
Chronic Kidney Disease in Boys with Posterior Urethral Valves–Pathogenesis, Prognosis and Management


Abstract
:1. Introduction
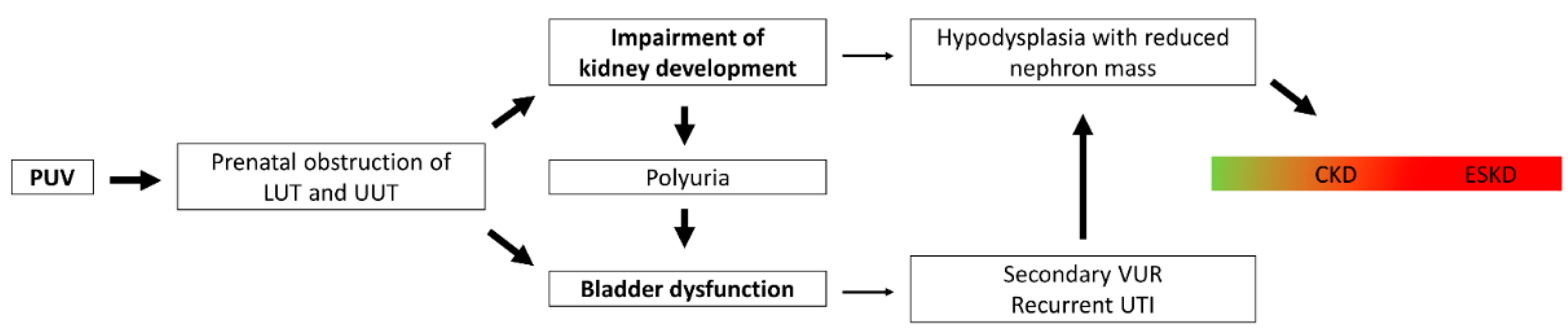
2. Pathophysiology of Chronic Kidney Disease in Posterior Urethral Valves
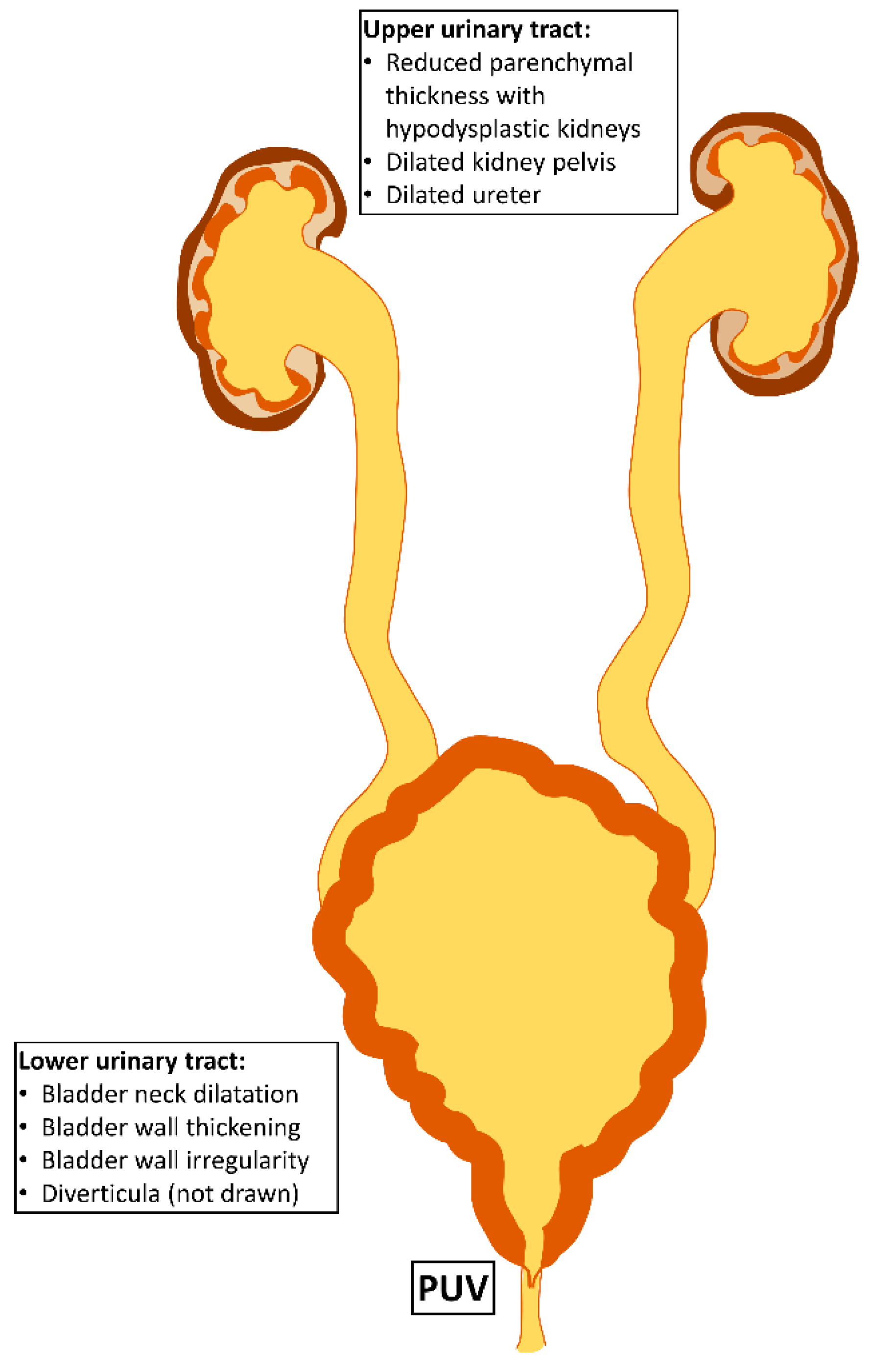
2.1. Intrauterine Obstruction Impairs Kidney Development
2.2. Bladder Dysfunction Results from Muscular Hypertrophy and Fibrotic Remodelling
2.3. Genetic Causes of Posterior Urethral Valves
3. Epidemiology of Chronic Kidney Disease in Posterior Urethral Valves
4. Prognostic Factors for Chronic Kidney Disease Development
4.1. Prenatal Prognostic Factors
4.2. Postnatal Prognostic Factors
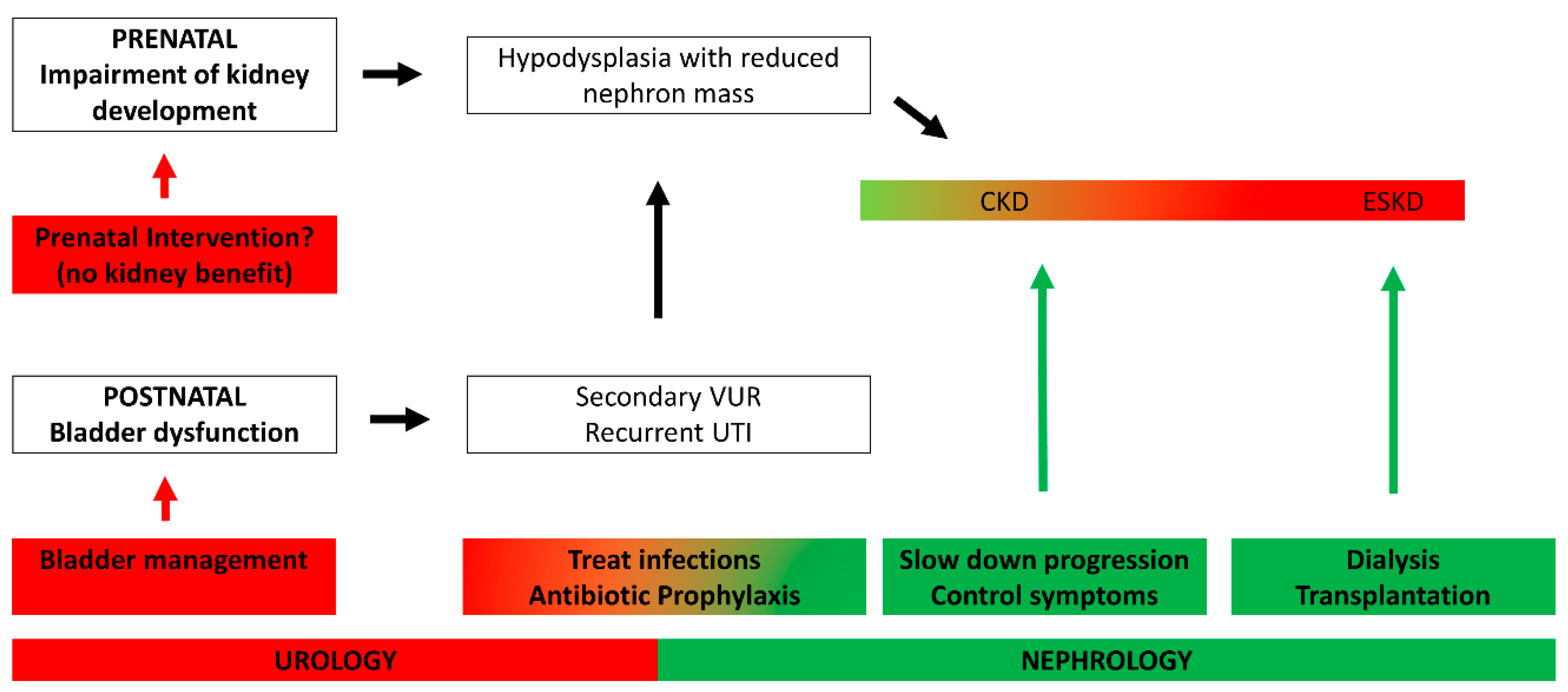
5. Management of Chronic Kidney Disease in Posterior Urethral Valves
5.1. Prenatal Intervention Does Not Prevent CKD
5.2. Optimal Bladder Control Leads to Improved Graft Survival in Kidney Transplantation
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| AI | artificial intelligence |
| CAKUT | congenital anomalies of the kidneys and urinary tract |
| CKD | chronic kidney disease |
| ESRD | end-stage renal disease |
| LUTO | lower urinary tract obstruction |
| ML | machine learning |
| PUV | posterior urethral valves |
| RRT | renal replacement therapy |
| TUI | transurethral incision |
| UTI | urinary tract infection |
| UUO | unilateral ureteral obstruction |
| VAS | vesicoamniotic shunt |
References
- Warady, B.A.; Chadha, V. Chronic kidney disease in children: The global perspective. Pediatr. Nephrol. 2007, 22, 1999–2009. [Google Scholar] [CrossRef] [PubMed]
- Ardissino, G.; Dacco, V.; Testa, S.; Bonaudo, R.; Claris-Appiani, A.; Taioli, E.; Marra, G.; Edefonti, A.; Sereni, F.; ItalKid, P. Epidemiology of chronic renal failure in children: Data from the ItalKid project. Pediatrics 2003, 111, e382–e387. [Google Scholar] [CrossRef] [PubMed]
- Lange-Sperandio, B.; Rosenblum, N.D. Book chapter: Pediatric obstructive uropathy. In Pediatric Nephrology, 8th ed.; Emma, F., Goldstein, S., Bagga, A., Bates, C.M., Shroff, R., Eds.; Springer: New York, NY, USA, 2022. [Google Scholar]
- Malin, G.; Tonks, A.M.; Morris, R.K.; Gardosi, J.; Kilby, M.D. Congenital lower urinary tract obstruction: A population-based epidemiological study. BJOG 2012, 119, 1455–1464. [Google Scholar] [CrossRef] [PubMed]
- Herbst, K.W.; Tomlinson, P.; Lockwood, G.; Mosha, M.H.; Wang, Z.; D’Alessandri-Silva, C. Survival and Kidney Outcomes of Children with an Early Diagnosis of Posterior Urethral Valves. Clin. J. Am. Soc. Nephrol 2019, 14, 1572–1580. [Google Scholar] [CrossRef] [PubMed]
- Brownlee, E.; Wragg, R.; Robb, A.; Chandran, H.; Knight, M.; McCarthy, L.; Baps, C. Current epidemiology and antenatal presentation of posterior urethral valves: Outcome of BAPS CASS National Audit. J. Pediatr. Surg. 2019, 54, 318–321. [Google Scholar] [CrossRef]
- Parkhouse, H.F.; Barratt, T.M.; Dillon, M.J.; Duffy, P.G.; Fay, J.; Ransley, P.G.; Woodhouse, C.R.; Williams, D.I. Long-term outcome of boys with posterior urethral valves. Br. J. Urol. 1988, 62, 59–62. [Google Scholar] [CrossRef] [PubMed]
- Maranya, G.A. Posterior urethral valves in the adult: Report of two cases. East. Afr. Med. J. 2004, 81, 430–432. [Google Scholar] [CrossRef]
- Jank, M.; Stein, R.; Younsi, N. Postnatal Management in Congenital Lower Urinary Tract Obstruction With and Without Prenatal Vesicoamniotic Shunt. Front. Pediatr. 2021, 9, 635950. [Google Scholar] [CrossRef]
- Song, R.; Yosypiv, I.V. Genetics of congenital anomalies of the kidney and urinary tract. Pediatr. Nephrol. 2011, 26, 353–364. [Google Scholar] [CrossRef]
- Kandasamy, Y.; Smith, R.; Wright, I.M. Oligonephropathy of prematurity. Am. J. Perinatol. 2012, 29, 115–120. [Google Scholar] [CrossRef]
- Rodriguez, M.M.; Gomez, A.H.; Abitbol, C.L.; Chandar, J.J.; Duara, S.; Zilleruelo, G.E. Histomorphometric analysis of postnatal glomerulogenesis in extremely preterm infants. Pediatr. Dev. Pathol. 2004, 7, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Bertram, J.F.; Douglas-Denton, R.N.; Diouf, B.; Hughson, M.D.; Hoy, W.E. Human nephron number: Implications for health and disease. Pediatr. Nephrol. 2011, 26, 1529–1533. [Google Scholar] [CrossRef]
- Abitbol, C.L.; DeFreitas, M.J.; Strauss, J. Assessment of kidney function in preterm infants: Lifelong implications. Pediatr. Nephrol. 2016, 31, 2213–2222. [Google Scholar] [CrossRef] [PubMed]
- Luyckx, V.A. Preterm Birth and its Impact on Renal Health. Semin. Nephrol. 2017, 37, 311–319. [Google Scholar] [CrossRef]
- Iacobelli, S.; Guignard, J.P. When the progresses in neonatology lead to severe congenital nephron deficit: Is there a pilot in the NICU? Pediatr. Nephrol. 2022, 37, 1277–1284. [Google Scholar] [CrossRef] [PubMed]
- Chevalier, R.L. Congenital urinary tract obstruction: The long view. Adv. Chronic. Kidney Dis. 2015, 22, 312–319. [Google Scholar] [CrossRef]
- Jackson, L.; Woodward, M.; Coward, R.J. The molecular biology of pelvi-ureteric junction obstruction. Pediatr. Nephrol. 2018, 33, 553–571. [Google Scholar] [CrossRef] [PubMed]
- Wyczanska, M.; Lange-Sperandio, B. DAMPs in Unilateral Ureteral Obstruction. Front. Immunol. 2020, 11, 588245. [Google Scholar] [CrossRef]
- Popper, B.; Rammer, M.T.; Gasparitsch, M.; Singer, T.; Keller, U.; Doring, Y.; Lange-Sperandio, B. Neonatal obstructive nephropathy induces necroptosis and necroinflammation. Sci. Rep. 2019, 9, 18600. [Google Scholar] [CrossRef]
- Hennus, P.M.; van der Heijden, G.J.; Bosch, J.L.; de Jong, T.P.; de Kort, L.M. A systematic review on renal and bladder dysfunction after endoscopic treatment of infravesical obstruction in boys. PLoS ONE 2012, 7, e44663. [Google Scholar] [CrossRef] [PubMed]
- Thomas, J. Etiopathogenesis and management of bladder dysfunction in patients with posterior urethral valves. Indian J. Urol. 2010, 26, 480–489. [Google Scholar] [CrossRef] [PubMed]
- Cao, K.X.; Milmoe, N.J.; Cuckow, P.M.; Olsen, L.H.; Johal, N.S.; Douglas Winyard, P.J.; Long, D.A.; Fry, C.H. Antenatal biological models in the characterization and research of congenital lower urinary tract disorders. J. Pediatr. Urol. 2021, 17, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Workman, S.J.; Kogan, B.A. Fetal bladder histology in posterior urethral valves and the prune belly syndrome. J. Urol. 1990, 144, 337–339. [Google Scholar] [CrossRef]
- Freedman, A.L.; Qureshi, F.; Shapiro, E.; Lepor, H.; Jacques, S.M.; Evans, M.I.; Smith, C.A.; Gonzalez, R.; Johnson, M.P. Smooth muscle development in the obstructed fetal bladder. Urology 1997, 49, 104–107. [Google Scholar] [CrossRef]
- Johal, N.; Cao, K.; Arthurs, C.; Millar, M.; Thrasivoulou, C.; Ahmed, A.; Jabr, R.I.; Wood, D.; Cuckow, P.; Fry, C.H. Contractile function of detrusor smooth muscle from children with posterior urethral valves-The role of fibrosis. J. Pediatr. Urol. 2021, 17, 100.e1–100.e10. [Google Scholar] [CrossRef]
- Dinneen, M.D.; Duffy, P.G.; Barratt, T.M.; Ransley, P.G. Persistent polyuria after posterior urethral valves. Br. J. Urol. 1995, 75, 236–240. [Google Scholar] [CrossRef]
- Kolvenbach, C.M.; Dworschak, G.C.; Frese, S.; Japp, A.S.; Schuster, P.; Wenzlitschke, N.; Yilmaz, O.; Lopes, F.M.; Pryalukhin, A.; Schierbaum, L.; et al. Rare Variants in BNC2 Are Implicated in Autosomal-Dominant Congenital Lower Urinary-Tract Obstruction. Am. J. Hum. Genet. 2019, 104, 994–1006. [Google Scholar] [CrossRef]
- McLeod, D.J.; Szymanski, K.M.; Gong, E.; Granberg, C.; Reddy, P.; Sebastiao, Y.; Fuchs, M.; Gargollo, P.; Whittam, B.; VanderBrink, B.A.; et al. Renal Replacement Therapy and Intermittent Catheterization Risk in Posterior Urethral Valves. Pediatrics 2019, 143. [Google Scholar] [CrossRef]
- Coquillette, M.; Lee, R.S.; Pagni, S.E.; Cataltepe, S.; Stein, D.R. Renal outcomes of neonates with early presentation of posterior urethral valves: A 10-year single center experience. J. Perinatol. 2020, 40, 112–117. [Google Scholar] [CrossRef]
- Weaver, D.J., Jr.; Somers, M.J.G.; Martz, K.; Mitsnefes, M.M. Clinical outcomes and survival in pediatric patients initiating chronic dialysis: A report of the NAPRTCS registry. Pediatr. Nephrol. 2017, 32, 2319–2330. [Google Scholar] [CrossRef]
- Sarhan, O.M.; Helmy, T.E.; Alotay, A.A.; Alghanbar, M.S.; Nakshabandi, Z.M.; Hafez, A.T. Did antenatal diagnosis protect against chronic kidney disease in patients with posterior urethral valves? A multicenter study. Urology 2013, 82, 1405–1409. [Google Scholar] [CrossRef] [PubMed]
- Vasconcelos, M.A.; Simoes, E.S.A.C.; Dias, C.S.; Gomes, I.R.; Carvalho, R.A.; Figueiredo, S.V.; Dumont, T.R.; Oliveira, M.C.L.; Pinheiro, S.V.; Mak, R.H.; et al. Posterior urethral valves: Comparison of clinical outcomes between postnatal and antenatal cohorts. J. Pediatr. Urol. 2019, 15, 167.e1–167.e8. [Google Scholar] [CrossRef] [PubMed]
- Yadav, P.; Rickard, M.; Weaver, J.; Chua, M.; Kim, J.K.; Khondker, A.; Milford, K.; Keefe, D.T.; Lolas, M.; Dos Santos, J.; et al. Pre-versus postnatal presentation of posterior urethral valves: A multi-institutional experience. BJU Int. 2022. [Google Scholar] [CrossRef] [PubMed]
- Moscardi, P.R.M.; Katsoufis, C.P.; Jahromi, M.; Blachman-Braun, R.; DeFreitas, M.J.; Kozakowski, K.; Castellan, M.; Labbie, A.; Gosalbez, R.; Alam, A. Prenatal renal parenchymal area as a predictor of early end-stage renal disease in children with vesicoamniotic shunting for lower urinary tract obstruction. J. Pediatr. Urol. 2018, 14, 320.e1–320.e6. [Google Scholar] [CrossRef] [PubMed]
- Matsell, D.G.; Yu, S.; Morrison, S.J. Antenatal Determinants of Long-Term Kidney Outcome in Boys with Posterior Urethral Valves. Fetal Diagn. Ther. 2016, 39, 214–221. [Google Scholar] [CrossRef]
- Fontanella, F.; van Scheltema, P.N.A.; Duin, L.; Cohen-Overbeek, T.E.; Pajkrt, E.; Bekker, M.N.; Willekes, C.; Oepkes, D.; Bilardo, C.M. Antenatal staging of congenital lower urinary tract obstruction. Ultrasound Obstet. Gynecol. 2019, 53, 520–524. [Google Scholar] [CrossRef]
- Ruano, R.; Sananes, N.; Wilson, C.; Au, J.; Koh, C.J.; Gargollo, P.; Shamshirsaz, A.A.; Espinoza, J.; Safdar, A.; Moaddab, A.; et al. Fetal lower urinary tract obstruction: Proposal for standardized multidisciplinary prenatal management based on disease severity. Ultrasound Obstet. Gynecol. 2016, 48, 476–482. [Google Scholar] [CrossRef]
- Dreux, S.; Rosenblatt, J.; Moussy-Durandy, A.; Patin, F.; Favre, R.; Lortat-Jacob, S.; El Ghoneimi, A.; Oury, J.F.; Deschenes, G.; Ville, Y.; et al. Urine biochemistry to predict long-term outcomes in fetuses with posterior urethral valves. Prenat Diagn. 2018, 38, 964–970. [Google Scholar] [CrossRef]
- Fedou, C.; Breuil, B.; Golovko, I.; Decramer, S.; Magalhaes, P.; Muller, F.; Dreux, S.; Zurbig, P.; Klein, J.; Schanstra, J.P.; et al. Comparison of the amniotic fluid and fetal urine peptidome for biomarker discovery in renal developmental disease. Sci. Rep. 2020, 10, 21706. [Google Scholar] [CrossRef]
- Klein, J.; Lacroix, C.; Caubet, C.; Siwy, J.; Zurbig, P.; Dakna, M.; Muller, F.; Breuil, B.; Stalmach, A.; Mullen, W.; et al. Fetal urinary peptides to predict postnatal outcome of renal disease in fetuses with posterior urethral valves (PUV). Sci. Transl. Med. 2013, 5, 198ra106. [Google Scholar] [CrossRef]
- Buffin-Meyer, B.; Tkaczyk, M.; Stanczyk, M.; Breuil, B.; Siwy, J.; Szaflik, K.; Talar, T.; Wojtera, J.; Krzeszowski, W.; Decramer, S.; et al. A single-center study to evaluate the efficacy of a fetal urine peptide signature predicting postnatal renal outcome in fetuses with posterior urethral valves. Pediatr. Nephrol. 2020, 35, 469–475. [Google Scholar] [CrossRef] [PubMed]
- Buffin-Meyer, B.; Klein, J.; van der Zanden, L.F.M.; Levtchenko, E.; Moulos, P.; Lounis, N.; Conte-Auriol, F.; Hindryckx, A.; Wuhl, E.; Persico, N.; et al. The ANTENATAL multicentre study to predict postnatal renal outcome in fetuses with posterior urethral valves: Objectives and design. Clin. Kidney J. 2020, 13, 371–379. [Google Scholar] [CrossRef] [PubMed]
- Bajpai, M.; Singh, A. Plasma renin activity: An early marker of progressive renal disease in posterior urethral valves. J. Indian Assoc. Pediatr. Surg. 2013, 18, 143–146. [Google Scholar] [CrossRef]
- Bajpai, M.; Pratap, A.; Tripathi, M.; Bal, C.S. Posterior urethral valves: Preliminary observations on the significance of plasma Renin activity as a prognostic marker. J. Urol. 2005, 173, 592–594. [Google Scholar] [CrossRef] [PubMed]
- Demirkan, H.; Yesildal, C. Serum creatinine levels in cases of posterior urethral valve: 29 years experience of a pediatric urology reference center. Low Urin. Tract Symptoms 2020, 12, 274–277. [Google Scholar] [CrossRef] [PubMed]
- Pohl, M.; Mentzel, H.J.; Vogt, S.; Walther, M.; Ronnefarth, G.; John, U. Risk factors for renal insufficiency in children with urethral valves. Pediatr. Nephrol. 2012, 27, 443–450. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.Q.; Blum, E.S.; Patil, D.; Shin, H.S.; Smith, E.A. Predicting childhood chronic kidney disease severity in infants with posterior urethral valve: A critical analysis of creatinine values in the first year of life. Pediatr. Nephrol. 2021, 37, 1339–1345. [Google Scholar] [CrossRef]
- Sarhan, O.M.; El-Ghoneimi, A.A.; Helmy, T.E.; Dawaba, M.S.; Ghali, A.M.; Ibrahiem el, H.I. Posterior urethral valves: Multivariate analysis of factors affecting the final renal outcome. J. Urol. 2011, 185, 2491–2495. [Google Scholar] [CrossRef]
- Coleman, R.; King, T.; Nicoara, C.D.; Bader, M.; McCarthy, L.; Chandran, H.; Parashar, K. Nadir creatinine in posterior urethral valves: How high is low enough? J. Pediatr Urol 2015, 11, 356.e1–356.e5. [Google Scholar] [CrossRef]
- Coleman, R.; King, T.; Nicoara, C.D.; Bader, M.; McCarthy, L.; Chandran, H.; Parashar, K. Combined creatinine velocity and nadir creatinine: A reliable predictor of renal outcome in neonatally diagnosed posterior urethral valves. J. Pediatr. Urol. 2015, 11, 214.e1–214.e3. [Google Scholar] [CrossRef]
- Ansari, M.S.; Gulia, A.; Srivastava, A.; Kapoor, R. Risk factors for progression to end-stage renal disease in children with posterior urethral valves. J. Pediatr. Urol. 2010, 6, 261–264. [Google Scholar] [CrossRef] [PubMed]
- Sarhan, O.; El-Dahshan, K.; Sarhan, M. Prognostic value of serum creatinine levels in children with posterior urethral valves treated by primary valve ablation. J. Pediatr. Urol. 2010, 6, 11–14. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, A.V.; Alsaywid, B.S.; Smith, G.H. Setting the speed limit: A pilot study of the rate of serum creatinine decrease after endoscopic valve ablation in neonates. J. Urol. 2011, 185, 2497–2500. [Google Scholar] [CrossRef] [PubMed]
- Warshaw, B.L.; Hymes, L.C.; Trulock, T.S.; Woodard, J.R. Prognostic features in infants with obstructive uropathy due to posterior urethral valves. J. Urol. 1985, 133, 240–243. [Google Scholar] [CrossRef]
- Vasconcelos, M.A.; ACS, E.S.; Gomes, I.R.; Carvalho, R.A.; Pinheiro, S.V.; Colosimo, E.A.; Yorgin, P.; Mak, R.H.; Oliveira, E.A. A clinical predictive model of chronic kidney disease in children with posterior urethral valves. Pediatr. Nephrol. 2019, 34, 283–294. [Google Scholar] [CrossRef]
- DeFoor, W.; Clark, C.; Jackson, E.; Reddy, P.; Minevich, E.; Sheldon, C. Risk factors for end stage renal disease in children with posterior urethral valves. J. Urol. 2008, 180, 1705–1708, discussion 1708. [Google Scholar] [CrossRef]
- Lopez Pereira, P.; Martinez Urrutia, M.J.; Espinosa, L.; Lobato, R.; Navarro, M.; Jaureguizar, E. Bladder dysfunction as a prognostic factor in patients with posterior urethral valves. BJU Int. 2002, 90, 308–311. [Google Scholar] [CrossRef]
- Delefortrie, T.; Ferdynus, C.; Paye-Jaouen, A.; Peycelon, M.; Michel, J.L.; Dobremez, E.; El Ghoneimi, A.; Harper, L. Nadir creatinine predicts long-term bladder function in boys with posterior urethral valves. J. Pediatr. Urol. 2022, 18, 186.e1–186.e4. [Google Scholar] [CrossRef]
- Heikkila, J.; Holmberg, C.; Kyllonen, L.; Rintala, R.; Taskinen, S. Long-term risk of end stage renal disease in patients with posterior urethral valves. J. Urol. 2011, 186, 2392–2396. [Google Scholar] [CrossRef]
- Kumar, N.; Yadav, P.; Jain, S.; Kumar, G.A.; Kaushik, V.N.; Ansari, M.S. Evaluation of polyuria and polydipsia along with other established prognostic factors in posterior urethral valves for progression to kidney failure: Experience from a developing country. Pediatr. Nephrol. 2021, 36, 1817–1824. [Google Scholar] [CrossRef]
- Ezel Celakil, M.; Ekinci, Z.; Bozkaya Yucel, B.; Mutlu, N.; Gunlemez, A.; Bek, K. Outcome of posterior urethral valve in 64 children: A single center’s 22-year experience. Minerva Urol. Nefrol. 2019, 71, 651–656. [Google Scholar] [CrossRef] [PubMed]
- Harper, L.; Blanc, T.; Peycelon, M.; Michel, J.L.; Leclair, M.D.; Garnier, S.; Flaum, V.; Arnaud, A.P.; Merrot, T.; Dobremez, E.; et al. Circumcision and Risk of Febrile Urinary Tract Infection in Boys with Posterior Urethral Valves: Result of the CIRCUP Randomized Trial. Eur. Urol. 2022, 81, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Amesty, M.V.; Garcia-Vaz, C.; Espinosa, L.; Martinez-Urrutia, M.J.; Lopez-Pereira, P. Long-Term Renal Transplant Outcome in Patients With Posterior Urethral Valves. Prognostic Factors Related to Bladder Dysfunction Management. Front. Pediatr. 2021, 9, 646923. [Google Scholar] [CrossRef] [PubMed]
- Marchal, S.; Kalfa, N.; Iborra, F.; Badet, L.; Karam, G.; Broudeur, L.; Branchereau, J.; Abdo, N.; Thuret, R. Long-term Outcome of Renal Transplantation in Patients with Congenital Lower Urinary Tract Malformations: A Multicenter Study. Transplantation 2020, 104, 165–171. [Google Scholar] [CrossRef]
- Assefa, H.G.; Getachew, H.; Tadesse, A.; Kiflu, W.; Temesgen, F.; Dejene, B.; Mammo, T.N. Outcome of PUV Patients Following Ablation in a Tertiary Teaching Hospital in Addis Ababa, Ethiopia. Res. Rep. Urol. 2021, 13, 639–645. [Google Scholar] [CrossRef]
- Kostic, D.; Dos Santos Beozzo, G.P.N.; do Couto, S.B.; Kato, A.H.T.; Lima, L.; Palmeira, P.; Krebs, V.L.J.; Bunduki, V.; Francisco, R.P.V.; Zugaib, M.; et al. First-year profile of biomarkers for early detection of renal injury in infants with congenital urinary tract obstruction. Pediatr. Nephrol. 2019, 34, 1117–1128. [Google Scholar] [CrossRef]
- Trnka, P.; Ivanova, L.; Hiatt, M.J.; Matsell, D.G. Urinary biomarkers in obstructive nephropathy. Clin. J. Am. Soc. Nephrol. 2012, 7, 1567–1575. [Google Scholar] [CrossRef]
- Panigrahi, P.; Chowdhary, S.; Sharma, S.P.; Kumar, R.; Agarwal, N.; Sharma, S.P. Role of Urinary Transforming Growth Factor Beta-B1 and Monocyte Chemotactic Protein-1 as Prognostic Biomarkers in Posterior Urethral Valve. J. Indian Assoc. Pediatr. Surg. 2020, 25, 219–224. [Google Scholar] [CrossRef]
- Barbour, S.J.; Coppo, R.; Zhang, H.; Liu, Z.H.; Suzuki, Y.; Matsuzaki, K.; Katafuchi, R.; Er, L.; Espino-Hernandez, G.; Kim, S.J.; et al. Evaluating a New International Risk-Prediction Tool in IgA Nephropathy. JAMA Intern. Med. 2019, 179, 942–952. [Google Scholar] [CrossRef]
- Rovin, B.H.; Adler, S.G.; Barratt, J.; Bridoux, F.; Burdge, K.A.; Chan, T.M.; Floege, J. KDIGO 2021 Clinical Practice Guideline for the Management of Glomerular Diseases. Kidney Int. 2021, 100, S1–S276. [Google Scholar] [CrossRef]
- Barbour, S.J.; Coppo, R.; Er, L.; Russo, M.L.; Liu, Z.H.; Ding, J.; Katafuchi, R.; Yoshikawa, N.; Xu, H.; Kagami, S.; et al. Updating the International IgA Nephropathy Prediction Tool for use in children. Kidney Int. 2021, 99, 1439–1450. [Google Scholar] [CrossRef] [PubMed]
- Abdovic, S.; Cuk, M.; Cekada, N.; Milosevic, M.; Geljic, A.; Fusic, S.; Bastic, M.; Bahtijarevic, Z. Predicting posterior urethral obstruction in boys with lower urinary tract symptoms using deep artificial neural network. World J. Urol. 2019, 37, 1973–1979. [Google Scholar] [CrossRef] [PubMed]
- Bertsimas, D.; Li, M.; Estrada, C.; Nelson, C.; Scott Wang, H.H. Selecting Children with Vesicoureteral Reflux Who are Most Likely to Benefit from Antibiotic Prophylaxis: Application of Machine Learning to RIVUR. J. Urol. 2021, 205, 1170–1179. [Google Scholar] [CrossRef] [PubMed]
- Lorenzo, A.J.; Rickard, M.; Braga, L.H.; Guo, Y.; Oliveria, J.P. Predictive Analytics and Modeling Employing Machine Learning Technology: The Next Step in Data Sharing, Analysis, and Individualized Counseling Explored With a Large, Prospective Prenatal Hydronephrosis Database. Urology 2019, 123, 204–209. [Google Scholar] [CrossRef]
- Kwong, J.C.; Khondker, A.; Kim, J.K.; Chua, M.; Keefe, D.T.; Dos Santos, J.; Skreta, M.; Erdman, L.; D’Souza, N.; Selman, A.F.; et al. Posterior Urethral Valves Outcomes Prediction (PUVOP): A machine learning tool to predict clinically relevant outcomes in boys with posterior urethral valves. Pediatr. Nephrol. 2022, 37, 1067–1074. [Google Scholar] [CrossRef]
- Vinit, N.; Gueneuc, A.; Bessieres, B.; Dreux, S.; Heidet, L.; Salomon, R.; Lapillonne, A.; De Bernardis, G.; Salomon, L.J.; Stirnemann, J.J.; et al. Fetal Cystoscopy and Vesicoamniotic Shunting in Lower Urinary Tract Obstruction: Long-Term Outcome and Current Technical Limitations. Fetal Diagn. Ther. 2020, 47, 74–83. [Google Scholar] [CrossRef]
- Morris, R.K.; Malin, G.L.; Quinlan-Jones, E.; Middleton, L.J.; Hemming, K.; Burke, D.; Daniels, J.P.; Khan, K.S.; Deeks, J.; Kilby, M.D.; et al. Percutaneous vesicoamniotic shunting versus conservative management for fetal lower urinary tract obstruction (PLUTO): A randomised trial. Lancet 2013, 382, 1496–1506. [Google Scholar] [CrossRef]
- Nassr, A.A.; Shazly, S.A.M.; Abdelmagied, A.M.; Araujo Junior, E.; Tonni, G.; Kilby, M.D.; Ruano, R. Effectiveness of vesicoamniotic shunt in fetuses with congenital lower urinary tract obstruction: An updated systematic review and meta-analysis. Ultrasound Obstet. Gynecol. 2017, 49, 696–703. [Google Scholar] [CrossRef]
- Kohl, T.; Fimmers, R.; Axt-Fliedner, R.; Degenhardt, J.; Bruckmann, M. Vesico-amniotic shunt insertion prior to the completion of 16 weeks results in improved preservation of renal function in surviving fetuses with isolated severe lower urinary tract obstruction (LUTO). J. Pediatr. Urol. 2022, 18, 116–126. [Google Scholar] [CrossRef]
- Wuhl, E.; van Stralen, K.J.; Verrina, E.; Bjerre, A.; Wanner, C.; Heaf, J.G.; Zurriaga, O.; Hoitsma, A.; Niaudet, P.; Palsson, R.; et al. Timing and outcome of renal replacement therapy in patients with congenital malformations of the kidney and urinary tract. Clin. J. Am. Soc. Nephrol. 2013, 8, 67–74. [Google Scholar] [CrossRef]
- McKay, A.M.; Kim, S.; Kennedy, S.E. Long-term outcome of kidney transplantation in patients with congenital anomalies of the kidney and urinary tract. Pediatr. Nephrol. 2019, 34, 2409–2415. [Google Scholar] [CrossRef] [PubMed]
- Salomon, L.; Fontaine, E.; Gagnadoux, M.F.; Broyer, M.; Beurton, D. Posterior urethral valves: Long-term renal function consequences after transplantation. J. Urol. 1997, 157, 992–995. [Google Scholar] [CrossRef]
- Reinberg, Y.; Gonzalez, R.; Fryd, D.; Mauer, S.M.; Najarian, J.S. The outcome of renal transplantation in children with posterior urethral valves. J. Urol. 1988, 140, 1491–1493. [Google Scholar] [CrossRef]
- Cornwell, L.B.; Ingulli, E.G.; Mason, M.D.; Ewing, E.; Riddell, J.V. Renal Transplants Due to Congenital Anomalies of the Kidney and Urinary Tract (CAKUT) Have Better Graft Survival Than Non-CAKUT Controls: Analysis of Over 10,000 Patients. Urology 2021, 154, 255–262. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Prenatal | Postnatal |
|---|---|
| Ultrasound Signs of hypodysplasia | Ultrasound Signs of hypodysplasia |
| Fetal urine β-2-microglobuline ↑, chloride ↑ 12PUV (peptide-panel) | Nadir serum creatinine <0.4 mg/dL: very low risk for ESRD >0.8–1.0 mg/dL high risk for ESRD |
| Presence of bladder dysfunction | |
| Recurrent febrile UTI | |
| Urinary markers microalbuminuria TGF-β ↑, MCP-1 ↑ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klaus, R.; Lange-Sperandio, B. Chronic Kidney Disease in Boys with Posterior Urethral Valves–Pathogenesis, Prognosis and Management. Biomedicines 2022, 10, 1894. https://doi.org/10.3390/biomedicines10081894
Klaus R, Lange-Sperandio B. Chronic Kidney Disease in Boys with Posterior Urethral Valves–Pathogenesis, Prognosis and Management. Biomedicines. 2022; 10(8):1894. https://doi.org/10.3390/biomedicines10081894
Chicago/Turabian StyleKlaus, Richard, and Bärbel Lange-Sperandio. 2022. "Chronic Kidney Disease in Boys with Posterior Urethral Valves–Pathogenesis, Prognosis and Management" Biomedicines 10, no. 8: 1894. https://doi.org/10.3390/biomedicines10081894
APA StyleKlaus, R., & Lange-Sperandio, B. (2022). Chronic Kidney Disease in Boys with Posterior Urethral Valves–Pathogenesis, Prognosis and Management. Biomedicines, 10(8), 1894. https://doi.org/10.3390/biomedicines10081894