
Oral Brincidofovir Therapy for Monkeypox Outbreak: A Focused Review on the Therapeutic Potential, Clinical Studies, Patent Literature, and Prospects

 ,
,  , ,
, ,  ,
,  , , and
, , and 
Abstract
1. Introduction
2. Brincidofovir (BCV)
2.1. Chemistry
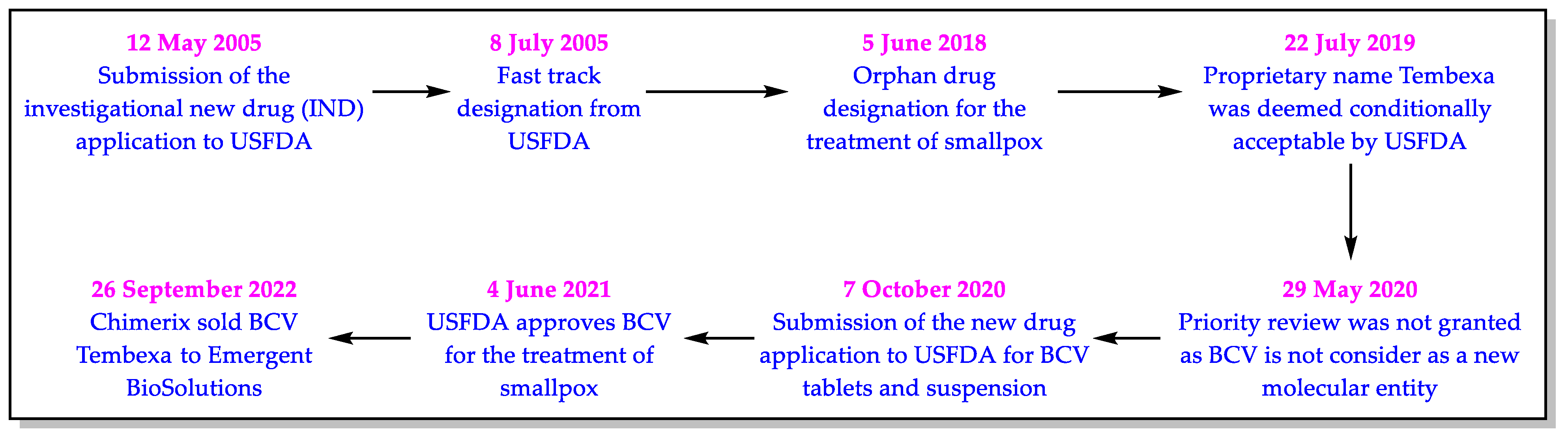
2.2. Regulatory Approval
2.3. Pharmacology of BCV
2.3.1. In Vitro Anti-OPXV Activity of BCV
2.3.2. Efficacy of BCV in Animal Model
2.3.3. Mechanism of Action of BCV
2.3.4. Other Pharmacological Parameters of BCV
3. Clinical Studies (CSs) on BCV
4. Patent Searching and Patent Summary
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- MacNeill, A.L. Comparative pathology of zoonotic orthopoxviruses. Pathogens 2022, 11, 892. [Google Scholar] [CrossRef] [PubMed]
- Kampf, G. Efficacy of biocidal agents and disinfectants against the monkeypox virus and other orthopoxviruses. J. Hosp. Infect. 2022, 127, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Almehmadi, M.; Allahyani, M.; Alsaiari, A.A.; Alshammari, M.K.; Alharbim, A.S.; Hussain, K.H.; Alsubaihi, L.I.; Kamal, M.; Alotaibi, S.S.; Alotaibi, A.N.; et al. A glance at the development and patent literature of tecovirimat: The first-in-class therapy for emerging monkeypox outbreak. Viruses 2022, 14, 1870. [Google Scholar] [CrossRef] [PubMed]
- Multi-Country Outbreak of Monkeypox, External Situation Report #8. Available online: https://www.who.int/publications/m/item/multi-country-outbreak-of-monkeypox--external-situation-report--8---19-october-2022 (accessed on 29 October 2022).
- Moore, M.; Zahra, F. Monkeypox. In StatPearls [Internet]; StatPearls Publishing: Tampa, FL, USA, 2022. [Google Scholar]
- Kabuga, A.I.; El Zowalaty, M.E. A review of the monkeypox virus and a recent outbreak of skin rash disease in Nigeria. J. Med. Virol. 2019, 91, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.; Leggat, P.A. Human monkeypox: Current state of knowledge and implications for the future. Trop. Med. Infect. Dis. 2016, 1, 8. [Google Scholar] [CrossRef]
- Learned, L.A.; Reynolds, M.G.; Wassa, D.W.; Li, Y.; Olson, V.A.; Karem, K.; Stempora, L.L.; Braden, Z.H.; Kline, R.; Likos, A.; et al. Extended interhuman transmission of monkeypox in a hospital community in the Republic of the Congo, 2003. Am. J. Trop. Med. Hyg. 2005, 73, 428–434. [Google Scholar] [CrossRef]
- Huhn, G.D.; Bauer, A.M.; Yorita, K.; Graham, M.B.; Sejvar, J.; Likos, A.; Damon, I.K.; Reynolds, M.G.; Kuehnert, M.J. Clinical characteristics of human monkeypox, and risk factors for severe disease. Clin. Infect. Dis. 2005, 41, 1742–1751. [Google Scholar] [CrossRef]
- Zhu, M.; Ji, J.; Shi, D.; Lu, X.; Wang, B.; Wu, N.; Wu, J.; Yao, H.; Li, L. Unusual global outbreak of monkeypox: What should we do? Front. Med. 2022, 16, 507–517. [Google Scholar] [CrossRef]
- Out, A.; Ebenso, B.; Walley, J.; Barceló, J.M.; Ochu, C.L. Global human monkeypox outbreak: Atypical presentation demanding urgent public health action. Lancet Microbe. 2022, 3, e554–e555. [Google Scholar]
- Adler, H.; Gould, S.; Hine, P.; Snell, L.B.; Wong, W.; Houlihan, C.F.; Osborne, J.C.; Rampling, T.; Beadsworth, M.B.; Duncan, C.J.; et al. NHS England High Consequence Infectious Diseases (Airborne) Network. Clinical features and management of human monkeypox: A retrospective observational study in the UK. Lancet Infect. Dis. 2022, 22, 1153–1162. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Monkeypox Symptoms. Available online: https://www.cdc.gov/poxvirus/monkeypox/symptoms.html (accessed on 29 October 2022).
- World Health Organization. Monkeypox. Available online: https://www.who.int/news-room/fact-sheets/detail/monkeypox (accessed on 29 October 2022).
- Jain, N.; Lansiaux, E.; Simanis, R. The new face of monkeypox virus: An emerging global emergency. New Microbes New Infect. 2022, 47, 100989. [Google Scholar] [CrossRef] [PubMed]
- Center for Drug Evaluation and Research. Product Quality Review(s). Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2021/214460Orig1s000,%20214461Orig1s000ChemR.pdf (accessed on 29 October 2022).
- Delaune, D.; Iseni, F. Drug development against smallpox: Present and future. Antimicrob. Agents Chemother. 2020, 64, e01683-19. [Google Scholar] [CrossRef] [PubMed]
- Lanier, R.; Trost, L.; Tippin, T.; Lampert, B.; Robertson, A.; Foster, S.; Rose, M.; Painter, W.; O’Mahony, R.; Almond, M.; et al. Development of CMX001 for the treatment of poxvirus infections. Viruses 2010, 2, 2740–2762. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, M.W. Therapeutic strategies to address monkeypox. Expert Rev. Anti-Infect. 2022, 20, 1249–1252. [Google Scholar] [CrossRef] [PubMed]
- Foster, S.A.; Parker, S.; Lanier, R. The role of brincidofovir in preparation for a potential smallpox outbreak. Viruses 2017, 9, 320. [Google Scholar] [CrossRef] [PubMed]
- Tembexa. Available online: https://www.chimerix.com/products/tembexa/ (accessed on 29 October 2022).
- Orange Book. Approved Drug Products with Therapeutic Equivalence Evaluation. Available online: https://www.accessdata.fda.gov/scripts/cder/ob/index.cfm (accessed on 29 October 2022).
- Rizk, J.G.; Lippi, G.; Henry, B.M.; Forthal, D.N.; Rizk, Y. Prevention and treatment of monkeypox. Drugs 2022, 82, 957–963. [Google Scholar] [CrossRef]
- Anderson, P.O. Monkeypox prevention and treatment while nursing. Breastfeed. Med. 2022, 17, 707–708. [Google Scholar] [CrossRef]
- Aldhaeefi, M.; Rungkitwattanakul, D.; Unonu, J.; Franklin, C.J.; Lyons, J.; Hager, K.; Daftary, M.N. The 2022 human monkeypox outbreak: Clinical review and management guidance. Am. J. Health Syst. Pharm. 2022, 80, 44–52. [Google Scholar] [CrossRef]
- Center for Drug Evaluation and Research. Clinical Microbiology/Virology Review(s). Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2021/214460Orig1s000,%20214461Orig1s000MicroR.pdf (accessed on 29 October 2022).
- Olson, V.A.; Smith, S.K.; Foster, S.; Li, Y.; Lanier, E.R.; Gates, I.; Trost, L.C.; Damon, I.K. In vitro efficacy of brincidofovir against variola virus. Antimicrob. Agents Chemother. 2014, 58, 5570–5571. [Google Scholar] [CrossRef]
- Bidanset, D.J.; Beadle, J.R.; Wan, W.B.; Hostetler, K.Y.; Kern, E.R. Oral activity of ether lipid ester prodrugs of cidofovir against experimental human cytomegalovirus infection. J. Infect. Dis. 2004, 190, 499–503. [Google Scholar] [CrossRef]
- Buller, R.M.; Owens, G.; Schriewer, J.; Melman, L.; Beadle, J.R.; Hostetler, K.Y. Efficacy of oral active ether lipid analogs of cidofovir in a lethal mousepox model. Virology 2004, 318, 474–481. [Google Scholar] [CrossRef] [PubMed]
- Duraffour, S.; Mertens, B.; Meyer, H.; van den Oord, J.J.; Mitera, T.; Matthys, P.; Snoeck, R.; Andrei, G. Emergence of cowpox: Study of the virulence of clinical strains and evaluation of antivirals. PLoS ONE 2013, 8, e55808. [Google Scholar] [CrossRef] [PubMed]
- Chan-Tack, K.; Harrington, P.; Bensman, T.; Choi, S.Y.; Donaldson, E.; O’Rear, J.; McMillan, D.; Myers, L.; Seaton, M.; Ghantous, H.; et al. Benefit-risk assessment for brincidofovir for the treatment of smallpox: U.S. Food and Drug Administration’s Evaluation. Antivir. Res. 2021, 195, 105182. [Google Scholar] [CrossRef]
- Center for Drug Evaluation and Research. Risk Assessment and Risk Mitigation Review(s). Available online: http://www.accessdata.fda.gov/drugsatfda_docs/nda/2021/214460Orig1s000,%20214461Orig1s000RiskR.pdf (accessed on 29 October 2022).
- Center for Drug Evaluation and Research. Labeling. Available online: http://www.accessdata.fda.gov/drugsatfda_docs/nda/2021/214460Orig1s000,%20214461Orig1s000lbl.pdf (accessed on 29 October 2022).
- Hutson, C.L.; Kondas, A.V.; Mauldin, M.R.; Doty, J.B.; Grossi, I.M.; Morgan, C.N.; Ostergaard, S.D.; Hughes, C.M.; Nakazawa, Y.; Kling, C.; et al. Pharmacokinetics and efficacy of a potential smallpox therapeutic, brincidofovir, in a lethal monkeypox virus animal model. mSphere 2021, 6, e00927-20. [Google Scholar] [CrossRef] [PubMed]
- Center for Drug Evaluation and Research. Clinical Pharmacology and Biopharmaceutics Review(s). Available online: http://www.accessdata.fda.gov/drugsatfda_docs/nda/2021/214460Orig1s000,%20214461Orig1s000ClinPharmR.pdf (accessed on 29 October 2022).
- National Institute of Health. Available online: http://www.clinicaltrials.gov/ (accessed on 29 October 2022).
- Marty, F.M.; Winston, D.J.; Chemaly, R.F.; Mullane, K.M.; Shore, T.B.; Papanicolaou, G.A.; Chittick, G.; Brundage, T.M.; Wilson, C.; Morrison, M.E.; et al. SUPPRESS Trial Clinical Study Group. A randomized, double-blind, placebo-controlled phase 3 trial of oral brincidofovir for cytomegalovirus prophylaxis in allogeneic hematopoietic cell transplantation. Biol. Blood Marrow. Transpl. 2019, 25, 369–381. [Google Scholar] [CrossRef]
- Hiwarkar, P.; Amrolia, P.; Sivaprakasam, P.; Lum, S.H.; Doss, H.; O’Rafferty, C.; Petterson, T.; Patrick, K.; Silva, J.; Slatter, M.; et al. United Kingdom Paediatric Bone Marrow Transplant Group. Brincidofovir is highly efficacious in controlling adenoviremia in pediatric recipients of hematopoietic cell transplants. Blood 2017, 129, 2033–2037. [Google Scholar] [CrossRef]
- Chittick, G.; Morrison, M.; Brundage, T.; Nichols, W.G. Short-term clinical safety profile of brincidofovir: A favorable benefit-risk proposition in the treatment of smallpox. Antivir. Res. 2017, 143, 269–277. [Google Scholar] [CrossRef]
- Grimley, M.S.; Chemaly, R.F.; Englund, J.A.; Kurtzberg, J.; Chittick, G.; Brundage, T.M.; Bae, A.; Morrison, M.E.; Prasad, V.K. Brincidofovir for asymptomatic adenovirus viremia in pediatric and adult allogeneic hematopoietic cell transplant recipients: A randomized placebo-controlled phase II trial. Biol. Blood Marrow Transpl. 2017, 23, 512–521. [Google Scholar] [CrossRef]
- Dunning, J.; Kennedy, S.B.; Antierens, A.; Whitehead, J.; Ciglenecki, I.; Carson, G.; Kanapathipillai, R.; Castle, L.; Howell-Jones, R.; Pardinaz-Solis, R.; et al. RAPIDE-BCV trial team. Experimental treatment of ebola virus disease with brincidofovir. PLoS ONE 2016, 11, e0162199. [Google Scholar] [CrossRef]
- Lanier, E.R.; Foster, S.; Brundage, T.; Chou, S.; Prichard, M.N.; Kleiboeker, S.; Wilson, C.; Colville, D.; Mommeja-Marin, H. Analysis of mutations in the gene encoding cytomegalovirus DNA polymerase in a phase 2 clinical trial of brincidofovir prophylaxis. J. Infect. Dis. 2016, 214, 32–35. [Google Scholar] [CrossRef]
- Marty, F.M.; Winston, D.J.; Rowley, S.D.; Vance, E.; Papanicolaou, G.A.; Mullane, K.M.; Brundage, T.M.; Robertson, A.T.; Godkin, S.; Momméja-Marin, H.; et al. CMX001-201 Clinical Study Group. CMX001 to prevent cytomegalovirus disease in hematopoietic-cell transplantation. N. Engl. J. Med. 2013, 369, 1227–1236. [Google Scholar] [CrossRef] [PubMed]
- Painter, W.; Robertson, A.; Trost, L.C.; Godkin, S.; Lampert, B.; Painter, G. First pharmacokinetic and safety study in humans of the novel lipid antiviral conjugate CMX001, a broad-spectrum oral drug active against double-stranded DNA viruses. Antimicrob. Agents Chemother. 2012, 56, 2726–2734. [Google Scholar] [CrossRef] [PubMed]
- Imran, M.; Khan, S.A.; Alshammari, M.K.; Alreshidi, M.A.; Alreshidi, A.A.; Alghonaim, R.S.; Alanazi, F.A.; Alshehri, S.; Ghoneim, M.M.; Shakeel, F. Discovery, development, inventions, and patent trends on mobocertinib succinate: The first-in-class oral treatment for NSCLC with EGFR exon 20 insertions. Biomedicines 2021, 9, 1938. [Google Scholar] [CrossRef] [PubMed]
- Imran, M.; Khan, S.A.; Abida; Alshrari, A.S.; Eltahir, M.M.; Alshammari, M.K.; Harshan, A.A.; Alshammari, N.A. Small molecules as kinetoplastid specific proteasome inhibitors for leishmaniasis: A patent review from 1998 to 2021. Expert Opin. Pat. 2022, 32, 591–604. [Google Scholar] [CrossRef]
- Imran, M.; Fatima, W.; Alzahrani, A.K.; Suhail, N.; Alshammari, M.K.; Alghitran, A.A.; Alshammari, F.N.; Ghoneim, M.M.; Alshehri, S.; Shakeel, F. Development of therapeutic and prophylactic zinc compositions for use against COVID-19: A glimpse of the trends, inventions, and patents. Nutrients 2022, 14, 1227. [Google Scholar] [CrossRef]
- Imran, M.; Thabet, H.K.; Alaqel, S.I.; Alzahrani, A.R.; Abida; Alshammari, M.K.; Kamal, M.; Diwan, A.; Asdaq, S.M.B.; Alshehri, S. The therapeutic and prophylactic potential of quercetin against COVID-19: An outlook on the clinical studies, inventive compositions, and patent literature. Antioxidants 2022, 11, 876. [Google Scholar] [CrossRef]
- Imran, M.; Khan, S.A.; Alshammari, M.K.; Alqahtani, A.M.; Alanazi, T.A.; Kamal, M.; Jawaid, T.; Ghoneim, M.M.; Alshehri, S.; Shakeel, F. Discovery, development, inventions and patent review of fexinidazole: The first all-oral therapy for Human African Trypanosomiasis. Pharmaceuticals 2022, 15, 128. [Google Scholar] [CrossRef]
- Imran, M.; Asdaq, S.M.B.; Khan, S.A.; Unnikrishnan, M.D.; Alamri, A.S.; Alsanie, W.F.; Alhomrani, M.; Mohzari, Y.; Alrashed, A.; AlMotairi, M.; et al. Innovations and patent trends in the development of USFDA approved protein kinase inhibitors in the last two decades. Pharmaceuticals 2021, 14, 710. [Google Scholar] [CrossRef]
- Ware, R.W.; Almond, M.R.; Lampert, B.M. Phosphonate Ester Derivatives and Methods of Synthesis Thereof. U.S. Patent US9303051B2, 5 April 2016. [Google Scholar]
- Ware, J.R.W.; Downey, A.L. Morphic Forms of Hexadecyloxypropyl-Phosphonate Esters and Methods of Synthesis Thereof. U.S. Patent US8962829B1, 24 February 2015. [Google Scholar]
- Ware, J.R.W.; Downey, A.L. Morphic forms of Hexadecyloxypropyl-Phosphonate Esters and Methods of Synthesis Thereof. U.S. Patent US9371344B2, 21 June 2016. [Google Scholar]
- Ware, R.W.; Downey, A.L. Morphic Forms of Hexadecyloxypropyl-Phosphonate Esters and Methods of Synthesis Thereof. U.S. Patent US10487061B2, 26 November 2019. [Google Scholar]
- Ware, R.W.; Downey, A.L. Morphic Forms of Hexadecyloxypropyl-Phosphonate Esters and Methods of Synthesis Thereof. U.S. Patent US10112909B2, 30 October 2018. [Google Scholar]
- Ware, R.W.; Almond, M.R.; Lampert, B.M. Phosphonate Ester Derivatives and Methods of Synthesis Thereof. U.S. Patent US8569321B2, 29 October 2013. [Google Scholar]
- Ware, J.R.W.; Downey, A.L. Morphic Forms of Hexadecyloxypropyl-Phosphonate Esters and Methods of Synthesis Thereof. U.S. Patent US9862687B2, 9 January 2018. [Google Scholar]
- Ware, R.W.; Downey, A.L. Morphic Forms of Hexadecyloxypropyl-Phosphonate Esters and Methods of Synthesis Thereof. U.S. Patent US11066373B2, 20 July 2021. [Google Scholar]
- Vainorius, E.; Brundage, T.; Chittick, G.; Nichols, W.G.; Painter, G.R. Treatment of Adenovirus with Brincidofovir. PCT Patent Application Publication Number WO2018156879A1, 30 August 2018. [Google Scholar]
- Ware, R.W.; Kabir, M.A.; Naderer, O.J.; Grossi, I.M. Formulations of Brincidofovir. U.S. Patent Application Publication Number US2017368082A1, 28 December 2017. [Google Scholar]
- Kabir, M.A.; Naderer, O.J.; Grossi, I.M. Formulations of Brincidofovir. U.S. Patent Application Publication Number US2020138835A1, 7 May 2020. [Google Scholar]
- Öberg, B.; Broberg, A.; Guss, B.; Levenfors, J.; Bjerketorp, J.; Nord, C. Method of Treating Bacterial Infections. U.S. Patent US10828317B2, 10 November 2020. [Google Scholar]
- Kowalik, T.F.; Rodriguez-Gonzalez, M.; Lagadinos, A. Modulation of Human Cytomegalovirus Replication by micro-RNA 132 (miR132), micro-RNA 145 (miR145) and micro-RNA 212 (miR212). U.S. Patent US9562232B2, 7 February 2017. [Google Scholar]
- Kyratsous, C.; Olson, W.; Mason, P.; Stahl, N. Human Antibodies to Ebola Virus Glycoprotein. U.S. Patent US10081670B2, 25 September 2018. [Google Scholar]
- Checcone, E.A.; Ramirez, C. Viral Prophylaxis Treatment Methods and Pre-Exposure Prophylaxis Kits. U.S. Patent US11071745B2, 27 July 2021. [Google Scholar]
- Komanduri, K.; Wieder, E.; Camargo, J.; Kimble, E. Materials and Methods for Subjects at Risk for Viral Reactivation. U.S. Patent US2020072848A1, 5 March 2020. [Google Scholar]
- Wolf, D. Methods and Synergic Compositions for Treating Viral Infections. U.S. Patent US2021000839A1, 7 January 2021. [Google Scholar]
- Baker, B.H.J. Methods of Treating Bone Infections. PCT Patent WO2022072842A1, 7 April 2022. [Google Scholar]
- Millard, J.W.; Baker, B.H.J. Bismuth Thiol Compounds and Compositions and Methods of Treating Microbial Co-Infections. PCT Patent WO2021195236A1, 30 September 2021. [Google Scholar]
- Frenkel-Morgenstern, M.; Mukherjee, S.; Tworowski, D. Molecules that Target Proteins of Coronaviruses and Uses Thereof as Anti-Viral “Cocktail”. PCT Patent WO2021186439A1, 23 September 2021. [Google Scholar]
- Siegrist, E.A.; Sassine, J. Antivirals with activity against monkeypox: A clinically oriented review. Clin. Infect. Dis. 2022, 76, 155–164. [Google Scholar] [CrossRef]
- See, K.C. Vaccination for monkeypox virus infection in humans: A review of key considerations. Vaccines 2022, 10, 1342. [Google Scholar] [CrossRef] [PubMed]
- Hostetler, K.Y. Synthesis and early development of hexadecyloxypropylcidofovir: An oral antipoxvirus nucleoside phosphonate. Viruses 2010, 2, 2213–2225. [Google Scholar] [CrossRef]
- Islam, M.R.; Hossain, M.J.; Roy, A.; Hasan, A.H.M.N.; Rahman, M.A.; Shahriar, M.; Bhuiyan, M.A. Repositioning potentials of smallpox vaccines and antiviral agents in monkeypox outbreak: A rapid review on comparative benefits and risks. Health Sci. Rep. 2022, 5, e798. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Cardona, J.J.; Whited, L.K.; Chemaly, R.F. Brincidofovir: Understanding its unique profile and potential role against adenovirus and other viral infections. Future Microbiol. 2020, 15, 389–400. [Google Scholar] [CrossRef] [PubMed]
- Rice, A.D.; Adams, M.M.; Lampert, B.; Foster, S.; Robertson, A.; Painter, G.; Moyer, R.W. Efficacy of CMX001 as a prophylactic and presymptomatic antiviral agent in New Zealand white rabbits infected with rabbitpox virus, a model for orthopoxvirus infections of humans. Viruses 2011, 3, 63–82. [Google Scholar] [CrossRef] [PubMed]
- Stabenow, J.; Buller, R.M.; Schriewer, J.; West, C.; Sagartz, J.E.; Parker, S. A mouse model of lethal infection for evaluating prophylactics and therapeutics against Monkeypox virus. J. Virol. 2010, 84, 3909–3920. [Google Scholar] [CrossRef]
- Crump, R.; Korom, M.; Buller, R.M.; Parker, S. Buccal viral DNA as a trigger for brincidofovir therapy in the mousepox model of smallpox. Antivir. Res. 2017, 139, 112–116. [Google Scholar] [CrossRef]
- Hussien, M.A.; Abdelaziz, A.E.M. Molecular docking suggests repurposing of brincidofovir as a potential drug targeting SARS-CoV-2 ACE2 receptor and main protease. Netw. Model. Anal. Health Inform. Bioinform. 2020, 9, 56. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Proprietary Name (Active Ingredient; Applicant; Marketing Status) | Dosage Form (Route of Administration) | Strength (Approval Date) | Exclusivity Data | Approved Indication |
|---|---|---|---|---|
| Tembexa (Brincidofovir; Chimerix Inc; Prescription) | Tablet (Oral) | 100 mg (4 June 2021) | New product exclusivity expires on 4 June 2024; Orphan drug exclusivity expires on 4 June 2028 | Treatment of human smallpox diseases caused by variola virus in adult and pediatric patients, including neonates |
| Suspension (Oral) | 10 mg/ mL (4 June 2021) |
| OPXV | Strains | Cells | EC50 Range (µM) |
|---|---|---|---|
| VARV [26] | BSH74, SOM77, JAP51, UNK52, BRZ66, and BSH | BSC-40, Vero 76, and MK2 | 0.04–0.21 |
| Rabbitpox virus (RPXV) [26] | Utrecht | BSC-40 and Vero 76 | 0.5–1.89 |
| Ectromelia virus [26] | Moscow | BSC-40, CV-1, and BSC-1 | 0.125–0.5 |
| VACV [26] | WR, Copenhagen, Lister, Elstree, and IHD | CV-1, HEL, HFF, Vero, C127I, and PHK | 0.004–1.2 |
| CPXV [26] | Brighton and five different isolates | HFF, HEL, and PHK | 0.007–0.6 |
| CMLV [26] | Iran (CML1) | HEL | 0.021–0.024 |
| MPXV [26] | No data | No data | 0.023–0.12 |
| VACV/RPXV chimera [26] | VACV-WR/RPXV E9L | BSC-40 | 1.75 |
| Model | Dose Regimen | Treatment Initiation Day | % Survival | |
|---|---|---|---|---|
| Placebo | BCV | |||
| Rabbitpox [26,32] | 20/5/5 mg/kg (fully effective dose in the rabbitpox model) | Day 4 | 29% | 90% |
| Mousepox [26,32] | 10/5/5 mg/kg (fully effective dose in the mousepox model) | Day 4 | 13% | 78% |
| Parameter | Summary |
|---|---|
| Dose | Maximum 200 mg/day for patients weighing ≥ 48 kg. BCV can be taken on an empty stomach or with a low-fat meal (about 400 calories, 25% fat). Healthy adults tolerated single doses of BCV up to 350 mg PO (tablet) and 50 mg IV and multiple doses (total of 4) of BCV up to 20 mg IV. |
| Treatment duration | Weekly dose for two weeks because CDV-DP has an exceedingly longer duration of action. No dose adjustment is necessary for patients with hepatic/renal impairment because treatment consists of only two doses (day one and day 8). The shorter duration also reduces the chances of adverse reactions. |
| Absorption | Oral bioavailability: 13.4% (Tablet) and 16.8% (suspension); Cmax of BCV: 480 ng/mL; Tmax of BCV: 3 h; absorption decreases with the fatty meal because BCV is an acidic drug. |
| Volume of distribution | 1230 L |
| Protein binding | >99.9% bound to human plasma proteins |
| Blood plasma ratio | 0.48 to 0.61 in healthy adults |
| Metabolism | Acid sphingomyelinase (ASM) is an important enzyme for the metabolism of BCV to CDV. The CYPF42 pathway converts BCV to inactive metabolites (CMX103 and CMX064) (Figure 4). |
| Route of elimination | The metabolites are excreted in urine (51%) and feces (49%). Unchanged BCV has not been detected in urine or feces. |
| Half-life | BCV: 19.3 h; CDV-DP: 113 h |
| Clearance | 44.1 L/h |
| Adverse Effects | Diarrhea; abdominal pain; nausea; vomiting; elevation in hepatic transaminase/bilirubin; toxic to embryo-fetus; human carcinogen; male infertility. |
| Drug interaction | BCV is a substrate of OATP1B1 or 1B3 membrane uptake transporters. BCV exposures can be increased by the concomitant use of OATP1B1 or 1B3 inhibitors. Coadministration of BCV with a proton pump inhibitor could theoretically increase either the absorption rate or the extent of absorption. |
| Contraindication | Avoid BCV coadministration with CDV |
| Toxicity/Overdose | No clinical case of toxicity/overdose was reported. |
| QT prolongation | No significant QTc prolongation effect of BCV (200 mg) was detected in a TQT study using moxifloxacin (400 mg) as the positive control. |
| NCT Numbers (Sponsor; Location) | Condition/Disease (Intervention) | Assessment | Phase (Study Type; Purpose; Number Enrolled) | Status (Completion Date; Last Update on the Database) |
|---|---|---|---|---|
| NCT02087306 (Chimerix; United States) | AdV (BCV) | Safety and efficacy | 3 (Interventional; Treatment; 201) | Completed (August 2016; 13 August 2021) |
| NCT01143181 (Chimerix; United States) | ds-DNAV (BCV) | Treatment | 3 (Interventional; Treatment; 210) | Completed (December 2012; 12 August 2021) |
| NCT01241344 (Chimerix; United States) | AdV (BCV; Placebo) | Safety and efficacy | 2 (Interventional; Treatment; 52) | Completed (June 2013; 21 July 2021) |
| NCT00793598 (Chimerix; United States) | BKV viruria (BCV; Placebo) | Treatment | 1 and 2 (Interventional; Treatment; 29) | Completed (October 2010; 16 August 2021) |
| NCT00942305 (Chimerix; United States) | CMV (BCV; Placebo) | Prevention/control | 2 (Interventional; Prevention; 239) | Completed (January 2012; 16 July 2021) |
| NCT01769170 (Chimerix; United States) | CMV (BCV; Placebo) | Safety and efficacy | 3 (Interventional; Treatment; 452) | Completed (January 2016; 21 July 2021) |
| NCT00780182 (Chimerix and NIH; United States) | Healthy subjects (BCV) | Effect of high-fat food on the bioavailability | 1 (Interventional; Treatment; 24) | Completed (January 2009; 2 February 2010) |
| NCT04542252 (SymBio Pharmaceuticals; Japan) | Drug–drug interaction (BCV; cyclosporine; SyB V-1901) | Pharmacokinetic | 1 (Interventional; Drug interaction; 13) | Completed (January 29, 2021; 27 April 2021) |
| NCT05391724 (Chimerix; United States) | Hepatic impairment (BCV) | Safety and pharmacokinetic | 1 (Interventional; Not mentioned; 25) | Completed (September 2011; 26 May 2022) |
| NCT05511779 (SymBio Pharmaceuticals; Australia) | BKV, nephropathy, and kidney transplantation (BCV) | Safety and tolerability | 2 (Interventional; Treatment; 36) | Not yet recruiting (Not yet recruiting; 23 August 2022) |
| NCT04706923 (SymBio Pharmaceuticals; United States) | AdV (BCV) | Safety and tolerability of IV BCV | 2 (Interventional; Treatment; 24) | Recruiting (Recruiting; 31 May 2022) |
| NCT03481244 (Assistance Publique; France) | AdV (BCV; CCDV) | Efficacy and toxicity | Not mentioned (Observational; Prospective; 400) | Not yet recruiting (Not yet recruiting; 10 February 2020) |
| NCT02439957 (Chimerix; United States) | CMV and kidney transplant infection (BCV; Valganciclovir) | Safety and efficacy of BCV versus valganciclovir | 3 (Interventional; Prevention; 6) | Terminated (Terminated; 16 July 2021) |
| NCT02439970 (Chimerix; United States) | CMV (BCV; Valganciclovir) | Safety and efficacy | 3 (Interventional; Prevention; 5) | Terminated (Terminated; 16 July 2021) |
| NCT03339401 (Chimerix; United States) | AdV (Standard of care (Soc); BCV) | Safety and efficacy | 2 (Interventional; Treatment; 29) | Terminated (Terminated; 25 January 2021) |
| NCT02420080 (Chimerix; United States) | AdV (BCV) | To obtain retrospective data | Not mentioned (Observational; Determine rates of AdV progression and mortality; 100) | Terminated (Terminated; 9 January 2017) |
| NCT02167685 (Chimerix; United States) | Outcomes and survival rates (BCV) | To establish a registry database | Not mentioned (Observational; Prospective; 550) | Terminated (Terminated; 17 May 2019) |
| NCT01610765 (University of Alabama; United States) | Herpes simplex virus (BCV; Placebo) | Safety and dose determination | 1 and 2 (Interventional; Treatment; zero) | Withdrawn (Withdrawn; 7 June 2016) |
| NCT04268966 (Chimerix and USFDA; United States) | EV (BCV) | Safety and tolerability | 2 (Interventional; Treatment; zero) | Withdrawn (Withdrawn; 26 February 2020) |
| NCT02271347 (Chimerix; Not mentioned) | EV (BCV) | Safety and efficacy | 2 (Interventional; Treatment; Zero) | Withdrawn (Withdrawn; 2 February 2015) |
| NCT03532035 (Chimerix; United States) | AdV (BCV; SoC) | Safety, tolerability, and pharmacokinetic | 2 (Interventional; Treatment; Zero) | Withdrawn (Withdrawn; 21 July 2021) |
| NCT02596997 (Chimerix; United States) | AdV (BCV) | Treatment | Not mentioned (Expanded access; Treatment; Not mentioned) | No longer available (Not available; 14 March 2022) |
| Year [Ref. No.] | Summary |
|---|---|
| 2019 [37] | This study is related to NCT01769170 and evaluated oral BCV for the prevention of CMV infection in allogeneic hematopoietic cell transplant (HCT) patients. BCV did not demonstrate a lowering in CMV infections, even after 24 weeks and showed gastrointestinal toxicity. |
| 2017 [38] | The study relates to the treatment of HCT-linked adenoviremia with BCV. BCV was highly efficacious and tolerable in controlling adenoviremia. Abdominal cramps and diarrhea were observed as side effects, but no nephrotoxicity was noticed. |
| 2017 [39] | This study evaluated the BCV benefit-to-risk profile for treating smallpox. BCV was well tolerated in adults and children at doses and durations equivalent to smallpox treatment. Mild gastrointestinal problems and transitory, asymptomatic transaminase increases were most prevalent. |
| 2017 [40] | This CS tested BCV for preventing AdV illness in HCT patients (pediatric/adult). This trial verified BCV’s anti-AdV activity. The most commonly observed side effect was diarrhea. Myelosuppression and nephrotoxicity were not noted. |
| 2016 [41] | This CS focused on BCV’s efficacy against the EV. However, the CS was halted because the BCV’s manufacturer decided to stop working on it as a treatment for EV disease (EVD). No serious side effects were found. Because of the low sample size, it was impossible to determine if BCV worked to treat EVD. |
| 2016 [42] | This study assessed the development of mutation and resistance in CMV’s gene involved in the production of CMV DNA polymerase. The results did not reveal mutation and CMV antiviral resistance among BCV-treated subjects. |
| 2013 [43] | This study is related to NCT00942305 and assessed the safety and efficacy of BCV against CMV infection in allogeneic HCT patients. Patients who took BCV (100 mg two times per week) experienced fewer CMV episodes than those who received a placebo. The most commonly observed side effect was diarrhea. Myelosuppression and nephrotoxicity were not noted. |
| 2012 [44] | The study evaluated BCV’s safety and pharmacokinetics after single and multiple doses. Blood chemistry, hematology, renal function, and intraocular pressure did not change clinically. There were no BCV-related mucosal alterations. Maximum plasma concentrations of BCV were seen 2 to 3 h post-dose. In healthy volunteers, BCV was well tolerated (2 mg/kg or 140 mg) in adults. |
| Patent/Application (Applicant/Status) | Summary of the Claims |
|---|---|
| Patents/patent applications filed by Chimerix | |
| US9303051B2 (Patented case) | This OB-listed patent claims crystalline Form B of BCV. It also claims a pharmaceutical composition comprising BCV and a pharmaceutically acceptable carrier. It further claims the treatment of many viral diseases, including smallpox, MPX, cowpox, camelpox, and ebola using BCV. It also discloses the sodium salt of BCV [51]. |
| US8962829B1 (Patented case) | This OB-listed patent claims crystalline Form II of BCV and its preparation method. It also discloses Form H and some process-related impurities of BCV [52]. |
| US9371344B2 (Patented case) | This OB-listed patent claims a method of preparing Form II of BCV. It also claims a composition of Form II of BCV with compounds designated as compounds A, B, C, and D [53]. |
| US10487061B2 (Patented case) | This OB-listed patent claims a method of preventing/treating viral infections (a double-stranded DNA viral infection) using a composition of Form II of BCV and a pharmaceutically acceptable carrier. It also discloses an amorphous form of BCV [54]. |
| US10112909B2 (Patented case) | This OB-listed patent claims a method of preventing/treating viral infections (ds-DNA viral infection) using Form II of BCV [55]. |
| US8569321B2 (Patented case) | Crystalline Form A of BCV, its pharmaceutical composition, and method of preparation [56]. |
| US9862687B2 (Patented case) | A method of synthesizing a compound that can be used to synthesize BCV [57]. |
| US11066373B2 (Patented case) | A method of preparing crystalline Form II of BCV [58]. |
| WO2018156879A1 (No national phase entry) | The use of BCV in preventing/treating AdV infection in patients experiencing toxic side effects or nephrotoxicity due to other treatments (CDV, cyclic CDV, tenofovir, and adefovir) [59]. |
| US2017368082A1 (Abandoned) | A pharmaceutical composition having a pH of about 8, wherein the composition comprises BCV, a bulking agent, a buffer, and water. It also claims a lyophilized powder containing BCV, mannitol, and arginine. It further relates to using the claimed compositions to treat viral infections, including AdV, CMV, OPXVs, etc. [60]. |
| US2020138835A1 (Abandoned) | A lyophilized powder comprising BCV, mannitol, and arginine. It also claims a method of treating a viral infection (AdV, CMV, OPXVs, etc.) using the claimed lyophilized powder [61]. |
| Patents/patent applications filed by other companies | |
| US10828317B2 (Ultupharma; Patented case) | A composition comprising a nucleoside analog (gemcitabine, didanosine, 5-fluorouracil, CDV, BCV, etc.) capable of decreasing bacterial colonization or infection of a subject; a second compound (uridine or cytidine) capable of reducing mitochondrial toxicity and increasing the antibacterial effect of the nucleoside analog; and iclaprim capable of decreasing the concentration in bacteria of nucleosides and nucleotides known to compete with nucleoside analogs [62]. |
| US9562232B2 (University of Massachusetts; Patented case) | A method of inhibiting HCMV replication in a cell using a miR132 antagonist (antisense locked nucleic acid) alone or in combination with an antiviral agent (CDV, BCV, ganciclovir, valganciclovir, and acyclovir) [63]. |
| US10081670B2 (Regeneron Pharmaceuticals; Patented case) | A method of neutralizing infectious EBV utilizing anti-EBV antibodies or antigen-binding fragments alone or in combination with additional antiviral agents (BCV and favipiravir) [64]. |
| US11071745B2 (Elian; Patented case) | A method of preventing HSV infection employing a composition comprising valacyclovir and famciclovir, which may additionally include CDV or BCV [65]. |
| US2020072848A1 (University of Miami; Under examination) | A prophylactic method for an immune-compromised patient (organ transplant or cancer therapy patient) with a high risk of viral infection using an antiviral agent (CDV, BCV, and letermovir) [66]. |
| US2021000839A1 (Hadasit Medical Research Services and Development; Under examination) | A method of treating a viral infection (HSV and CMV) in a patient (newborn, a pregnant woman, and a transplant recipient) using a synergistic combination of an antiviral agent (BCV, CDV, valganciclovir, letermovir, and ganciclovir) and artemisone [67]. |
| WO2022072842A1 (Microbion Corporation; No national phase entry) | A method for treating osteomyelitis using a bismuth-thiol (BT) composition alone or in combination with an antimicrobial agent (BCV) [68]. |
| WO2021195236A1 (Microbion Corporation; No national phase entry) | A method for treating respiratory viral infection (viral pneumonia, viral bronchiolitis, and post-lung transplantation) using a bismuth-thiol (BT) composition alone or in combination with an antimicrobial agent (BCV) [69]. |
| WO2021186439A1 (Bar-Ilan University; No national phase entry) | A method of treating coronavirus infection using a combination of a macrolide (azithromycin) and a corticosteroid (desoxycortone), wherein this combination may optionally contain BCV [70]. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Imran, M.; Alshammari, M.K.; Arora, M.K.; Dubey, A.K.; Das, S.S.; Kamal, M.; Alqahtani, A.S.A.; Sahloly, M.A.Y.; Alshammari, A.H.; Alhomam, H.M.; et al. Oral Brincidofovir Therapy for Monkeypox Outbreak: A Focused Review on the Therapeutic Potential, Clinical Studies, Patent Literature, and Prospects. Biomedicines 2023, 11, 278. https://doi.org/10.3390/biomedicines11020278
Imran M, Alshammari MK, Arora MK, Dubey AK, Das SS, Kamal M, Alqahtani ASA, Sahloly MAY, Alshammari AH, Alhomam HM, et al. Oral Brincidofovir Therapy for Monkeypox Outbreak: A Focused Review on the Therapeutic Potential, Clinical Studies, Patent Literature, and Prospects. Biomedicines. 2023; 11(2):278. https://doi.org/10.3390/biomedicines11020278
Chicago/Turabian StyleImran, Mohd., Mohammed Kanan Alshammari, Mandeep Kumar Arora, Amit Kumar Dubey, Sabya Sachi Das, Mehnaz Kamal, Abdulaziz Saad Abdulrahman Alqahtani, Mohammed Ahmed Yahya Sahloly, Ahmed Hammad Alshammari, Hessah Mohammed Alhomam, and et al. 2023. "Oral Brincidofovir Therapy for Monkeypox Outbreak: A Focused Review on the Therapeutic Potential, Clinical Studies, Patent Literature, and Prospects" Biomedicines 11, no. 2: 278. https://doi.org/10.3390/biomedicines11020278
APA StyleImran, M., Alshammari, M. K., Arora, M. K., Dubey, A. K., Das, S. S., Kamal, M., Alqahtani, A. S. A., Sahloly, M. A. Y., Alshammari, A. H., Alhomam, H. M., Mahzari, A. M., Abida, Rabaan, A. A., & Dzinamarira, T. (2023). Oral Brincidofovir Therapy for Monkeypox Outbreak: A Focused Review on the Therapeutic Potential, Clinical Studies, Patent Literature, and Prospects. Biomedicines, 11(2), 278. https://doi.org/10.3390/biomedicines11020278