

The Vastus Lateralis Muscle Interstitium Proteome Changes after an Acute Nociception in Patients with Fibromyalgia Compared to Healthy Subjects—A Microdialysis Study
 , ,
, ,  , , and
, , and
Abstract
1. Introduction
2. Material and Methods
2.1. Recruitment Process and Participants
2.2. Ethics
2.3. Background Data and Patient-Reported Outcome Measures
2.4. Resistance Exercise Program
2.5. Microdialysis Procedure
2.6. Protein Extraction and Digestion
2.7. Proteomic Analysis
2.8. Statistics
2.9. Bioinformatics
3. Results
3.1. Background Data
3.2. Patient-Reported Outcome Measures and Muscle Functional Measures
3.3. Protein Patterns Differentiating FM and CON
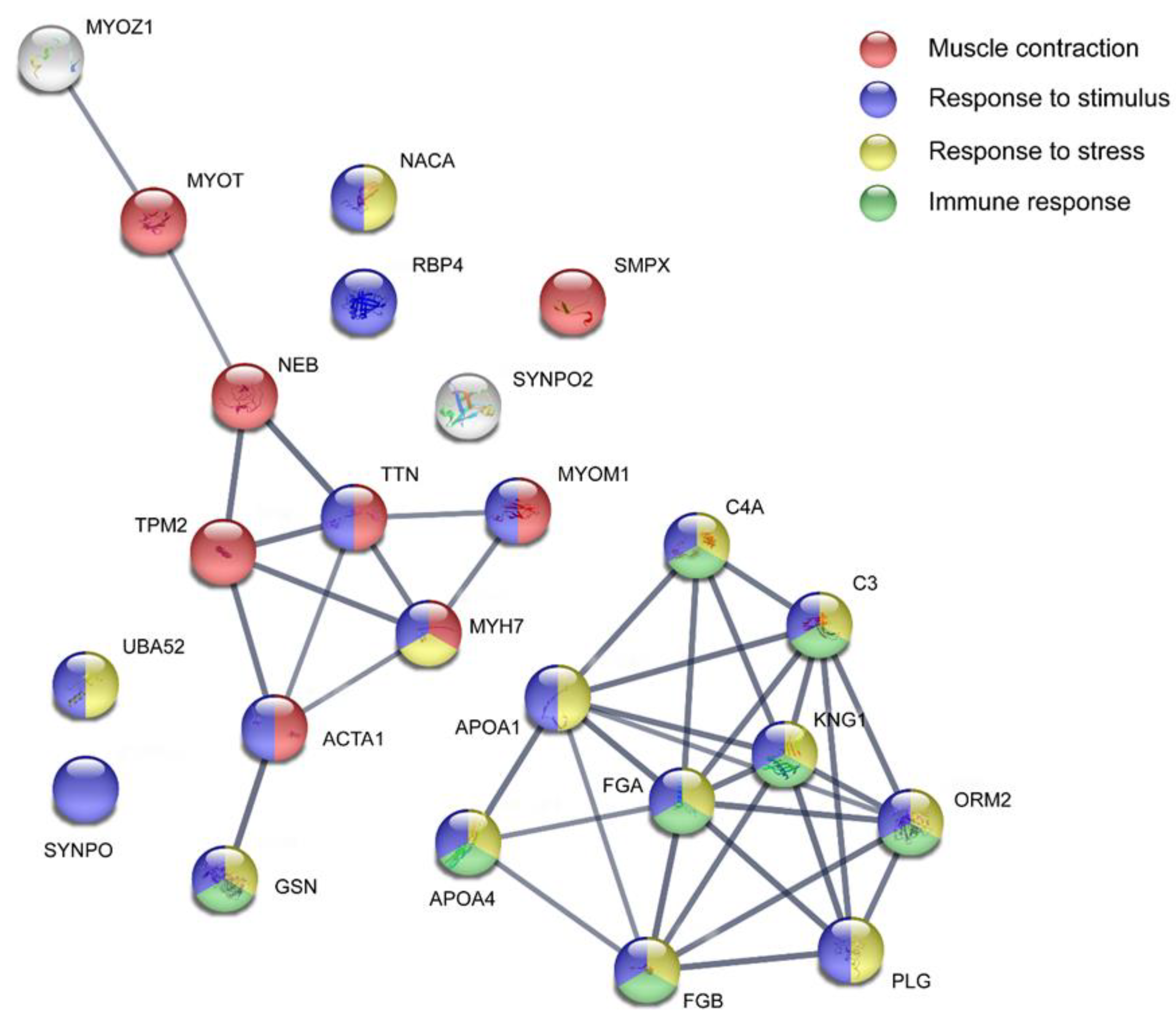
3.4. Pathway Analysis of Proteins at Baseline
3.5. Normalization of Protein Expression Levels between Groups
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gatchel, R.J.; Peng, Y.B.; Peters, M.L.; Fuchs, P.N.; Turk, D.C. The biopsychosocial approach to chronic pain: Scientific advances and future directions. Psychol. Bull 2007, 133, 581–624. [Google Scholar] [CrossRef]
- Perez de Heredia-Torres, M.; Huertas-Hoyas, E.; Máximo-Bocanegra, N.; Palacios-Ceña, D.; Fernández-De-Las-Peñas, C. Cognitive performance in women with fibromyalgia: A case-control study. Aust. Occup. Ther. J. 2016, 63, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Siracusa, R.; Paola, R.D.; Cuzzocrea, S.; Impellizzeri, D. Fibromyalgia: Pathogenesis, Mechanisms, Diagnosis and Treatment Options Update. Int. J. Mol. Sci. 2021, 22, 3891. [Google Scholar] [CrossRef]
- Terol Cantero, M.C.; Buunk, A.P.; Cabrera, V.; Bernabé, M.; Martin-Aragón Gelabert, M. Profiles of Women with Fibromyalgia and Social Comparison Processes. Front. Psychol. 2020, 11, 440. [Google Scholar] [CrossRef] [PubMed]
- Cetingok, S.; Seker, O.; Cetingok, H. The relationship between fibromyalgia and depression, anxiety, anxiety sensitivity, fear avoidance beliefs, and quality of life in female patients. Medicine 2022, 101, 39. [Google Scholar] [CrossRef]
- Clauw, D.J. Fibromyalgia: A clinical review. JAMA 2014, 311, 1547–1555. [Google Scholar] [CrossRef]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Häuser, W.; Katz, R.L.; Mease, P.J.; Russell, A.S.; Russell, I.J.; Walitt, B. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin. Arthritis. Rheum. 2016, 46, 319–329. [Google Scholar] [CrossRef]
- Marques, A.P.; Santo, A.S.D.E.; Berssaneti, A.A.; Matsutani, L.A.; Yuan, S.L.K. Prevalence of fibromyalgia: Literature review update. Rev. Bras. De Reumatol. (Engl. Ed.) 2017, 57, 356–363. [Google Scholar] [CrossRef]
- Macfarlane, G.J.; Kronisch, C.; Dean, L.E.; Atzeni, F.; Häuser, W.; Fluß, E.; Choy, E.; Kosek, E.; Amris, K.; Branco, J.; et al. EULAR revised recommendations for the management of fibromyalgia. Ann. Rheum. Dis. 2017, 76, 318–328. [Google Scholar] [CrossRef]
- Busch, A.J.; Webber, S.C.; Richards, R.S.; Bidonde, J.; Schachter, C.L.; Schafer, L.A.; Danyliw, A.; Sawant, A.; Dal Bello-Haas, V.; Rader, T.; et al. Resistance exercise training for fibromyalgia. Cochrane Database Syst. Rev. 2013, 2013, CD010884. [Google Scholar] [CrossRef] [PubMed]
- Assumpção, A.; Matsutani, L.A.; Yuan, S.L.; Santo, A.S.; Sauer, J.; Mango, P.; Marques, A.P. Muscle stretching exercises and resistance training in fibromyalgia: Which is better? A three-arm randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2018, 54, 663–670. [Google Scholar] [CrossRef] [PubMed]
- Ericsson, A.; Palstam, A.; Larsson, A.; Löfgren, M.; Bileviciute-Ljungar, I.; Bjersing, J.; Gerdle, B.; Kosek, E.; Mannerkorpi, K. Resistance exercise improves physical fatigue in women with fibromyalgia: A randomized controlled trial. Arthritis Res. Ther. 2016, 18, 176. [Google Scholar] [CrossRef]
- Hooten, M.W.; Qu, W.; Townsend, C.O.; Judd, J.W. Effects of strength vs aerobic exercise on pain severity in adults with fibromyalgia: A randomized equivalence trial. Pain 2012, 153, 915–923. [Google Scholar] [CrossRef] [PubMed]
- Gerdle, B.; Larsson, B.; Forsberg, F.; Ghafouri, N.; Karlsson, L.; Stensson, N.; Ghafouri, B. Chronic widespread pain: Increased glutamate and lactate concentrations in the trapezius muscle and plasma. Clin. J. Pain 2014, 30, 409–420. [Google Scholar] [CrossRef] [PubMed]
- Gerdle, B.; Söderberg, K.; Salvador Puigvert, L.; Rosendal, L.; Larsson, B. Increased interstitial concentrations of pyruvate and lactate in the trapezius muscle of patients with fibromyalgia: A microdialysis study. J. Rehabil. Med. 2010, 42, 679–687. [Google Scholar] [CrossRef]
- Gerdle, B.; Ghafouri, B.; Lund, E.; Bengtsson, A.; Lundberg, P.; Ettinger-Veenstra, H.V.; Leinhard, O.D.; Forsgren, M.F. Evidence of Mitochondrial Dysfunction in Fibromyalgia: Deviating Muscle Energy Metabolism Detected Using Microdialysis and Magnetic Resonance. J. Clin. Med. 2020, 9, 3527. [Google Scholar] [CrossRef]
- Sorensen, L.B.; Gazerani, P.; Wåhlén, K.; Ghafouri, N.; Gerdle, B.; Ghafouri, B. Investigation of biomarkers alterations after an acute tissue trauma in human trapezius muscle, using microdialysis. Sci. Rep. 2018, 8, 3034. [Google Scholar] [CrossRef] [PubMed]
- Kadetoff, D.; Lampa, J.; Westman, M.; Andersson, M.; Kosek, E. Evidence of central inflammation in fibromyalgia-increased cerebrospinal fluid interleukin-8 levels. J. Neuroimmunol. 2012, 242, 33–38. [Google Scholar] [CrossRef]
- O’Mahony, L.F.; Srivastava, A.; Mehta, P.; Ciurtin, C. Is fibromyalgia associated with a unique cytokine profile? A systematic review and meta-analysis. Rheumatology 2021, 60, 2602–2614. [Google Scholar] [CrossRef]
- Bjersing, J.L.; Dehlin, M.; Erlandsson, M.; Bokarewa, M.I.; Mannerkorpi, K. Changes in pain and insulin-like growth factor 1 in fibromyalgia during exercise: The involvement of cerebrospinal inflammatory factors and neuropeptides. Arthritis Res. Ther. 2012, 14, R162. [Google Scholar] [CrossRef]
- Jablochkova, A.; Bäckryd, E.; Kosek, E.; Mannerkorpi, K.; Ernberg, M.; Gerdle, B.; Ghafouri, B. Unaltered low nerve growth factor and high brain-derived neurotrophic factor levels in plasma from patients with fibromyalgia after a 15-week progressive resistance exercise. J. Rehabil. Med. 2019, 51, 779–787. [Google Scholar] [CrossRef]
- D’Amico, R.; Fusco, R.; Siracusa, R.; Impellizzeri, D.; Peritore, A.F.; Gugliandolo, E.; Interdonato, L.; Sforza, A.M.; Crupi, R.; Cuzzocrea, S.; et al. Inhibition of P2X7 Purinergic Receptor Ameliorates Fibromyalgia Syndrome by Suppressing NLRP3 Pathway. Int. J. Mol. Sci. 2021, 22, 6471. [Google Scholar] [CrossRef]
- Shippenberg, T.S.; Thompson, A.C. Overview of microdialysis. Curr. Protoc. Neurosci. 1997, 7.1.1–7.1.22. [Google Scholar] [CrossRef]
- Ernberg, M.; Hedenberg-Magnusson, B.; Alstergren, P.; Kopp, S. The level of serotonin in the superficial masseter muscle in relation to local pain and allodynia. Life Sci. 1999, 65, 313–325. [Google Scholar] [CrossRef] [PubMed]
- Turkina, M.V.; Ghafouri, N.; Gerdle, B.; Ghafouri, B. Evaluation of dynamic changes in interstitial fluid proteome following microdialysis probe insertion trauma in trapezius muscle of healthy women. Sci. Rep. 2017, 7, 43512. [Google Scholar] [CrossRef]
- Olausson, P.; Gerdle, B.; Ghafouri, N.; Sjöström, D.; Blixt, E.; Ghafouri, B. Protein alterations in women with chronic widespread pain—An explorative proteomic study of the trapezius muscle. Sci. Rep. 2015, 5, 11894. [Google Scholar] [CrossRef] [PubMed]
- Christidis, N.; Ghafouri, B.; Larsson, A.; Palstam, A.; Mannerkorpi, K.; Bileviciute-Ljungar, I.; Löfgren, M.; Bjersing, J.; Kosek, E.; Gerdle, B.; et al. Comparison of the Levels of Pro-Inflammatory Cytokines Released in the Vastus Lateralis Muscle of Patients with Fibromyalgia and Healthy Controls during Contractions of the Quadriceps Muscle—A Microdialysis Study. PLoS ONE 2015, 10, e0143856. [Google Scholar] [CrossRef] [PubMed]
- Ernberg, M.; Christidis, N.; Ghafouri, B.; Bileviciute-Ljungar, I.; Löfgren, M.; Larsson, A.; Palstam, A.; Bjersing, J.; Mannerkorpi, K.; Kosek, E.; et al. Effects of 15 weeks of resistance exercise on pro-inflammatory cytokine levels in the vastus lateralis muscle of patients with fibromyalgia. Arthritis Res. Ther. 2016, 18, 137. [Google Scholar] [CrossRef]
- Gerdle, B.; Ernberg, M.; Mannerkorpi, K.; Larsson, B.; Kosek, E.; Christidis, N.; Ghafouri, B. Increased Interstitial Concentrations of Glutamate and Pyruvate in Vastus Lateralis of Women with Fibromyalgia Syndrome Are Normalized after an Exercise Intervention—A Case-Control Study. PLoS ONE 2016, 11, e0162010. [Google Scholar] [CrossRef]
- Wåhlén, K.; Ernberg, M.; Kosek, E.; Mannerkorpi, K.; Gerdle, B.; Ghafouri, B. Significant correlation between plasma proteome profile and pain intensity, sensitivity, and psychological distress in women with fibromyalgia. Sci. Rep. 2020, 10, 12508. [Google Scholar] [CrossRef]
- Wåhlén, K.; Yan, H.; Welinder, C.; Ernberg, M.; Kosek, E.; Mannerkorpi, K.; Gerdle, B.; Ghafouri, B. Proteomic Investigation in Plasma from Women with Fibromyalgia in Response to a 15-wk Resistance Exercise Intervention. Med. Sci. Sport. Exerc. 2022, 54, 232–246. [Google Scholar] [CrossRef] [PubMed]
- Palstam, A.; Larsson, A.; Bjersing, J.; Löfgren, M.; Ernberg, M.; Bileviciute-Ljungar, I.; Ghafouri, B.; Sjörs, A.; Larsson, B.; Gerdle, B.; et al. Perceived exertion at work in women with fibromyalgia: Explanatory factors and comparison with healthy women. J. Rehabil. Med. 2014, 46, 773–780. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, F.; Smythe, H.A.; Yunus, M.B.; Bennett, R.M.; Bombardier, C.; Goldenberg, D.L.; Tugwell, P.; Campbell, S.M.; Abeles, M.; Clark, P. The American College of Rheumatology 1990 Criteria for the Classification of Fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis Rheum 1990, 33, 160–172. [Google Scholar] [CrossRef]
- Larsson, A.; Palstam, A.; Löfgren, M.; Ernberg, M.; Bjersing, J.; Bileviciute-Ljungar, I.; Gerdle, B.; Kosek, E.; Mannerkorpi, K. Resistance exercise improves muscle strength, health status and pain intensity in fibromyalgia—A randomized controlled trial. Arthritis Res. Ther. 2015, 17, 161. [Google Scholar] [CrossRef] [PubMed]
- Zigmond, A.S.; Snaith, R. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Boonstra, A.M.; Schiphorst Preuper, H.R.; Balk, G.A.; Stewart, R.E. Cut-off points for mild, moderate, and severe pain on the visual analogue scale for pain in patients with chronic musculoskeletal pain. Pain 2014, 155, 2545–2550. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, M.J.L.; Bishop, S.; Pivik, J. The Pain Catastrophizing Scale: Development and validation. Psychol. Assess. 1995, 7, 524–532. [Google Scholar] [CrossRef]
- Hedin, P.J.; Hamne, M.; Burckhardt, C.S.; Engström-Laurent, A. The Fibromyalgia Impact Questionnaire, a Swedish translation of a new tool for evaluation of the fibromyalgia patient. Scand. J. Rheumatol. 1995, 24, 69–75. [Google Scholar] [CrossRef]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef]
- Ware, J.E., Jr.; Gandek, B. Overview of the SF-36 health survey and the international quality of life assessment (IQOLA) project. J. Clin. Epidemiol. 1998, 51, 903–912. [Google Scholar] [CrossRef]
- Wåhlén, K.; Olausson, P.; Carlsson, A.; Ghafouri, N.; Gerdle, B.; Ghafouri, B. Systemic alterations in plasma proteins from women with chronic widespread pain compared to healthy controls: A proteomic study. J. Pain Res. 2017, 10, 797–809. [Google Scholar] [CrossRef] [PubMed]
- Wheelock, A.M.; Wheelock, C.E. Trials and tribulations of omics data analysis: Assessing quality of SIMCA-based multivariate models using examples from pulmonary medicine. Mol. Biosyst. 2013, 9, 2589–2596. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, L.; Johansson, E.; Kettaneh-Wold, N.; Trygg, J.; Wikström, C.; Wold, S. Multi- and Megavariate Data Analysis, Part I and II, 2nd ed.; Umetrics AB: Umeå, Sweden, 2016. [Google Scholar]
- Szklarczyk, D.; Gable, A.L.; Lyon, D.; Junge, A.; Wyder, S.; Huerta-Cepas, J.; Simonovic, M.; Doncheva, N.T.; Morris, J.H.; Bork, P.; et al. STRING v11: Protein-protein association networks with increased coverage, supporting functional discovery in genome-wide experimental datasets. Nucleic Acids Res. 2019, 47, D607–D613. [Google Scholar] [CrossRef]
- Ghafouri, B.; Edman, E.; Löf, M.; Lund, E.; Leinhard, O.D.; Lundberg, P.; Forsgren, M.F.; Gerdle, B.; Dong, H.J. Fibromyalgia in women: Association of inflammatory plasma proteins, muscle blood flow, and metabolism with body mass index and pain characteristics. Pain Rep. 2022, 7, e1042. [Google Scholar] [CrossRef]
- Han, C.L.; Sheng, Y.C.; Wang, S.Y.; Chen, Y.H.; Kang, J.H. Serum proteome profiles revealed dysregulated proteins and mechanisms associated with fibromyalgia syndrome in women. Sci. Rep. 2020, 10, 12347. [Google Scholar] [CrossRef]
- Ramirez-Tejero, J.A.; Martínez-Lara, E.; Rus, A.; Camacho, M.V.; Del Moral, M.L.; Siles, E. Insight into the biological pathways underlying fibromyalgia by a proteomic approach. J. Proteom. 2018, 186, 47–55. [Google Scholar] [CrossRef]
- Khoonsari, P.E.; Ossipova, E.; Lengqvist, J.; Svensson, C.I.; Kosek, E.; Kadetoff, D.; Jakobsson, P.J.; Kultima, K.; Lampa, J. The human CSF pain proteome. J. Proteom. 2019, 190, 67–76. [Google Scholar] [CrossRef]
- Ciregia, F.; Giacomelli, C.; Giusti, L.; Boldrini, C.; Piga, I.; Pepe, P.; Consensi, A.; Gori, S.; Lucacchini, A.; Mazzoni, M.R.; et al. Putative salivary biomarkers useful to differentiate patients with fibromyalgia. J. Proteom. 2019, 190, 44–54. [Google Scholar] [CrossRef] [PubMed]
- Parisien, M.; Lima, L.V.; Dagostino, C.; El-Hachem, N.; Drury, G.L.; Grant, A.V.; Huising, J.; Verma, V.; Meloto, C.B.; Silva, J.R.; et al. Acute inflammatory response via neutrophil activation protects against the development of chronic pain. Sci. Transl. Med. 2022, 14, eabj9954. [Google Scholar] [CrossRef]
- Schrøder, H.D.; Drewes, A.M.; Andreasen, A. Muscle biopsy in fibromyalgia. J. Musculoskelet. Pain 1993, 1, 165–169. [Google Scholar] [CrossRef]
- Ruggiero, L.; Manganelli, F.; Santoro, L. Muscle pain syndromes and fibromyalgia: The role of muscle biopsy. Curr. Opin. Support Palliat. Care 2018, 12, 382–387. [Google Scholar] [CrossRef] [PubMed]
- Olausson, P.; Gerdle, B.; Ghafouri, N.; Larsson, B.; Ghafouri, B. Identification of proteins from interstitium of trapezius muscle in women with chronic myalgia using microdialysis in combination with proteomics. PLoS ONE 2012, 7, e52560. [Google Scholar] [CrossRef] [PubMed]
- Srikuea, R.; Symons, T.B.; Long, D.E.; Lee, J.D.; Shang, Y.; Chomentowski, P.J.; Yu, G.; Crofford, L.J.; Peterson, C.A. Association of fibromyalgia with altered skeletal muscle characteristics which may contribute to postexertional fatigue in postmenopausal women. Arthritis Rheum 2013, 65, 519–528. [Google Scholar] [CrossRef] [PubMed]
- Katz, D.L.; Greene, L.; Ali, A.; Faridi, Z. The pain of fibromyalgia syndrome is due to muscle hypoperfusion induced by regional vasomotor dysregulation. Med. Hypotheses 2007, 69, 517–525. [Google Scholar] [CrossRef] [PubMed]
- Holloway, K.V.; O’Gorman, M.; Woods, P.; Morton, J.P.; Evans, L.; Cable, N.T.; Goldspink, D.F.; Burniston, J.G. Proteomic investigation of changes in human vastus lateralis muscle in response to interval-exercise training. Proteomics 2009, 9, 5155–5174. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | CON n = 28 | FM n = 26 | p-Value |
|---|---|---|---|
| Age (years) | 53.4 (±9.8) | 54.0 (±8.1) | 0.98 |
| BMI (kg/m2) | 24.5 (±4.8) | 27.5 (±5.4) | 0.02 |
| FM duration (years) | - | 14.1 (±7.8) | - |
| Systolic BP (mmHg) | 131 (±15.4) | 134 (±20) | 0.73 |
| Diastolic BP (mmHg) | 82 (±8.2) | 84 (±9.9) | 0.59 |
| Tender points (n) | - | 16 (±1.5) | - |
| Clinical Variables | CON Baseline n = 28 | FM Baseline n = 26 | FM vs. CON Baseline p-Value | CON Post Exercise n = 26 | FM Post Exercise n = 25 | FM vs. CON Post Exercise p-Value | FM Baseline vs. Post Exercise p-Value |
|---|---|---|---|---|---|---|---|
| Pain intensity (Global VAS) | 2.2 (±6.4) | 48.4 (±24.0) | <0.001 | 5.5 (±15.6) | 34.1 (±23.3) | <0.001 | 0.021 |
| HADS depression | 1.6 (±1.7) | 6.0 (±4.0) | <0.001 | 1.5 (±2.1) | 5.5 (±4.3) | <0.001 | 0.138 |
| HADS anxiety | 3.3 (±3.1) | 6.7 (±4.4) | 0.003 | 2.8 (±3.0) | 6.8 (±4.7) | 0.001 | 1.00 |
| PCS | 7.0 (±11.5) | 17.8 (±11.4) | 0.002 | 3.5 (±4.8) | 16.7 (±10.1) | <0.001 | 0.244 |
| FIQ | 6.9 (±9.3) | 59. 8 (±13.9) | <0.001 | 9.1 (±13.9) | 55.2 (±20.1) | <0.001 | 0.179 |
| SF-36 PSC | 54. 6 (±4.6) | 29.6 (±7.7) | <0.001 | 53.3 (±9.2) | 33.1 (±8.6) | <0.001 | 0.036 |
| SF-36 MCS | 51.4 (±6.0) | 42.7 (±10.9) | 0.010 | 52.4 (±7.4) | 43.3 (±11.9) | 0.003 | 0.274 |
| PDI | 8.5 (±2.9) | 36.2 (±13.7) | <0.001 | 10.1 (±6.9) | 31.5 (±12.9) | <0.001 | 0.015 |
| Protein Accession Number (Uniprot) | Protein Abbrev. | Protein Name | VIPpred | p(corr) | CON Baseline Mean (±SD) n = 28 | CON Post Mean (±SD) n = 26 | p-Value CON Baseline vs. Post | Ratio CON Post/Baseline | FM Baseline Mean (±SD) n = 26 | FM Post Mean (±SD) n = 25 | p-Value FM Baseline vs. Post | Ratio FM Post/Baseline | Ratio FM/CON Baseline | Ratio FM/CON Post |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Q9NP98 | MYOZ1 | Myozenin-1 | 1.54 | 0.50 | 1.15 × 107 (±9.19 × 106) | 1.16 × 107 (±1.13 × 107) | 0.79 | 1.00 | 6.19 × 106 (±8.65 × 106) | 8.87 × 106 (±8.99 × 106) | 0.26 | 1.43 | 0.54 | 0.77 |
| P68133 | ACTA1 | Actin, alpha skeletal muscle (Alpha-actin-1) | 1.52 | 0.49 | 2.96 × 107 (±2.11 × 107) | 2.47 × 107 (±1.43 × 107) | 0.07 | 0.84 | 2.11 × 107 (±1.56 × 107) | 2.72 × 107 (±1.70 × 107) | 0.14 | 1.29 | 0.71 | 1.10 |
| P06727 | APOA4 | Apolipoprotein A-IV | 1.45 | 0.47 | 5.86 × 105 (±9.64 × 105) | 2.46 × 105 (±7.31 × 105) | 0.24 | 0.42 | 2.29 × 105 (±6.56 × 105) | 3.83 × 105 (±7.31 × 105) | 0.12 | 1.67 | 0.39 | 1.56 |
| P12883 | MYH7 | Myosin-7 | 1.43 | 0.46 | 1.33 × 108 (±1.04 × 108) | 1.18 × 108 (±8.98 × 107) | 0.31 | 0.89 | 6.74 × 107 (±6.70 × 107) | 7.48 × 107 (±7.31 × 107) | 0.73 | 1.11 | 0.51 | 0.63 |
| P20929 | NEB | Nebulin | 1.39 | 0.45 | 1.72 × 107 (±1.70 × 107) | 1.72 × 107 (±1.71 × 107) | 0.76 | 1.00 | 9.44 × 106 (±1.01 × 107) | 1.46 × 107 (±1.86 × 107) | 0.55 | 1.55 | 0.55 | 0.85 |
| P02753 | RBP4 | Retinol-binding protein 4 | 1.38 | 0.45 | 5.23 × 106 (±2.86 × 106) | 4.19 × 106 (±3.78 × 106) | 0.26 | 0.80 | 3.20 × 106 (±3.14 × 106) | 5.59 × 106 (±4.03 × 106) | 0.03 | 1.75 | 0.61 | 1.33 |
| Q9UBF9 | MYOT | Myotilin | 1.37 | 0.44 | 1.16 × 106 (±1.72 × 106) | 7.62 × 105 (±1.23 × 106) | 0.24 | 0.65 | 3.08 × 105 (±8.26 × 105) | 6.27 × 105 (±8.88 × 105) | 0.26 | 2.04 | 0.26 | 0.82 |
| P07951 | TPM2 | Tropomyosin beta chain | 1.26 | 0.41 | 1.18 × 106 (±2.23 × 106) | 7.06 × 105 (±1.15 × 106) | 0.21 | 0.60 | 3.95 × 105 (±8.04 × 105) | 4.36 × 105 (±8.28 × 105) | 0.78 | 1.10 | 0.34 | 0.62 |
| P19652 | ORM2 | Alpha-1-acid glycoprotein 2 | 1.25 | −0.40 | 2.08 × 107 (±1.37 × 107) | 2.29 × 107 (±2.62 × 107) | 0.58 | 1.10 | 2.98 × 107 (±2.02 × 107) | 1.55 × 107 (±1.03 × 107) | 0.01 | 0.52 | 1.44 | 0.68 |
| P06396 | GSN | Gelsolin | 1.23 | 0.40 | 2.64 × 106 (±2.87 × 106) | 9.78 × 105 (±1.06 × 106) | 0.07 | 0.37 | 1.38 × 106 (±2.03 × 106) | 1.66 × 106 (±1.67 × 106) | 0.44 | 1.20 | 0.52 | 1.69 |
| Q9UMS6 | SYNPO2 | Synaptopodin-2 | 1.21 | 0.39 | 4.60 × 10−6 (±5.05 × 106) | 3.49 × 106 (±4.50 × 106) | 0.45 | 0.76 | 2.94 × 106 (±3.93 × 106) | 4.87 × 106 (±7.05 × 106) | 0.84 | 1.66 | 0.64 | 1.40 |
| P0C0L4 | C4A | Complement C4-A | 1.19 | 0.39 | 9.33 × 106 (±7.61 × 106) | 1.03 × 107 (±1.27 × 107) | 0.63 | 1.11 | 7.60 × 106 (±5.98 × 106) | 8.48 × 106 (±6.77 × 106) | 0.93 | 1.12 | 0.81 | 0.82 |
| Q8N3V7 | SYNPO | Synaptopodin | 1.19 | 0.39 | 1.31 × 106 (±2.04 × 106) | 6.77 × 105 (±1.46 × 106) | 0.17 | 0.52 | 4.79 × 105 (±9.18 × 105) | 1.35 × 106 (±2.46 × 106) | 0.14 | 2.83 | 0.37 | 2.00 |
| P01834 | IGKC | Immunoglobulin kappa constant | 1.18 | 0.38 | 1.83 × 107 (±1.37 × 107) | 9.30 × 106 (±1.51 × 107) | 0.02 | 0.51 | 1.28 × 107 (±1.14 × 107) | 1.49 × 107 (±1.25 × 107) | 0.35 | 1.16 | 0.70 | 1.60 |
| P01042 | KNG1 | Kininogen-1 | 1.18 | 0.38 | 1.43 × 106 (±1.55 × 106) | 3.29 × 105 (±8.31 × 105) | 0.04 | 0.23 | 8.79 × 105 (±1.31 × 106) | 1.19 × 106 (±1.17 × 106) | 0.16 | 1.36 | 0.62 | 3.62 |
| Q9UHP9 | SMPX | Small muscular protein | 1.18 | 0.38 | 2.48 × 106 (±3.23 × 106) | 2.91 × 106 (±3.56 × 106) | 0.30 | 1.17 | 1.01 × 106 (±1.72 × 106) | 2.16 × 106 (±2.60 × 106) | 0.12 | 2.14 | 0.41 | 0.74 |
| P02675 | FGB | Fibrinogen beta chain | 1.17 | 0.38 | 2.50 × 107 (±2.75 × 107) | 3.50 × 107 (±5.03 × 107) | 0.90 | 1.40 | 1.52 × 107 (±1.36 × 107) | 2.44 × 107 (±2.91 × 107) | 0.32 | 1.61 | 0.61 | 0.70 |
| P01024 | C3 | Complement C3 | 1.15 | 0.37 | 1.14 × 107 (±1.16 × 107) | 1.21 × 107 (±3.24 × 107) | 0.13 | 1.07 | 9.14 × 106 (±1.17 × 107) | 1.21 × 107 (±1.57 × 107) | 0.60 | 1.33 | 0.80 | 1.00 |
| P00747 | PLG | Plasminogen | 1.14 | 0.37 | 1.32 × 107 (±8.55 × 106) | 9.35 × 106 (±6.78 × 106) | 0.03 | 0.71 | 8.33 × 106 (±1.02 × 107) | 8.06 × 106 (±4.82 × 106) | 0.71 | 0.97 | 0.63 | 0.86 |
| P02647 | APOA1 | Apolipoprotein A-I | 1.13 | 0.37 | 4.25 × 107 (±3.80 × 107) | 3.20 × 107 (±8.00 × 107) | 0.06 | 0.75 | 2.98 × 107 (±3.35 × 107) | 3.15 × 107 (±3.56 × 107) | 0.91 | 1.05 | 0.70 | 0.98 |
| Q8WZ42 | TTN | Titin | 1.13 | 0.37 | 8.73 × 107 (±8.22 × 107) | 9.42 × 107 (±8.56 × 107) | 0.83 | 1.08 | 5.49 × 107 (±4.46 × 107) | 8.13 × 107 (±9.36 × 107) | 0.45 | 1.48 | 0.63 | 0.86 |
| P52179 | MYOM1 | Myomesin-1 | 1.09 | 0.35 | 3.25 × 106 (±2.34 × 106) | 3.04 × 106 (±3.09 × 106) | 0.19 | 0.94 | 1.84 × 106 (±2.33 × 106) | 2.86 × 106 (±3.19 × 106) | 0.17 | 1.55 | 0.57 | 0.94 |
| E9PAV3 | NACA | Nascent polypeptide-associated complex subunit alpha, muscle-specific form | 1.09 | 0.35 | 9.37 × 105 (±1.67 × 106) | 1.74 × 106 (±2.26 × 106) | 0.39 | 1.86 | 2.23 × 105 (±7.01 × 105) | 1.41 × 106 (±3.74 × 106) | 0.16 | 6.31 | 0.24 | 0.81 |
| P62987 | UBA52 | Ubiquitin-60S ribosomal protein L40 | 1.09 | 0.35 | 9.94 × 106 (±2.10 × 107) | 1.15 × 107 (±1.65 × 107) | 0.34 | 1.16 | 2.91 × 106 (±3.32 × 106) | 6.63 × 106 (±8.65 × 106) | 0.13 | 2.28 | 0.29 | 0.57 |
| P01861 | IGHG4 | Immunoglobulin heavy constant gamma 4 | 1.08 | 0.35 | 6.01 × 106 (±5.90 × 106) | 2.39 × 106 (±5.04 × 106) | 0.04 | 0.40 | 3.46 × 106 (±5.57 × 106) | 2.92 × 106 (±3.51 × 106) | 0.92 | 0.85 | 0.58 | 1.22 |
| P02671 | FGA | Fibrinogen alpha chain | 1.03 | 0.33 | 1.59 × 108 (±1.25 × 108) | 1.84 × 108 (±1.95 × 108) | 0.85 | 1.15 | 1.20 × 108 (±9.54 × 107) | 1.12 × 108 (±7.09 × 107) | 0.82 | 0.93 | 0.75 | 0.61 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghafouri, B.; Matikhan, D.; Christidis, N.; Ernberg, M.; Kosek, E.; Mannerkorpi, K.; Gerdle, B.; Wåhlén, K. The Vastus Lateralis Muscle Interstitium Proteome Changes after an Acute Nociception in Patients with Fibromyalgia Compared to Healthy Subjects—A Microdialysis Study. Biomedicines 2023, 11, 206. https://doi.org/10.3390/biomedicines11010206
Ghafouri B, Matikhan D, Christidis N, Ernberg M, Kosek E, Mannerkorpi K, Gerdle B, Wåhlén K. The Vastus Lateralis Muscle Interstitium Proteome Changes after an Acute Nociception in Patients with Fibromyalgia Compared to Healthy Subjects—A Microdialysis Study. Biomedicines. 2023; 11(1):206. https://doi.org/10.3390/biomedicines11010206
Chicago/Turabian StyleGhafouri, Bijar, Daria Matikhan, Nikolaos Christidis, Malin Ernberg, Eva Kosek, Kaisa Mannerkorpi, Björn Gerdle, and Karin Wåhlén. 2023. "The Vastus Lateralis Muscle Interstitium Proteome Changes after an Acute Nociception in Patients with Fibromyalgia Compared to Healthy Subjects—A Microdialysis Study" Biomedicines 11, no. 1: 206. https://doi.org/10.3390/biomedicines11010206
APA StyleGhafouri, B., Matikhan, D., Christidis, N., Ernberg, M., Kosek, E., Mannerkorpi, K., Gerdle, B., & Wåhlén, K. (2023). The Vastus Lateralis Muscle Interstitium Proteome Changes after an Acute Nociception in Patients with Fibromyalgia Compared to Healthy Subjects—A Microdialysis Study. Biomedicines, 11(1), 206. https://doi.org/10.3390/biomedicines11010206