
Evaluation of the Kinetics of Pancreatic Stone Protein as a Predictor of Ventilator-Associated Pneumonia

 , ,
, ,  , , , , ,
, , , , ,  ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Inclusion and Exclusion Criteria
2.2. Measurement of PSP
2.3. Definitions
2.4. Outcomes
2.5. Statistical Analysis
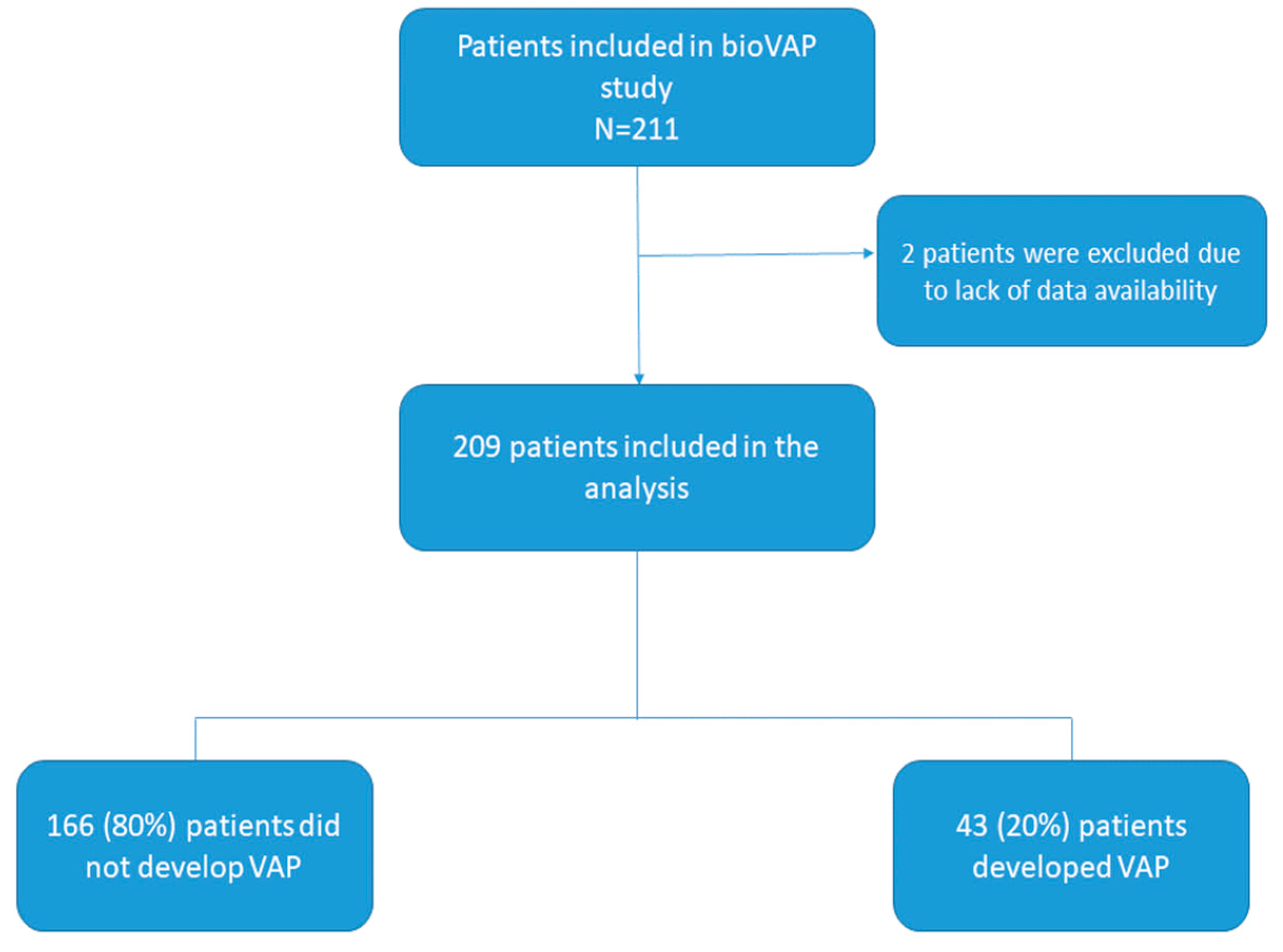
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BAL | broncho-alveolar lavage |
| CAP | community-acquired pneumonia |
| CFU | colony-forming units |
| COPD | chronic obstructive pulmonary disease |
| CRP | C-reactive protein |
| HAP | hospital-acquired pneumonia |
| HIV | human immunodeficiency virus |
| ICU | intensive care unit |
| LOS | length of stay |
| PaO2/FiO2 | ratio of arterial oxygen partial pressure to fractional inspired oxygen |
| PCT | procalcitonin |
| PSP | pancreatic stone protein |
| QTA | quantitative tracheal aspirate |
| SAPS | Simplified Acute Physiology Score |
| VAP | ventilator-associated pneumonia |
| WCC | white cell count |
References
- Vincent, J.L.; Sakr, Y.; Singer, M.; Martin-Loeches, I.; Machado, F.R.; Marshall, J.C.; Finfer, S.; Pelosi, P.; Brazzi, L.; Aditianingsih, D.; et al. Prevalence and Outcomes of Infection Among Patients in Intensive Care Units in 2017. JAMA 2020, 323, 1478–1487. [Google Scholar] [CrossRef] [PubMed]
- Torres, A.; Niederman, M.S.; Chastre, J.; Ewig, S.; Fernandez-Vandellos, P.; Hanberger, H.; Kollef, M.; Li Bassi, G.; Luna, C.M.; Martin-Loeches, I.; et al. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia: Guidelines for the management of hospital-acquired pneumonia (HAP)/ventilator-associated pneumonia (VAP) of the European Respiratory Society (ERS), European Society of Intensive Care Medicine (ESICM), European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and Asociación Latinoamericana del Tórax (ALAT). Eur. Respir. J. 2017, 50, 1700582. [Google Scholar] [PubMed]
- Fernando, S.M.; Tran, A.; Cheng, W.; Klompas, M.; Kyeremanteng, K.; Mehta, S.; English, S.W.; Muscedere, J.; Cook, D.J.; Torres, A.; et al. Diagnosis of ventilator-associated pneumonia in critically ill adult patients-a systematic review and meta-analysis. Intensive Care Med. 2020, 46, 1170–1179. [Google Scholar] [CrossRef] [PubMed]
- Álvarez-Lerma, F.; Palomar-Martínez, M.; Sánchez-García, M.; Martínez-Alonso, M.; Álvarez-Rodríguez, J.; Lorente, L.; Arias-Rivera, S.; García, R.; Gordo, F.; Añón, J.M.; et al. Prevention of Ventilator-Associated Pneumonia: The Multimodal Approach of the Spanish ICU “Pneumonia Zero” Program. Crit. Care Med. 2018, 46, 181–188. [Google Scholar] [CrossRef]
- Rouzé, A.; Martin-Loeches, I.; Povoa, P.; Makris, D.; Artigas, A.; Bouchereau, M.; Lambiotte, F.; Metzelard, M.; Cuchet, P.; Boulle Geronimi, C.; et al. Relationship between SARS-CoV-2 infection and the incidence of ventilator-associated lower respiratory tract infections: A European multicenter cohort study. Intensive Care Med. 2021, 47, 188–198. [Google Scholar] [CrossRef]
- Niederman, M.S. What COVID-19 Has Taught Us: Ventilator-associated Pneumonia Is Back! Am. J. Respir. Crit. Care Med. 2022, 206, 132–134. [Google Scholar] [CrossRef]
- Coelho, L.; Rabello, L.; Salluh, J.; Martin-Loeches, I.; Rodriguez, A.; Nseir, S.; Gomes, J.A.; Povoa, P.; TAVeM study Group. C-reactive protein and procalcitonin profile in ventilator-associated lower respiratory infections. J. Crit. Care 2018, 48, 385–389. [Google Scholar] [CrossRef]
- Póvoa, P.; Martin-Loeches, I.; Ramirez, P.; Bos, L.D.; Esperatti, M.; Silvestre, J.; Gili, G.; Goma, G.; Berlanga, E.; Espasa, M.; et al. Biomarker kinetics in the prediction of VAP diagnosis: Results from the BioVAP study. Ann. Intensive Care 2016, 6, 32. [Google Scholar] [CrossRef]
- Samanta, S.; Poddar, B.; Azim, A.; Singh, R.K.; Gurjar, M.; Baronia, A.K. Significance of Mini Bronchoalveolar Lavage Fluid Amylase Level in Ventilator-Associated Pneumonia: A Prospective Observational Study. Crit. Care Med. 2018, 46, 71–78. [Google Scholar] [CrossRef]
- Salluh, J.I.F.; Souza-Dantas, V.C.; Póvoa, P. The current status of biomarkers for the diagnosis of nosocomial pneumonias. Curr. Opin. Crit. Care 2017, 23, 391–397. [Google Scholar] [CrossRef]
- Palazzo, S.J.; Simpson, T.; Schnapp, L. Biomarkers for Ventilator-Associated Pneumonia: Review of the Literature. Heart Lung 2011, 40, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Jin, C.X.; Hayakawa, T.; Ko, S.B.H.; Ishiguro, H.; Kitagawa, M. Pancreatic stone protein/regenerating protein family in pancreatic and gastrointestinal diseases. Intern. Med. 2011, 50, 1507–1516. [Google Scholar] [CrossRef] [PubMed]
- Eggimann, P.; Que, Y.-A.; Rebeaud, F. Measurement of pancreatic stone protein in the identification and management of sepsis. Biomark Med. 2019, 13, 135–145. [Google Scholar] [CrossRef] [PubMed]
- Fidalgo, P.; Nora, D.; Coelho, L.; Povoa, P. Pancreatic Stone Protein: Review of a New Biomarker in Sepsis. J. Clin. Med. 2022, 11, 1085. [Google Scholar] [CrossRef]
- Pugin, J.; Daix, T.; Pagani, J.L.; Morri, D.; Giacomucci, A.; Dequin, P.F.; Guitton, C.; Que, Y.A.; Zani, G.; Brealey, D.; et al. Serial measurement of pancreatic stone protein for the early detection of sepsis in intensive care unit patients: A prospective multicentric study. Crit. Care 2021, 25, 151. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar] [CrossRef]
- Rizopoulos, D. Joint Modeling of Longitudinal and Time-to-Event Data with Applications in R.; CRC Press: Boca Raton, FL, USA, 2021; p. 289. [Google Scholar]
- Rizopoulos, D. Dynamic predictions and prospective accuracy in joint models for longitudinal and time-to-event data. Biometrics 2011, 67, 819–829. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria. Available online: https://www.R-project.org/ (accessed on 26 August 2022).
- Rizopoulos D. GLMMadaptive: Generalized Linear Mixed Models using Adaptive Gaussian Quadrature. v. 0.9-0. Available online: https://drizopoulos.github.io/GLMMadaptive/ (accessed on 26 July 2022).
- Rizopoulos, D.; Papageorgiou, G.; Miranda Afonso, P.D. JMbayes2: Extended Joint Models for Longitudinal and Time-to-Event Data. R package. v. 0.4-5. Available online: https://drizopoulos.github.io/JMbayes2/ (accessed on 26 July 2022).
- Wickham H.ggplot2: Elegant Graphics for Data Analysis. Springrr-Verlag New York. 2016. Available online: https://ggplot2.tidyverse.org/authors.html#citation (accessed on 26 July 2022).
- García de Guadiana-Romualdo, L.; Albaladejo-Otón, M.D.; Berger, M.; Jiménez-Santos, E.; Jiménez-Sánchez, R.; Esteban-Torrella, P.; Rebollo-Acebes, S.; Hernando-Holgado, A.; Ortín-Freire, A.; Trujillo-Santos, J. Prognostic performance of pancreatic stone protein in critically ill patients with sepsis. Biomark. Med. 2019, 13, 1469–1480. [Google Scholar] [CrossRef]
- Prazak, J.; Irincheeva, I.; Llewelyn, M.J.; Stolz, D.; García de Guadiana Romualdo, L.; Graf, R.; Reding, T.; Klein, H.J.; Eggimann, P.; Que, Y.A. Accuracy of pancreatic stone protein for the diagnosis of infection in hospitalized adults: A systematic review and individual patient level meta-analysis. Crit. Care 2021, 25, 182. [Google Scholar] [CrossRef]
- GTEx Portal. Available online: https://www.gtexportal.org/home/aboutGTEx (accessed on 31 March 2023).
- Tissue Expression of REG1B—Staining in Lung—The Human Protein Atlas. Available online: https://www.proteinatlas.org/ENSG00000172023-REG1B/tissue/lung (accessed on 31 March 2023).
- Conway Morris, A.; Rynne, J.; Shankar-Hari, M. Compartmentalisation of immune responses in critical illness: Does it matter? Intensive Care Med. 2022, 48, 1617–1620. [Google Scholar] [CrossRef]
- Conway Morris, A.; Kefala, K.; Wilkinson, T.S.; Moncayo-Nieto, O.L.; Dhaliwal, K.; Farrell, L.; Walsh, T.S.; Mackenzie, S.J.; Swann, D.G.; Andrews, P.J.; et al. Diagnostic importance of pulmonary interleukin-1beta and interleukin-8 in ventilator-associated pneumonia. Thorax 2010, 65, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Boeck, L.; Graf, R.; Eggimann, P.; Pargger, H.; Raptis, D.A.; Smyrnios, N.; Thakkar, N.; Siegemund, M.; Rakic, J.; Tamm, M.; et al. Pancreatic stone protein: A marker of organ failure and outcome in ventilator-associated pneumonia. Chest 2011, 140, 925–932. [Google Scholar] [CrossRef]
- Barichello, T.; Generoso, J.S.; Singer, M.; Dal-Pizzol, F. Biomarkers for sepsis: More than just fever and leukocytosis—A narrative review. Crit. Care 2022, 26, 14. [Google Scholar] [CrossRef] [PubMed]
- Kalil, A.C.; Metersky, M.L.; Klompas, M.; Muscedere, J.; Sweeney, D.A.; Palmer, L.B.; Napolitano, L.M.; O’Grady, N.P.; Bartlett, J.G.; Carratalà, J.; et al. Management of Adults with Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin. Infect. Dis. 2016, 63, e61–e111. [Google Scholar] [CrossRef] [PubMed]
- Ferreira-Coimbra, J.; Ardanuy, C.; Diaz, E.; Leone, M.; De Pascale, G.; Póvoa, P.; Prat-Aymerich, C.; Serrano-Garcia, R.; Solé-Violan, J.; Zaragoza, R.; et al. Ventilator-associated pneumonia diagnosis: A prioritization exercise based on multi-criteria decision analysis. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Sackett, D.L.; Haynes, R.B. The architecture of diagnostic research. BMJ 2002, 324, 539–541. [Google Scholar] [CrossRef] [PubMed]
- Rué, M.; Andrinopoulou, E.-R.; Alvares, D.; Armero, C.; Forte, A.; Blanch, L. Bayesian joint modeling of bivariate longitudinal and competing risks data: An application to study patient-ventilator asynchronies in critical care patients. Biom. J. 2017, 59, 1184–1203. [Google Scholar] [CrossRef]
- Lavalley-Morelle, A.; Timsit, J.-F.; Mentré, F.; Mullaert, J.; OUTCOMEREA Network. Joint modeling under competing risks: Application to survival prediction in patients admitted in Intensive Care Unit for sepsis with daily Sequential Organ Failure Assessment score assessments. CPT Pharmacomet. Syst. Pharmacol. 2022, 11, 1472–1484. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Overall (N = 209) | Non-VAP (N = 166) | VAP (N = 43) |
|---|---|---|---|
| Age, years | 63 (48, 74) | 64.5 (50.2, 75) | 59 (41, 66) |
| Female | 71 (34%) | 60 (36.1%) | 11 (25.6%) |
| Main cause of hospital admission | |||
| Medical | 158 (75.6%) | 127 (76.5%) | 31 (72.1%) |
| Elective surgery | 30 (14.4%) | 20 (12.0%) | 10 (23.3%) |
| Trauma | 3 (1.44%) | 3 (1.81%) | 0 (0.00%) |
| Emergency surgery | 18 (8.61%) | 16 (9.64%) | 2 (4.65%) |
| Infection at ICU admission | |||
| Non-infected | 136 (65.1%) | 101 (60.8%) | 35 (81.4%) |
| Infected | 73 (34.9%) | 65 (39.2%) | 8 (18.6%) |
| Site of infection at ICU admission | |||
| Pulmonary infection | 44 (60.3%) | 38 (22.9%) | 6 (14.0%) |
| Non-pulmonary infection | 29 (39.7%) | 27 (16.3%) | 2 (4.65%) |
| Corticosteroid | 8 (3.83%) | 6 (3.61%) | 2 (4.65%) |
| COPD | 31 (14.8%) | 21 (12.7%) | 10 (23.3%) |
| Diabetes | 31 (14.8%) | 26 (15.7%) | 5 (11.6%) |
| Immunosuppression | 14 (6.70%) | 10 (6.02%) | 4 (9.30%) |
| Heart failure | 34 (16.3%) | 30 (18.1%) | 4 (9.30%) |
| Renal failure | 19 (9.09%) | 14 (8.43%) | 5 (11.6%) |
| HIV | 5 (2.39%) | 4 (2.41%) | 1 (2.33%) |
| Cause of mechanical ventilation | |||
| Respiratory failure | 85 (40.7%) | 73 (44.0%) | 12 (27.9%) |
| Shock | 33 (15.8%) | 25 (15.1%) | 8 (18.6%) |
| Coma | 85 (40.7%) | 64 (38.6%) | 21 (48.8%) |
| Other | 6 (2.87%) | 4 (2.41%) | 2 (4.65%) |
| Apache II at ICU admission | 23 (17, 29) | 22 (17, 29.8) | 24 (19.5, 28.5) |
| SAPS II at ICU admission | 50.3 (19) | 49.4 (19.4) | 53.6 (17.0) |
| CRP, mg/dL | |||
| At admission | 5.38 (1.59, 12.8) | 6.36 (1.84, 17.1) | 4.3 (1.1, 7.1) |
| Day 2 | 12.4 (7.89, 19.9) | 13.1 (8.55, 19.9) | 9.70 (5.9, 16.3) |
| Day 5 | 10.2 (4.65, 16.5) | 9.57 (4.82, 15.7) | 13.7 (4.54, 25.9) |
| Day 7 | 9.05 (3.95, 14.4) | 9.05 (3.8, 13.7) | 12.4 (6.11, 21.8) |
| PCT, ng/mL | |||
| At admission | 0.83 (0.21, 6.88) | 0.74 (0.20, 7.58) | 1.19 (0.24, 2.44) |
| Day 2 | 0.88 (0.2, 4.84) | 0.76 (0.2, 5.05) | 1.02 (0.38, 4.49) |
| Day 5 | 0.31 (0.15, 1.75) | 0.31 (0.14, 1.63) | 0.68 (0.16, 2.67) |
| Day 7 | 0.38 (0.13, 1.21) | 0.38 (0.13, 1.25) | 0.13 (0.13, 1.09) |
| PSP, ng/mL | |||
| At admission | 132 (68, 352) | 110 (54, 372) | 161 (129, 202) |
| Day 2 | 136 (67, 296) | 134 (60, 306) | 165 (77.5, 276) |
| Day 5 | 208 (93, 370) | 195 (79.5, 331) | 291 (151, 411) |
| Day 7 | 146 (99, 428) | 145 (90.5, 396) | 184 (124, 534) |
| PaO2/FiO2 at admission | 198 (135, 311) | 192 (128, 317) | 233 (177, 287) |
| Hospital LOS, days | 26 (16, 47) | 26 (17, 46.8) | 27 (16, 48) |
| In-ICU mortality | 47 (22.5%) | 34 (20.5%) | 13 (30.2%) |
| Days before VAP | VAP Diagnosis | Days after VAP | |||||
|---|---|---|---|---|---|---|---|
| 3 | 2 | 1 | 1 | 2 | 3 | ||
| Raw values (ng/mL), mean (SD) | 309.9 (182.2) | 225.8 (179.7) | 235.2 (165) | 254.8 (165.6) | 316.5 (201.1) | 310.3 (195) | 262.3 (173.3) |
| Adjusted values by means of a mixed-effect model (ng/mL), mean (95% CI) | 291.1 (241.5, 341.8) | 298.7 (249.6, 348.5) | 304.1 (255.1, 353.5) | 307.1 (258.4, 356.0) | 307.6 (259.7, 355.6) | 305.3 (259.1, 351.9) | 300.2 (256.0, 344.9) |
| HR (95% CrI) a | ||
|---|---|---|
| Model 1 | PSP (normalized to a 0–1 range) value | 0.998 (0.87; 1.14) |
| PSP (normalized to a 0–1 range) daily change | 0.97 (0.64; 1.43) | |
| PSP (normalized to a 0–1 range) cumulative area | 1.04 (0.48; 2.27) | |
| Infected (vs. Non-infected) | 0.35 (0.11; 0.97) | |
| Model 2 | PSP (normalized to a 0–1 range) value | 1.01 (0.97; 1.06) |
| log(CRP) value | 0.999 (0.82; 1.22) | |
| log(PCT) value | 0.94 (0.82; 1.07) | |
| Infected (vs. Non-infected) | 0.36 (0.12; 0.99) | |
| Model 3 | PSP (normalized to a 0–1 range) daily change | 1.15 (0.93; 1.41) |
| log(CRP) daily change | 0.78 (0.37; 1.59) | |
| log(PCT) daily change | 0.74 (0.40; 1.37) | |
| Infected (vs. Non-infected) | 0.35 (0.11; 0.97) | |
| Model 4 | PSP (normalized to a 0–1 range) value | 1.01 (0.97; 1.05) |
| PSP (normalized to a 0–1 range) daily change | 1.15 (0.94; 1.41) | |
| log(CRP) value | 1.004 (0.83; 1.22) | |
| log(CRP) daily change | 0.76 (0.35; 1.58) | |
| log(PCT) value | 0.95 (0.82; 1.08) | |
| log(PCT) daily change | 0.77 (0.40; 1.45) | |
| Infected (vs. Non-infected) | 0.35 (0.11; 0.99) | |
| Model 5 | PSP (normalized to a 0–1 range) value | 1.07 (0.95; 1.21) |
| PSP (normalized to a 0–1 range) daily change | 0.93 (0.67; 1.28) | |
| PSP (normalized to a 0–1 range) cumulative area | 0.66 (0.29; 1.39) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ceccato, A.; Camprubí-Rimblas, M.; Bos, L.D.J.; Povoa, P.; Martin-Loeches, I.; Forné, C.; Areny-Balagueró, A.; Campaña-Duel, E.; Morales-Quinteros, L.; Quero, S.; et al. Evaluation of the Kinetics of Pancreatic Stone Protein as a Predictor of Ventilator-Associated Pneumonia. Biomedicines 2023, 11, 2676. https://doi.org/10.3390/biomedicines11102676
Ceccato A, Camprubí-Rimblas M, Bos LDJ, Povoa P, Martin-Loeches I, Forné C, Areny-Balagueró A, Campaña-Duel E, Morales-Quinteros L, Quero S, et al. Evaluation of the Kinetics of Pancreatic Stone Protein as a Predictor of Ventilator-Associated Pneumonia. Biomedicines. 2023; 11(10):2676. https://doi.org/10.3390/biomedicines11102676
Chicago/Turabian StyleCeccato, Adrian, Marta Camprubí-Rimblas, Lieuwe D. J. Bos, Pedro Povoa, Ignacio Martin-Loeches, Carles Forné, Aina Areny-Balagueró, Elena Campaña-Duel, Luis Morales-Quinteros, Sara Quero, and et al. 2023. "Evaluation of the Kinetics of Pancreatic Stone Protein as a Predictor of Ventilator-Associated Pneumonia" Biomedicines 11, no. 10: 2676. https://doi.org/10.3390/biomedicines11102676
APA StyleCeccato, A., Camprubí-Rimblas, M., Bos, L. D. J., Povoa, P., Martin-Loeches, I., Forné, C., Areny-Balagueró, A., Campaña-Duel, E., Morales-Quinteros, L., Quero, S., Ramirez, P., Esperatti, M., Torres, A., Blanch, L., & Artigas, A. (2023). Evaluation of the Kinetics of Pancreatic Stone Protein as a Predictor of Ventilator-Associated Pneumonia. Biomedicines, 11(10), 2676. https://doi.org/10.3390/biomedicines11102676