
Dynamics of Circulating CD14/CD16 Monocyte Subsets in Obstructive Sleep Apnea Syndrome Patients upon Hypoglossal Nerve Stimulation

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Blood Collection and Clinical Data
2.3. FACS Analysis of Monocyte Subsets in Whole Blood
2.4. Statistical Analysis
3. Results
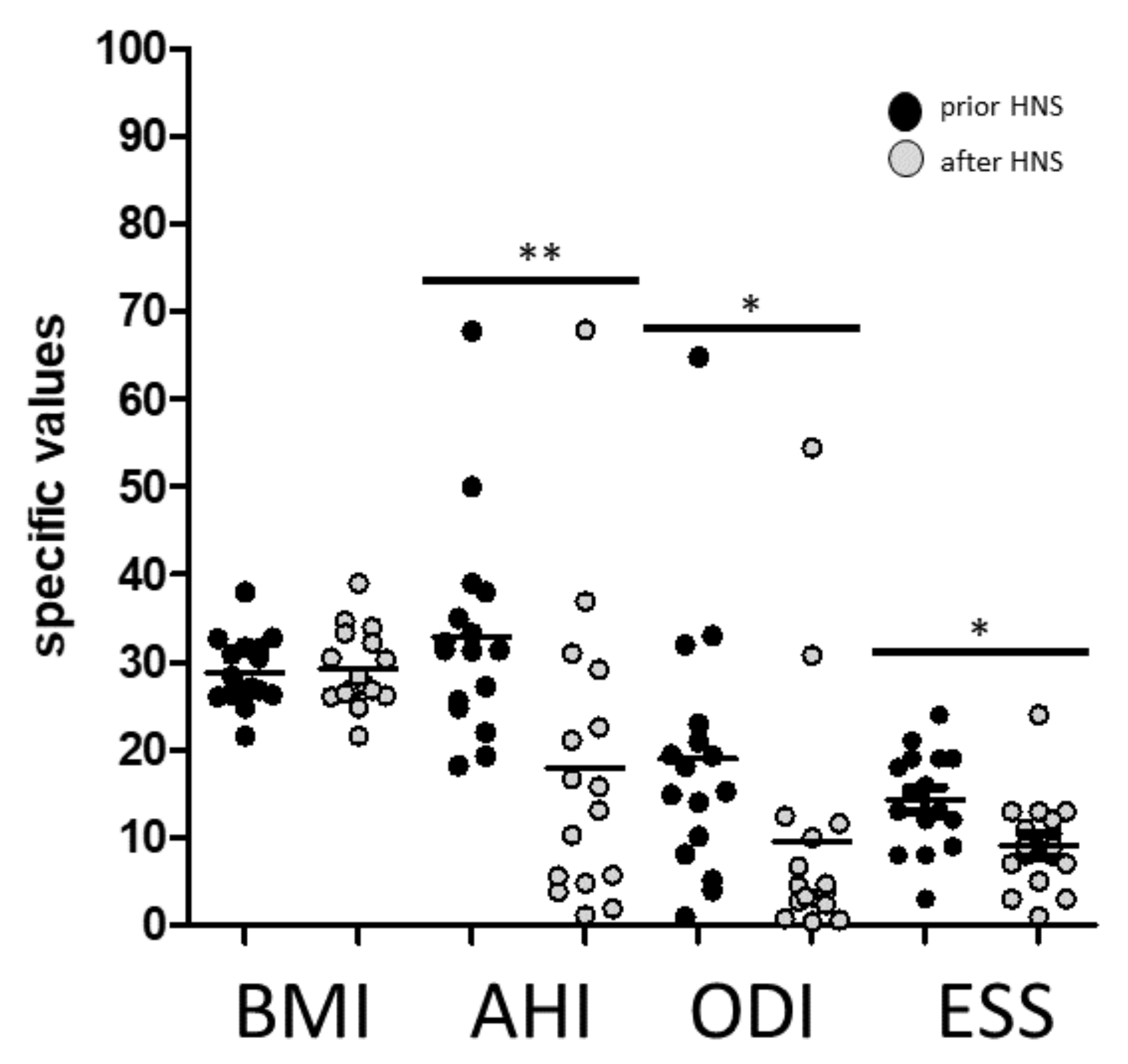
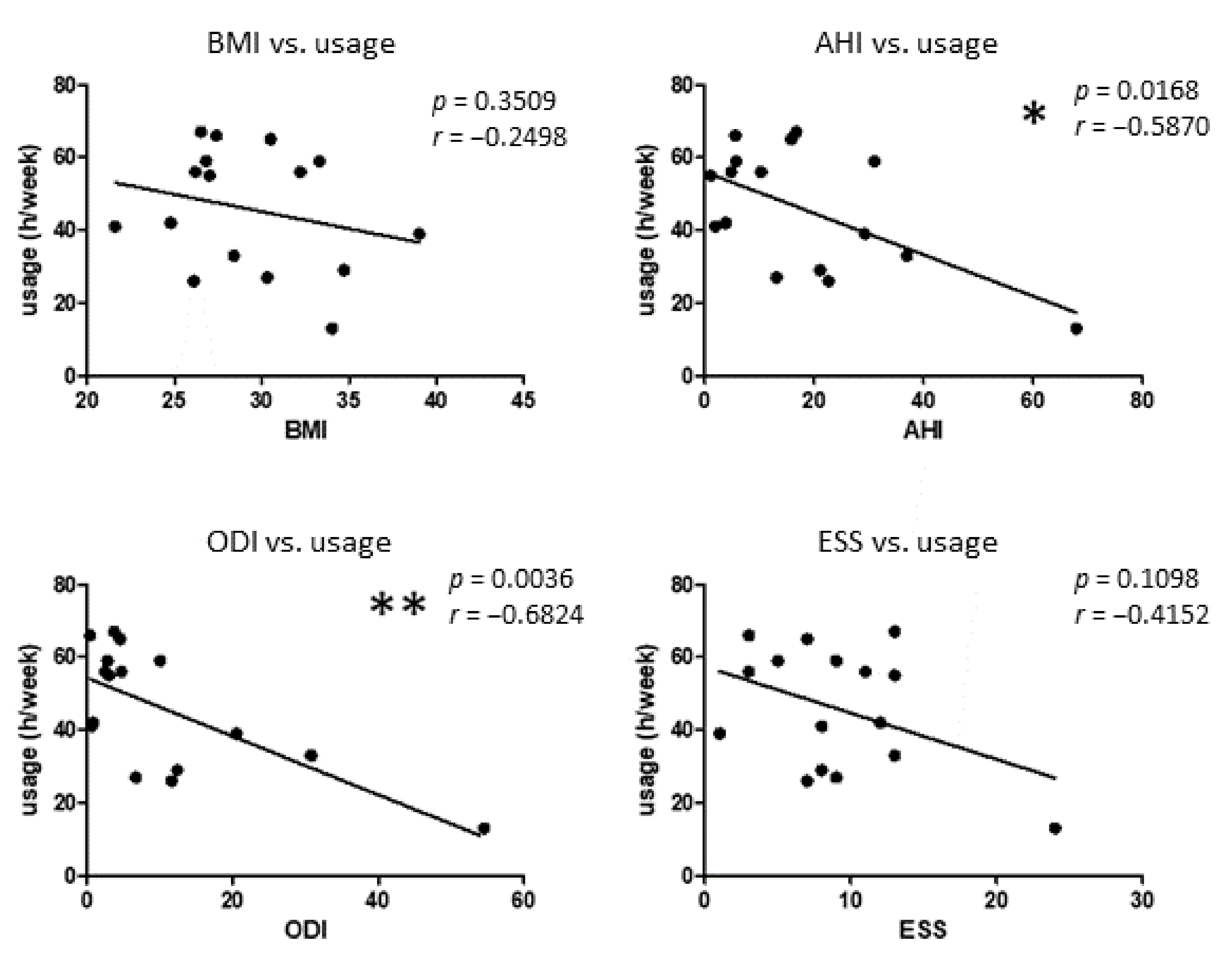
3.1. Patients Characteristics and Response to HNS Therapy
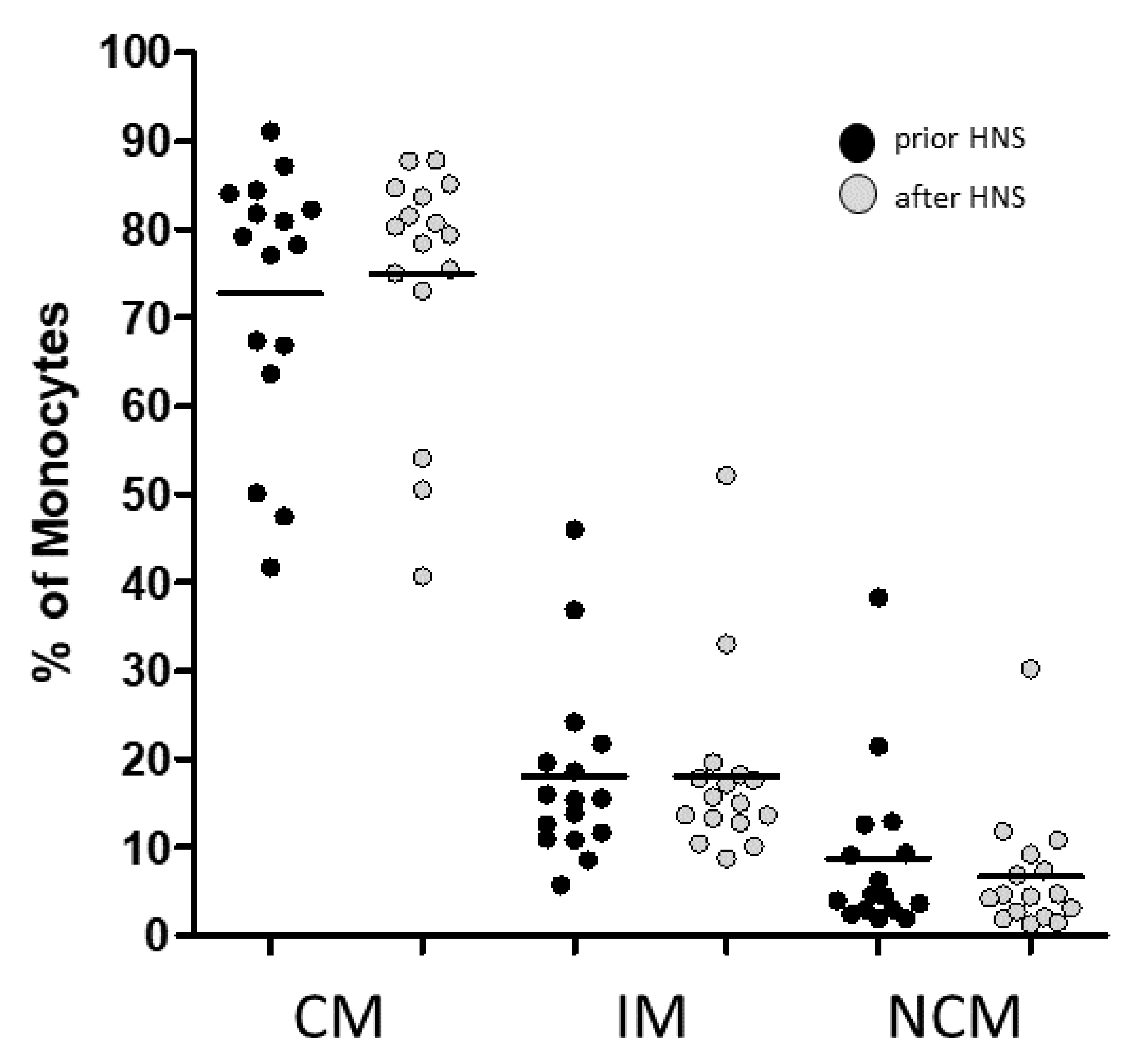
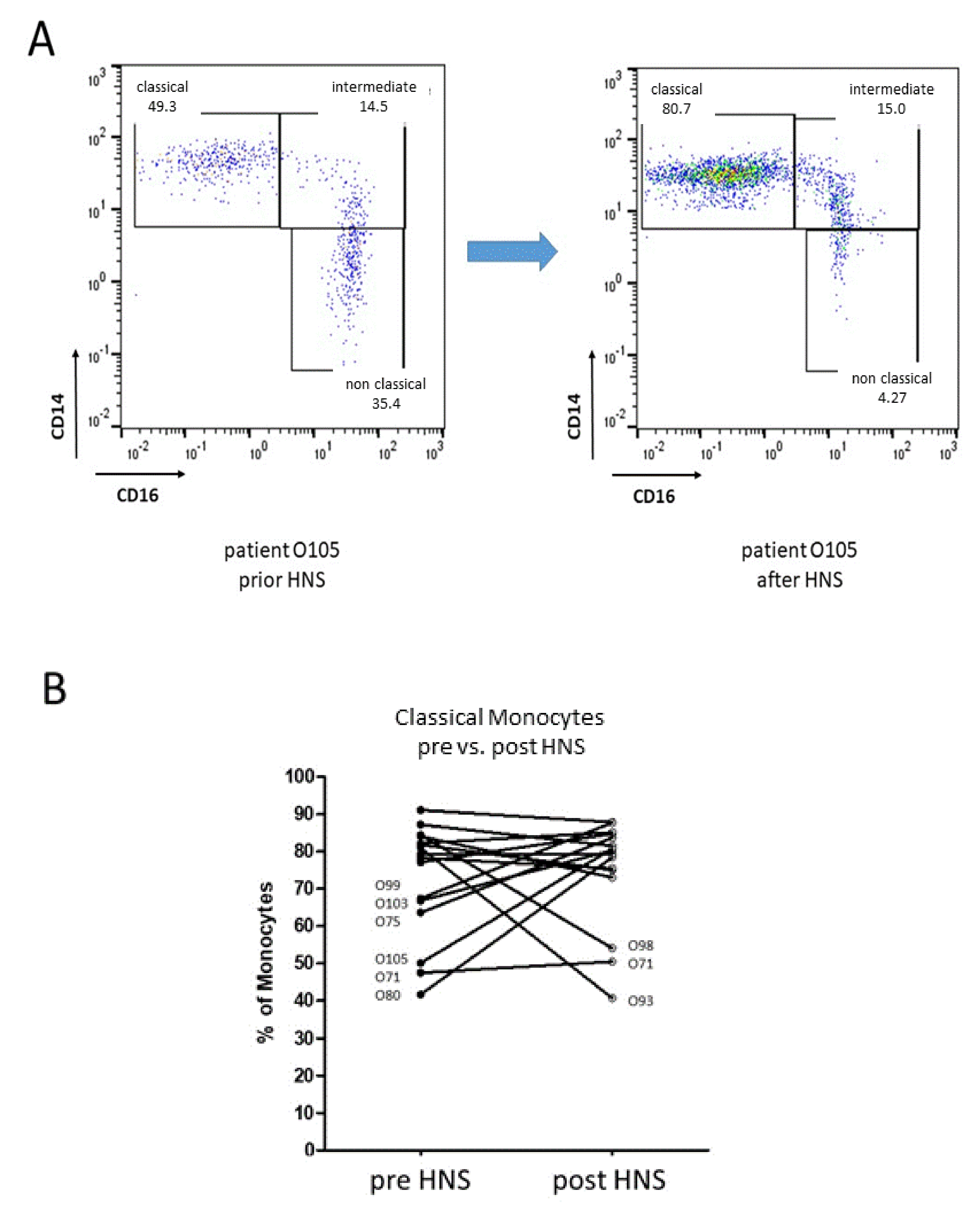
3.2. Monocyte Subset Distribution upon HNS Therapy
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Maniaci, A.; Iannella, G.; Cocuzza, S.; Vicini, C.; Magliulo, G.; Ferlito, S.; Cammaroto, G.; Meccariello, G.; De Vito, A.; Nicolai, A.; et al. Oxidative Stress and Inflammation Biomarker Expression in Obstructive Sleep Apnea Patients. J. Clin. Med. 2021, 10, 277. [Google Scholar] [CrossRef] [PubMed]
- Kapur, V.K.; Auckley, D.H.; Chowdhuri, S.; Kuhlmann, D.C.; Mehra, R.; Ramar, K.; Harrod, C.G. Clinical Practice Guideline for Diagnostic Testing for Adult Obstructive Sleep Apnea: An American Academy of Sleep Medicine Clinical Practice Guideline. J. Clin. Sleep Med. 2017, 13, 479–504. [Google Scholar] [CrossRef] [PubMed]
- McEvoy, R.; Antic, N.; Heeley, E.; Luo, Y.; Ou, Q.; Zhang, X.; Mediano, O.; Chen, R.; Drager, L.; Liu, Z.; et al. CPAP for Prevention of Cardiovascular Events in Obstructive Sleep Apnea. N. Engl. J. Med. 2016, 375, 919–931. [Google Scholar] [CrossRef] [PubMed]
- Aro, M.; Anttalainen, U.; Polo, O.; Saaresranta, T. Mood, sleepiness, and weight gain after three years on CPAP therapy for sleep apnoea. Eur. Clin. Respir. J. 2021, 8, 1888394. [Google Scholar] [CrossRef]
- Huber, F.; Furian, M.; Kohler, M.; Latshang, T.; Nussbaumer-Ochsner, Y.; Turk, A.; Schoch, O.; Laube, I.; Thurnheer, R.; Bloch, K. Health Preference Measures in Patients with Obstructive Sleep Apnea Syndrome Undergoing Continuous Positive Airway Pressure Therapy: Data from a Randomized Trial. Respiration 2021, 100, 328–338. [Google Scholar] [CrossRef]
- Kent, B.; Ryan, S.; McNicholas, W. Obstructive sleep apnea and inflammation: Relationship to cardiovascular co-morbidity. Respir. Physiol. Neurobiol. 2011, 178, 475–481. [Google Scholar] [CrossRef]
- Strollo, P.J., Jr.; Soose, R.J.; Maurer, J.T.; de Vries, N.; Cornelius, J.; Froymovich, O.; Hanson, R.D.; Padhya, T.A.; Steward, D.L.; Gillespie, M.B.; et al. Upper-airway stimulation for obstructive sleep apnea. N. Engl. J. Med. 2014, 370, 139–149. [Google Scholar] [CrossRef] [Green Version]
- Steffen, A.; Heiser, C.; Galetke, W.; Herkenrath, S.D.; Maurer, J.T.; Gunther, E.; Stuck, B.A.; Woehrle, H.; Lohler, J.; Randerath, W. Hypoglossal nerve stimulation for obstructive sleep apnea: Updated position paper of the German Society of Oto-Rhino-Laryngology, Head and Neck Surgery. Eur. Arch. Oto-Rhino-Laryngol. Off. J. Eur. Fed. Oto-Rhino-Laryngol. Soc. 2022, 279, 61–66. [Google Scholar] [CrossRef]
- Ryan, S.; Taylor, C.T.; McNicholas, W.T. Systemic inflammation: A key factor in the pathogenesis of cardiovascular complications in obstructive sleep apnoea syndrome? Thorax 2009, 64, 631–636. [Google Scholar] [CrossRef] [Green Version]
- Kapellos, T.S.; Bonaguro, L.; Gemund, I.; Reusch, N.; Saglam, A.; Hinkley, E.R.; Schultze, J.L. Human Monocyte Subsets and Phenotypes in Major Chronic Inflammatory Diseases. Front. Immunol. 2019, 10, 2035. [Google Scholar] [CrossRef] [Green Version]
- Kurobe, H.; Urata, M.; Ueno, M.; Ueki, M.; Ono, S.; Izawa-Ishizawa, Y.; Fukuhara, Y.; Lei, Y.; Ripen, A.M.; Kanbara, T.; et al. Role of hypoxia-inducible factor 1alpha in T cells as a negative regulator in development of vascular remodeling. Arterioscler. Thromb. Vasc. Biol. 2010, 30, 210–217. [Google Scholar] [CrossRef] [Green Version]
- Cubillos-Zapata, C.; Avendano-Ortiz, J.; Hernandez-Jimenez, E.; Toledano, V.; Casas-Martin, J.; Varela-Serrano, A.; Torres, M.; Almendros, I.; Casitas, R.; Fernandez-Navarro, I.; et al. Hypoxia-induced PD-L1/PD-1 crosstalk impairs T-cell function in sleep apnoea. Eur. Respir. J. 2017, 50, 1700833. [Google Scholar] [CrossRef]
- Domagała-Kulawik, J.; Osińska, I.; Piechuta, A.; Bielicki, P.; Skirecki, T. NKT Cells in Systemic Inflammation in Obstructive Sleep Apnoea. Mediators Inflamm. 2015, 46, PA382. [Google Scholar] [CrossRef]
- Ye, J.; Liu, H.; Zhang, G.; Li, P.; Wang, Z.; Huang, S.; Yang, Q.; Li, Y. The treg/th17 imbalance in patients with obstructive sleep apnoea syndrome. Mediators Inflamm. 2012, 2012, 815308. [Google Scholar] [CrossRef] [Green Version]
- Tamaki, S.; Yamauchi, M.; Fukuoka, A.; Makinodan, K.; Koyama, N.; Tomoda, K.; Yoshikawa, M.; Kimura, H. Production of inflammatory mediators by monocytes in patients with obstructive sleep apnea syndrome. Intern. Med. 2009, 48, 1255–1262. [Google Scholar] [CrossRef] [Green Version]
- Inonu Koseoglu, H.; Pazarli, A.C.; Kanbay, A.; Demir, O. Monocyte Count/HDL Cholesterol Ratio and Cardiovascular Disease in Patients With Obstructive Sleep Apnea Syndrome: A Multicenter Study. Clin. Appl. Thromb./Hemost. 2018, 24, 139–144. [Google Scholar] [CrossRef]
- Zhou, J.; Bai, W.; Liu, Q.; Cui, J.; Zhang, W. Intermittent Hypoxia Enhances THP-1 Monocyte Adhesion and Chemotaxis and Promotes M1 Macrophage Polarization via RAGE. BioMed Res. Int. 2018, 2018, 1650456. [Google Scholar] [CrossRef]
- Polasky, C.; Steffen, A.; Loyal, K.; Lange, C.; Bruchhage, K.; Pries, R. Redistribution of Monocyte Subsets in Obstructive Sleep Apnea Syndrome Patients Leads to an Imbalanced PD-1/PD-L1 Cross-Talk with CD4/CD8 T Cells. J. Immunol. 2021, 206, 51–58. [Google Scholar] [CrossRef]
- Auffray, C.; Fogg, D.; Garfa, M.; Elain, G.; Join-Lambert, O.; Kayal, S.; Sarnacki, S.; Cumano, A.; Lauvau, G.; Geissmann, F. Monitoring of blood vessels and tissues by a population of monocytes with patrolling behavior. Science 2007, 317, 666–670. [Google Scholar] [CrossRef] [Green Version]
- Wong, K.L.; Yeap, W.H.; Tai, J.J.; Ong, S.M.; Dang, T.M.; Wong, S.C. The three human monocyte subsets: Implications for health and disease. Immunol. Res. 2012, 53, 41–57. [Google Scholar] [CrossRef]
- Patel, A.A.; Zhang, Y.; Fullerton, J.N.; Boelen, L.; Rongvaux, A.; Maini, A.A.; Bigley, V.; Flavell, R.A.; Gilroy, D.W.; Asquith, B.; et al. The fate and lifespan of human monocyte subsets in steady state and systemic inflammation. J. Exp. Med. 2017, 214, 1913–1923. [Google Scholar] [CrossRef]
- Ziegler-Heitbrock, L. Blood Monocytes and Their Subsets: Established Features and Open Questions. Front. Immunol. 2015, 6, 423. [Google Scholar] [CrossRef]
- Boyette, L.B.; Macedo, C.; Hadi, K.; Elinoff, B.D.; Walters, J.T.; Ramaswami, B.; Chalasani, G.; Taboas, J.M.; Lakkis, F.G.; Metes, D.M. Phenotype, function, and differentiation potential of human monocyte subsets. PLoS ONE 2017, 12, 0176460. [Google Scholar] [CrossRef] [PubMed]
- Jakubzick, C.V.; Randolph, G.J.; Henson, P.M. Monocyte differentiation and antigen-presenting functions. Nat. Rev. Immunol. 2017, 17, 349–362. [Google Scholar] [CrossRef] [PubMed]
- Polasky, C.; Steffen, A.; Loyal, K.; Lange, C.; Bruchhage, K.L.; Pries, R. Reconstitution of Monocyte Subsets and PD-L1 Expression but Not T Cell PD-1 Expression in Obstructive Sleep Apnea Patients upon PAP Therapy. Int. J. Mol. Sci. 2021, 22, 11375. [Google Scholar] [CrossRef] [PubMed]
- Moniuszko, M.; Bodzenta-Lukaszyk, A.; Kowal, K.; Lenczewska, D.; Dabrowska, M. Enhanced frequencies of CD14++CD16+, but not CD14+CD16+, peripheral blood monocytes in severe asthmatic patients. Clin. Immunol. 2009, 130, 338–346. [Google Scholar] [CrossRef]
- Chen, Y.H.; Wu, M.F.; Wen, C.Y.; Chang, S.P.; Lin, C.Y.; Chen, Y.C.; Lin, C.C.; Chen, H.C.; Huang, W.C.; Chang, K.M. Interactions between Obstructive Sleep Apnea Syndrome Severity, Obesity, Sex Difference and Attention-Deficit/Hyperactivity Disorder on Health-Related Quality of Life: A Non-Interventional Prospective Observational Study. Biomedicines 2022, 10, 1576. [Google Scholar] [CrossRef]
- Lee, S.; Song, P.; Choi, S.; Suh, S.; Kwon, S.; Joo, E. The impact of the shift system on health and quality of life of sleep technicians. Sleep Med. 2020, 76, 72–79. [Google Scholar] [CrossRef]
- Israel, L.P.; Benharoch, D.; Gopas, J.; Goldbart, A.D. A pro-inflammatory role of nuclear factor kappa B in childhood obstructive sleep apnea syndrome. Sleep 2013, 36, 1947–1955. [Google Scholar] [CrossRef] [Green Version]
- Almendros, I.; Martinez-Garcia, M.A.; Farre, R.; Gozal, D. Obesity, sleep apnea, and cancer. Int. J. Obes. 2020, 44, 1653–1667. [Google Scholar] [CrossRef]
- Jin, F.; Liu, J.; Zhang, X.; Cai, W.; Zhang, Y.; Zhang, W.; Yang, J.; Lu, G.; Zhang, X. Effect of continuous positive airway pressure therapy on inflammatory cytokines and atherosclerosis in patients with obstructive sleep apnea syndrome. Mol. Med. Rep. 2017, 16, 6334–6339. [Google Scholar] [CrossRef]
- Steiropoulos, P.; Kotsianidis, I.; Nena, E.; Tsara, V.; Gounari, E.; Hatzizisi, O.; Kyriazis, G.; Christaki, P.; Froudarakis, M.; Bouros, D. Long-term effect of continuous positive airway pressure therapy on inflammation markers of patients with obstructive sleep apnea syndrome. Sleep 2009, 32, 537–543. [Google Scholar] [CrossRef]
- Bouloukaki, I.; Mermigkis, C.; Kallergis, E.; Moniaki, V.; Mauroudi, E.; Schiza, S. Obstructive sleep apnea syndrome and cardiovascular disease: The influence of C-reactive protein. World J. Exp. Med. 2015, 5, 77–83. [Google Scholar] [CrossRef]
- Ryan, S.; Arnaud, C.; Fitzpatrick, S.F.; Gaucher, J.; Tamisier, R.; Pepin, J.L. Adipose tissue as a key player in obstructive sleep apnoea. Eur. Respir. Rev. 2019, 28, 190006. [Google Scholar] [CrossRef]
- Jordan, A.S.; McSharry, D.G.; Malhotra, A. Adult obstructive sleep apnoea. Lancet 2014, 383, 736–747. [Google Scholar] [CrossRef] [Green Version]
- Ng, S.; Liu, E.; Ma, R.; Chan, T.; To, K.; Chan, K.; Ngai, J.; Yip, W.; Ko, F.; Wong, C.; et al. Effects of CPAP therapy on visceral fat thickness, carotid intima-media thickness and adipokines in patients with obstructive sleep apnoea. Respirology 2017, 22, 786–792. [Google Scholar] [CrossRef]
- Suurna, M.V.; Jacobowitz, O.; Chang, J.; Koutsourelakis, I.; Smith, D.; Alkan, U.; D’Agostino, M.; Boon, M.; Heiser, C.; Hoff, P.; et al. Improving outcomes of hypoglossal nerve stimulation therapy: Current practice, future directions, and research gaps. J. Clin. Sleep Med. 2021, 17, 2477–2487. [Google Scholar] [CrossRef]
- Suurna, M.V.; Steffen, A.; Boon, M.; Chio, E.; Copper, M.; Patil, R.D.; Green, K.; Hanson, R.; Heiser, C.; Huntley, C.; et al. Impact of Body Mass Index and Discomfort on Upper Airway Stimulation: ADHERE Registry 2020 Update. Laryngoscope 2021, 131, 2616–2624. [Google Scholar] [CrossRef]
- Paoloni, V.; Cretella Lombardo, E.; Placidi, F.; Ruvolo, G.; Cozza, P.; Lagana, G. Obstructive sleep apnea in children with Marfan syndrome: Relationships between three-dimensional palatal morphology and apnea-hypopnea index. Int. J. Pediatric Otorhinolaryngol. 2018, 112, 6–9. [Google Scholar] [CrossRef]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pries, R.; Lange, C.; Behn, N.; Bruchhage, K.-L.; Steffen, A. Dynamics of Circulating CD14/CD16 Monocyte Subsets in Obstructive Sleep Apnea Syndrome Patients upon Hypoglossal Nerve Stimulation. Biomedicines 2022, 10, 1925. https://doi.org/10.3390/biomedicines10081925
Pries R, Lange C, Behn N, Bruchhage K-L, Steffen A. Dynamics of Circulating CD14/CD16 Monocyte Subsets in Obstructive Sleep Apnea Syndrome Patients upon Hypoglossal Nerve Stimulation. Biomedicines. 2022; 10(8):1925. https://doi.org/10.3390/biomedicines10081925
Chicago/Turabian StylePries, Ralph, Christian Lange, Nicole Behn, Karl-Ludwig Bruchhage, and Armin Steffen. 2022. "Dynamics of Circulating CD14/CD16 Monocyte Subsets in Obstructive Sleep Apnea Syndrome Patients upon Hypoglossal Nerve Stimulation" Biomedicines 10, no. 8: 1925. https://doi.org/10.3390/biomedicines10081925
APA StylePries, R., Lange, C., Behn, N., Bruchhage, K.-L., & Steffen, A. (2022). Dynamics of Circulating CD14/CD16 Monocyte Subsets in Obstructive Sleep Apnea Syndrome Patients upon Hypoglossal Nerve Stimulation. Biomedicines, 10(8), 1925. https://doi.org/10.3390/biomedicines10081925