
Plasma Levels of Proprotein Convertase Subtilisin/Kexin Type 9 Are Inversely Associated with N-Terminal Pro B-Type Natriuretic Peptide in Older Men and Women

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Clinical and Lab Parameters
2.3. NT-proBNP Assay
2.4. PCSK9 Assay
2.5. Statistical Analysis
3. Results
3.1. General Characteristics
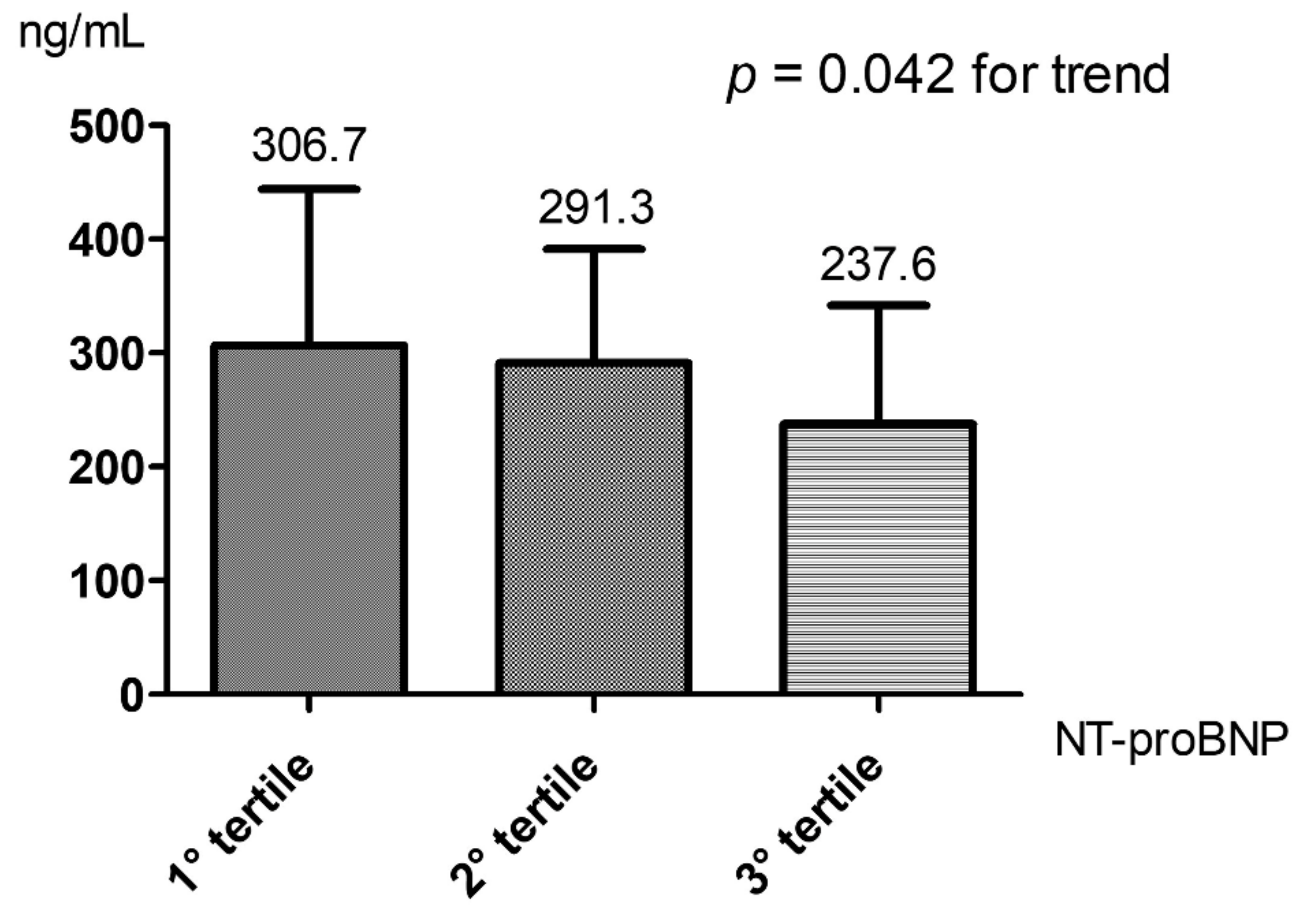
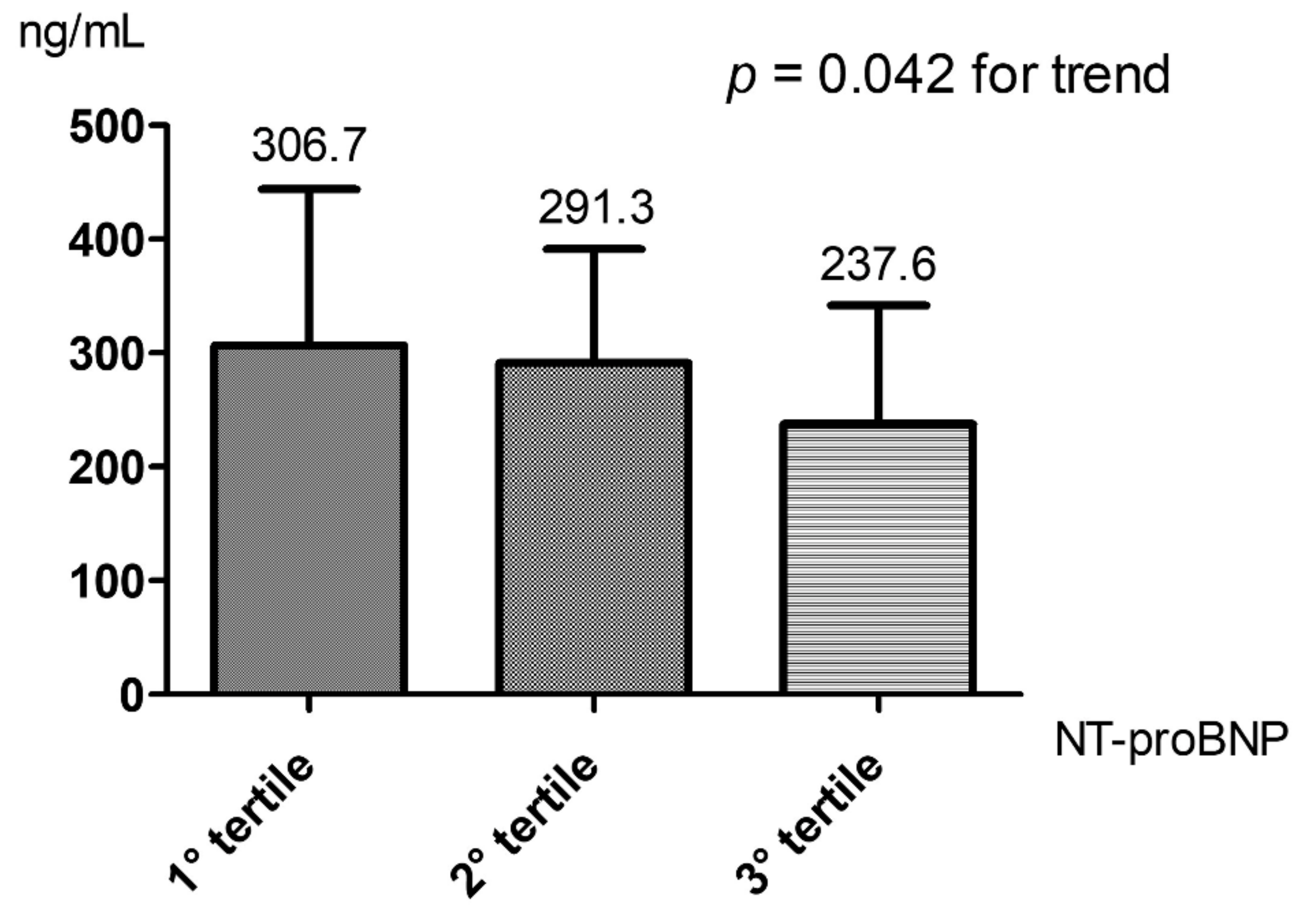
3.2. Plasma PCSK9 and NT-proBNP
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ference, B.A.; Ginsberg, H.N.; Graham, I.; Ray, K.K.; Packard, C.J.; Bruckert, E.; Hegele, R.A.; Krauss, R.M.; Raal, F.J.; Schunkert, H.; et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel. Eur. Heart J. 2017, 38, 2459–2472. [Google Scholar] [CrossRef]
- Luo, Y.; Warren, L.; Xia, D.; Jensen, H.; Sand, T.; Petras, S.; Qin, W.; Miller, K.S.; Hawkins, J. Function and distribution of circulating human PCSK9 expressed extrahepatically in transgenic mice. J. Lipid Res. 2009, 50, 1581–1588. [Google Scholar] [CrossRef] [PubMed]
- Seidah, N.G.; Benjannet, S.; Wickham, L.; Marcinkiewicz, J.; Jasmin, S.B.; Stifani, S.; Basak, A.; Prat, A.; Chrétien, M. The secretory proprotein convertase neural apoptosis-regulated convertase 1 (NARC-1): Liver regeneration and neuronal differentiation. Proc. Natl. Acad. Sci. USA 2003, 100, 928–933. [Google Scholar] [CrossRef]
- Bordicchia, M.; Spannella, F.; Ferretti, G.; Bacchetti, T.; Vignini, A.; Di Pentima, C.; Mazzanti, L.; Sarzani, R. PCSK9 is Expressed in Human Visceral Adipose Tissue and Regulated by Insulin and Cardiac Natriuretic Peptides. Int. J. Mol. Sci. 2019, 20, 245. [Google Scholar] [CrossRef]
- Shimada, Y.J.; Cannon, C.P. PCSK9 (Proprotein convertase subtilisin/kexin type 9) inhibitors: Past, present, and the future. Eur. Heart J. 2015, 36, 2415–2424. [Google Scholar] [CrossRef]
- Seidah, N.G.; Awan, Z.; Chrétien, M.; Mbikay, M. PCSK9: A key modulator of cardiovascular health. Circ. Res. 2014, 114, 1022–1036. [Google Scholar] [CrossRef]
- Han, B.; Eacho, P.I.; Knierman, M.; Troutt, J.S.; Konrad, R.J.; Yu, X.; Schroeder, K.M. Isolation and characterization of the circulating truncated form of PCSK9. J. Lipid Res. 2014, 55, 1505–1514. [Google Scholar] [CrossRef] [PubMed]
- Moreau, F.; Thédrez, A.; Garçon, D.; Ayer, A.; Sotin, T.; Dijk, W.; Blanchard, C.; Chadeuf, G.; Arnaud, L.; Croyal, M.; et al. PCSK9 is not secreted from mature differentiated intestinal cells. J. Lipid Res. 2021, 62, 100096. [Google Scholar] [CrossRef] [PubMed]
- Schlueter, N.; de Sterke, A.; Willmes, D.M.; Spranger, J.; Jordan, J.; Birkenfeld, A.L. Metabolic actions of natriuretic peptides and therapeutic potential in the metabolic syndrome. Pharmacol. Ther. 2014, 144, 12–27. [Google Scholar] [CrossRef] [PubMed]
- Spannella, F.; Giulietti, F.; Bordicchia, M., Jr.; Burnett, J.C.; Sarzani, R. Association between Cardiac Natriuretic Peptides and Lipid Profile: A Systematic Review and Meta-Analysis. Sci. Rep. 2019, 9, 19178. [Google Scholar] [CrossRef] [PubMed]
- Volpe, M. Natriuretic peptides and cardio-renal disease. Int. J. Cardiol. 2014, 176, 630–639. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Spannella, F.; Giulietti, F.; Cocci, G.; Landi, L.; Borioni, E.; Lombardi, F.; Rosettani, G.; Bernardi, B.; Bordoni, V.; Giordano, P.; et al. N-terminal pro B-Type natriuretic peptide is inversely correlated with low density lipoprotein cholesterol in the very elderly. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 629–635. [Google Scholar] [CrossRef] [PubMed]
- Martin, S.S.; Blaha, M.J.; Elshazly, M.; Toth, P.P.; Kwiterovich, P.O.; Blumenthal, R.S.; Jones, S.R. Comparison of a Novel Method vs the Friedewald Equation for Estimating Low-Density Lipoprotein Cholesterol Levels From the Standard Lipid Profile. JAMA 2013, 310, 2061–2068. [Google Scholar] [CrossRef]
- Morris, J.N.; Fries, B.E.; Morris, S.A. Scaling ADLs within the MDS. J. Gerontol. Series A 1999, 54, M546–M553. [Google Scholar] [CrossRef] [PubMed]
- Rozzini, R.; Frisoni, G.B.; Ferrucci, L.; Barbisoni, P.; Sabatini, T.; Ranieri, P.; Guralnik, J.M.; Trabucchi, M. Geriatric Index of Comorbidity: Validation and comparison with other measures of comorbidity. Age Ageing 2002, 31, 277–285. [Google Scholar] [CrossRef] [PubMed]
- Ruscica, M.; Simonelli, S.; Botta, M.; Ossoli, A.; Lupo, M.G.; Magni, P.; Corsini, A.; Arca, M.; Pisciotta, L.; Veglia, F.; et al. Plasma PCSK9 levels and lipoprotein distribution are preserved in carriers of genetic HDL disorders. Biochim. Biophys. Acta (BBA) -Mol. Cell Biol. Lipids 2018, 1863, 991–997. [Google Scholar] [CrossRef] [PubMed]
- Norata, G.D.; Tibolla, G.; Catapano, A.L. Targeting PCSK9 for Hypercholesterolemia. Annu. Rev. Pharmacol. Toxicol. 2014, 54, 273–293. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Yan, B.; Tai, S.; Zhou, S.; Zheng, X.-L. PCSK9: Associated with cardiac diseases and their risk factors? Arch. Biochem. Biophys. 2020, 704, 108717. [Google Scholar] [CrossRef] [PubMed]
- Ramin-Mangata, S.; Wargny, M.; Pichelin, M.; Le May, C.; Thedrez, A.; Blanchard, V.; Nativel, B.; Santos, R.D.; Benseñor, I.M.; Lotufo, P.A.; et al. Circulating PCSK9 levels are not associated with the conversion to type 2 diabetes. Atherosclerosis 2020, 293, 49–56. [Google Scholar] [CrossRef]
- Shi, J.; Li, X.; Zhang, W.; Niu, Y.; Lin, N.; Zhang, H.; Ning, G.; Fan, J.; Qin, L.; Su, Q.; et al. Circulating Proprotein Convertase Subtilisin/Kexin Type 9 Levels and Cardiometabolic Risk Factors: A Population-Based Cohort Study. Front. Cardiovasc. Med. 2021, 8, 664583. [Google Scholar] [CrossRef] [PubMed]
- Wong, Y.-K.; Tse, H.-F. Circulating Biomarkers for Cardiovascular Disease Risk Prediction in Patients with Cardiovascular Disease. Front. Cardiovasc. Med. 2021, 8, 713191. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.M.; Anderson, T.J.; Sikdar, K.; Fung, M.; McQueen, M.J.; Lonn, E.M.; Verma, S. Association of Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) with Cardiovascular Risk in Primary Prevention. Arter. Thromb. Vasc. Biol. 2015, 35, 2254–2259. [Google Scholar] [CrossRef] [PubMed]
- Kheirkhah, A.; Lamina, C.; Rantner, B.; Kollerits, B.; Stadler, M.; Pohlhammer, J.; Klein-Weigel, P.; Fraedrich, G.; Kronenberg, F. Elevated levels of serum PCSK9 in male patients with symptomatic peripheral artery disease: The CAVASIC study. Atherosclerosis 2020, 316, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Bae, K.-H.; Kim, S.W.; Choi, Y.-K.; Seo, J.B.; Kim, N.; Kim, C.-Y.; Lee, W.K.; Lee, S.; Kim, J.G.; Lee, I.-K.; et al. Serum Levels of PCSK9 Are Associated with Coronary Angiographic Severity in Patients with Acute Coronary Syndrome. Diabetes Metab. J. 2018, 42, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Caselli, C.; Del Turco, S.; Ragusa, R.; Lorenzoni, V.; De Graaf, M.; Basta, G.; Scholte, A.; De Caterina, R.; Neglia, D. Association of PCSK9 plasma levels with metabolic patterns and coronary atherosclerosis in patients with stable angina. Cardiovasc. Diabetol. 2019, 18, 144. [Google Scholar] [CrossRef] [PubMed]
- Lakoski, S.G.; Lagace, T.A.; Cohen, J.C.; Horton, J.D.; Hobbs, H.H. Genetic and Metabolic Determinants of Plasma PCSK9 Levels. J. Clin. Endocrinol. Metab. 2009, 94, 2537–2543. [Google Scholar] [CrossRef] [PubMed]
- Zaid, A.; Roubtsova, A.; Essalmani, R.; Marcinkiewicz, J.; Chamberland, A.; Hamelin, J.; Tremblay, M.; Jacques, H.; Jin, W.; Davignon, J.; et al. Proprotein convertase subtilisin/kexin type 9 (PCSK9): Hepatocyte-specific low-density lipoprotein receptor degradation and critical role in mouse liver regeneration. Hepatology 2008, 48, 646–654. [Google Scholar] [CrossRef] [PubMed]
- Khedoe, P.P.S.J.; Hoeke, G.; Kooijman, S.; Dijk, W.; Buijs, J.T.; Kersten, S.; Havekes, L.M.; Hiemstra, P.S.; Berbée, J.F.P.; Boon, M.R.; et al. Brown adipose tissue takes up plasma triglycerides mostly after lipolysis. J. Lipid Res. 2015, 56, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Sengenès, C.; Berlan, M.; De Glisezinski, I.; Lafontan, M.; Galitzky, J. Natriuretic peptides: A new lipolytic pathway in human adipocytes. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol. 2000, 14, 1345–1351. [Google Scholar]
- Kim, S.W.; Park, K.-G. Response: Serum Levels of PCSK9 Are Associated with Coronary Angiographic Severity in Patients with Acute Coronary Syndrome (Diabetes Metab J 2018;42:207-14). Diabetes Metab. J. 2018, 42, 350–352. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Qiu, Y.; Wu, J.; Diao, W.; Zhang, H.; Wang, S.; Du, Z.; Dong, J.; Zhang, M.; Jiang, L. Acute-Phase Plasma PCSK9 Levels and Recurrent Cardiovascular Events in a Chinese Acute Myocardial Infarction Cohort. Cardiology 2018, 141, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Zeller, M.; Lambert, G.; Farnier, M.; Maza, M.; Nativel, B.; Rochette, L.; Vergely, C.; Cottin, Y. PCSK9 levels do not predict severity and recurrence of cardiovascular events in patients with acute myocardial infarction. Nutr. Metab. Cardiovasc. Dis. 2020, 31, 880–885. [Google Scholar] [CrossRef] [PubMed]
- Bayes-Genis, A.; Núñez, J.; Zannad, F.; Ferreira, J.P.; Anker, S.D.; Cleland, J.G.; Dickstein, K.; Filippatos, G.; Lang, C.; Ng, L.; et al. The PCSK9-LDL Receptor Axis and Outcomes in Heart Failure: BIOSTAT-CHF Subanalysis. J. Am. Coll. Cardiol. 2017, 70, 2128–2136. [Google Scholar] [CrossRef] [PubMed]
- Da Dalt, L.; Castiglioni, L.; Baragetti, A.; Audano, M.; Svecla, M.; Bonacina, F.; Pedretti, S.; Uboldi, P.; Benzoni, P.; Giannetti, F.; et al. PCSK9 deficiency rewires heart metabolism and drives heart failure with preserved ejection fraction. Eur. Heart J. 2021, 42, 3078–3090. [Google Scholar] [CrossRef] [PubMed]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk: The Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS). Eur. Heart J. 2019, 41, 111–188. [Google Scholar] [CrossRef]

{kind=link}
| Clinical Characteristics | All Patients (n° 160) | 1st PCSK9 Tertile (n° 54) | 2nd PCSK9 Tertile (n° 53) | 3rd PCSK9 Tertile (n° 53) | p |
|---|---|---|---|---|---|
| Age (years) | 87.8 ± 6.4 | 88.2 ± 5.8 | 87.2 ± 6.7 | 88.0 ± 6.5 | 0.690 |
| Sex (female) | 62.5% | 64.8% | 60.4% | 62.3% | 0.893 |
| GIC (high comorbidity) | 70.3% | 78.0% | 69.8% | 63.5% | 0.274 |
| ADL hierarchy scale: assistance required | 54.8% | 58.0% | 54.7% | 51.9% | 0.471 |
| ADL hierarchy scale: dependence | 12.9% | 8.0% | 18.9% | 11.5% | |
| History of hypertension | 69.7% | 76.0% | 73.6% | 59.6% | 0.148 |
| Type 2 diabetes mellitus | 21.9% | 24.0% | 24.5% | 17.3% | 0.612 |
| History of CAD | 12.3% | 8.0% | 22.6% | 5.8% | 0.017 |
| History of chronic HF | 38.1% | 40.0% | 45.3% | 28.8% | 0.210 |
| Previous TIA/stroke | 15.5% | 18.0% | 13.2% | 15.4% | 0.798 |
| Cognitive impairment | 45.7% | 57.1% | 36.0% | 44.2% | 0.104 |
| Lab parameters | |||||
| TC (mg/dL) | 151.2 ± 39.2 | 147.4 ± 45.0 | 148.5 ± 35.0 | 159.0 ± 35.9 | 0.297 |
| HDL-C (mg/dL) | 46.2 ± 16.9 | 49.3 ± 17.8 | 43.9 ± 14.9 | 45.0 ± 17.7 | 0.240 |
| LDL-C (mg/dL) | 82.7 ± 31.0 | 79.1 ± 35.5 | 80.9 ± 26.2 | 89.1 ± 29.7 | 0.256 |
| Non-HDL-C (mg/dL) | 102.4 ± 36.5 | 98.1 ± 40.2 | 104.6 ± 32.8 | 104.6 ± 36.2 | 0.586 |
| (Non-HDL-C + Non-LDL-C) | 20.0 (15.0–25.0) | 16.0 (13.0–22.0) | 21.0 (15.0–28.0) | 22.0 (17.0–29.0) | 0.026 |
| Triglycerides (mg/dL) | 100.0 (73.3–122.8) | 78.0 (64.3–110.8) | 104.0 (78.0–140.0) | 112.0 (86.0–145.0) | <0.001 |
| NT-proBNP (pg/mL) | 2340 (814–5397) | 3896 (1234–6776) | 2970 (1124–6346) | 1431 (510–3341) | 0.005 |
| Plasma PCSK9 (ng/mL) | 275.2 ± 113.2 | 157.5 ± 42.2 | 262.5 ± 27.4 | 407.8 ± 64.1 | <0.001 |
| Hgb (g/dL) | 11.4 ± 1.8 | 11.1 ± 1.8 | 11.4 ± 1.7 | 11.6 ± 2.0 | 0.295 |
| eGFR (mL/min/1.73 m2) | 54.1 ± 24.6 | 52.8 ± 23.1 | 55.6 ± 24.2 | 53.9 ± 26.7 | 0.846 |
| Glycaemia (mg/dL) | 102.0 (86.5–137.5) | 95.5 (83.0–127.0) | 103.0 (87.0–137.0) | 109.0 (84.0–140.8) | 0.457 |
| Albumin (g/dL) | 3.3 ± 0.6 | 3.4 ± 0.5 | 3.4 ± 0.6 | 3.2 ± 0.5 | 0.053 |
| Βeta | B (95% CI) | p | |
|---|---|---|---|
| ln(NT-proBNP) | −0.361 | −31.33 (−49.49–−13.16) | 0.001 |
| Age (years) | 0.070 | 1.37 (−2.30–5.04) | 0.461 |
| Sex (ref. female) | −0.051 | −12.21 (−51.50–27.08) | 0.540 |
| Albumin (g/dL) | −0.232 | −47.23 (−83.93–10.54) | 0.012 |
| History of chronic HF | 0.065 | 15.02 (−29.76–59.80) | 0.508 |
| Cognitive impairment | −0.012 | −2.80 (−42.80–37.20) | 0.890 |
| GIC (ref. low comorbidity) | −0.107 | −26.87 (−70.00–16.27) | 0.220 |
| Βeta | B (95% CI) | p | |
|---|---|---|---|
| NT-proBNP tertiles | −0.330 | −45.96 (−73.21–−18.70) | 0.001 |
| Age (years) | 0.048 | 0.95 (−2.65–4.54) | 0.604 |
| Sex (ref. female) | −0.065 | −15.52 (−55.18–24.15) | 0.440 |
| Albumin (g/dL) | −0.210 | −42.85 (−79.44–−6.27) | 0.022 |
| History of chronic HF | 0.033 | 7.71 (−35.60–51.03) | 0.725 |
| Cognitive impairment | −0.029 | −6.58 (−46.51–33.35) | 0.745 |
| GIC (ref. low comorbidity) | −0.112 | −28.02 (−71.17–15.13) | 0.201 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spannella, F.; Giulietti, F.; Galeazzi, R.; Passarelli, A.; Re, S.; Di Pentima, C.; Allevi, M.; Magni, P.; Sarzani, R. Plasma Levels of Proprotein Convertase Subtilisin/Kexin Type 9 Are Inversely Associated with N-Terminal Pro B-Type Natriuretic Peptide in Older Men and Women. Biomedicines 2022, 10, 1961. https://doi.org/10.3390/biomedicines10081961
Spannella F, Giulietti F, Galeazzi R, Passarelli A, Re S, Di Pentima C, Allevi M, Magni P, Sarzani R. Plasma Levels of Proprotein Convertase Subtilisin/Kexin Type 9 Are Inversely Associated with N-Terminal Pro B-Type Natriuretic Peptide in Older Men and Women. Biomedicines. 2022; 10(8):1961. https://doi.org/10.3390/biomedicines10081961
Chicago/Turabian StyleSpannella, Francesco, Federico Giulietti, Roberta Galeazzi, Anna Passarelli, Serena Re, Chiara Di Pentima, Massimiliano Allevi, Paolo Magni, and Riccardo Sarzani. 2022. "Plasma Levels of Proprotein Convertase Subtilisin/Kexin Type 9 Are Inversely Associated with N-Terminal Pro B-Type Natriuretic Peptide in Older Men and Women" Biomedicines 10, no. 8: 1961. https://doi.org/10.3390/biomedicines10081961
APA StyleSpannella, F., Giulietti, F., Galeazzi, R., Passarelli, A., Re, S., Di Pentima, C., Allevi, M., Magni, P., & Sarzani, R. (2022). Plasma Levels of Proprotein Convertase Subtilisin/Kexin Type 9 Are Inversely Associated with N-Terminal Pro B-Type Natriuretic Peptide in Older Men and Women. Biomedicines, 10(8), 1961. https://doi.org/10.3390/biomedicines10081961