
Developing a COVID-19 Mortality Prediction (CoMPred) Indicator for ICU Diabetic Patients Treated with Tocilizumab in Saudi Arabia: A Proof-of-Concept Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. The Development of the COVID-19 Mortality Prediction (CoMPred) Scoring
2.3. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
3.2. The Biological Changes in COVID-19 Patients Admitted to the ICU
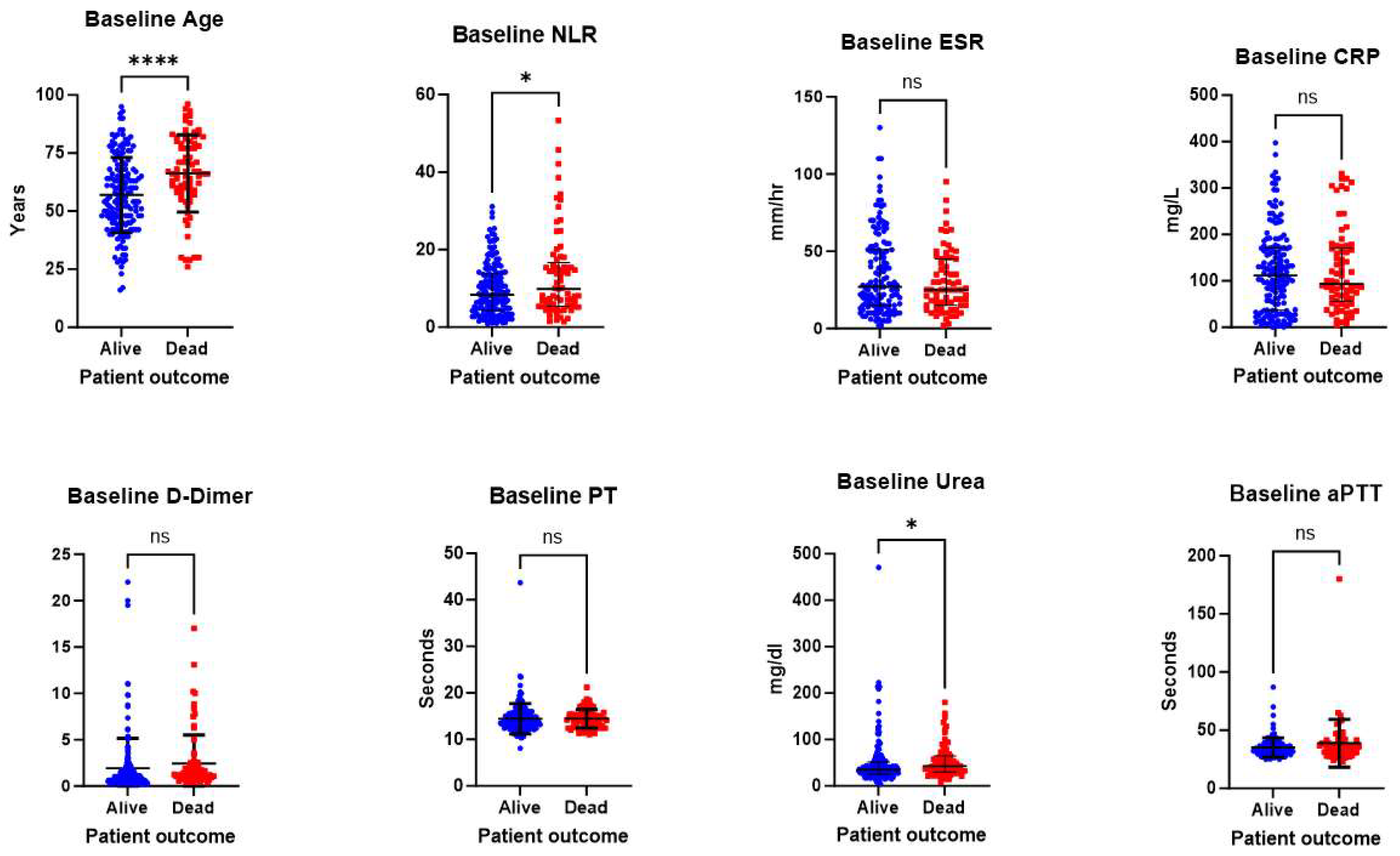
3.3. Identifying the Elements Needed for the Development of the CoMPred Indicator
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nussbaumer-Streit, B.; Mayr, V.; Dobrescu, A.I.; Chapman, A.; Persad, E.; Klerings, I.; Wagner, G.; Siebert, U.; Ledinger, D.; Zachariah, C.; et al. Quarantine alone or in combination with other public health measures to control COVID-19: A rapid review. Cochrane Database Syst. Rev. 2020, 9, CD013574. [Google Scholar] [CrossRef] [PubMed]
- Qian, M.; Jiang, J. COVID-19 and social distancing. J. Public Health 2020, 30, 259–261. [Google Scholar] [CrossRef] [PubMed]
- Sayed, A.A. The Progressive Public Measures of Saudi Arabia to Tackle COVID-19 and Limit Its Spread. Int. J. Environ. Res. Public Health 2021, 18, 783. [Google Scholar] [CrossRef]
- John Hopkins University & Medicine (JHI). Mortality Analysis. Available online: https://coronavirus.jhu.edu/data/mortality (accessed on 28 May 2023).
- Khatrawi, E.M.; Sayed, A.A. Assessing the Dynamics of COVID-19 Morbidity and Mortality in Response to Mass Vaccination: A Comparative Study Between Saudi Arabia and the United Kingdom. Cureus 2022, 14, e33042. [Google Scholar] [CrossRef] [PubMed]
- Majumder, J.; Minko, T. Recent Developments on Therapeutic and Diagnostic Approaches for COVID-19. AAPS J. 2021, 23, 14. [Google Scholar] [CrossRef]
- Safadi, M.A.P.; da Silva, C.A.A. The challenging and unpredictable spectrum of COVID-19 in children and adolescents. Rev. Paul. Pediatr. 2021, 39, e2020192. [Google Scholar] [CrossRef] [PubMed]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19). JAMA 2020, 324, 782. [Google Scholar] [CrossRef]
- Jacobi, A.; Chung, M.; Bernheim, A.; Eber, C. Portable chest X-ray in coronavirus disease-19 (COVID-19): A pictorial review. Clin. Imaging 2020, 64, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Ye, Z.; Zhang, Y.; Wang, Y.; Huang, Z.; Song, B. Chest CT manifestations of new coronavirus disease 2019 (COVID-19): A pictorial review. Eur. Radiol. 2020, 30, 4381–4389. [Google Scholar] [CrossRef]
- Sayed, A.A.; Allam, A.A.; Sayed, A.I.; Alraey, M.A.; Joseph, M.V. The use of neutrophil-to-lymphocyte ratio (NLR) as a marker for COVID-19 infection in Saudi Arabia. Saudi Med. J. 2021, 42, 370–376. [Google Scholar] [CrossRef]
- Wang, Y.; Zhao, J.; Yang, L.; Hu, J.; Yao, Y. Value of the Neutrophil-Lymphocyte Ratio in Predicting COVID-19 Severity: A Meta-analysis. Dis. Markers 2021, 2021, 2571912. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.S.; Rout, A. Use of Neutrophil-to-Lymphocyte and Platelet-to-Lymphocyte Ratios in COVID-19. J. Clin. Med. Res. 2020, 12, 448–453. [Google Scholar] [CrossRef] [PubMed]
- Ponti, G.; Maccaferri, M.; Ruini, C.; Tomasi, A.; Ozben, T. Biomarkers associated with COVID-19 disease progression. Crit. Rev. Clin. Lab. Sci. 2020, 57, 389–399. [Google Scholar] [CrossRef] [PubMed]
- Saudi Ministry of Health (MoH). Protocol for Patients Suspected of/Confirmed with COVID-19. Available online: https://www.moh.gov.sa/Ministry/MediaCenter/Publications/Documents/MOH-therapeutic-protocol-for-COVID-19.pdf (accessed on 5 August 2022).
- Armstrong, R.A.; Kane, A.D.; Kursumovic, E.; Oglesby, F.C.; Cook, T.M. Mortality in patients admitted to intensive care with COVID-19: An updated systematic review and meta-analysis of observational studies. Anaesthesia 2021, 76, 537–548. [Google Scholar] [CrossRef]
- Conti, V.; Corbi, G.; Sellitto, C.; Sabbatino, F.; Maci, C.; Bertini, N.; De Bellis, E.; Iuliano, A.; Davinelli, S.; Pagliano, P.; et al. Effect of Tocilizumab in Reducing the Mortality Rate in COVID-19 Patients: A Systematic Review with Meta-Analysis. J. Pers. Med. 2021, 11, 628. [Google Scholar] [CrossRef]
- Weiskopf, D.; Weinberger, B.; Grubeck-Loebenstein, B. The aging of the immune system. Transpl. Int. 2009, 22, 1041–1050. [Google Scholar] [CrossRef]
- Chen, Y.; Klein, S.L.; Garibaldi, B.T.; Li, H.; Wu, C.; Osevala, N.M.; Li, T.; Margolick, J.B.; Pawelec, G.; Leng, S.X. Aging in COVID-19: Vulnerability, immunity and intervention. Ageing Res. Rev. 2021, 65, 101205. [Google Scholar] [CrossRef]
- Alhoufie, S.T.; Mumena, W.A.; Alsharif, N.; Makhdoom, H.M.; Almutawif, Y.A.; Alfarouk, K.O.; Alharbi, M.Z.; Aljabri, K.; Aljifri, A. Epidemiological Characteristics and Outcomes Predictors for Intensive Care Unit COVID-19 Patients in Al-Madinah, Saudi Arabia. Retrospective Cohort Study. Infect. Drug Resist. 2023, 16, 5573–5586. [Google Scholar] [CrossRef]
- Mobarki, A.A.; Dobie, G.; Saboor, M.; Madkhali, A.M.; Akhter, M.S.; Hakamy, A.; Humran, A.; Hamali, Y.; Jackson, D.E.; Hamali, H.A. MPR and NLR as Prognostic Markers in ICU-Admitted Patients with COVID-19 in Jazan, Saudi Arabia. Infect. Drug Resist. 2021, 14, 4859–4864. [Google Scholar] [CrossRef]
- Wei, Y.-Y.; Wang, R.-R.; Zhang, D.-W.; Chen, S.-H.; Tan, Y.-Y.; Zhang, W.-T.; Han, M.-F.; Fei, G.-H. Differential Characteristics of Patients for Hospitalized Severe COVID-19 Infected by the Omicron Variants and Wild Type of SARS-CoV-2 in China. J. Inflamm. Res. 2023, 16, 3063–3078. [Google Scholar] [CrossRef]
- Regolo, M.; Vaccaro, M.; Sorce, A.; Stancanelli, B.; Colaci, M.; Natoli, G.; Russo, M.; Alessandria, I.; Motta, M.; Santangelo, N.; et al. Neutrophil-to-Lymphocyte Ratio (NLR) Is a Promising Predictor of Mortality and Admission to Intensive Care Unit of COVID-19 Patients. J. Clin. Med. 2022, 11, 2235. [Google Scholar] [CrossRef]
- Regolo, M.; Sorce, A.; Vaccaro, M.; Colaci, M.; Stancanelli, B.; Natoli, G.; Motta, M.; Isaia, I.; Castelletti, F.; Giangreco, F.; et al. Assessing Humoral Immuno-Inflammatory Pathways Associated with Respiratory Failure in COVID-19 Patients. J. Clin. Med. 2023, 12, 4057. [Google Scholar] [CrossRef] [PubMed]
- Buonacera, A.; Stancanelli, B.; Colaci, M.; Malatino, L. Neutrophil to Lymphocyte Ratio: An Emerging Marker of the Relationships between the Immune System and Diseases. Int. J. Mol. Sci. 2022, 23, 3636. [Google Scholar] [CrossRef] [PubMed]
- Sayed, A.A. The Cost-Effectiveness of Requesting a Complete Blood Count (CBC) in the Management of COVID-19 in Saudi Arabia. Healthcare 2022, 10, 1780. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Yin, L.; Patel, J.; Tang, L.; Huang, Y. The inflammatory markers of multisystem inflammatory syndrome in children (MIS-C) and adolescents associated with COVID-19: A meta-analysis. J. Med. Virol. 2021, 93, 4358–4369. [Google Scholar] [CrossRef]
- Zeng, F.; Huang, Y.; Guo, Y.; Yin, M.; Chen, X.; Xiao, L.; Deng, G. Association of inflammatory markers with the severity of COVID-19: A meta-analysis. Int. J. Infect. Dis. 2020, 96, 467–474. [Google Scholar] [CrossRef]
- Ibnouf, A.A.O.; Khalil, M.H.; Khalid, R.; Elshibli, E.M.; Elsayed, O.; Fadl-Elmula, I. Blood markers (lymphocyte percentages, neutrophils, CRP and ESR) can help in prioritizing rRT-PCR test for suspected COVID-19 patients in countries with limited health resources. Pan Afr. Med. J. 2020, 37, 331. [Google Scholar] [CrossRef]
- Abo-Haded, H.M.; Alshengeti, A.M.; Alawfi, A.D.; Khoshhal, S.Q.; Al-Harbi, K.M.; Allugmani, M.D.; El-Agamy, D.S. Cytokine Profiling among Children with Multisystem Inflammatory Syndrome versus Simple COVID-19 Infection: A Study from Northwest Saudi Arabia. Biology 2022, 11, 946. [Google Scholar] [CrossRef]
- Mohamadi Yarijani, Z.; Najafi, H. Kidney injury in COVID-19 patients, drug development and their renal complications: Review study. Biomed. Pharmacother. 2021, 142, 111966. [Google Scholar] [CrossRef]
- Rohini, K.; Surekha Bhat, M.; Srikumar, P.S.; Mahesh Kumar, A. Assessment of Hematological Parameters in Pulmonary Tuberculosis Patients. Indian J. Clin. Biochem. 2016, 31, 332–335. [Google Scholar] [CrossRef]
- Al-Samkari, H.; Karp Leaf, R.S.; Dzik, W.H.; Carlson, J.C.T.; Fogerty, A.E.; Waheed, A.; Goodarzi, K.; Bendapudi, P.K.; Bornikova, L.; Gupta, S.; et al. COVID-19 and coagulation: Bleeding and thrombotic manifestations of SARS-CoV-2 infection. Blood 2020, 136, 489–500. [Google Scholar] [CrossRef]
- Thachil, J.; Tang, N.; Gando, S.; Falanga, A.; Cattaneo, M.; Levi, M.; Clark, C.; Iba, T. ISTH interim guidance on recognition and management of coagulopathy in COVID-19. J. Thromb. Haemost. 2020, 18, 1023–1026. [Google Scholar] [CrossRef]
- Tang, N.; Li, D.; Wang, X.; Sun, Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 844–847. [Google Scholar] [CrossRef]
- Singh, A.K.; Gupta, R.; Ghosh, A.; Misra, A. Diabetes in COVID-19: Prevalence, pathophysiology, prognosis and practical considerations. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Guo, W.; Li, M.; Dong, Y.; Zhou, H.; Zhang, Z.; Tian, C.; Qin, R.; Wang, H.; Shen, Y.; Du, K.; et al. Diabetes is a risk factor for the progression and prognosis of COVID-19. Diabetes Metab. Res. Rev. 2020, 36, e3319. [Google Scholar] [CrossRef] [PubMed]
- Toor, S.M.; Saleh, R.; Sasidharan Nair, V.; Taha, R.Z.; Elkord, E. T-cell responses and therapies against SARS-CoV-2 infection. Immunology 2021, 162, 30–43. [Google Scholar] [CrossRef] [PubMed]
- Nassar, M.; Daoud, A.; Nso, N.; Medina, L.; Ghernautan, V.; Bhangoo, H.; Nyein, A.; Mohamed, M.; Alqassieh, A.; Soliman, K.; et al. Diabetes Mellitus and COVID-19: Review Article. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 102268. [Google Scholar] [CrossRef] [PubMed]
- Hadj Hassine, I. COVID-19 vaccines and variants of concern: A review. Rev. Med. Virol. 2022, 32, e2313. [Google Scholar] [CrossRef]
- Kemp, S.A.; Collier, D.A.; Datir, R.P.; Ferreira, I.A.T.M.; Gayed, S.; Jahun, A.; Hosmillo, M.; Rees-Spear, C.; Mlcochova, P.; Lumb, I.U.; et al. SARS-CoV-2 evolution during treatment of chronic infection. Nature 2021, 592, 277–282. [Google Scholar] [CrossRef]
- Yang, Z.; Zhang, S.; Tang, Y.-P.; Zhang, S.; Xu, D.-Q.; Yue, S.-J.; Liu, Q.-L. Clinical Characteristics, Transmissibility, Pathogenicity, Susceptible Populations, and Re-infectivity of Prominent COVID-19 Variants. Aging Dis. 2022, 13, 402. [Google Scholar] [CrossRef]
- Liu, C.; Lu, J.; Li, P.; Feng, S.; Guo, Y.; Li, K.; Zhao, B.; Su, Y.; Chen, T.; Zou, X. A comparative study on epidemiological characteristics, transmissibility, and pathogenicity of three COVID-19 outbreaks caused by different variants. Int. J. Infect. Dis. 2023, 134, 78–87. [Google Scholar] [CrossRef] [PubMed]
- Jarjour, N.N.; Masopust, D.; Jameson, S.C. T Cell Memory: Understanding COVID-19. Immunity 2021, 54, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; John Wherry, E. T cell responses in patients with COVID-19. Nat. Rev. Immunol. 2020, 20, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Sosa-Hernández, V.A.; Torres-Ruíz, J.; Cervantes-Díaz, R.; Romero-Ramírez, S.; Páez-Franco, J.C.; Meza-Sánchez, D.E.; Juárez-Vega, G.; Pérez-Fragoso, A.; Ortiz-Navarrete, V.; Ponce-de-León, A.; et al. B Cell Subsets as Severity-Associated Signatures in COVID-19 Patients. Front. Immunol. 2020, 11, 611004. [Google Scholar] [CrossRef]
- Quast, I.; Tarlinton, D. B cell memory: Understanding COVID-19. Immunity 2021, 54, 205–210. [Google Scholar] [CrossRef]
- Fricke-Galindo, I.; Falfán-Valencia, R. Genetics Insight for COVID-19 Susceptibility and Severity: A Review. Front. Immunol. 2021, 12, 622176. [Google Scholar] [CrossRef]
- Chlamydas, S.; Papavassiliou, A.G.; Piperi, C. Epigenetic mechanisms regulating COVID-19 infection. Epigenetics 2021, 16, 263–270. [Google Scholar] [CrossRef]
- Setia, M. Methodology series module 3: Cross-sectional studies. Indian J. Dermatol. 2016, 61, 261. [Google Scholar] [CrossRef]
- Lambden, S.; Laterre, P.F.; Levy, M.M.; Francois, B. The SOFA score—Development, utility and challenges of accurate assessment in clinical trials. Crit. Care 2019, 23, 374. [Google Scholar] [CrossRef]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Element (Unit) | Cut-off Level | Assigned Score |
|---|---|---|
| Patient’s age (years) | <50 | 0 |
| 50–64 | 1 | |
| ≥65 | 2 | |
| D-Dimer (mg/L) | <0.5 | 0 |
| ≥0.5 | 1 | |
| PT (seconds) | <13.5 | 0 |
| ≥13.5 | 1 | |
| aPTT (seconds) | <35 | 0 |
| ≥35 | 1 | |
| NLR | <4 | 0 |
| ≥4 < 8 | 1 | |
| ≥8 | 2 | |
| ESR (mm/hr) | <30 | 0 |
| ≥30 | 1 | |
| CRP (mg/L) | <10 | 0 |
| ≥10 | 1 | |
| Urea (mg/dL) | <35 | 0 |
| ≥35 | 1 |
| Characteristics (Unit) | Values |
|---|---|
| Age (years) | 59.87 (±16.88) ^ |
| Gender | Male: 175 |
| Female: 74 | |
| Nationality | Saudi: 153 (61.45%) |
| Non-Saudi: 96 (38.55%) | |
| ICU admission Outcome | Alive: 169 (67.87%) |
| Dead: 80 (32.13%) | |
| Use of Tocilizumab | Yes: 235 (94.37%) |
| No: 14 (5.63%) | |
| Diabetic | Yes: 168 (67.47%) |
| No: 81 (32.53%) | |
| Duration of stay (days) | 17 (11–23.75) ^^ |
| Characteristics | Baseline | Follow-up | p Value |
|---|---|---|---|
| WBC (×103/mL) | 8.44 (5.8–12.01) | 10.32 (7.32–14.83) | <0.0001 **** |
| RBC count | 4.86 (4.38–5.26) | 4.74 (4.14–5.34) | 0.2 |
| Hemoglobin | 13.32 (11.96–14.6) | 13.07 (11.42) | 0.25 |
| Hematocrit | 41 (37.05–44.25) | 39.80 (34.60–43.35) | 0.2 |
| MCV | 85.40 (81–88.95) | 84.90 (81.20–88.95) | 0.65 |
| MCH | 28 (26.10–29.60) | 27.90 (26.10–29.50) | 0.95 |
| MCHC | 32.80 (31.65–33.90) | 32.90 (31.75–34) | 0.94 |
| RDW | 13.20 (12.30–14.38) | 13.60 (12.60–14.50) | 0.0002 *** |
| Platelet count | 236 (178–314.2) | 292.1 (188–387.4) | <0.0001 **** |
| Mean platelet volume | 8.6 (7.18–9.6) | 8.6 (7.35–9.5) | 0.92 |
| Neutrophil count | 7.62 (4.42–11) | 8.57 (5.74–12.80) | 0.0006 *** |
| Lymphocyte count | 0.77 (0.56–1.22) | 0.76 (0.54–1.3) | 0.65 |
| NLR | 8.86 (4.89–15.37) | 11.87 (5.85–19.28) | 0.0077 ** |
| Monocyte count | 0.35 (0.23–0.55) | 0.48 (0.29–0.72) | <0.0001 **** |
| Eosinophil count | 0.03 (0–0.06) | 0.04 (0.01–0.08) | 0.0003 *** |
| Basophil count | 0.04 (0.02–0.06) | 0.04 (0.02–0.07) | 0.004 ** |
| ESR | 26 (14–49) | 20 (11–39) | <0.0001 **** |
| CRP | 103 (49.81–170.6) | 8.02 (3.39–33.83) | <0.0001 **** |
| Urea | 36.38 (27.82–54.63) | 55.64 (38.52–96.30) | <0.0001 **** |
| Creatinine | 0.9 (0.77–1.26) | 0.85 (0.73–1.3) | 0.0039 ** |
| ALT | 35 (23–53) | 54 (34–91.50) | <0.0001 **** |
| AST | 43 (29–64.50) | 42 (28–69.50) | 0.65 |
| D-Dimer | 1.025 (0.61–1.78) | 1.55 (0.9–4) | <0.0001 **** |
| PT | 14 (12.75–15.5) | 13.8 (12.3–15.65) | 0.92 |
| aPTT | 35.1 (30.03–40.88) | 31.15 (27.18–38.83) | 0.0055 ** |
| INR | 1.13 (1.04–1.24) | 1.12 (1.04–1.25) | 0.56 |
| Characteristics (Unit) | Survivors (n = 169) | Non-Survivors (n = 80) | p Value |
|---|---|---|---|
| Gender | Male: 124 | Male: 54 | 0.37 |
| Female: 45 | Female: 26 | ||
| Nationality | Saudi: 103 | Saudi: 48 | 0.89 |
| Non-Saudi: 66 | Non-Saudi: 32 | ||
| Diabetic | Yes: 108 | Yes: 61 | 0.08 |
| No: 58 | No: 19 | ||
| Use of Tocilizumab | Yes: 157 | Yes: 74 | 0.99 |
| No: 12 | No: 6 | ||
| WBC (×103/mL) | 8.70 (5.42–12.10) | 8.33 (5.97–11.75) | 0.82 |
| RBC count | 4.87 (4.38–5.31) | 4.7 (4.25–5.10) | 0.16 |
| Hemoglobin | 13.60 (11.95–14.60) | 12.90 (11.85–14.46) | 0.15 |
| Hematocrit | 41.30 (37.03–44.50) | 40.40 (36.95–43.55) | 0.36 |
| MCV | 85.05 (81.03–88.50) | 86.40 (80.95–89.75) | 0.13 |
| MCH | 27.95 (26.30–29.40) | 28 (25.75–29.90) | 0.84 |
| MCHC | 32.90 (31.80–33.90) | 32.50 (31.30–33.90) | 0.19 |
| RDW | 13.10 (12.20–14) | 13.70 (12.75–15) | 0.003 * |
| Platelet count | 247.70 (188.50–331.90) | 217.60 (148–227.50) | 0.009 * |
| Mean Platelet volume | 8.50 (7.14–9.40) | 8.90 (7.42–9.70) | 0.11 |
| Neutrophil count | 7.41 (4.08–10.50) | 6.94 (5.09–10.58) | 0.83 |
| Lymphocyte count | 0.83 (0.59–1.28) | 0.71 (0.45–1.14) | 0.01 * |
| Monocyte count | 0.40 (0.24–0.60) | 0.30 (0.18–0.46) | 0.002 * |
| Eosinophil count | 0.03 (0.00–0.07) | 0.02 (0.00–0.06) | 0.22 |
| Basophil count | 0.04 (0.02–0.06) | 0.03 (0.02–0.04) | 0.63 |
| Creatinine | 0.86 (0.76–1.22) | 1.03 (0.82–1.4) | 0.03 * |
| ALT | 34 (20.50–53) | 38 (24–56) | 0.39 |
| AST | 40 (27.50–56.50) | 53 (36–79) | 0.0008 * |
| INR | 1.12 (1.04–1.23) | 1.15 (1.06–1.27) | 0.49 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sayed, A.A.; Al Nozha, O.M. Developing a COVID-19 Mortality Prediction (CoMPred) Indicator for ICU Diabetic Patients Treated with Tocilizumab in Saudi Arabia: A Proof-of-Concept Study. Biomedicines 2023, 11, 2649. https://doi.org/10.3390/biomedicines11102649
Sayed AA, Al Nozha OM. Developing a COVID-19 Mortality Prediction (CoMPred) Indicator for ICU Diabetic Patients Treated with Tocilizumab in Saudi Arabia: A Proof-of-Concept Study. Biomedicines. 2023; 11(10):2649. https://doi.org/10.3390/biomedicines11102649
Chicago/Turabian StyleSayed, Anwar A., and Omar M. Al Nozha. 2023. "Developing a COVID-19 Mortality Prediction (CoMPred) Indicator for ICU Diabetic Patients Treated with Tocilizumab in Saudi Arabia: A Proof-of-Concept Study" Biomedicines 11, no. 10: 2649. https://doi.org/10.3390/biomedicines11102649
APA StyleSayed, A. A., & Al Nozha, O. M. (2023). Developing a COVID-19 Mortality Prediction (CoMPred) Indicator for ICU Diabetic Patients Treated with Tocilizumab in Saudi Arabia: A Proof-of-Concept Study. Biomedicines, 11(10), 2649. https://doi.org/10.3390/biomedicines11102649