
Exploiting Bacteria for Improving Hypoxemia of COVID-19 Patients


 ,
,  ,
, 
 , and
, and 
Abstract
:1. Background
2. Methods
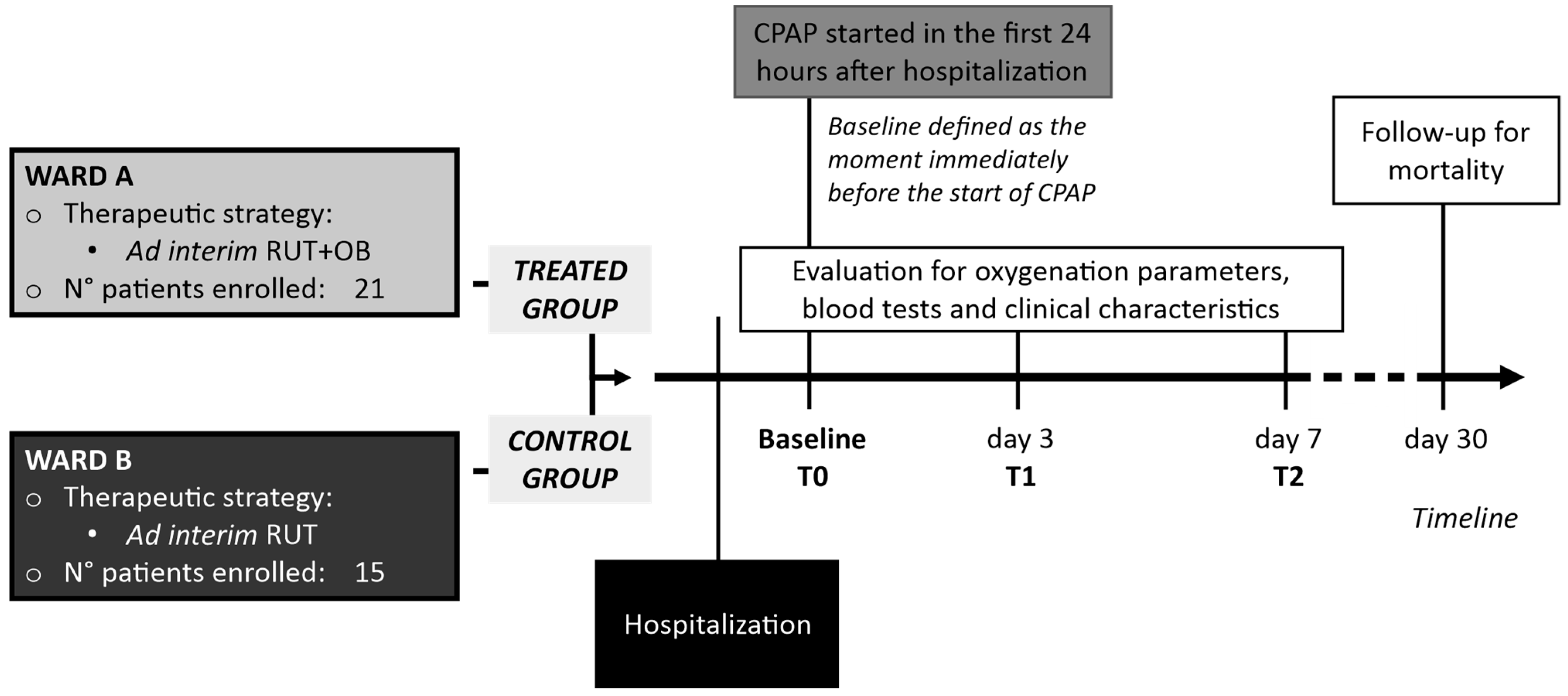
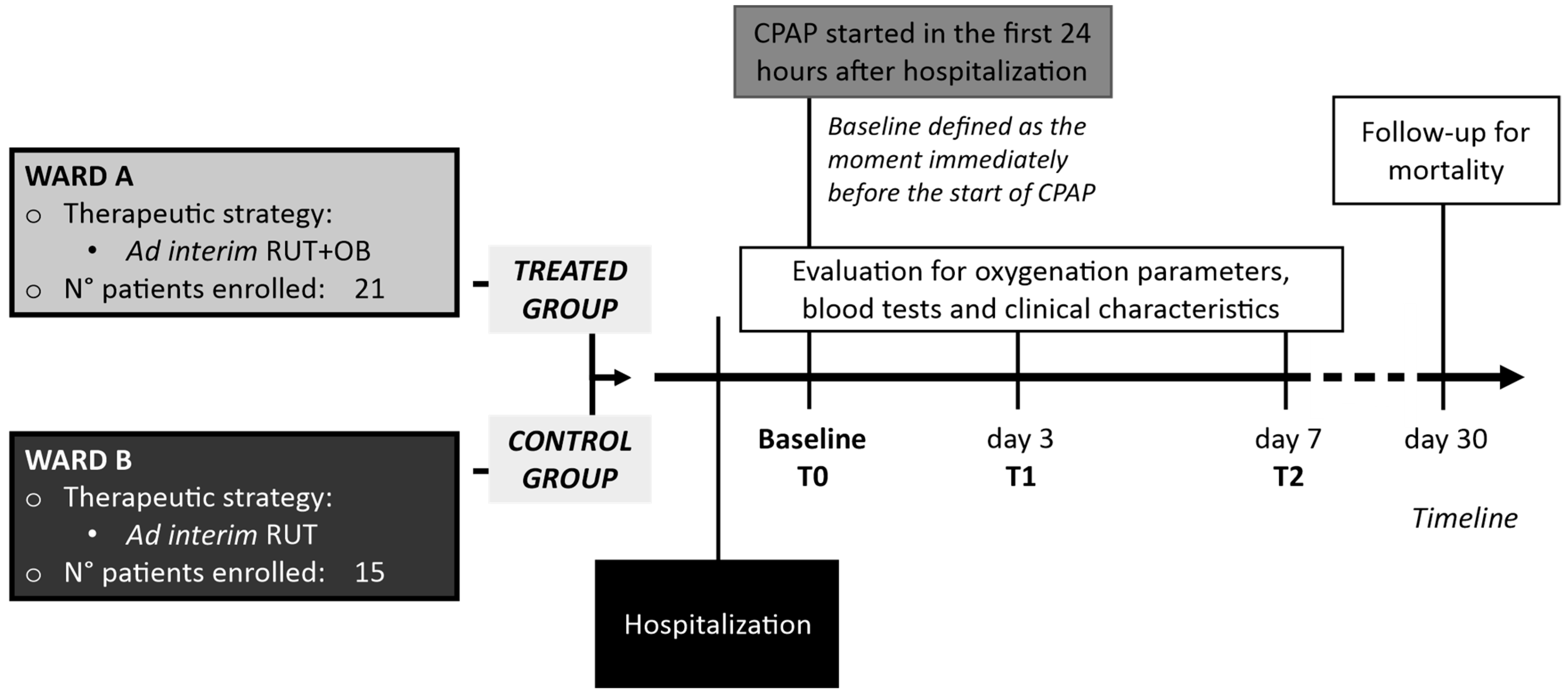
2.1. Design of the Study, Population, Settings and Data Collection
2.2. Diagnosis of SARS-CoV-2 Infection, Radiological Staging and Treatment
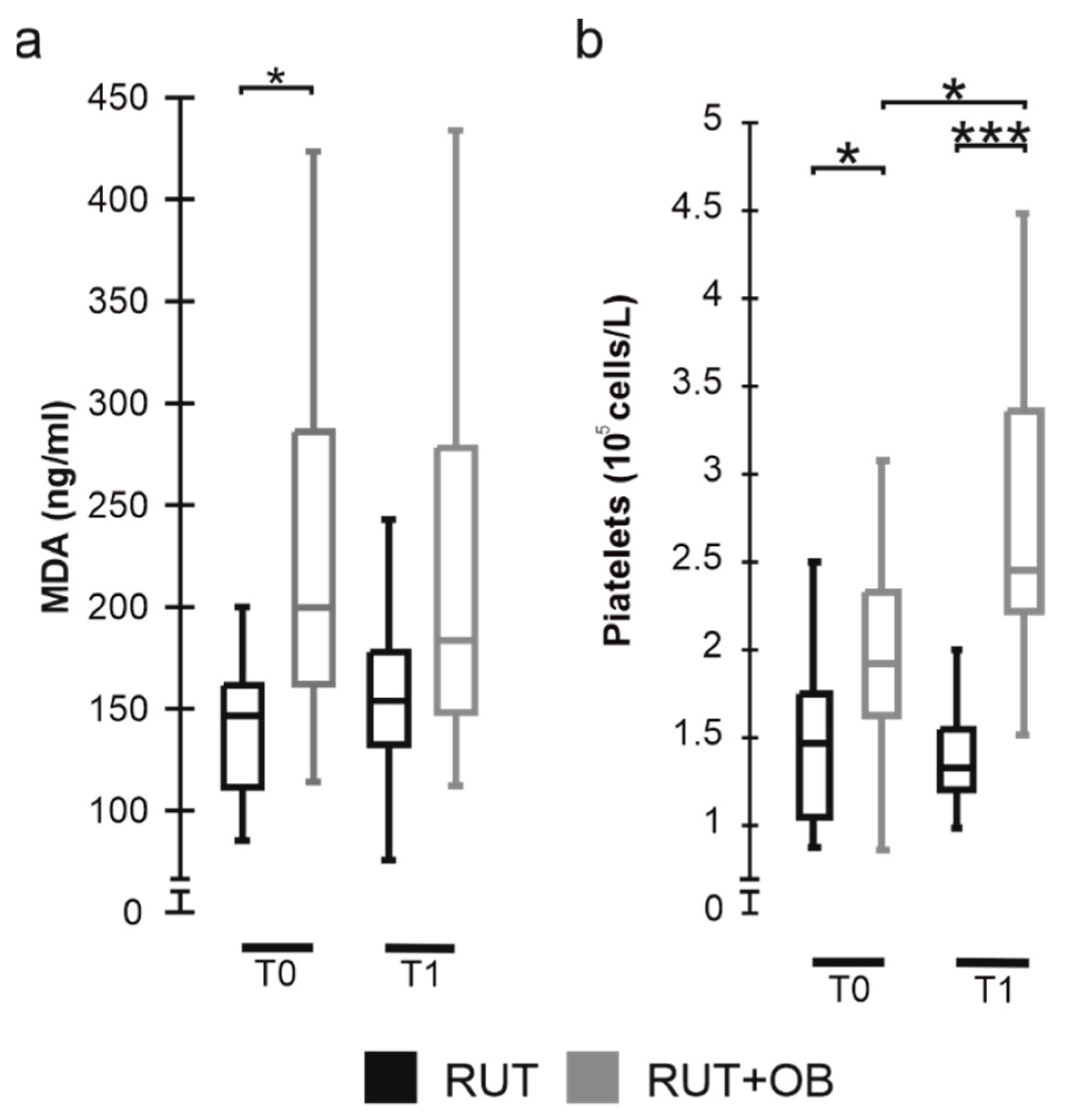
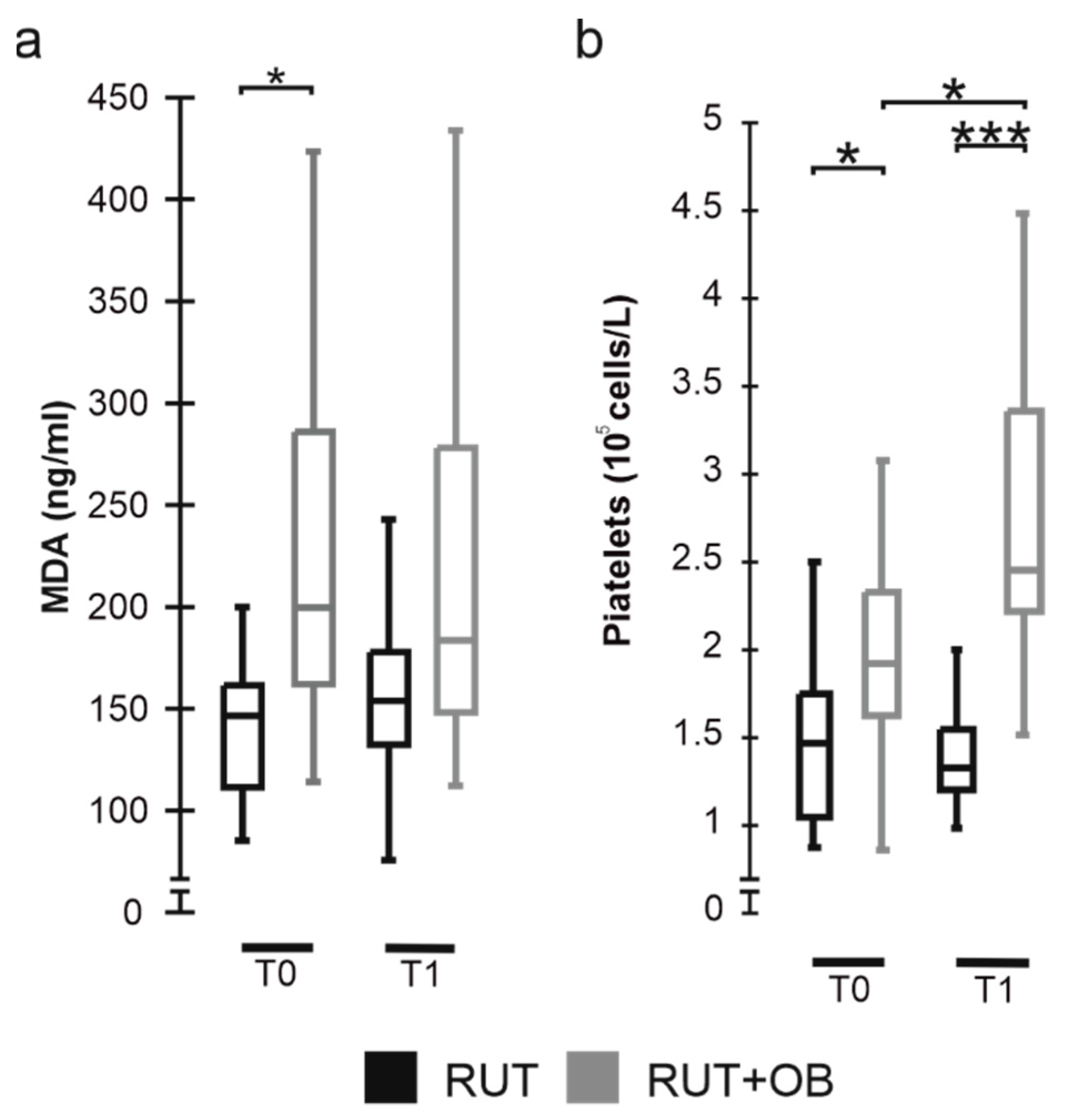
2.3. Malondialdehyde (MDA) Level Assay
2.4. Ethics Committee Approval
2.5. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Acosta, R.A.H.; Garrigos, Z.E.; Marcelin, J.R.; Vijayvargiya, P. COVID-19 Pathogenesis and Clinical Manifestations. Infect. Dis. Clin. N. Am. 2022, 36, 231–249. [Google Scholar] [CrossRef] [PubMed]
- Chavez, S.; Brady, W.J.; Gottlieb, M.; Carius, B.M.; Liang, S.Y.; Koyfman, A.; Long, B. Clinical update on COVID-19 for the emergency clinician: Airway and resuscitation. Am. J. Emerg. Med. 2022, 58, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Okabe, R.; Toyofumi, F.; Yoshikawa, C.; Yoneyama, Y.; Yokoyama, Y.; Tanaka, S.; Yoshizawa, A.; Thompson, W.L.; Kannan, G.; Kobayashi, E.; et al. Mammalian enteral ventilation ameliorates respiratory failure. Med 2021, 2, 773–783. [Google Scholar] [CrossRef] [PubMed]
- Singhal, R.; Shah, Y.M. Oxygen battle in the gut: Hypoxia and hypoxia-inducible factors in metabolic and inflammatory responses in the intestine. J. Biol. Chem. 2020, 295, 10493–10505. [Google Scholar] [CrossRef] [PubMed]
- Callapina, M.; Zhou, J.; Schnitzer, S.; Metzen, E.; Lohr, C.; Deitmer, J.W.; Brüne, B. Nitric oxide reverses desferrioxamine- and hypoxia-evoked HIF-1α accumulation—Implications for prolyl hydroxylase activity and iron. Exp. Cell Res. 2005, 306, 274–284. [Google Scholar] [CrossRef] [PubMed]
- Ceccarelli, G.; Marazzato, M.; Celani, L.; Lombardi, F.; Piccirilli, A.; Mancone, M.; Trinchieri, V.; Pugliese, F.; Mastroianni, C.M.; D’Ettorre, G. Oxygen Sparing Effect of Bacteriotherapy in COVID-19. Nutrients 2021, 13, 2898. [Google Scholar] [CrossRef]
- Bonfili, L.; Gong, C.; Lombardi, F.; Cifone, M.G.; Eleuteri, A.M. Strategic Modification of Gut Microbiota through Oral Bacteriotherapy Influences Hypoxia Inducible Factor-1α: Therapeutic Implication in Alzheimer’s Disease. Int. J. Mol. Sci. 2021, 23, 357. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Case Definition for Coronavirus Disease 2019 (COVID-19). 2020. Available online: https://www.ecdc.europa.eu/en/covid-19/surveillance/case-definition (accessed on 1 February 2021).
- World Health Organization. Clinical Management of COVID-19; WHO: Geneva, Switzerland, 2020; pp. 1–62. [Google Scholar]
- Mussini, C.; Falcone, M.; Nozza, S.; Sagnelli, C.; Parrella, R.; Meschiari, M.; Petrosillo, N.; Mastroianni, C.; Cascio, A.; Iaria, C.; et al. Therapeutic strategies for severe COVID-19: A position paper from the Italian Society of Infectious and Tropical Diseases (SIMIT). Clin. Microbiol. Infect. 2020, 27, 389–395. [Google Scholar] [CrossRef]
- Duca, A.; Memaj, I.; Zanardi, F.; Preti, C.; Alesi, A.; Della Bella, L.; Ghezzi, E.; di Marco, F.; Lorini, L.F.; Venturelli, S.; et al. Severity of respiratory failure and outcome of patients needing a ventilatory support in the Emergency Department during Italian novel coronavirus SARS-CoV-2 outbreak: Preliminary data on the role of Helmet CPAP and Non-Invasive Positive Pressure Ventilation. eClinicalMedicine 2020, 24, 100419. [Google Scholar] [CrossRef]
- Brusasco, C.; Corradi, F.; Di Domenico, A.; Raggi, F.; Timossi, G.; Santori, G.; Brusasco, V.; CPAP-COVID-19 Study Group; Collaborators of the Galliera CPAP-COVID-19 Study Group. Continuous positive airway pressure in COVID-19 patients with moderate-to-severe respiratory failure. Eur. Respir. J. 2020, 57, 2002524. [Google Scholar] [CrossRef]
- Sundararaman, A.; Ray, M.; Ravindra, P.V.; Halami, P.M. Role of probiotics to combat viral infections with emphasis on COVID-19. Appl. Microbiol. Biotechnol. 2020, 104, 8089–8104. [Google Scholar] [CrossRef] [PubMed]
- Lau, H.C.-H.; Ng, S.C.; Yu, J. Targeting the Gut Microbiota in Coronavirus Disease 2019: Hype or Hope? Gastroenterology 2022, 162, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Ferreiro, A.; Formigo-Couceiro, F.J.; Veiga-Gutierrez, R.; Maldonado-Lobón, J.A.; Hermida-Cao, A.M.; Rodriguez, C.; Bañuelos, O.; Olivares, M.; Blanco-Rojo, R. Effects of Loigolactobacillus coryniformis K8 CECT 5711 on the Immune Response of Elderly Subjects to COVID-19 Vaccination: A Randomized Controlled Trial. Nutrients 2022, 14, 228. [Google Scholar] [CrossRef] [PubMed]
- Wischmeyer, P.E.; Tang, H.; Ren, Y.; Bohannon, L.; Ramirez, Z.E.; Andermann, T.M.; Julia, A.; Sung, J.A.; Jensen, D.; Jung, S.; et al. Daily Lactobacillus Probiotic versus Placebo in COVID-19-Exposed Household Contacts (PROTECT-EHC): A Randomized Clinical Trial. medRxiv 2022. [Google Scholar] [CrossRef]
- D’Ettorre, G.; Ceccarelli, G.; Marazzato, M.; Campagna, G.; Pinacchio, C.; Alessandri, F.; Ruberto, F.; Rossi, G.; Celani, L.; Scagnolari, C.; et al. Challenges in the Management of SARS-CoV-2 Infection: The Role of Oral Bacteriotherapy as Complementary Therapeutic Strategy to Avoid the Progression of COVID-19. Front. Med. 2020, 7, 389. [Google Scholar] [CrossRef] [PubMed]
- Ceccarelli, G.; Borrazzo, C.; Pinacchio, C.; Santinelli, L.; Innocenti, G.P.; Cavallari, E.N.; Celani, L.; Marazzato, M.; Alessandri, F.; Ruberto, F.; et al. Oral Bacteriotherapy in Patients With COVID-19: A Retrospective Cohort Study. Front. Nutr. 2021, 7, 613928. [Google Scholar] [CrossRef]
- Ceccarelli, G.; Scagnolari, C.; Pugliese, F.; Mastroianni, C.M.; D’Ettorre, G. Probiotics and COVID-19. Lancet Gastroenterol. Hepatol. 2020, 5, 721–722. [Google Scholar] [CrossRef]
- De Angelis, M.; Mariotti, L.; Rossi, J.; Servili, M.; Fox, P.F.; Rollán, G.; Gobbetti, M. Arginine Catabolism by Sourdough Lactic Acid Bacteria: Purification and Characterization of the Arginine Deiminase Pathway Enzymes from Lactobacillus sanfranciscensis CB1. Appl. Environ. Microbiol. 2002, 68, 6193–6201. [Google Scholar] [CrossRef] [Green Version]
- Dillon, B.J.; Holtsberg, F.W.; Ensor, C.M.; Bomalaski, J.S.; Clark, M.A. Biochemical characterization of the arginine degrading enzymes arginase and arginine deiminase and their effect on nitric oxide production. Med. Sci. Monit. 2002, 8, BR248–BR253. [Google Scholar]
- Riccia, D.D.; Bizzini, F.; Perilli, M.; Polimeni, A.; Trinchieri, V.; Amicosante, G.; Cifone, M.G. Anti-inflammatory effects of Lactobacillus brevis (CD2) on periodontal disease. Oral Dis. 2007, 13, 376–385. [Google Scholar] [CrossRef]
- Andrew, P.J. Enzymatic function of nitric oxide synthases. Cardiovasc. Res. 1999, 43, 521–531. [Google Scholar] [CrossRef]
- Król, M.; Kepinska, M. Human Nitric Oxide Synthase—Its Functions, Polymorphisms, and Inhibitors in the Context of Inflammation, Diabetes and Cardiovascular Diseases. Int. J. Mol. Sci. 2020, 22, 56. [Google Scholar] [CrossRef] [PubMed]
- Lundquist, P.; Artursson, P. Oral absorption of peptides and nanoparticles across the human intestine: Opportunities, limitations and studies in human tissues. Adv. Drug Deliv. Rev. 2016, 106, 256–276. [Google Scholar] [CrossRef] [PubMed]
- Rohlfing, A.-K.; Rath, D.; Geisler, T.; Gawaz, M. Platelets and COVID-19. Hamostaseologie 2021, 41, 379–385. [Google Scholar] [CrossRef]
- Bao, C.; Tao, X.; Cui, W.; Yi, B.; Pan, T.; Young, K.H.; Qian, W. SARS-CoV-2 induced thrombocytopenia as an important biomarker significantly correlated with abnormal coagulation function, increased intravascular blood clot risk and mortality in COVID-19 patients. Exp. Hematol. Oncol. 2020, 9, 16. [Google Scholar] [CrossRef]
- Barrett, T.J.; Bilaloglu, S.; Cornwell, M.; Burgess, H.M.; Virginio, V.W.; Drenkova, K.; Ibrahim, H.; Yuriditsky, E.; Aphinyanaphongs, Y.; Lifshitz, M.; et al. Platelets contribute to disease severity in COVID-19. J. Thromb. Haemost. 2021, 19, 3139–3153. [Google Scholar] [CrossRef] [PubMed]
- Jevtic, S.D.; Nazy, I. The COVID Complex: A Review of Platelet Activation and Immune Complexes in COVID-19. Front. Immunol. 2022, 13, 807934. [Google Scholar] [CrossRef] [PubMed]
- Shen, D.; Wang, Y. Effects of hypoxia on platelet activation in pilots. Aviat. Space Environ. Med. 1994, 65, 646–648. [Google Scholar] [PubMed]
- Chaurasia, S.N.; Kushwaha, G.; Kulkarni, P.P.; Mallick, R.L.; Latheef, N.A.; Mishra, J.K.; Dash, D. Platelet HIF-2α promotes thrombogenicity through PAI-1 synthesis and extracellular vesicle release. Haematologica 2019, 104, 2482–2492. [Google Scholar] [CrossRef]
- Forcados, G.E.; Muhammad, A.; Oladipo, O.O.; Makama, S.; Meseko, C.A. Metabolic Implications of Oxidative Stress and Inflammatory Process in SARS-CoV-2 Pathogenesis: Therapeutic Potential of Natural Antioxidants. Front. Cell. Infect. Microbiol. 2021, 11, 654813. [Google Scholar] [CrossRef] [PubMed]
- Ito, F.; Sono, Y.; Ito, T. Measurement and Clinical Significance of Lipid Peroxidation as a Biomarker of Oxidative Stress: Oxidative Stress in Diabetes, Atherosclerosis, and Chronic Inflammation. Antioxidants 2019, 8, 72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kosanovic, T.; Sagic, D.; Djukic, V.; Pljesa-Ercegovac, M.; Savic-Radojevic, A.; Bukumiric, Z.; Lalosevic, M.; Djordjevic, M.; Coric, V.; Simic, T. Time Course of Redox Biomarkers in COVID-19 Pneumonia: Relation with Inflammatory, Multiorgan Impairment Biomarkers and CT Findings. Antioxidants 2021, 10, 1126. [Google Scholar] [CrossRef] [PubMed]
- Wozniak, D.R.; Rubino, A.; Tan, A.L.; Jones, N.L.; Webb, S.T.; Vuylsteke, A.; Palas, E.; Quinnell, T.G.; Smith, E.I.; Davies, M.G. Positive role of continuous positive airway pressure for intensive care unit patients with severe hypoxaemic respiratory failure due to COVID-19 pneumonia: A single centre experience. J. Intensiv. Care Soc. 2020, 23, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Radovanovic, D.; Rizzi, M.; Pini, S.; Saad, M.; Chiumello, D.A.; Santus, P. Helmet CPAP to Treat Acute Hypoxemic Respiratory Failure in Patients with COVID-19: A Management Strategy Proposal. J. Clin. Med. 2020, 9, 1191. [Google Scholar] [CrossRef] [PubMed]
- Aliberti, S.; Radovanovic, D.; Billi, F.; Sotgiu, G.; Costanzo, M.; Pilocane, T.; Saderi, L.; Gramegna, A.; Rovellini, A.; Perotto, L.; et al. Helmet CPAP treatment in patients with COVID-19 pneumonia: A multicentre cohort study. Eur. Respir. J. 2020, 56, 2001935. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| RUT (No. 21) Median(IQR) or No.(%) | RUT+OB (No. 15) Median(IQR) or No.(%) | p-Value | |
|---|---|---|---|
| Gender (Female) | 4 (28.6) | 13 (65) | 0.08 |
| Age (Years) | 66 (60–68) | 64 (54–73) | 0.74 |
| D-dimer µg/L | 667.5 (379.7–1332) | 749 (447–1094) | 0.94 |
| Fibrinogen g/L | 4.5 (3.6–5.1) | 4.4 (3.7–5.1) | 0.92 |
| Protein C reactive PCR µg/L | 14,500 (1300–52,550) | 28,000 (12,200–53,200) | 0.51 |
| High Flux Oxygen (%) | 14/14 (100) | 21/21 (100) | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trinchieri, V.; Marazzato, M.; Ceccarelli, G.; Lombardi, F.; Piccirilli, A.; Santinelli, L.; Maddaloni, L.; Vassalini, P.; Mastroianni, C.M.; d’Ettorre, G. Exploiting Bacteria for Improving Hypoxemia of COVID-19 Patients. Biomedicines 2022, 10, 1851. https://doi.org/10.3390/biomedicines10081851
Trinchieri V, Marazzato M, Ceccarelli G, Lombardi F, Piccirilli A, Santinelli L, Maddaloni L, Vassalini P, Mastroianni CM, d’Ettorre G. Exploiting Bacteria for Improving Hypoxemia of COVID-19 Patients. Biomedicines. 2022; 10(8):1851. https://doi.org/10.3390/biomedicines10081851
Chicago/Turabian StyleTrinchieri, Vito, Massimiliano Marazzato, Giancarlo Ceccarelli, Francesca Lombardi, Alessandra Piccirilli, Letizia Santinelli, Luca Maddaloni, Paolo Vassalini, Claudio Maria Mastroianni, and Gabriella d’Ettorre. 2022. "Exploiting Bacteria for Improving Hypoxemia of COVID-19 Patients" Biomedicines 10, no. 8: 1851. https://doi.org/10.3390/biomedicines10081851
APA StyleTrinchieri, V., Marazzato, M., Ceccarelli, G., Lombardi, F., Piccirilli, A., Santinelli, L., Maddaloni, L., Vassalini, P., Mastroianni, C. M., & d’Ettorre, G. (2022). Exploiting Bacteria for Improving Hypoxemia of COVID-19 Patients. Biomedicines, 10(8), 1851. https://doi.org/10.3390/biomedicines10081851