
Real-Life Effectiveness of Mepolizumab in Refractory Chronic Rhinosinusitis with Nasal Polyps

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
3. Statistical Analysis
4. Inclusion and Exclusion Criteria
5. Results
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fokkens, W.J.; Lund, V.J.; Hopkins, C.; Hellings, P.W.; Kern, R.; Reitsma, S.; Toppila-Salmi, S.; Bernal-Sprekelsen, M.; Mullol, J.; Alobid, I.; et al. European position paper on rhinosinusitis and nasal polyps 2020. Rhinology 2020, 58, 464. [Google Scholar] [CrossRef] [PubMed]
- Orlandi, R.R.; Kingdom, T.T.; Hwang, P.H.; Smith, T.L.; Alt, J.A.; Baroody, F.M.; Batra, P.S.; Bernal-Sprekelsen, M.; Bhattacharyya, N.; Chandra, R.K.; et al. International consensus statement on allergy and rhinology: Rhinosinusitis. Int. Forum. Allergy Rhinol. 2016, 6 (Suppl. 1), S22–S209. [Google Scholar] [CrossRef] [PubMed]
- Settipane, G.A.; Chafee, F.H. Nasal polyps in asthma and rhinitis: A review of 6,037 patients. J. Allergy Clin. Immunol. 1977, 59, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Hedman, J.; Kaprio, J.; Poussa, T.; Nieminen, M.M. Prevalence of asthma, aspirin intolerance, nasal polyposis, and chronic ob-structive pulmonary disease in a population-based study. Int. J. Epidemiol. 1999, 28, 717–722. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeld, R.M.; Piccirillo, J.F.; Chandrasekhar, S.S.; Brook, I.; Kumar, K.A.; Kramper, M.; Orlandi, R.R.; Palmer, J.N.; Patel, Z.M.; Peters, A.; et al. Clinical Practice Guideline (Update): Adult Sinusitis. Otolaryngol.-Head Neck Surg. 2015, 152 (Suppl. 2), S1–S39. [Google Scholar] [CrossRef]
- Koennecke, M.; Klimek, L.; Mullol, J.; Gevaert, P.; Wollenberg, B. Subtyping of polyposis nasi: Phenotypes, endotypes and comorbidities. Allergo J. Int. 2018, 27, 56–65. [Google Scholar] [CrossRef]
- Tomassen, P.; Vandeplas, G.; Van Zele, T.; Cardell, L.-O.; Arebro, J.; Olze, H.; Förster-Ruhrmann, U.; Kowalski, M.L.; Olszewska-Ziąber, A.; Holtappels, G.; et al. Inflammatory endotypes of chronic rhinosinusitis based on cluster analysis of biomarkers. J. Allergy Clin. Immunol. 2016, 137, 1449–1456.e4. [Google Scholar] [CrossRef]
- Gliklich, R.E.; Metson, R. The health impact of chronic sinusitis in patients seeking otolaryngologic care. Otolaryngol. Head Neck Surg. 1995, 113, 104–109. [Google Scholar] [CrossRef]
- Tsetsos, N.; Goudakos, J.; Daskalakis, D.; Konstantinidis, I.; Markou, K. Monoclonal antibodies for the treatment of chronic rhinosinusitis with nasal polyposis: A systematic review. Rhinology 2018, 56, 11–21. [Google Scholar] [CrossRef]
- Han, J.K. Subclassification of chronic rhinosinusitis. Laryngoscope 2013, 123, S15–S27. [Google Scholar] [CrossRef]
- Bachert, C.; Zhang, N.; Cavaliere, C.; Weiping, W.; Gevaert, E.; Krysko, O. Biologics for chronic rhinosinusitis with nasal polyps. J. Allergy Clin. Immunol. 2020, 145, 725–739. [Google Scholar] [CrossRef]
- Bachert, C.; Zhang, N.; Holtappels, G.; De Lobel, L.; van Cauwenberge, P.; Liu, S.; Lin, P.; Bousquet, J.; Van Steen, K. Presence of IL-5 protein and IgE antibodies to staphylococcal enterotoxins in nasal polyps is associated with comorbid asthma. J. Allergy Clin. Immunol. 2010, 126, 962–968.e6. [Google Scholar] [CrossRef] [PubMed]
- Hamilos, D.L.; Leung, D.Y.; Huston, D.P.; Kamil, A.; Wood, R.; Hamid, Q. GM-CSF, IL-5 and RANTES immunoreactivity and mRNA expression in chronic hyperplastic sinusitis with nasal polyposis (NP). Clin. Exp. Allergy 1998, 28, 1145–1152. [Google Scholar] [CrossRef] [PubMed]
- Hox, V.; Lourijsen, E.; Jordens, A.; Aasbjerg, K.; Agache, I.; Alobid, I.; Bachert, C.; Boussery, K.; Campo, P.; Fokkens, W.; et al. Benefits and harm of systemic steroids for short- and long-term use in rhinitis and rhi-nosinusitis: An EAACI position paper. Clin. Transl. Allergy 2020, 10, 1. [Google Scholar] [CrossRef] [PubMed]
- Vlaminck, S.; Vauterin, T.; Hellings, P.W.; Jorissen, M.; Acke, F.; Van Cauwenberge, P.; Bachert, C.; Gevaert, P. The importance of local eosinophilia in the surgical outcome of chronic rhi-nosinusitis: A 3-year prospective observational study. Am. J. Rhinol. Allergy 2014, 28, 260–264. [Google Scholar] [CrossRef]
- DeConde, A.S.; Mace, J.C.; Levy, J.M.; Rudmik, L.; Alt, J.A.; Smith, T.L. Prevalence of polyp recurrence after endoscopic sinus surgery for chronic rhinosinusitis with nasal polyposis. Laryngoscope 2017, 127, 550–555. [Google Scholar] [CrossRef]
- Rosati, D.; Rosato, C.; Pagliuca, G.; Cerbelli, B.; Della Rocca, C.; Di Cristofano, C.; Martellucci, S.; Gallo, A. Predictive markers of long-term recurrence in chronic rhinosinusitis with nasal polyps. Am. J. Otolaryngol. 2020, 41, 102286. [Google Scholar] [CrossRef]
- Bachert, C.; Akdis, C.A. Phenotypes and Emerging Endotypes of Chronic Rhinosinusitis. J. Allergy Clin. Immunol. Pract. 2016, 4, 621–628. [Google Scholar] [CrossRef]
- Akdis, C.A.; Bachert, C.; Cingi, C.; Dykewicz, M.S.; Hellings, P.W.; Naclerio, R.M.; Schleimer, R.P.; Ledford, D. Endotypes and phenotypes of chronic rhinosinusitis: A PRACTALL document of the European Academy of Allergy and Clinical Immunology and the American Academy of Allergy, Asthma & Immunology. J. Allergy Clin. Immunol. 2013, 131, 1479–1490. [Google Scholar] [CrossRef]
- Larsen, K. The Clinical Relationship of Nasal Polyps to Asthma. Allergy Asthma Proc. 1996, 17, 243–249. [Google Scholar] [CrossRef]
- Rajan, J.P.; Wineinger, N.E.; Stevenson, D.D.; White, A.A. Prevalence of aspirin-exacerbated respiratory disease among asthmatic patients: A meta-analysis of the literature. J. Allergy Clin. Immunol. 2015, 135, 676–681.e1. [Google Scholar] [CrossRef]
- Stevens, W.W.; Peters, A.T.; Hirsch, A.G.; Nordberg, C.M.; Schwartz, B.S.; Mercer, D.G.; Mahdavinia, M.; Grammer, L.C.; Hulse, K.E.; Kern, R.C.; et al. Clinical Characteristics of Patients with Chronic Rhinosinusitis with Nasal Polyps, Asthma, and Aspirin-Exacerbated Respiratory Disease. J. Allergy Clin. Immunol. Pract. 2017, 5, 1061–1070.e3. [Google Scholar] [CrossRef]
- White, A.A.; Stevenson, D.D. Aspirin-exacerbated respiratory disease. N. Engl. J. Med. 2018, 379, 1060–1070. [Google Scholar] [CrossRef]
- Franzese, C.B. The Role of Biologics in the Treatment of Nasal Polyps. Immunol. Allergy Clin. N. Am. 2020, 40, 295–302. [Google Scholar] [CrossRef]
- Gallo, S.; Castelnuovo, P.; Spirito, L.; Feduzi, M.; Seccia, V.; Visca, D.; Spanevello, A.; Statuti, E.; Latorre, M.; Montuori, C.; et al. Mepolizumab Improves Outcomes of Chronic Rhinosinusitis with Nasal Polyps in Severe Asthmatic Patients: A Multicentric Real-Life Study. J. Pers. Med. 2022, 12, 1304. [Google Scholar] [CrossRef]
- Han, J.K.; Bachert, C.; Fokkens, W.; Desrosiers, M.; Wagenmann, M.; Lee, S.E.; Smith, S.G.; Martin, N.; Mayer, B.; Yancey, S.W.; et al. Mepolizumab for chronic rhinosinusitis with nasal polyps (SYNAPSE): A randomized, double-blind, placebo-controlled, phase 3 trial. Lancet Respir. Med. 2021, 9, 1141–1153. [Google Scholar] [CrossRef]
- Reddel, H.K.; Bacharier, L.B.; Bateman, E.D.; Brightling, C.E.; Brusselle, G.G.; Buhl, R.; Cruz, A.A.; Duijts, L.; Drazen, J.M.; FitzGerald, J.M.; et al. Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention, 2022. Available online: www.ginasthma.org (accessed on 19 October 2021).
- Bousquet, J.; Schünemann, H.J.; Togias, A.; Bachert, C.; Erhola, M.; Hellings, P.W.; Klimek, L.; Pfaar, O.; Wallace, D.; Ansotegui, I.; et al. Next-generation Allergic Rhinitis and Its Impact on Asthma (ARIA) guidelines for allergic rhinitis based on Grading of Recommendations Assessment, Development and Evaluation (GRADE) and real-world evidence. J. Allergy Clin. Immunol. 2019, 145, 70–80.e3. [Google Scholar] [CrossRef]
- Chung, K.F.; Wenzel, S.E.; Brozek, J.L.; Bush, A.; Castro, M.; Sterk, P.J.; Adcock, I.M.; Bateman, E.D.; Bel, E.H.; Bleecker, E.R.; et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur. Respir. J. 2013, 43, 343–373. [Google Scholar] [CrossRef]
- Lund, V.J.; Kennedy, D.W. Staging for rhinosinusitis. Otolaryngol. Head Neck Surg. 1997, 117, S35–S40. [Google Scholar] [CrossRef]
- Lildholdt, T.; Rundcrantz, H.; Lindqvist, N. Efficacy of topical corticosteroid powder for nasal polyps: A double-blind, placebo-controlled study of budesonide. Clin. Otolaryngol. 1995, 20, 26–30. [Google Scholar] [CrossRef]
- Bachert, C.; Sousa, A.R.; Lund, V.J.; Scadding, G.K.; Gevaert, P.; Nasser, S.; Durham, S.R.; Cornet, M.E.; Kariyawasam, H.H.; Gilbert, J.; et al. Reduced need for surgery in severe nasal polyposis with mepolizumab: Randomized trial. J. Allergy Clin. Immunol. 2017, 140, 1024–1031.e14. [Google Scholar] [CrossRef]
- Gallo, S.; Russo, F.; Mozzanica, F.; Preti, A.; Bandi, F.; Costantino, C.; Gera, R.; Ottaviani, F.; Castelnuovo, P. Prognostic value of the Sinonasal Outcome Test 22 (SNOT-22) in chronic rhinosinusitis. Acta Otorhinolaryngol. Ital. 2020, 40, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Rosenkranz, G.K. A note on the Hodges-Lehmann estimator. Pharm. Stat. 2010, 9, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Drake-Lee, A.B.; Lowe, D.; Swanston, A.; Grace, A. Clinical Profile and recurrence of nasal polyps. J. Laryngol. Otol. 1984, 98, 783–793. [Google Scholar] [CrossRef] [PubMed]
- Bs, S.B.; Marino, M.J.; Rank, M.A.; Donaldson, A.M.; O’Brien, E.K.; Lal, D. Benefits of biologic therapy administered for asthma on co-existent chronic rhinosinusitis: A real-world study. Int. Forum Allergy Rhinol. 2021, 11, 1152–1161. [Google Scholar] [CrossRef]
- Hopkins, C.; Gillett, S.; Slack, R.; Lund, V.; Browne, J. Psychometric validity of the 22-item Sinonasal Outcome Test. Clin. Otolaryngol. 2009, 34, 447–454. [Google Scholar] [CrossRef]
- Kato, A.; Peters, A.T.; Stevens, W.W.; Schleimer, R.P.; Tan, B.K.; Kern, R.C. Endotypes of chronic rhinosinusitis: Relationships to disease phenotypes, pathogenesis, clinical findings, and treatment approaches. Allergy 2021, 77, 812–826. [Google Scholar] [CrossRef]
- Flood-Page, P.; Menzies-Gow, A.; Phipps, S.; Ying, S.; Wangoo, A.; Ludwig, M.S.; Barnes, N.; Robinson, D.; Kay, A.B. Anti-IL-5 treatment reduces deposition of ECM proteins in the bronchial subepithelial basement membrane of mild atopic asthmatics. J. Clin. Investig. 2003, 112, 1029–1036. [Google Scholar] [CrossRef]
- Pelaia, C.; Vatrella, A.; Busceti, M.T.; Gallelli, L.; Terracciano, R.; Savino, R.; Pelaia, G. Severe eosinophilic asthma: From the patho-genic role of interleukin-5 to the therapeutic action of mepolizumab. Drug Des. Dev. Ther. 2017, 11, 3137–3144. [Google Scholar] [CrossRef]
- European Medicines Agency. Mepolizumab Summary of Product Characteristics, 2021. Available online: https://www.ema.europa.eu/en/documents/product-information/nucala-epar-product-information_en.pdf (accessed on 30 March 2021).
- GlaxoSmithKline. Mepolizumab Prescribing Information. 2020. Available online: https://www.gsksource.com/pharma/content/dam/GlaxoSmithKline/US/en/Prescribig_Information/Nucala/pdf/NUCALA-PI-PIL-IFU-COMBINED.PDF (accessed on 30 March 2021).
- Bachert, C.; Sousa, A.R.; Han, J.K.; Schlosser, R.J.; Sowerby, L.J.; Hopkins, C.; Maspero, J.F.; Smith, S.G.; Kante, O.; Karidi-Andrioti, D.E.; et al. Mepolizumab for chronic rhinosinusitis with nasal polyps: Treatment efficacy by comorbidity and blood eosinophil count. J. Allergy Clin. Immunol. 2022, 149, 1711–1721.e6. [Google Scholar] [CrossRef]
- da Costa Martins, S.M.; Tinoco, E.; Cabrita, B.; Machado, D.; Franco, I.; Ladeira, I.; Pascoal, I.; Lima, R.; Valente, S. Mepolizumab in the treatment of severe asthma with nasal polyposis: Real-life study. Eur. Respir. J. 2021, 58, PA3727. [Google Scholar]
- Meier, E.C.; Schmid-Grendelmeier, P.; Steiner, U.C.; Soyka, M.B. Real-Life Experience of Monoclonal Antibody Treatments in Chronic Rhinosinusitis with Nasal Polyposis. Int. Arch. Allergy Immunol. 2021, 182, 736–743. [Google Scholar] [CrossRef]
- Seys, S.F.; De Bont, S.; Fokkens, W.J.; Bachert, C.; Alobid, I.; Bernal-Sprekelsen, M.; Bjermer, L.; Callebaut, I.; Cardell, L.; Carrie, S.; et al. Real-life assessment of chronic rhinosinusitis patients using mobile technology: The mySinusitisCoach project by EUFOREA. Allergy 2020, 75, 2867–2878. [Google Scholar] [CrossRef]
- Detoraki, A.; Tremante, E.; D’Amato, M.; Calabrese, C.; Casella, C.; Maniscalco, M.; Poto, R.; Brancaccio, R.; Boccia, M.; Martino, M.; et al. Mepolizumab improves sino-nasal symptoms and asthma control in severe eo-sinophilic asthma patients with chronic rhinosinusitis and nasal polyps: A 12-month real-life study. Ther. Adv. Respir. Dis. 2021, 15, 17534666211009398. [Google Scholar] [CrossRef]
- Bandi, F.; Gallo, S.; Preti, A.; Mozzanica, F.; Visca, D.; Marelli, M.; Maddalone, E.; Gambarini, C.; Vaghi, A.; Spanevello, A.; et al. Effects of biological therapies on chronic rhinosinusitis in severe asthmatic patients. Acta Otorhinolaryngol. Ital. 2020, 40, 435–443. [Google Scholar] [CrossRef]
- Hopkins, C.; Bachert, C.; Fokkens, W.; Desrosiers, M.; Wagenmann, M.; Lee, S.; Sousa, A.; Smith, S.; Martin, N.; Mayer, B.; et al. Late Breaking Abstract—Add-on mepolizumab for chronic rhinosinusitis with nasal polyps: SYNAPSE study. Eur. Respir. J. 2020, 56, 4616. [Google Scholar] [CrossRef]
- Lemiere, C.; Taillé, C.; Lee, J.K.; Smith, S.G.; Mallett, S.; Albers, F.C.; Bradford, E.S.; Yancey, S.W.; Liu, M.C. Impact of baseline clinical asthma characteristics on the response to mepolizumab: A post hoc meta-analysis of two Phase III trials. Respir. Res. 2021, 22, 184. [Google Scholar] [CrossRef]
- Guida, G.; Rolla, G.; Badiu, I.; Marsico, P.; Pizzimenti, S.; Bommarito, L.; De Stefani, A.; Usai, A.; Bugiani, M.; Malinovschi, A.; et al. Determinants of Exhaled Nitric Oxide in Chronic Rhinosinusitis. Chest 2010, 137, 658–664. [Google Scholar] [CrossRef]
- Paoletti, G.; Melone, G.; Guida, G.; Pirola, F.; Malvezzi, L.; Pelaia, C.; Mariani, A.; Racca, F.; Malipiero, G.; Ferri, S.; et al. Extended nitric oxide analysis in patients with chronic rhinosinusitis with nasal polyps, with or without associated asthma. J. Breath Res. 2020, 15, 016007. [Google Scholar] [CrossRef]
- Tiotiu, A.; Mendez-Brea, P.; Ioan, I.; Romero-Fernandez, R.; Oster, J.P.; Hoang, T.-C.; Roux, P.; Ochoa-Gutierrez, D.C.; Bonniaud, P.; de Blay, F.; et al. Real-Life Effectiveness of Benralizumab, Mepolizumab and Omalizumab in Severe Allergic Asthma Associated with Nasal Polyps. Clin. Rev. Allergy Immunol. 2022, 1–14. [Google Scholar] [CrossRef]
- Lou, H.; Zhang, N.; Bachert, C.; Zhang, L. Highlights of eosinophilic chronic rhinosinusitis with nasal polyps in definition, prognosis, and advancement. Int. Forum Allergy Rhinol. 2018, 8, 1218–1225. [Google Scholar] [CrossRef]
- Koski, R.R.; Hill, L.; Taavola, K. Efficacy and Safety of Biologics for Chronic Rhinosinusitis With Nasal Polyps. J. Pharm. Technol. 2022, 38, 289–296. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Male | Female | Overall | |
|---|---|---|---|
| Number of patients, n (%) | 20 (36) | 35 (64) | 55 |
| Age in years, mean ± SD | 53.3 ± 9.9 | 53.9 ± 11.7 | 53.7 ± 11.0 |
| Chronic rhinosinusitis with nasal polyps (CRSwNP), yes, n (%) | 20 (100) | 35 (100) | 55 (100) |
| Endoscopic sinus surgery (ESS), yes, n (%) | 11 (55) | 19 (54) | 30 (55) |
| Endoscopic sinus surgery (ESS), median (IQR) | 1 (0;2) | 1 (0;2.8) | 1 (0;2) |
| Asthma, yes, n (%) | 17 (85) | 32 (91) | 49 (89) |
| Respiratory disease exacerbated by aspirin and nonsteroidal anti-inflammatory drugs (AERD), yes, n (%) | 11 (55) | 17 (49) | 28 (51) |
| Smoker, yes, n (%) | 5 (25) | 4 (11) | 9 (16) |
| Allergic, yes, n (%) | 10 (50) | 19 (54) | 29 (53) |
| Corticosteroid dependent, yes, n (%) | 15 (75) | 29 (83) | 44 (80) |
| Lund-Mackay score, median (IQR) | 20 (19;2) | 20 (13;23) | 20 (16;22) |
| Baseline = Pre-Mepo * n = 55 | Post-Mepo * n = 55 | p Value | Median of the Differences, 95% CI | |
|---|---|---|---|---|
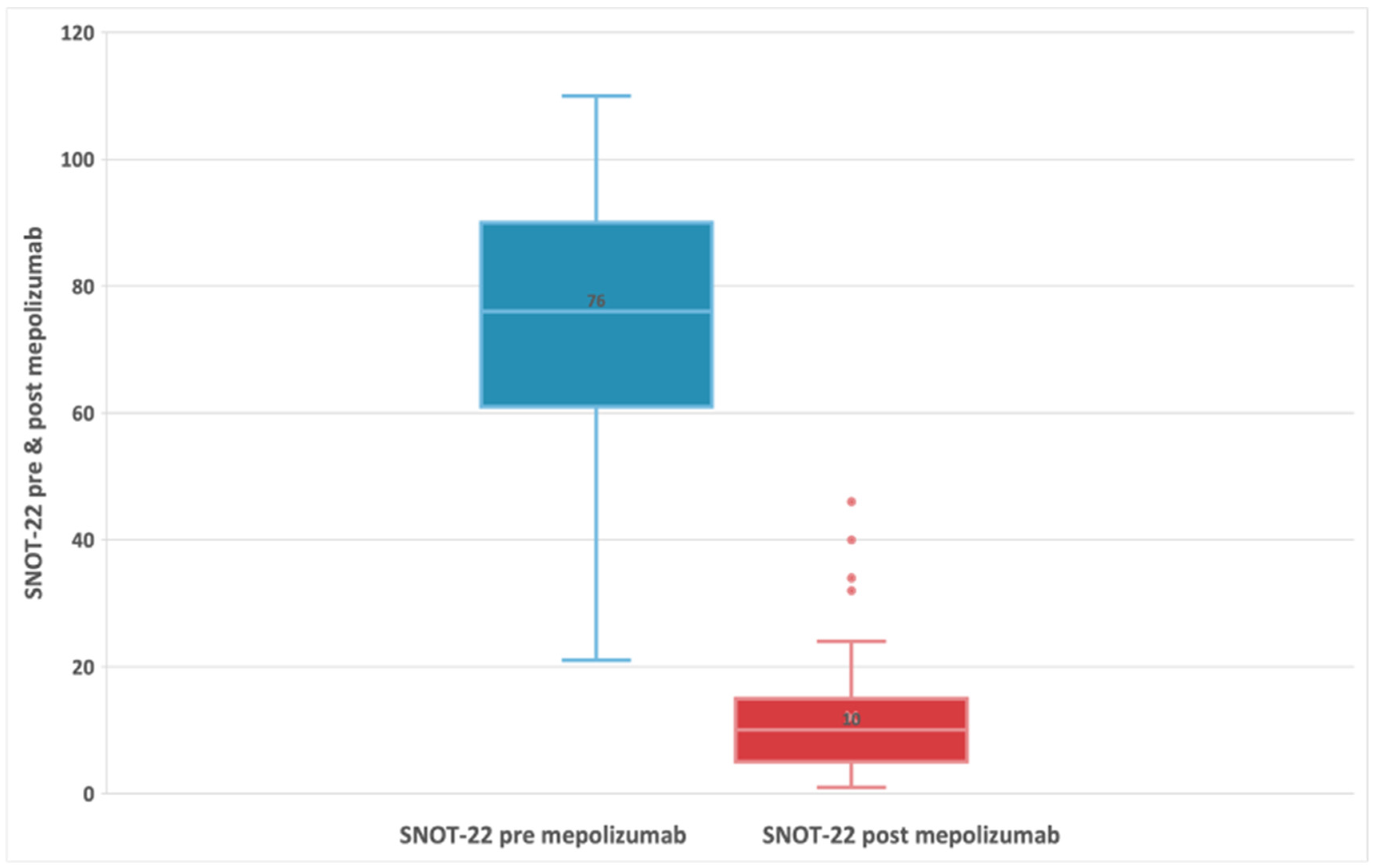
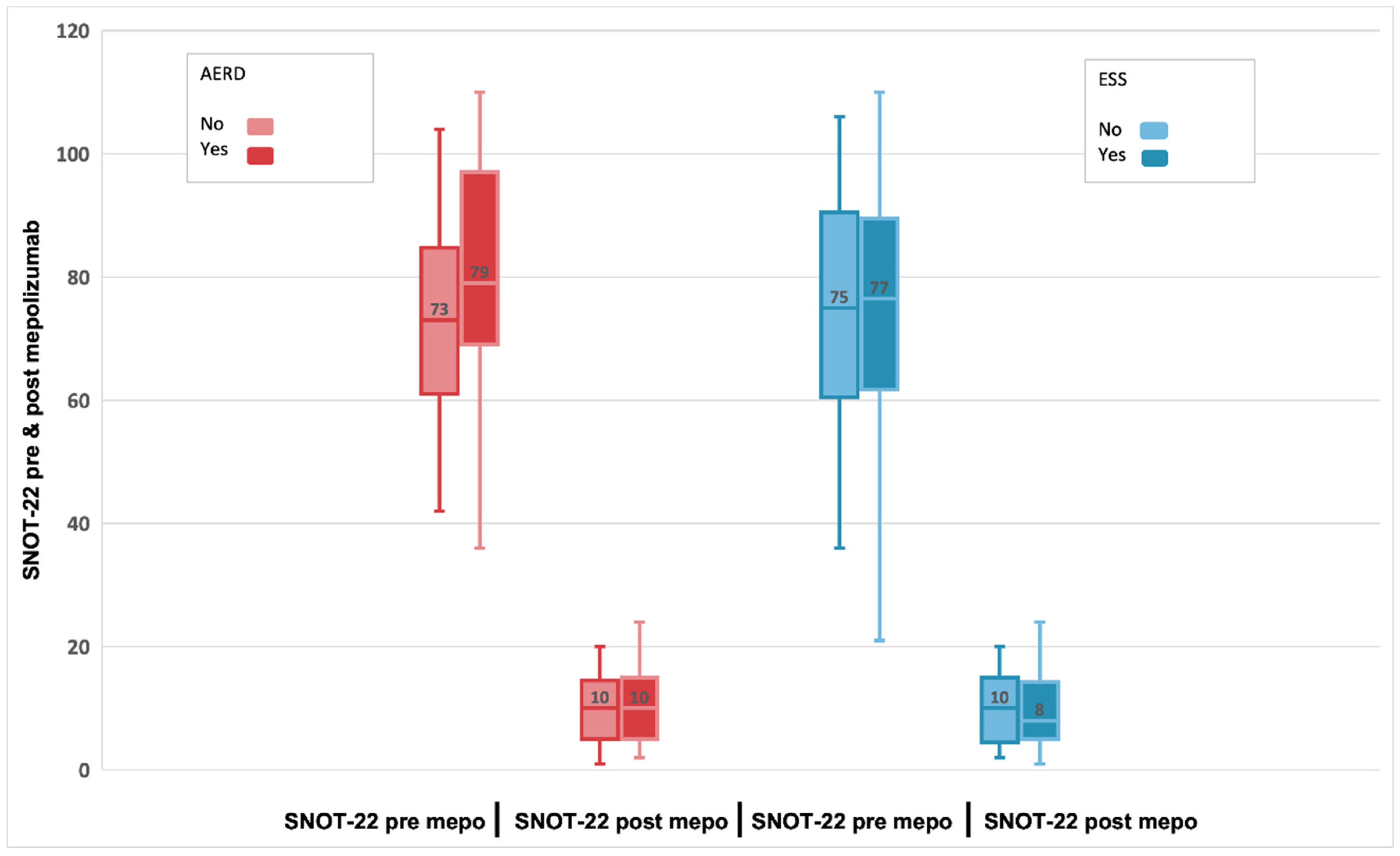
| Sinonasal outcome test (SNOT-22) total score, median (IQR); range 0–110 | 76 (61;90) | 10 (5;15) | <0.001 § | −63, (−68; −58) † |
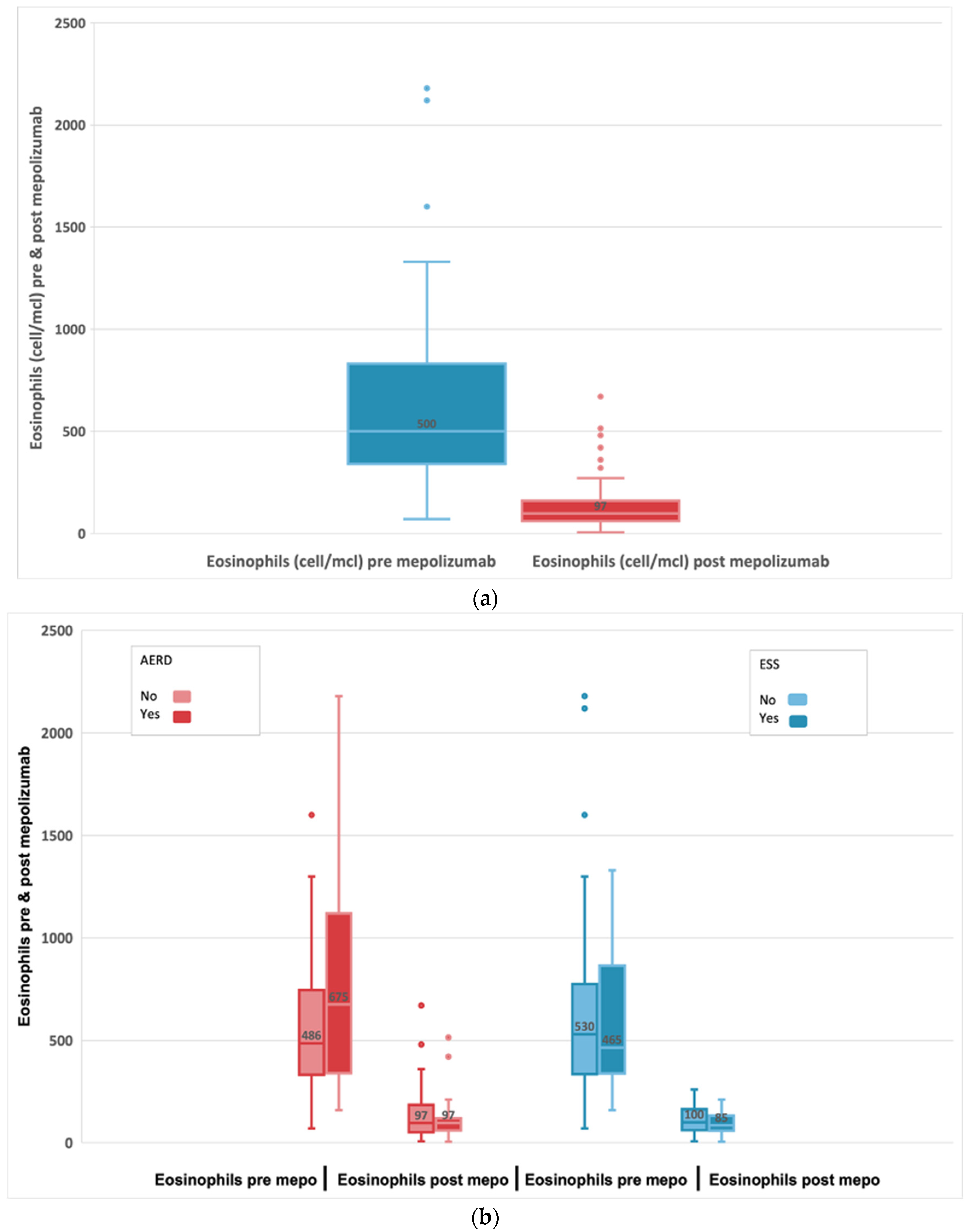
| Eosinophils (cell/mcl), median (IQR) | 500 (340;830) | 97 (60;160) | <0.001 § | −460, (−610; −353) † |
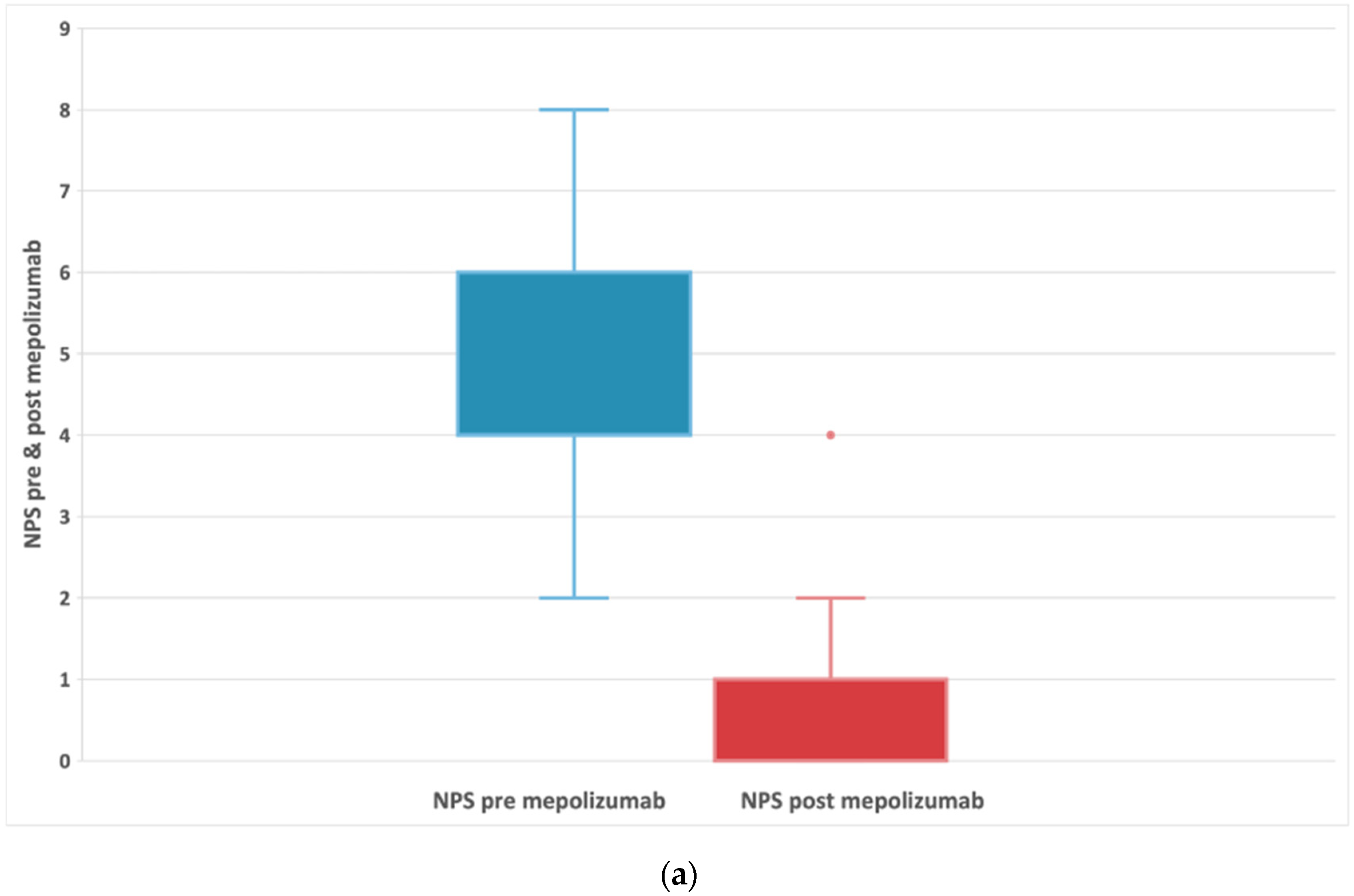
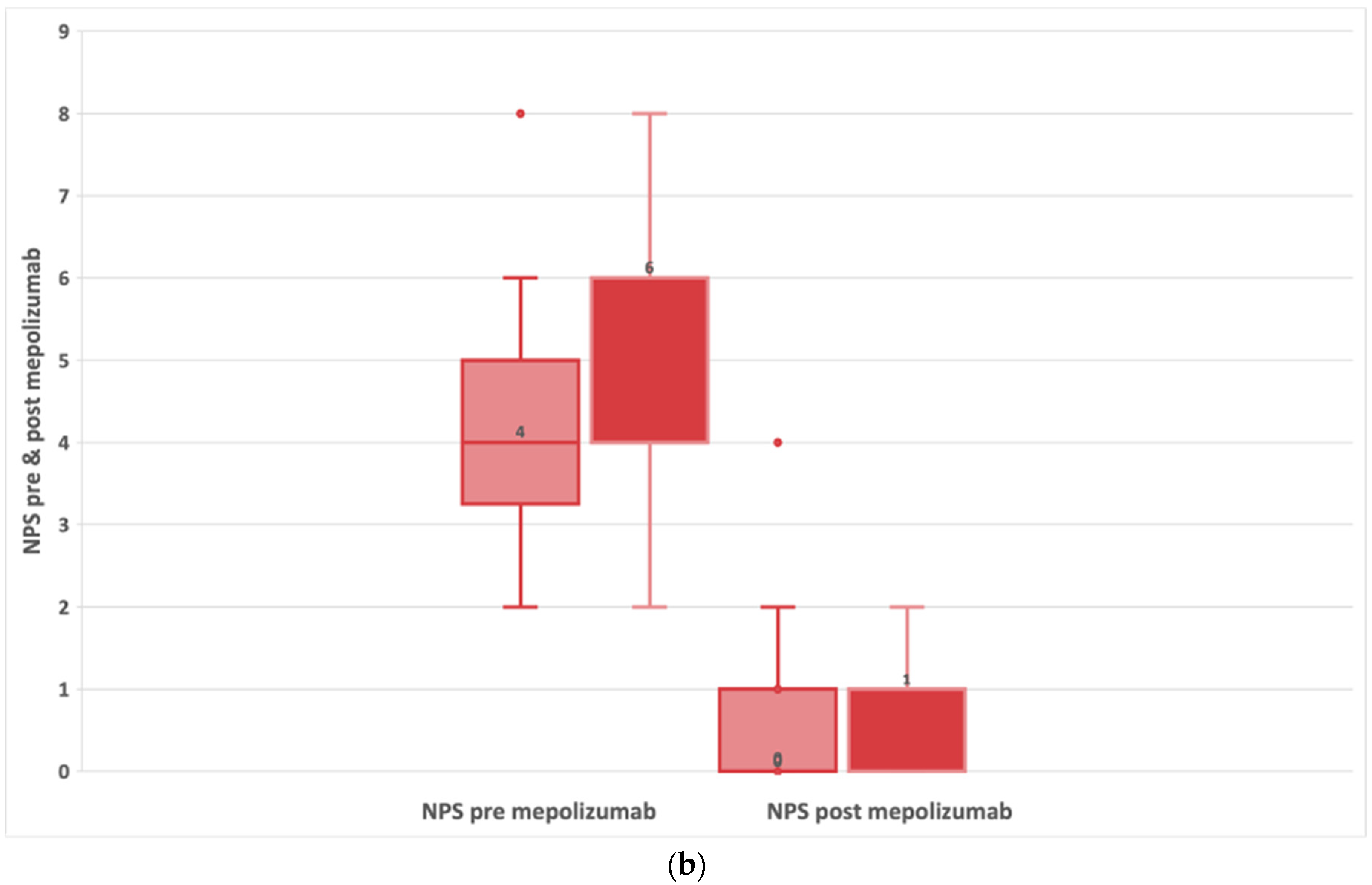
| Nasal endoscopic polyp score (NPS), median (IQR); range 0–8 | 4 (4;6) | 1 (0;1) | <0.001 § | −4, (−4.5; −3.5) † |
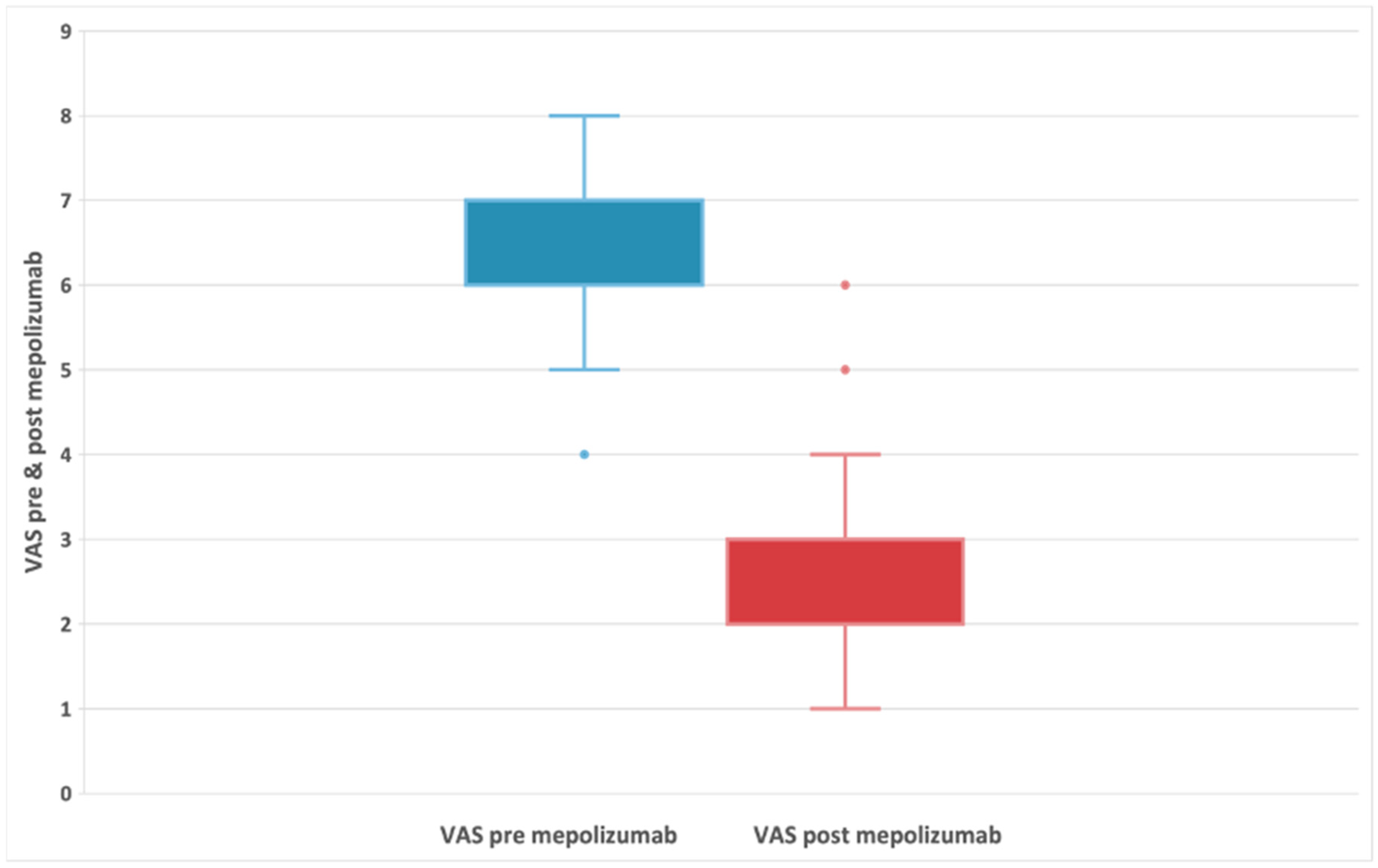
| Visual analogue scale (VAS), median (IQR) | 6 (6;7) | 2 (2;3) | <0.001 § | −4, (−4; −4) † |
| Asthma control test (ACT) total score, median (IQR); range 5–25 | 11 (5;25) | 21 (8;25) | <0.05 § | |
| Fractional exhaled nitric oxide (FeNO) ppb, median (IQR) | 50 (36;130) | 23 (14;36) | <0.05 § | |
| Oral corticosteroid use (OCS), yes, n (%) | 53 (96.4) | 2 (3.6) | <0.001 ‡ | |
| Hyposmia/Anosmia, yes, n (%) | 52 (94.5) | 19 (34.5) | <0.001 ‡ | |
| Nasal Obstruction, yes, n (%) | 52 (94.5) | 14 (25.5) | <0.001 ‡ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Domínguez-Sosa, M.S.; Cabrera-Ramírez, M.S.; Marrero-Ramos, M.d.C.; Dávila-Quintana, D.; Cabrera-López, C.; Carrillo-Díaz, T.; del Rosario, J.J.B. Real-Life Effectiveness of Mepolizumab in Refractory Chronic Rhinosinusitis with Nasal Polyps. Biomedicines 2023, 11, 485. https://doi.org/10.3390/biomedicines11020485
Domínguez-Sosa MS, Cabrera-Ramírez MS, Marrero-Ramos MdC, Dávila-Quintana D, Cabrera-López C, Carrillo-Díaz T, del Rosario JJB. Real-Life Effectiveness of Mepolizumab in Refractory Chronic Rhinosinusitis with Nasal Polyps. Biomedicines. 2023; 11(2):485. https://doi.org/10.3390/biomedicines11020485
Chicago/Turabian StyleDomínguez-Sosa, María Sandra, María Soledad Cabrera-Ramírez, Miriam del Carmen Marrero-Ramos, Delia Dávila-Quintana, Carlos Cabrera-López, Teresa Carrillo-Díaz, and Jesús Javier Benítez del Rosario. 2023. "Real-Life Effectiveness of Mepolizumab in Refractory Chronic Rhinosinusitis with Nasal Polyps" Biomedicines 11, no. 2: 485. https://doi.org/10.3390/biomedicines11020485
APA StyleDomínguez-Sosa, M. S., Cabrera-Ramírez, M. S., Marrero-Ramos, M. d. C., Dávila-Quintana, D., Cabrera-López, C., Carrillo-Díaz, T., & del Rosario, J. J. B. (2023). Real-Life Effectiveness of Mepolizumab in Refractory Chronic Rhinosinusitis with Nasal Polyps. Biomedicines, 11(2), 485. https://doi.org/10.3390/biomedicines11020485