8, 1801218. [Google Scholar] [CrossRef]
- Bi, F.; Chen, Y.; Liu, J.; Wang, Y.; Xu, D.; Tian, K. Anterior Cruciate Ligament Reconstruction in a Rabbit Model Using a Silk-Collagen Scaffold Modified by Hydroxyapatite at Both Ends: A Histological and Biomechanical Study. J. Orthop. Surg. Res. 2021, 16, 139. [Google Scholar] [CrossRef]
- Cai, J.; Zhang, Q.; Chen, J.; Jiang, J.; Mo, X.; He, C.; Zhao, J. Electrodeposition of Calcium Phosphate onto Polyethylene Terephthalate Artificial Ligament Enhances Graft-Bone Integration after Anterior Cruciate Ligament Reconstruction. Bioact. Mater. 2021, 6, 783–793. [Google Scholar] [CrossRef]
- Vassiliadis, S. Advances in Modern Woven Fabrics Technology; IntechOpen: Rijeka, Croatia, 2011; ISBN 978-953-307-337-8. [Google Scholar]
- Bilisik, K.; Karaduman, N.S.; Bilisik, N.E.; Bilisik, K.; Karaduman, N.S.; Bilisik, N.E. 3D Fabrics for Technical Textile Applications; IntechOpen: Rijeka, Croatia, 2016; ISBN 978-953-51-2271-5. [Google Scholar]
- Bauer, B.; Emonts, C.; Bonten, L.; Annan, R.; Merkord, F.; Vad, T.; Idrissi, A.; Gries, T.; Blaeser, A. Melt-Spun, Cross-Section Modified Polycaprolactone Fibers for Use in Tendon and Ligament Tissue Engineering. Fibers 2022, 10, 23. [Google Scholar] [CrossRef]
- Na, W.J.; Ahn, H.C.; Jeon, S.Y.; Lee, J.S.; Kang, H.M.; Yu, W.R. Prediction of the braid pattern on arbitrary-shaped mandrels using the minimum path condition. Compos. Sci. Technol. 2014, 91, 30–37. [Google Scholar] [CrossRef]
- Mouritz, A.P.; Bannister, M.K.; Falzon, P.J.; Leong, K.H. Review of Applications for Advanced Three-Dimensional Fibre Textile Composites. Compos. Part A Appl. Sci. Manuf. 1999, 30, 1445–1461. [Google Scholar] [CrossRef]
- Cantournet, S.; Corté, L.; Ku, D.N.; Cherkaoui, M.; Bach, J.S. Artificial Tendon or Ligament with Varying Stiffness along Its Length. Europen Patent Application EP 2,687,188, 22 January 2014. [Google Scholar]
- Li, X.; He, J.; Bian, W.; Li, Z.; Li, D.; Snedeker, J.G. A Novel Silk–TCP–PEEK Construct for Anterior Cruciate Ligament Reconstruction: An off-the Shelf Alternative to a Bone–Tendon–Bone Autograft*. Biofabrication 2014, 6, 015010. [Google Scholar] [CrossRef]
- Li, X.; Bian, W.; Li, D.; Lian, Q.; Jin, Z. Fabrication of Porous Beta-Tricalcium Phosphate with Microchannel and Customized Geometry Based on Gel-Casting and Rapid Prototyping. Proc. Inst. Mech. Eng. Part H 2011, 225, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Murray, M.M. Current Status and Potential of Primary ACL Repair. Clin. Sport. Med. 2009, 28, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Q.; Lee, B.L.-P.; Komvopoulos, K.; Yan, Z.; Li, S. Plasma Surface Chemical Treatment of Electrospun Poly(l-Lactide) Microfibrous Scaffolds for Enhanced Cell Adhesion, Growth, and Infiltration. Tissue Eng. Part A 2013, 19, 1188–1198. [Google Scholar] [CrossRef] [PubMed]
- Lai, H.-J.; Kuan, C.-H.; Wu, H.-C.; Tsai, J.-C.; Chen, T.-M.; Hsieh, D.-J.; Wang, T.-W. Tailored Design of Electrospun Composite Nanofibers with Staged Release of Multiple Angiogenic Growth Factors for Chronic Wound Healing. Acta Biomater. 2014, 10, 4156–4166. [Google Scholar] [CrossRef]
- Burdick, J.A.; Mason, M.N.; Hinman, A.D.; Thorne, K.; Anseth, K.S. Delivery of Osteoinductive Growth Factors from Degradable PEG Hydrogels Influences Osteoblast Differentiation and Mineralization. J. Control. Release 2002, 83, 53–63. [Google Scholar] [CrossRef]
- Zhang, P.; Han, F.; Li, Y.; Chen, J.; Chen, T.; Zhi, Y.; Jiang, J.; Lin, C.; Chen, S.; Zhao, P. Local Delivery of Controlled-Release Simvastatin to Improve the Biocompatibility of Polyethylene Terephthalate Artificial Ligaments for Reconstruction of the Anterior Cruciate Ligament. IJN 2016, 11, 465–478. [Google Scholar] [CrossRef]
- Paavolainen, P.; Mäkisalo, S.; Skutnabb, K.; Holmström, T. Biologic Anchorage of Cruciate Ligament Prosthesis: Bone Ingrowth and Fixation of the Gore-Tex® Ligament in Sheep. Acta Orthop. Scand. 1993, 64, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Han, F.; Chen, T.; Wu, Z.; Chen, S. “Swiss Roll”-like Bioactive Hybrid Scaffolds for Promoting Bone Tissue Ingrowth and Tendon-Bone Healing after Anterior Cruciate Ligament Reconstruction. Biomater. Sci. 2020, 8, 871–883. [Google Scholar] [CrossRef] [PubMed]
- Ficek, K.; Rajca, J.; Stolarz, M.; Stodolak-Zych, E.; Wieczorek, J.; Muzalewska, M.; Wyleżoł, M.; Wróbel, Z.; Binkowski, M.; Błażewicz, S. Bioresorbable Stent in Anterior Cruciate Ligament Reconstruction. Polymers 2019, 11, 1961. [Google Scholar] [CrossRef] [PubMed]
- Budnicka, M.; Szymaniak, M.; Kołbuk, D.; Ruśkowski, P.; Gadomska-Gajadhur, A. Biomineralization of Poly-l-Lactide Spongy Bone Scaffolds Obtained by Freeze-Extraction Method. J. Biomed. Mater. Res. Part B Appl. Biomater. 2020, 108, 868–879. [Google Scholar] [CrossRef]
- Yang, F.; Wolke, J.G.C.; Jansen, J.A. Biomimetic Calcium Phosphate Coating on Electrospun Poly(ɛ-Caprolactone) Scaffolds for Bone Tissue Engineering. Chem. Eng. J. 2008, 137, 154–161. [Google Scholar] [CrossRef]
- Chen, J.; Chu, B.; Hsiao, B.S. Mineralization of Hydroxyapatite in Electrospun Nanofibrous Poly(L-Lactic Acid) Scaffolds. J. Biomed. Mater. Res. Part A 2006, 79A, 307–317. [Google Scholar] [CrossRef]
- Stolarz, M.; Ficek, K.; Binkowski, M.; Wróbel, Z. Bone Tunnel Enlargement Following Hamstring Anterior Cruciate Ligament Reconstruction: A Comprehensive Review. Physician Sportsmed. 2017, 45, 31–40. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Artificial Scaffold | Autograft | Allograft and Xenograft | |
|---|---|---|---|
| Disadvantages | - Biodegradation—time of graft longer than declared by manufacturers, which results in poor integration with surrounding tissues and insufficient space for native ECM regeneration - 50% in 7–10 years of natural ligament reconstruction require reoperation - Permanent inflammation in tissues surrounding the implant/scaffold, in the case of the use of certain materials - Poor mechanical properties of artificial ligaments, leading to re-breaking | - Two operations at the same time, which increases the time and cost of the operation and the patient’s recovery time - Reconstruction of large defects requires taking a large amount of tissue from the donor, which weakens the surrounding tissues - Additional scar tissue formed in the donor may limit the mobility of the knee - Lack of autografts that could be used for the reconstruction of ligaments | - Inflammation leading to instability and weakness of muscles around the knee - Low risk of becoming infected with viruses (hepatitis B and C, bovine spongiform encephalopathy) - Poor mechanical properties of grafts due to radiation sterilization - Availability - Price |
| Advantages | - Variability - Availability - Knee stability - Mechanical properties - Possibility to the top-down design of materials (e.g., chemical composition, structure) - Production for larger scale - Without additional procedure/graft procurement (only cells may be obtained from the patient) | - Without the additional cost of the graft - Without the risk of rejection - Without the risk of becoming infected with viruses (hepatitis B and C, bovine spongiform encephalopathy) | - Variability - Availability - Without loss of the patient’s knee stability |
| Product | Company | Material | Degradation Time | Architecture | Other |
|---|---|---|---|---|---|
| Grafts and tapes | |||||
| Lars ACL | Corinium Centre (Cirencester, UK) | Polyethylene terephthalate (PET) | Not resorbable | 3D braid graft | High tensile strength; The potential for inflammatory reaction |
| Jewel ACL™ (DI 05060267130495 *) | Neoligaments (Leeds, UK) | Polyethylene terephthalate (PET) | Not resorbable | 3D braid graft | Gas plasma treatment surface; 7 mm ID × 710 mm; allowing bone and tissue ingrowth |
| UCL Internal Brace Implant (DI 00888867220980) | Arthrex Co. (Naples- Florida, USA) | Polyetheretherketone (PEEK) | Not resorbable | 3D braid tape facilitation of graft advancement and orientation | - |
| ACL TightRope with FiberTag (DI 00888867308459) | Arthrex Co. (Naples- Florida, USA) | Polyethylene terephthalate (PET) | Not resorbable | 3D braid tape | e.g., ACL TightRope with Fiber Tag, BTB TightRope® Implant |
| Membranes and meshes | |||||
| FlexBand™ Plus (DI 00850003396019) | International Life Sciences DBA Artelon® (Marietta, GA, USA) | Polycaprolactone-based polyurethaneurea | Resorbable | Mesh | As a temporary Support for the healing tissue; used for regeneration, e.g., rotator cuff, Achilles, patellar, biceps, quadriceps |
| X-Repair (DI B055009) | Synthasome 3030 Bunker Hill Street, (San Diego, CA USA) | Poly-L-lactic acid | Degradable | Mesh | A slowly degradable synthetic mesh |
| Vicryl Mesh (DI 10705031132719) | Ethicon, Inc. 4221 Richmond Rd., (N.W. Walker, MI USA) | Polyglactin 910 (PLGA) | Resorbable | Woven mesh & knitted mesh | It is coated with polyglactin 370 and calcium stearate to decrease tissue drag and bacterial adherence |
| Tissue Matrix/Xenograft | Zimmer (La Verne, USA) | Collagen and elastin | Resorbable, integrates with the surrounding tissues | Membrane | Crosslinked |
| Technique | Source of the Polymer | Mechanical Properties | In Vitro Studies (Cell Types, Culture Time) | In Vivo Studies (Type of Animal, Size of the Testing Group) | Other Features | Ref. | |
|---|---|---|---|---|---|---|---|
| Electrospun nonwovens | PLLA from Ji’nan Daigang Biomaterial Co., (Jinan, China) | The modulus 22.76 ± 5.63 vs. 0.63 ± 0.56 MPa; p < 0.001; stiffness (3.48 ± 1.09 vs. 0.07 ± 0.04 N/mm; p < 0.001 | analysis of the multidifferentiation potential of the hTSPCs toward osteogenesis, adipogenesis, and chondrogenesis | 8–10-week-old female mice, histological examination and Masson trichrome staining | Biodegradable | [33] | |
| PLGA from Purac Asia Pacific, growth factors from Raybiotech, (Norcross, GA, USA) | Not analyzed | Bone marrow cells from New Zealand rabbits, cultured for 14 days | Not analyzed | Resorbable, with bfgf | [34] | ||
| PLGA and PCL purchased from DURECT Corporation (Cupertino CA, USA) | The tensile strengths of 10–40 MPa; the modulus 190–420 MPa; elongation at break of 60–210% | BMSCS from rats, 3 days culture | Not analyzed | Biodegradable | [35] | ||
| PCL from Sigma-Aldrich (St Louis, MO, USA) | The modulus 1.54 ± 0.26 vs. 14.11 ± 3.76 MPa; ultimate tensile stress 0.45 ± 0.09 vs. 4.74 ± 1.64 MPa; | Tendon fibroblasts from equine superficial digital flexor tendons, cultured for 14 days | Not analyzed | Biodegradable yarn | [36] | ||
| Poly(ester amide)s (PEAs), Bovine serum albumin (BSA) and growth factors from Cedarlane, (Burlington, NC, USA) | Not analyzed | NIH-3T3, 10T1/2, and HCASMC, analysis of viability, metabolic activity and gene expression line line | Not analyzed | Resorbable, FGF added | [37] | ||
| PCL from Sigma Aldrich; Prolene surgical product; growth factors from Sigma Aldrich and Hoffman La-Roche (Basel, Switzerland) | Not analyzed | Mouse 3T3 fibroblast cells; 10 days cell culture | 27 Chinchilla rabbits | Resorbable, growth factors incorporated: IGF-1, bfgf, TGF-ß2 | [38] | ||
| PCL (Mw = 80 kDa), N,N′-dimethylformamide and calf skin Col type I was obtained from Sigma-Aldrich (St Louis, MO, USA). nHAp produced using a nanoemulsion method. | After 8 weeks of in vivo study: max at failure-60 N, stiffness at failure 16 N | MC3T3-E1 murine preosteoblast cell line; cellular: Morphology, proliferation, and mineralization after 1, 3, 5, and 7 days | 24 skeletally mature female New Zealand White rabbits; after 4 and 8 weeks, analyses of histological and biomechanical | Ligament-bone Mesh | [39] | ||
| PLGA from Sigma Aldrich and HBDS | Not analyzed | ASCS; cell culture carried up to 14 days | 15 adult mongrel dogs, 9 days of study | Growth factors released from HBDS | [40] | ||
| PLCL from GUNZE Co., Bombyxmori silkworm cocoons from Jiaxing Silk Co., Ltd. (Shanghai, China). | The modulus 29.72 ± 1.88 vs. 433.56 ± 48.06 MPa; Tensile strength 3.44 ± 0.21 vs. 39.10 ± 2.89 MPa | Mesenchymal stem cells (MSCs) from Sprague-Dawley rats, cultured for 28 days | Not analyzed | Biodegradable yarn made on a dual-collector system | [41] | ||
| poly(ε-caprolactone) from PuracPurasorb | Yarns sustained 3600 cycles per day for 21 days | Human mesenchymal stem cells derived from bone marrow, cultured for up to 21 days | Not analyzed | Biodegradable yarn | [42] | ||
| Microcrystalline cellulose powder, puri- fied chitosan medium molecular weight, poly-ε-caprolactone (PCL, average M n = 80,000) | Not analyzed | hASCS and hTDCS cells; Alamar Blue test and morphology after 1–28 d | Not analyzed | Electrospun yarns ware used to fabricate 3D braids | [43] | ||
| 3D Braiding | PLAGA from Ethicon, Somerville, NJ, USA | Maximum load 2.4 ± 0.2 907 ± 132 N; ultimate tensile strength 5.3 ± 1.8 429 ± 84 MPa | Primary ACL fibroblasts from New Zealand White rabbits, cultured 24 h | Not analyzed | Biodegradable | [44] | |
| Silk fibers (Bombyx mori) (Grege 20/22, Trudel Limited, Zurich, Switzerland); Wiring machine: wired, braided, and Straight fibered | Measured in dry and wet; ultimate Tensile strength 9.4− 7.370.4 N; Stiffness 1.07 −1.47 N/mm. 1.08 In cycling mode, analyzed up to 3% strain at 1 Hz in 250 loading cycles. | Human foreskin fibroblasts (HFFS); braids morphology and mechanical properties were described after cyclic loading | 14 healthy adult male pigs (Chinese Tri-hybrid pig: Xianyang breed) aged around 4 months and weighing 55.2 ± 3.7 kg (mean ± SD) | Histological transitions from the silk graft to bone were similar to features of native ACL to bone attachment | [45,46] | ||
| PLAGA, PGA and PLLA from Albany International Co. And fibronectin (Sigma Aldrich) | Tested before and after surface modification by fibronectin | Primary ACL fibroblasts from New Zealand White rabbits, cultured 24 h | Not analyzed | Biodegradable | [47] | ||
| Combination of various non-degradable and degradable polymers, both natural and synthetic | Load strength 500–3200 N, stiffness 200–700 N/mm, | Not described in patent submission | Not described in patent submission | Implanted with seeded cells | [48] | ||
| Bombyx mori silkworm fiber of 20/22 den and 250 T/m (Testex AG, Zurich, Switzerland) | Ultimate tensile strength 1450 N Stiffness 200 N/mm | Not analyzed | 33 mountain sheep, 6 and 12 months | Cell seeding led to increased tissue regeneration | [49] | ||
| 50% type I collagen (Col-I) and 50% polyvinyl alcohol (PVA) | At 24 weeks, maximum load and tensile strength were 472.43 ± 15.2 N and 29.71 ± 0.96 MPa, respectively | Cytotoxicity on L929 fibroblasts after 4 and 7 days | In vivo on China Bama mini-pigs during 24 weeks | After 24 weeks, morphology and major extracellular matrix components of the regenerated ligament resembled the native ACL | [50] | ||
| Silk | Ultimate tensile strength c.a 1450 N; stiffness 194 N/mm, | In vitro not described in this article | 33 female mature mountain sheep | Multi-stage structure of the scaffold—fibers form yarns, and yarns build strands that form the whole scaffold | [51] | ||
| Other techniques | Freeze-drying and braiding | Bombyx silk fibers; polymers, e.g., gelatine from Sigma Aldrich | Not analyzed | HMSCS cultured for up to 14 days | 48 New Zealand White rabbits, studies carried out up to 24 weeks | Biodegradable | [52] |
| Porcine diaphragms were decellularized; AUO and HA nanoparticles | - | L929 murine fibroblast cells from ATCC (Manassas, VA); cytotoxicity, proliferation after 3–10 days | - | Natural porcine diaphragm was harvested from swine euthanized and was used | [53] | ||
| Triphasic component scaffold (melted mesh and microspheres) | Phase A polyglactin 10:90 knitted Mesh (vicrylvkml, Ethicon, Somerville, NJ, USA). Phase B microspheres of poly(D-L-lactide-coglycolide) 85:15 copolymer (PLGA, Cambridge, MA, USA) Phase C microspheres consisting of a 4:1 ratio of PLGA and 45S5 bioactive glass (BG, 20 mm; Mo-Sci Corp., Rolla, MD, USA), | Not analyzed | Primary neonatal bovine (1–7-day-old calves) fibroblasts and osteoblasts for scaffold seeding before implantation | 27 male athymic rats (NIH-rnu, 225–250 g, Charles River Laboratories, Wilmington, MA) | Biodegradable scaffold which supports multilineage cellular interactions, infiltration and abundant matrix production in vivo. | [54] | |
| PLL braid and porous POC-HA | Polylacidpll braids with a (Warwick, RI, USA) and Porous poly(1,8-octanediol-co-citrate)-hydroxypatetytepoc–HA (synthetized in lab) | Maximum load 256.2 N, Modulus of the graft 17.5 MPa, | Not analyzed | Rabbits were euthanized 6 weeks | Biodegradable | [55] | |
| Silk fibroin-electrospunPCL;silk fibroin-electrospunp3hb | PCL Sigma Aldrich, P3HB from Tainan Biopolymer Company (Taiwan, China), SF silk fibroin Yarns from Kiashahr Co. (Kiashahr, Iran), silk with a linear density of approximately 200 Den | SF/ES-P3HB SF/ES-PCL Maximum load, Lmax 97.6 ± 11.4 110.5 ± 6.6 respectively; Maximum extension, Emax (mm) 9.8 ± 1.4 7.9 ± 1.8 respectively | L929 fibroblasts, Mttcytotocicity after 3 days | Not analyzed | Biodegradable | [56] | |
| Silk sponge | Bombyx mori silk cocoons from Chul Thai Silk Company (Phetchabun, Thailand) and polyethylene glycol solution (10 kda) | Young modulus 600–1200 kpa | Admscs viability, cytotoxicity and proliferation, and gene expression were determined | - | Biodegradable | [57] | |
| Sponge of collagen -platelet composite | Bovine tissue in an acidic solution | Range of motion and Lachman tests were done on mini-pigs’ knees after. Days of in-vivo: Preop. Extension (deg) 15.0 ± 4.0–34.4 ± 3.2; Change in flexion (deg) −9.3 ± 3.8–17.0 ± 4.5; Lachman at 15 wks (mm) 1.8 ± 0.9–6.3 ± 0.7 | - | 21 Yucatan minipigs, | Biodegradable | [58] | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Urbanek, O.; Moczulska-Heljak, M.; Wróbel, M.; Mioduszewski, A.; Kołbuk, D. Advanced Graft Development Approaches for ACL Reconstruction or Regeneration. Biomedicines 2023, 11, 507. https://doi.org/10.3390/biomedicines11020507
Urbanek O, Moczulska-Heljak M, Wróbel M, Mioduszewski A, Kołbuk D. Advanced Graft Development Approaches for ACL Reconstruction or Regeneration. Biomedicines. 2023; 11(2):507. https://doi.org/10.3390/biomedicines11020507
Chicago/Turabian StyleUrbanek, Olga, Maryla Moczulska-Heljak, Mikołaj Wróbel, Andrzej Mioduszewski, and Dorota Kołbuk. 2023. "Advanced Graft Development Approaches for ACL Reconstruction or Regeneration" Biomedicines 11, no. 2: 507. https://doi.org/10.3390/biomedicines11020507
APA StyleUrbanek, O., Moczulska-Heljak, M., Wróbel, M., Mioduszewski, A., & Kołbuk, D. (2023). Advanced Graft Development Approaches for ACL Reconstruction or Regeneration. Biomedicines, 11(2), 507. https://doi.org/10.3390/biomedicines11020507