
ESWT Diminishes Axonal Regeneration following Repair of the Rat Median Nerve with Muscle-In-Vein Conduits but Not after Autologous Nerve Grafting

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Animals and Surgery
2.2. Application of ESWT
2.3. Functional Analysis
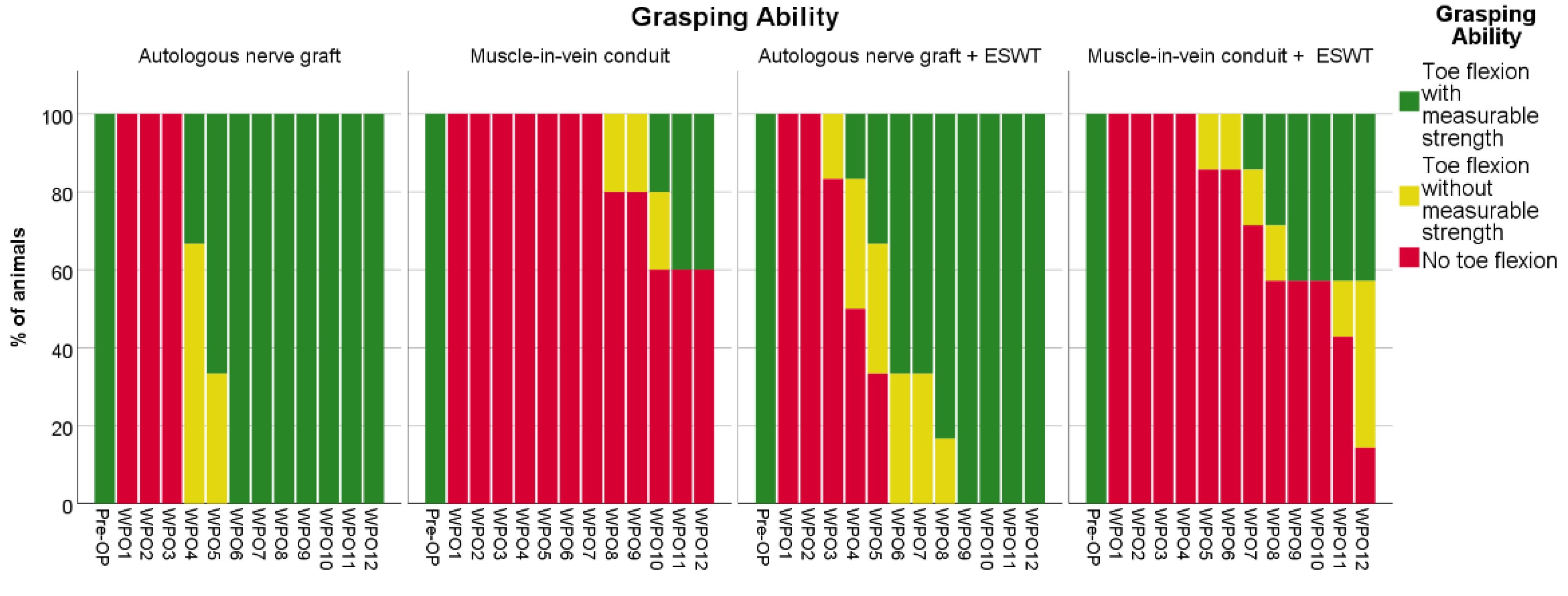
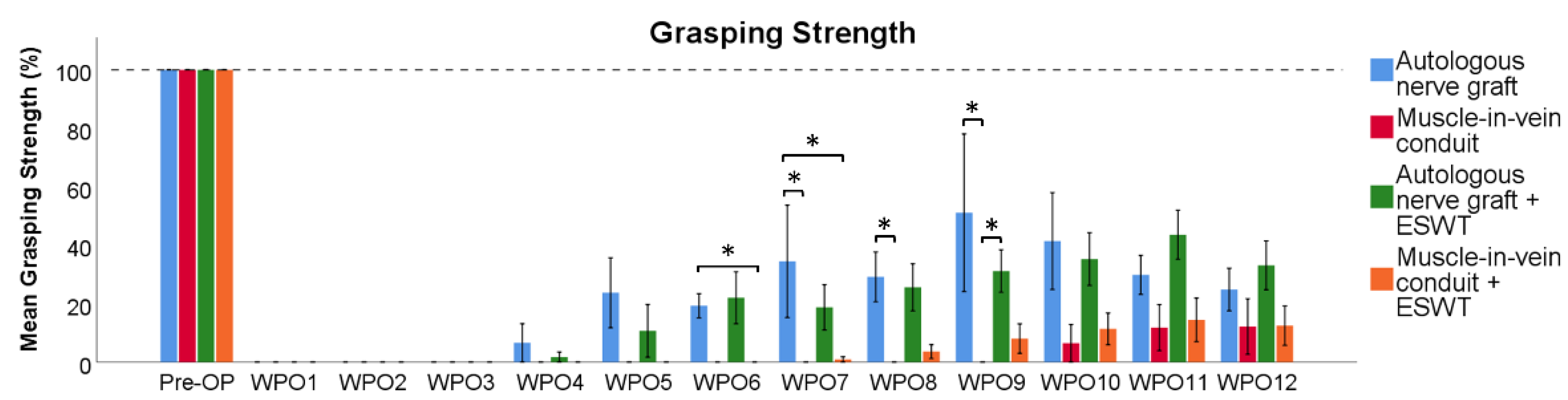
2.3.1. Reflex-Based Grasping
2.3.2. CatWalk XT Gait Analysis
2.3.3. Electrophysiological Analysis
2.4. Wet Muscle Weight
2.5. Histological Analysis
Automated Quantification of Axons, Lymphatic and Blood Vessels
2.6. Statistical Analysis
3. Results
3.1. Reflex-Based Grasping
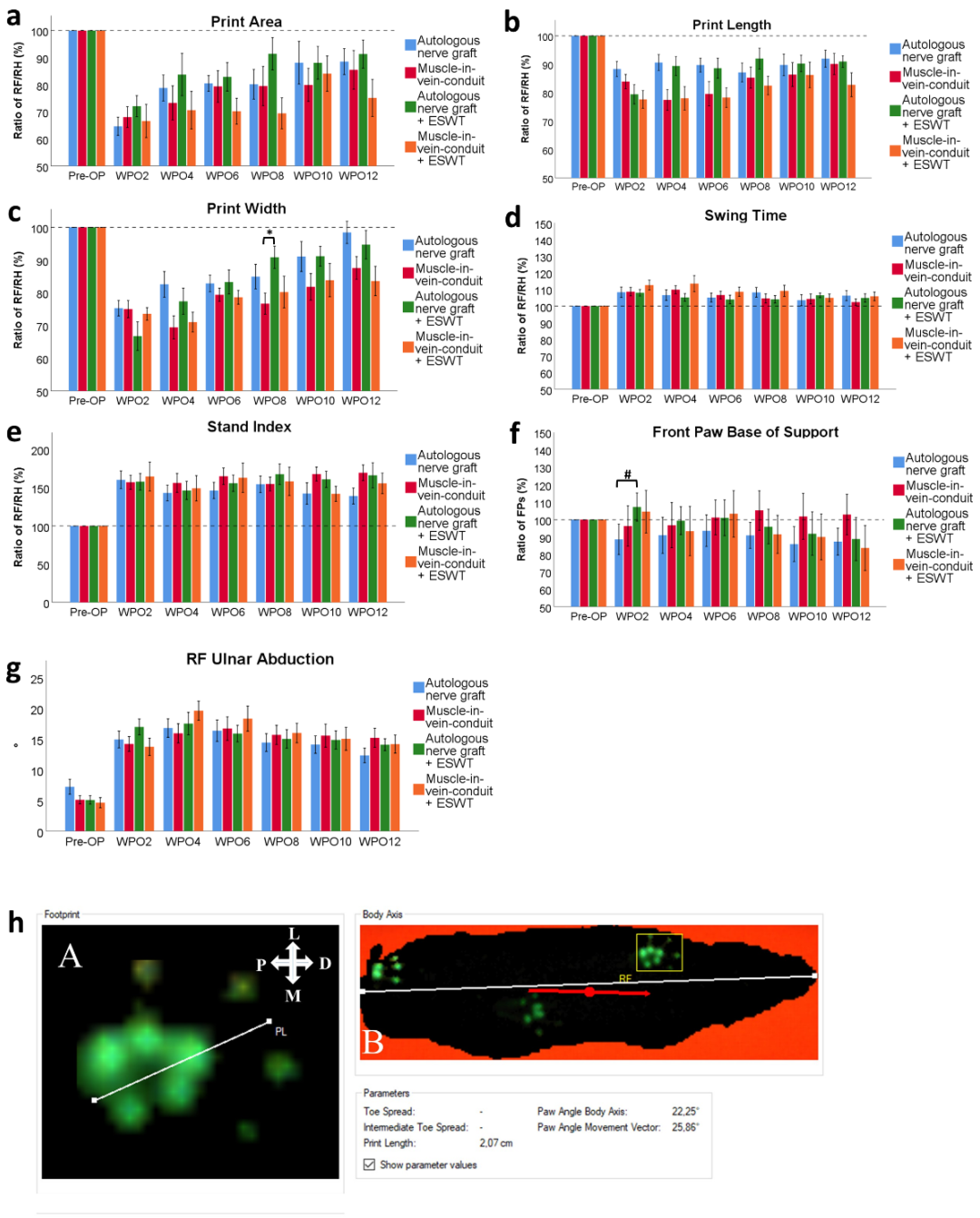
3.2. CatWalk XT Gait Analysis
3.2.1. Print Area
3.2.2. Print Length
3.2.3. Print Width
3.2.4. Swing Speed (Data Not Shown)
3.2.5. Swing Time
3.2.6. Duty Cycle (Data Not Shown)
3.2.7. Stand Index
3.2.8. FP BoS
3.2.9. Ulnar Abduction of the Right Front Paw
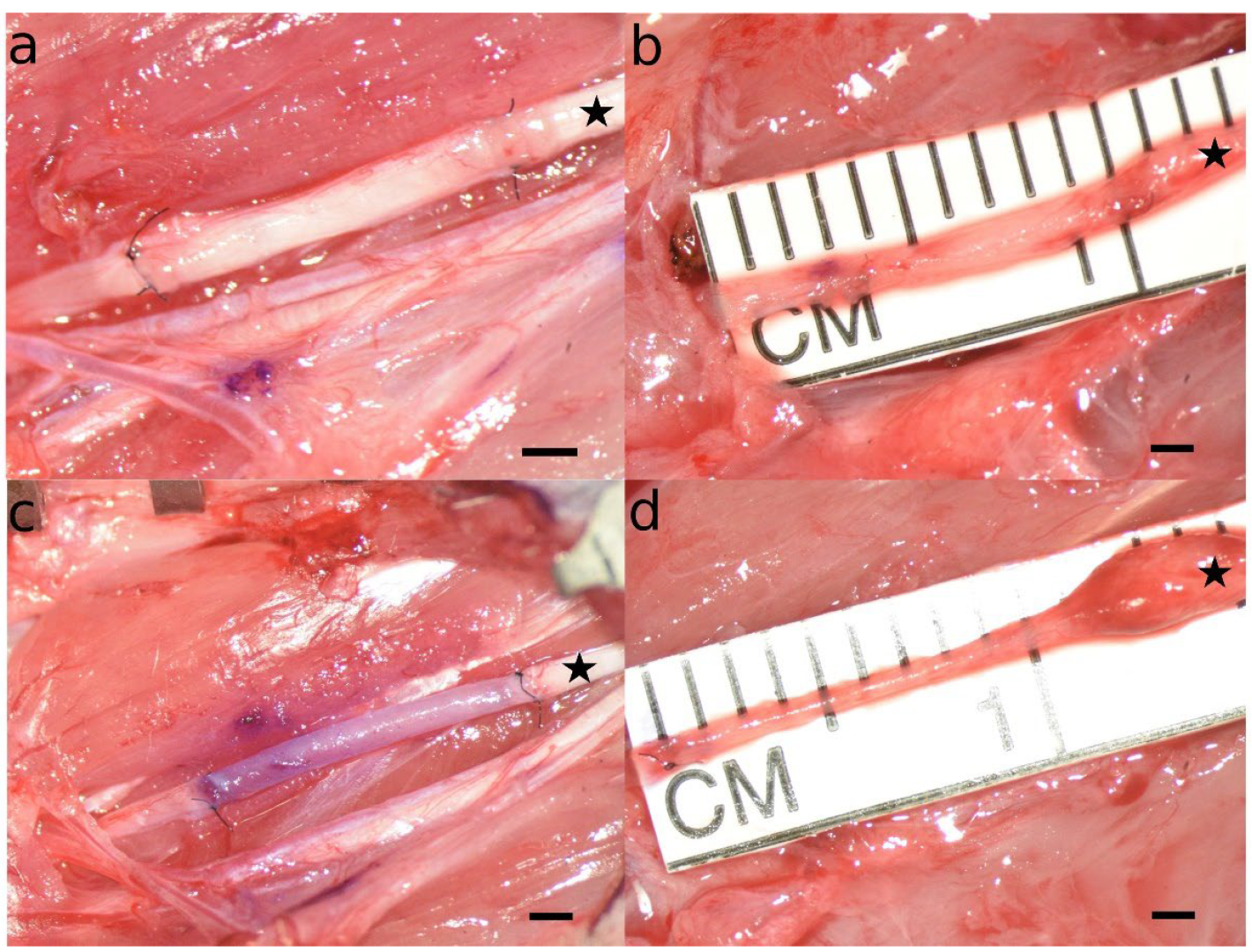
3.3. Appearance of the Reconstructed Median Nerve at WPO12
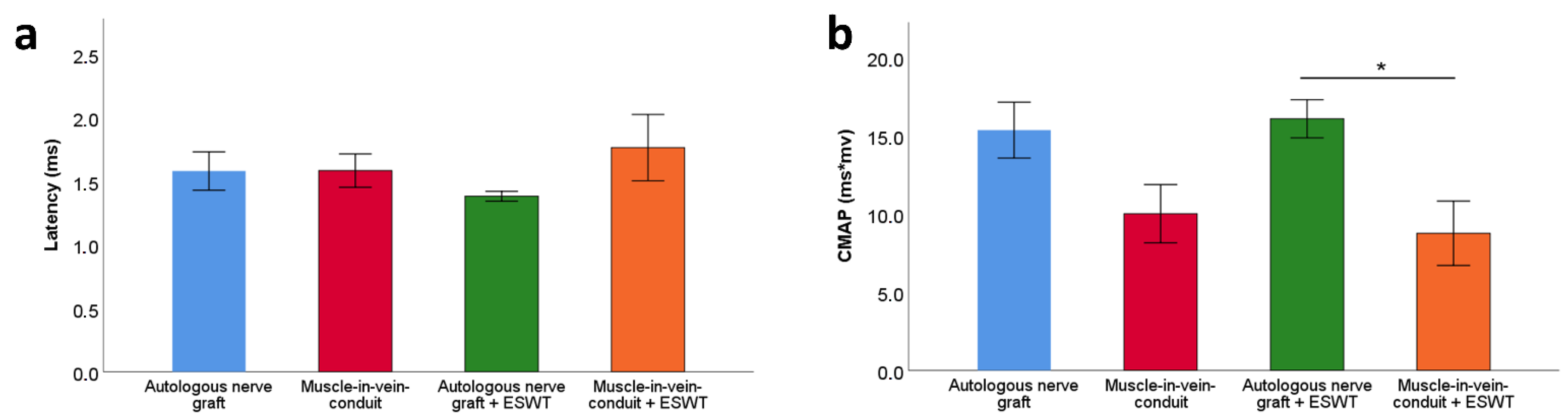
3.4. Electrophysiological Evaluations
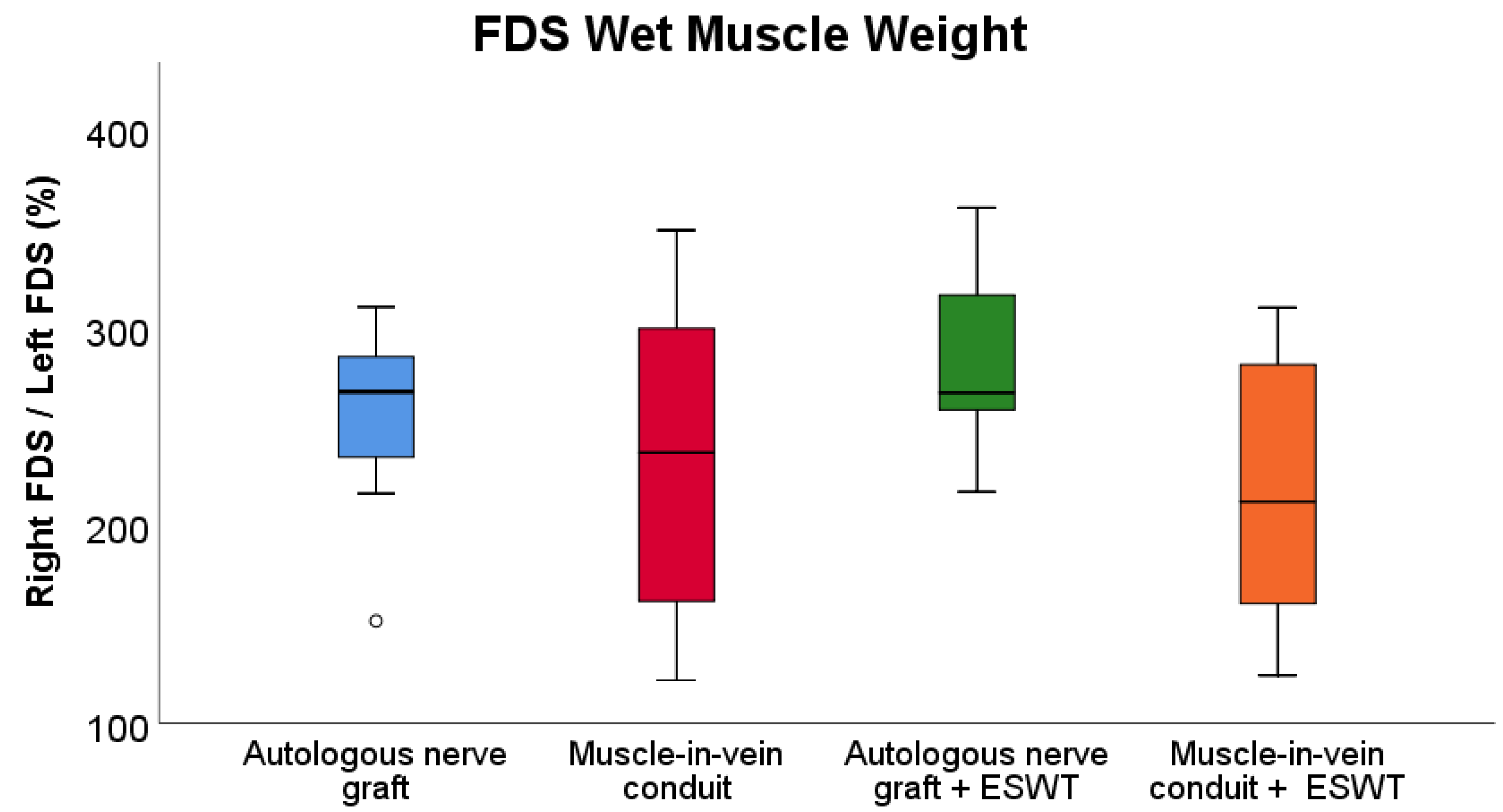
3.5. Wet Muscle Weight
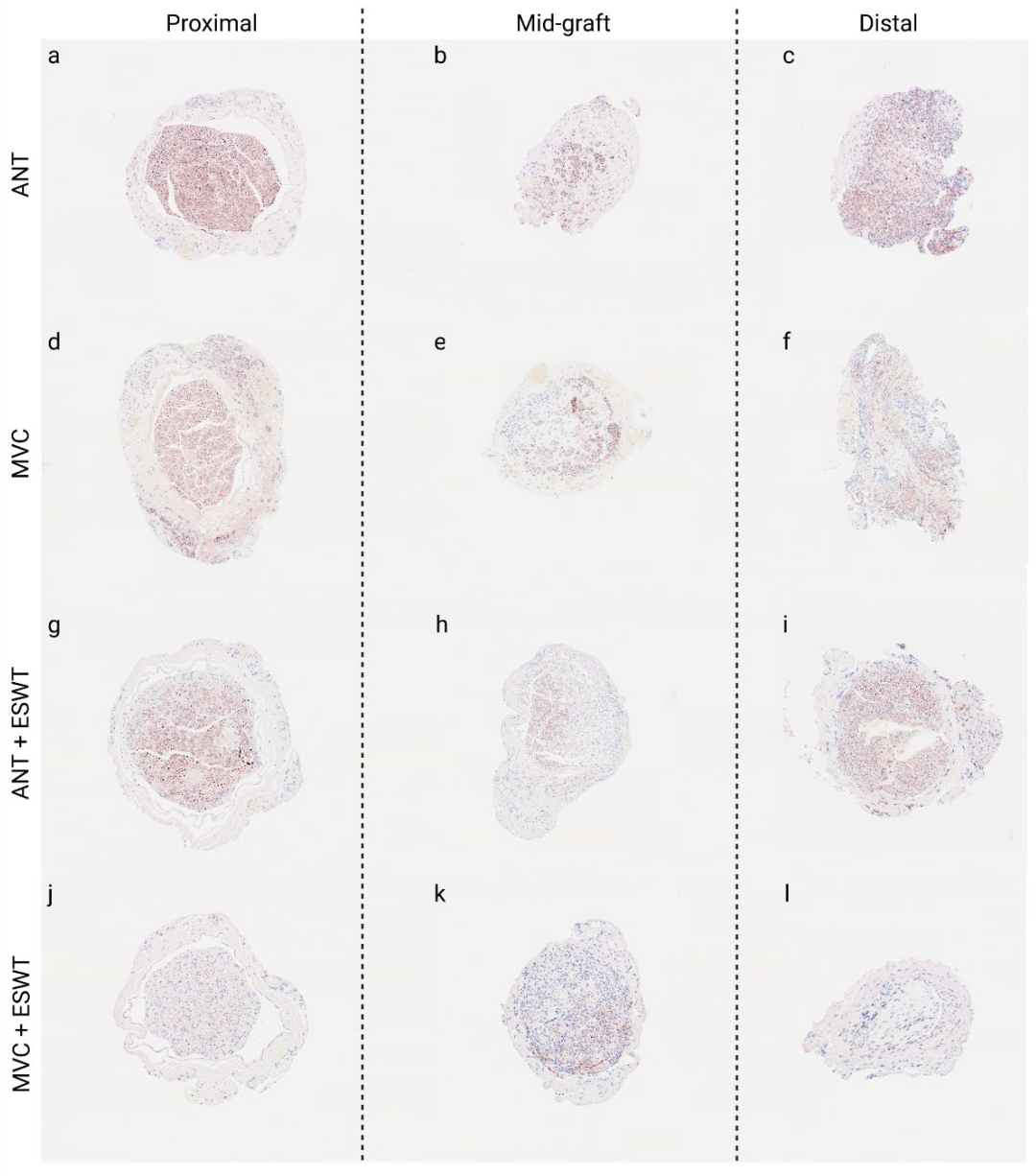
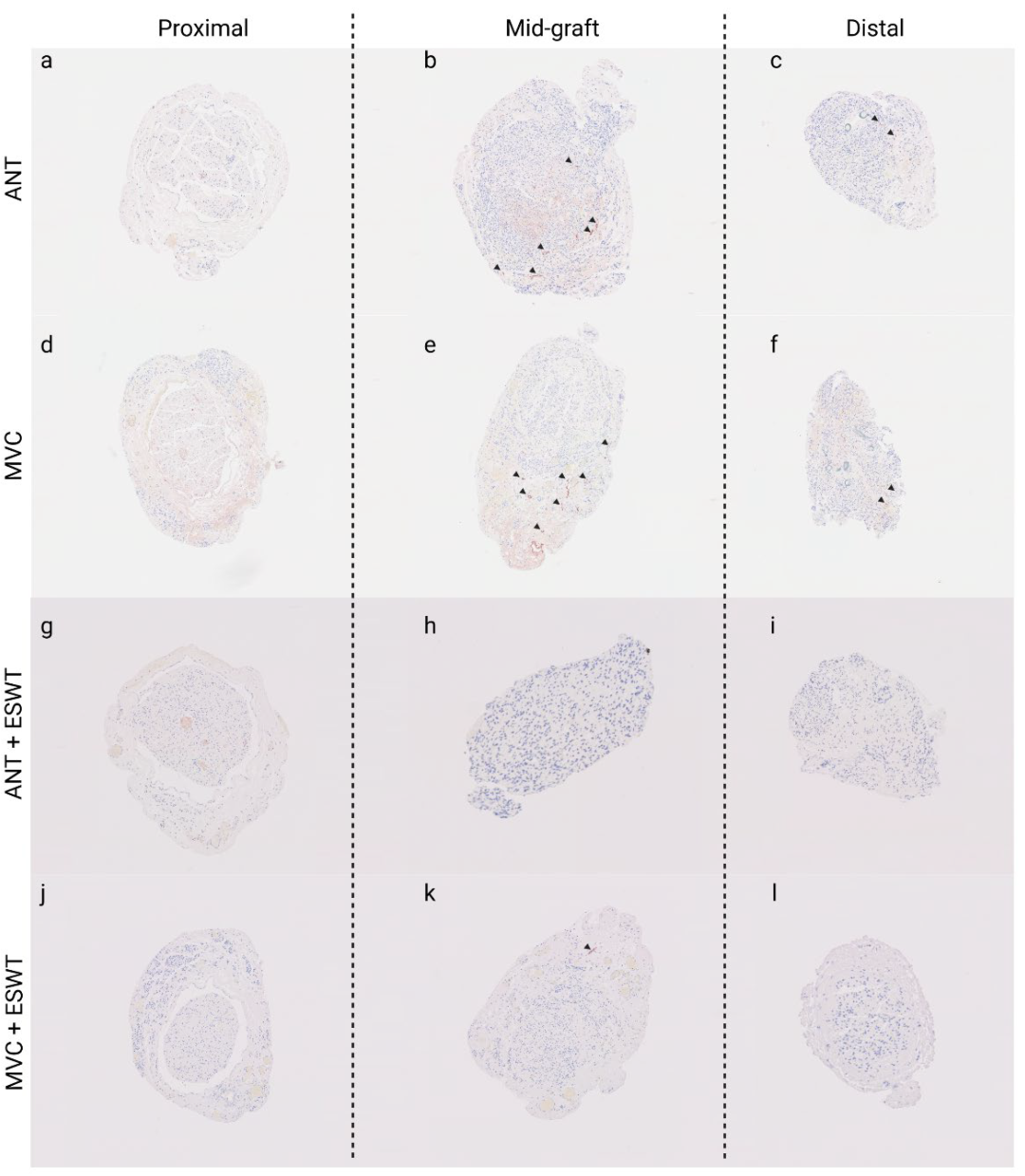
3.6. Histological Evaluations
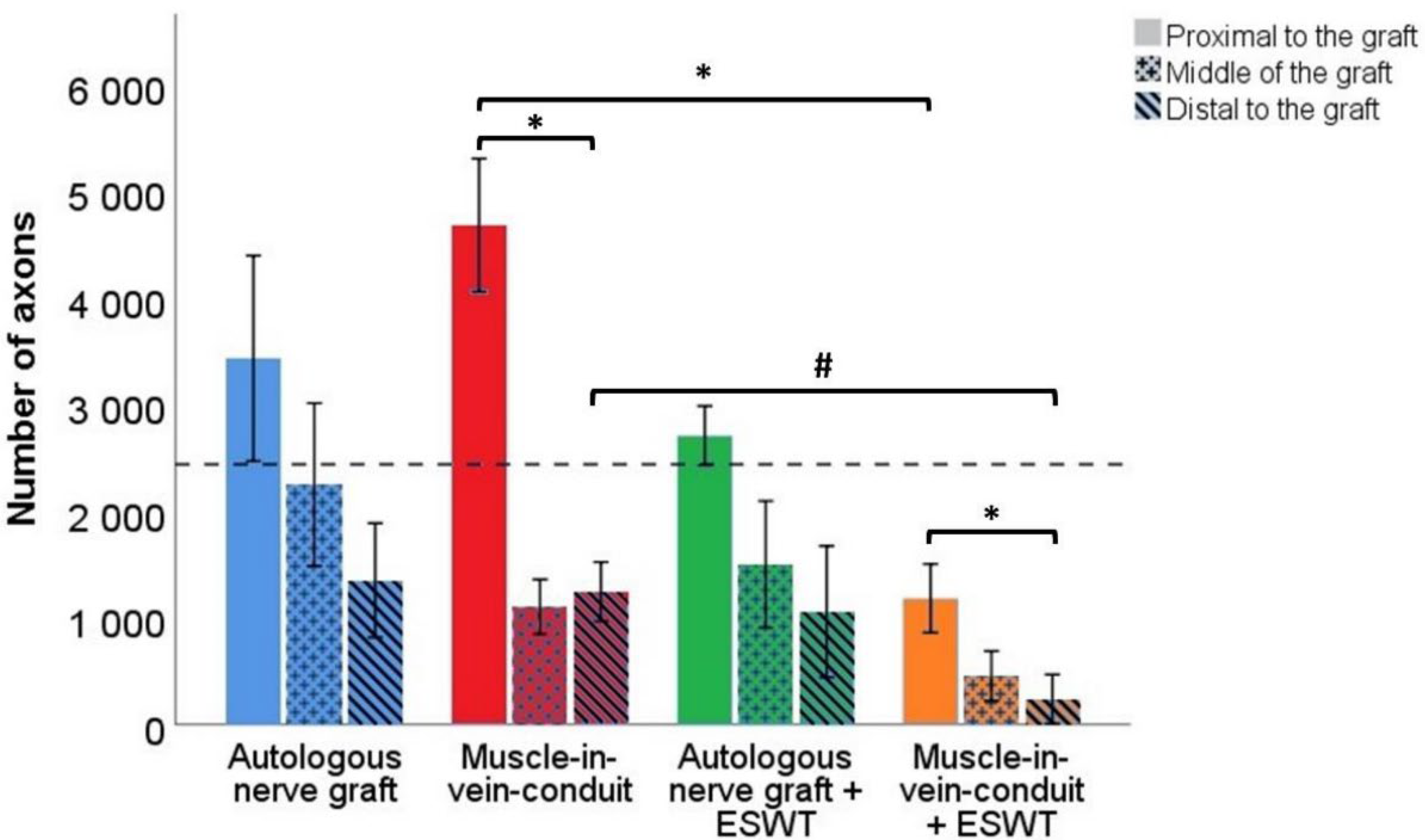
3.6.1. Number of Axons
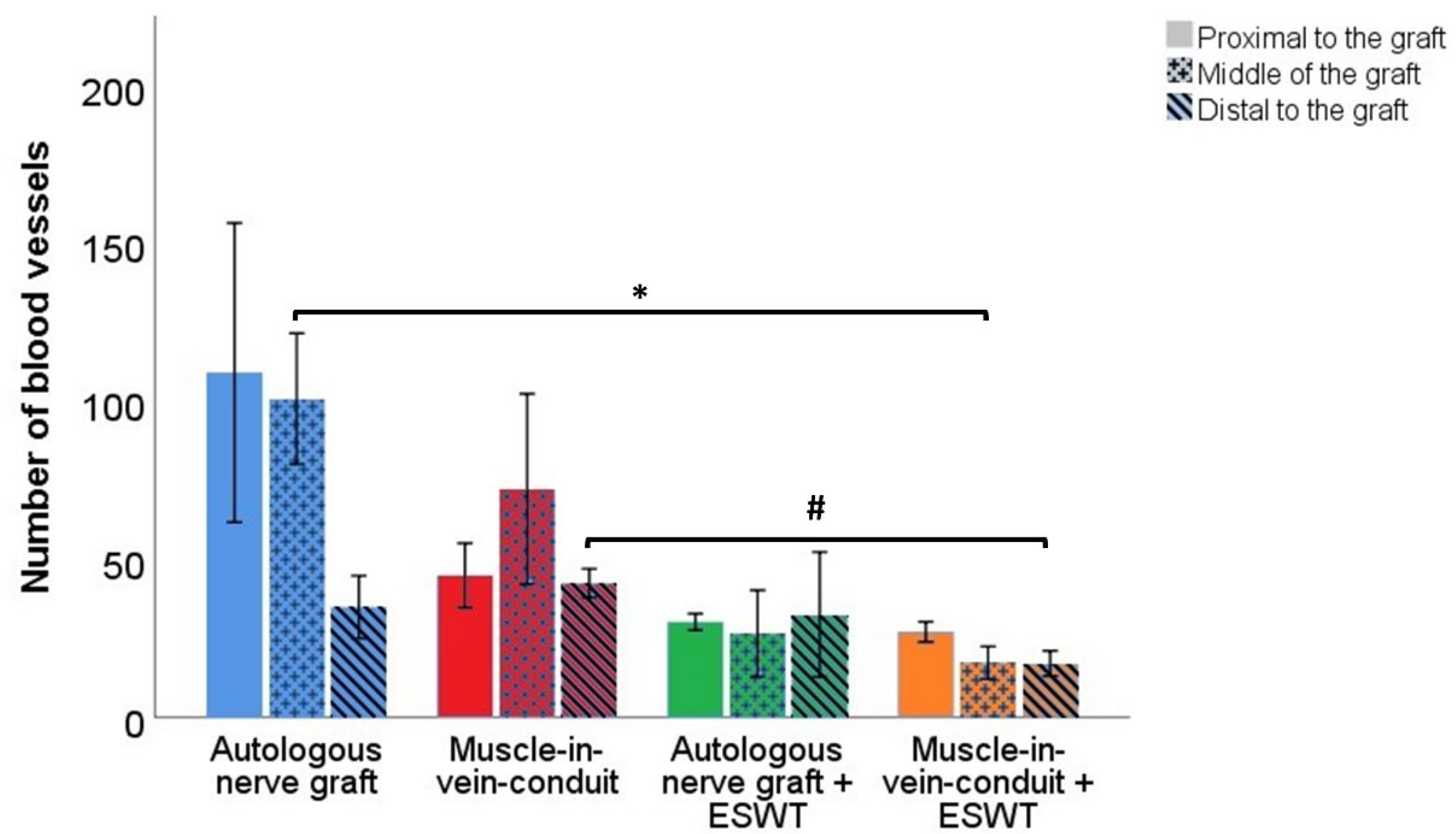
3.6.2. Number of Blood Vessels
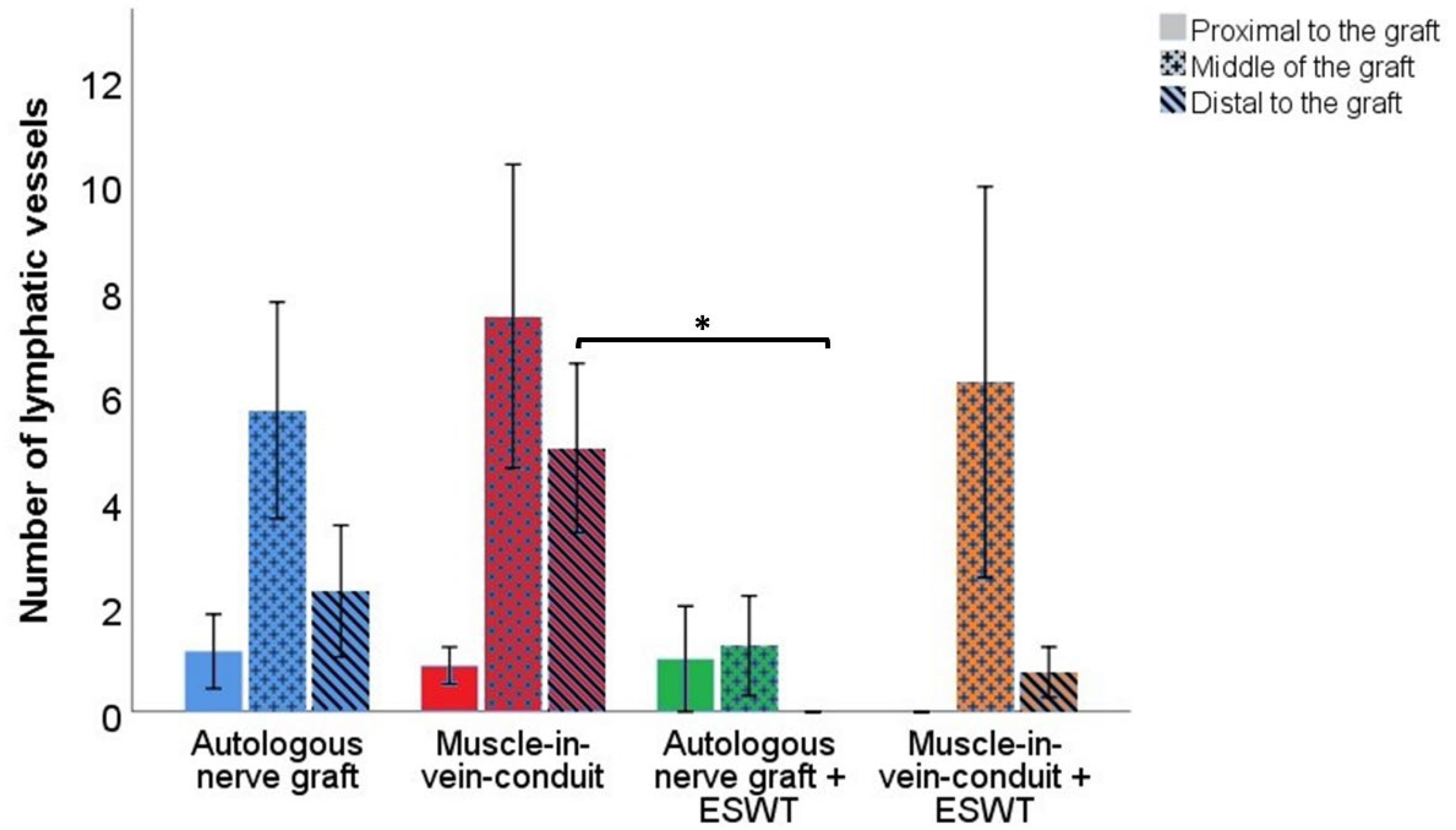
3.6.3. Number of Lymphatic Vessels
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huckhagel, T.; Nuchtern, J.; Regelsberger, J.; Lefering, R.; TraumaRegister DGU. Nerve injury in severe trauma with upper extremity involvement: Evaluation of 49,382 patients from the TraumaRegister DGU(R) between 2002 and 2015. Scand. J. Trauma Resusc. Emerg. Med. 2018, 26, 76. [Google Scholar] [CrossRef] [PubMed]
- Huckhagel, T.; Nüchtern, J.; Regelsberger, J.; Gelderblom, M.; Lefering, R.; TraumaRegister DGU. Nerve trauma of the lower extremity: Evaluation of 60,422 leg injured patients from the TraumaRegister DGU® between 2002 and 2015. Scand. J. Trauma Resusc. Emerg. Med. 2018, 26, 40. [Google Scholar] [CrossRef] [PubMed]
- Karsy, M.; Watkins, R.; Jensen, M.R.; Guan, J.; Brock, A.A.; Mahan, M.A. Trends and Cost Analysis of Upper Extremity Nerve Injury Using the National (Nationwide) Inpatient Sample. World Neurosurg. 2019, 123, e488–e500. [Google Scholar] [CrossRef] [PubMed]
- Foster, C.H.; Karsy, M.; Jensen, M.R.; Guan, J.; Eli, I.; Mahan, M.A. Trends and Cost-Analysis of Lower Extremity Nerve Injury Using the National Inpatient Sample. Neurosurgery 2019, 85, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Heinzel, J.C.; Dadun, L.F.; Prahm, C.; Winter, N.; Bressler, M.; Lauer, H.; Ritter, J.; Daigeler, A.; Kolbenschlag, J. Beyond the Knife—Reviewing the Interplay of Psychosocial Factors and Peripheral Nerve Lesions. J. Pers. Med. 2021, 11, 1200. [Google Scholar] [CrossRef]
- Bergmeister, K.D.; Grosse-Hartlage, L.; Daeschler, S.C.; Rhodius, P.; Bocker, A.; Beyersdorff, M.; Kern, A.O.; Kneser, U.; Harhaus, L. Acute and long-term costs of 268 peripheral nerve injuries in the upper extremity. PLoS ONE 2020, 15, e0229530. [Google Scholar] [CrossRef]
- Seddon, H.J. Three Types of Nerve Injury. Brain 1943, 66, 237–288. [Google Scholar] [CrossRef]
- Sunderland, S. A classification of peripheral nerve injuries producing loss of function. Brain 1951, 74, 491–516. [Google Scholar] [CrossRef]
- Pan, D.; Mackinnon, S.E.; Wood, M.D. Advances in the repair of segmental nerve injuries and trends in reconstruction. Muscle Nerve 2020, 61, 726–739. [Google Scholar] [CrossRef]
- Bassilios Habre, S.; Bond, G.; Jing, X.L.; Kostopoulos, E.; Wallace, R.D.; Konofaos, P. The Surgical Management of Nerve Gaps: Present and Future. Ann. Plast. Surg. 2018, 80, 252–261. [Google Scholar] [CrossRef]
- Kornfeld, T.; Vogt, P.M.; Radtke, C. Nerve grafting for peripheral nerve injuries with extended defect sizes. Wien. Med. Wochenschr. 2019, 169, 240–251. [Google Scholar] [CrossRef]
- Fowler, J.R.; Lavasani, M.; Huard, J.; Goitz, R.J. Biologic strategies to improve nerve regeneration after peripheral nerve repair. J. Reconstr. Microsurg. 2015, 31, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, C.R.; Oliveira, J.M.; Reis, R.L. Modern Trends for Peripheral Nerve Repair and Regeneration: Beyond the Hollow Nerve Guidance Conduit. Front. Bioeng. Biotechnol. 2019, 7, 337. [Google Scholar] [CrossRef]
- Navarro, X. Functional evaluation of peripheral nerve regeneration and target reinnervation in animal models: A critical overview. Eur. J. Neurosci. 2016, 43, 271–286. [Google Scholar] [CrossRef] [PubMed]
- Hussain, G.; Wang, J.; Rasul, A.; Anwar, H.; Qasim, M.; Zafar, S.; Aziz, N.; Razzaq, A.; Hussain, R.; de Aguilar, J.L.G.; et al. Current status of therapeutic approaches against peripheral nerve injuries: A detailed story from injury to recovery. Int. J. Biol. Sci. 2020, 16, 116–134. [Google Scholar] [CrossRef] [PubMed]
- Martínez de Albornoz, P.; Delgado, P.J.; Forriol, F.; Maffulli, N. Non-surgical therapies for peripheral nerve injury. Br. Med. Bull. 2011, 100, 73–100. [Google Scholar] [CrossRef]
- Li, H.X.; Zhang, Z.C.; Peng, J. Low-intensity extracorporeal shock wave therapy promotes recovery of sciatic nerve injury and the role of mechanical sensitive YAP/TAZ signaling pathway for nerve regeneration. Chin. Med. J. 2021, 134, 2710–2720. [Google Scholar] [CrossRef] [PubMed]
- Peng, D.; Tan, Y.; Reed-Maldonado, A.B.; Lin, G.; Lue, T.F. Molecular mechanism of action of low-intensity extracorporeal shockwave therapy for regenerating penile and peripheral nerves. Turk. J. Urol. 2020, 1. [Google Scholar] [CrossRef]
- Park, H.J.; Hong, J.; Piao, Y.; Shin, H.J.; Lee, S.J.; Rhyu, I.J.; Yi, M.H.; Kim, J.; Kim, D.W.; Beom, J. Extracorporeal shockwave therapy enhances peripheral nerve remyelination and gait function in a crush model. Adv. Clin. Exp. Med. 2020, 29, 819–824. [Google Scholar] [CrossRef]
- Sağir, D.; Bereket, C.; Onger, M.E.; Bakhit, N.; Keskin, M.; Ozkan, E. Efficacy of Extracorporeal Shockwaves Therapy on Peripheral Nerve Regeneration. J. Craniofac. Surg. 2019, 30, 2635–2639. [Google Scholar] [CrossRef]
- Simplicio, C.L.; Purita, J.; Murrell, W.; Santos, G.S.; Dos Santos, R.G.; Lana, J. Extracorporeal shock wave therapy mechanisms in musculoskeletal regenerative medicine. J. Clin. Orthop. Trauma 2020, 11, S309–S318. [Google Scholar] [CrossRef] [PubMed]
- Hausner, T.; Nogradi, A. The use of shock waves in peripheral nerve regeneration: New perspectives? Int. Rev. Neurobiol. 2013, 109, 85–98. [Google Scholar] [CrossRef] [PubMed]
- Murata, R.; Ohtori, S.; Ochiai, N.; Takahashi, N.; Saisu, T.; Moriya, H.; Takahashi, K.; Wada, Y. Extracorporeal shockwaves induce the expression of ATF3 and GAP-43 in rat dorsal root ganglion neurons. Auton. Neurosci. 2006, 128, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Hercher, D.; Redl, H.; Schuh, C. Motor and sensory Schwann cell phenotype commitment is diminished by extracorporeal shockwave treatment in vitro. J. Peripher. Nerv. Syst. 2020, 25, 32–43. [Google Scholar] [CrossRef] [PubMed]
- Schuh, C.M.; Hausner, T.; Redl, H.R. A therapeutic shock propels Schwann cells to proliferate in peripheral nerve injury. Brain Circ. 2016, 2, 138–140. [Google Scholar] [CrossRef]
- Wang, B.; Ning, H.; Reed-Maldonado, A.B.; Zhou, J.; Ruan, Y.; Zhou, T.; Wang, H.S.; Oh, B.S.; Banie, L.; Lin, G.; et al. Low-Intensity Extracorporeal Shock Wave Therapy Enhances Brain-Derived Neurotrophic Factor Expression through PERK/ATF4 Signaling Pathway. Int. J. Mol. Sci. 2017, 18, 433. [Google Scholar] [CrossRef]
- Hausner, T.; Pajer, K.; Halat, G.; Hopf, R.; Schmidhammer, R.; Redl, H.; Nogradi, A. Improved rate of peripheral nerve regeneration induced by extracorporeal shock wave treatment in the rat. Exp. Neurol. 2012, 236, 363–370. [Google Scholar] [CrossRef]
- Irintchev, A. Potentials and limitations of peripheral nerve injury models in rodents with particular reference to the femoral nerve. Ann. Anat. 2011, 193, 276–285. [Google Scholar] [CrossRef]
- Haastert-Talini, K. Appropriate Animal Models for Translational Nerve Research. In Peripheral Nerve Tissue Engineering and Regeneration; Phillips, J., Hercher, D., Hausner, T., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 1–17. [Google Scholar]
- Haastert-Talini, K. Peripheral Nerve Tissue Engineering: An Outlook on Experimental Concepts. In Modern Concepts of Peripheral Nerve Repair; Haastert-Talini, K., Assmus, H., Antoniadis, G., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 127–138. [Google Scholar]
- de Ruiter, G.C.; Spinner, R.J.; Verhaagen, J.; Malessy, M.J. Misdirection and guidance of regenerating axons after experimental nerve injury and repair. J. Neurosurg. 2014, 120, 493–501. [Google Scholar] [CrossRef]
- Dellon, A.L.; Mackinnon, S.E. Sciatic nerve regeneration in the rat. Validity of walking track assessment in the presence of chronic contractures. Microsurgery 1989, 10, 220–225. [Google Scholar] [CrossRef]
- Heinzel, J.C.; Hercher, D.; Redl, H. The course of recovery of locomotor function over a 10-week observation period in a rat model of femoral nerve resection and autograft repair. Brain Behav. 2020, 10, e01580. [Google Scholar] [CrossRef]
- Bertelli, J.A.; Taleb, M.; Saadi, A.; Mira, J.C.; Pecot-Dechavassine, M. The rat brachial plexus and its terminal branches: An experimental model for the study of peripheral nerve regeneration. Microsurgery 1995, 16, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Bertelli, J.A.; Orsal, D.; Mira, J.C. Median nerve neurotization by peripheral nerve grafts directly implanted into the spinal cord: Anatomical, behavioural and electrophysiological evidences of sensorimotor recovery. Brain Res. 1994, 644, 150–159. [Google Scholar] [CrossRef]
- Ronchi, G.; Morano, M.; Fregnan, F.; Pugliese, P.; Crosio, A.; Tos, P.; Geuna, S.; Haastert-Talini, K.; Gambarotta, G. The Median Nerve Injury Model in Pre-clinical Research—A Critical Review on Benefits and Limitations. Front. Cell. Neurosci. 2019, 13, 288. [Google Scholar] [CrossRef] [PubMed]
- Papalia, I.; Tos, P.; Stagno d’Alcontres, F.; Battiston, B.; Geuna, S. On the use of the grasping test in the rat median nerve model: A re-appraisal of its efficacy for quantitative assessment of motor function recovery. J. Neurosci. Methods 2003, 127, 43–47. [Google Scholar] [CrossRef]
- Stößel, M.; Rehra, L.; Haastert-Talini, K. Reflex-based grasping, skilled forelimb reaching, and electrodiagnostic evaluation for comprehensive analysis of functional recovery-The 7-mm rat median nerve gap repair model revisited. Brain Behav. 2017, 7, e00813. [Google Scholar] [CrossRef]
- Heinzel, J.C.; Oberhauser, V.; Keibl, C.; Swiadek, N.; Längle, G.; Frick, H.; Kolbenschlag, J.; Prahm, C.; Grillari, J.; Hercher, D. Evaluation of Functional Recovery in Rats After Median Nerve Resection and Autograft Repair Using Computerized Gait Analysis. Front. Neurosci. 2021, 14, 593545. [Google Scholar] [CrossRef]
- Daeschler, S.C.; Harhaus, L.; Bergmeister, K.D.; Boecker, A.; Hoener, B.; Kneser, U.; Schoenle, P. Clinically Available Low Intensity Ultrasound. Devices do not Promote Axonal Regeneration After Peripheral Nerve Surgery-A Preclinical Investigation of an FDA-Approved Device. Front. Neurol. 2018, 9, 1057. [Google Scholar] [CrossRef]
- Casal, D.; Mota-Silva, E.; Iria, I.; Pais, D.; Farinho, A.; Alves, S.; Pen, C.; Mascarenhas-Lemos, L.; Ferreira-Silva, J.; Ferraz-Oliveira, M.; et al. Functional and Physiological Methods of Evaluating Median Nerve Regeneration in the Rat. JoVE 2020, 158, e59767. [Google Scholar] [CrossRef]
- Ahmad, I.; Mir, M.A.; Khan, A.H. An Evaluation of Different Bridging Techniques for Short Nerve Gaps. Ann. Plast. Surg. 2017, 79, 482–485. [Google Scholar] [CrossRef]
- Manoli, T.; Schulz, L.; Stahl, S.; Jaminet, P.; Schaller, H.E. Evaluation of sensory recovery after reconstruction of digital nerves of the hand using muscle-in-vein conduits in comparison to nerve suture or nerve autografting. Microsurgery 2014, 34, 608–615. [Google Scholar] [CrossRef] [PubMed]
- Ederer, I.A.; Mayer, J.A.; Heinzel, J.; Kolbenschlag, J.; Daigeler, A.; Wahler, T. Outcome After Reconstruction of 43 Digital Nerve Defects With Muscle-in-Vein Conduits. J. Hand Surg. 2022, in press. [Google Scholar] [CrossRef] [PubMed]
- Heinzel, J.C.; Quyen Nguyen, M.; Kefalianakis, L.; Prahm, C.; Daigeler, A.; Hercher, D.; Kolbenschlag, J. A systematic review and meta-analysis of studies comparing muscle-in-vein conduits with autologous nerve grafts for nerve reconstruction. Sci. Rep. 2021, 11, 11691. [Google Scholar] [CrossRef] [PubMed]
- Bertelli, J.A.; Mira, J.C. The grasping test: A simple behavioral method for objective quantitative assessment of peripheral nerve regeneration in the rat. J. Neurosci. Methods 1995, 58, 151–155. [Google Scholar] [CrossRef]
- Heinzel, J.; Langle, G.; Oberhauser, V.; Hausner, T.; Kolbenschlag, J.; Prahm, C.; Grillari, J.; Hercher, D. Use of the CatWalk gait analysis system to assess functional recovery in rodent models of peripheral nerve injury—A systematic review. J. Neurosci. Methods 2020, 345, 108889. [Google Scholar] [CrossRef]
- Heinzel, J.; Swiadek, N.; Ashmwe, M.; Ruhrnossl, A.; Oberhauser, V.; Kolbenschlag, J.; Hercher, D. Automated Gait Analysis to Assess Functional Recovery in Rodents with Peripheral Nerve or Spinal Cord Contusion Injury. J. Vis Exp. 2020, 164, e61852. [Google Scholar] [CrossRef]
- Hromada, C.; Hartmann, J.; Oesterreicher, J.; Stoiber, A.; Daerr, A.; Schädl, B.; Priglinger, E.; Teuschl-Woller, A.H.; Holnthoner, W.; Heinzel, J.; et al. Occurrence of Lymphangiogenesis in Peripheral Nerve Autografts Contrasts Schwann Cell-Induced Apoptosis of Lymphatic Endothelial Cells In Vitro. Biomolecules 2022, 12, 820. [Google Scholar] [CrossRef]
- Turgut, M.C.; Saglam, G.; Toy, S. Efficacy of extracorporeal shock wave therapy for pillar pain after open carpal tunnel release: A double-blind, randomized, sham-controlled study. Korean J. Pain 2021, 34, 315–321. [Google Scholar] [CrossRef]
- Li, W.; Dong, C.; Wei, H.; Xiong, Z.; Zhang, L.; Zhou, J.; Wang, Y.; Song, J.; Tan, M. Extracorporeal shock wave therapy versus local corticosteroid injection for the treatment of carpal tunnel syndrome: A meta-analysis. J. Orthop. Surg. Res. 2020, 15, 556. [Google Scholar] [CrossRef]
- Chang, C.Y.; Chen, L.C.; Chou, Y.C.; Li, T.Y.; Ho, T.Y.; Wu, Y.T. The Effectiveness of Platelet-Rich Plasma and Radial Extracorporeal Shock Wave Compared with Platelet-Rich Plasma in the Treatment of Moderate Carpal Tunnel Syndrome. Pain Med. 2020, 21, 1668–1675. [Google Scholar] [CrossRef]
- Xu, D.; Ma, W.; Jiang, W.; Hu, X.; Jiang, F.; Mao, C.; Wang, Y.; Fang, L.; Luo, N.; Li, H.; et al. A randomized controlled trial: Comparing extracorporeal shock wave therapy versus local corticosteroid injection for the treatment of carpal tunnel syndrome. Int. Orthop. 2020, 44, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Leister, I.; Mittermayr, R.; Mattiassich, G.; Aigner, L.; Haider, T.; Machegger, L.; Kindermann, H.; Grazer-Horacek, A.; Holfeld, J.; Schaden, W. The effect of extracorporeal shock wave therapy in acute traumatic spinal cord injury on motor and sensory function within 6 months post-injury: A study protocol for a two-arm three-stage adaptive, prospective, multi-center, randomized, blinded, placebo-controlled clinical trial. Trials 2022, 23, 245. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, M.; Kanno, H.; Sugaya, T.; Yamaya, S.; Yahata, K.; Handa, K.; Shindo, T.; Shimokawa, H.; Ozawa, H.; Itoi, E. Low-energy extracorporeal shock wave therapy promotes BDNF expression and improves functional recovery after spinal cord injury in rats. Exp. Neurol. 2020, 328, 113251. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Jiang, Y.; Jiang, Z.; Han, L. Effect of low-energy extracorporeal shock wave on vascular regeneration after spinal cord injury and the recovery of motor function. Neuropsychiatr. Dis. Treat. 2016, 12, 2189–2198. [Google Scholar] [CrossRef] [PubMed]
- Yahata, K.; Kanno, H.; Ozawa, H.; Yamaya, S.; Tateda, S.; Ito, K.; Shimokawa, H.; Itoi, E. Low-energy extracorporeal shock wave therapy for promotion of vascular endothelial growth factor expression and angiogenesis and improvement of locomotor and sensory functions after spinal cord injury. J. Neurosurg. Spine 2016, 25, 745–755. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, S.G. Effects of extracorporeal shock wave therapy on functional recovery and neurotrophin-3 expression in the spinal cord after crushed sciatic nerve injury in rats. Ultrasound. Med. Biol. 2015, 41, 790–796. [Google Scholar] [CrossRef]
- Seo, M.; Lim, D.; Kim, S.; Kim, T.; Kwon, B.S.; Nam, K. Effect of Botulinum Toxin Injection and Extracorporeal Shock Wave Therapy on Nerve Regeneration in Rats with Experimentally Induced Sciatic Nerve Injury. Toxins 2021, 13, 879. [Google Scholar] [CrossRef]
- Lee, J.H.; Cho, S.H. Effect of extracorporeal shock wave therapy on denervation atrophy and function caused by sciatic nerve injury. J. Phys. Sci. 2013, 25, 1067–1069. [Google Scholar] [CrossRef][Green Version]
- Kaplan, H.M.; Mishra, P.; Kohn, J. The overwhelming use of rat models in nerve regeneration research may compromise designs of nerve guidance conduits for humans. J. Mater. Sci. Mater. Med. 2015, 26, 226. [Google Scholar] [CrossRef]
- Schiefer, J.L.; Schulz, L.; Rath, R.; Stahl, S.; Schaller, H.E.; Manoli, T. Comparison of short- with long-term regeneration results after digital nerve reconstruction with muscle-in-vein conduits. Neural Regen. Res. 2015, 10, 1674–1677. [Google Scholar] [CrossRef]
- Stößel, M.; Wildhagen, V.M.; Helmecke, O.; Metzen, J.; Pfund, C.B.; Freier, T.; Haastert-Talini, K. Comparative Evaluation of Chitosan Nerve Guides with Regular or Increased Bendability for Acute and Delayed Peripheral Nerve Repair: A Comprehensive Comparison with Autologous Nerve Grafts and Muscle-in-Vein Grafts. Anat. Rec. 2018, 301, 1697–1713. [Google Scholar] [CrossRef]
- Yamaya, S.; Ozawa, H.; Kanno, H.; Kishimoto, K.N.; Sekiguchi, A.; Tateda, S.; Yahata, K.; Ito, K.; Shimokawa, H.; Itoi, E. Low-energy extracorporeal shock wave therapy promotes vascular endothelial growth factor expression and improves locomotor recovery after spinal cord injury. J. Neurosurg. 2014, 121, 1514–1525. [Google Scholar] [CrossRef] [PubMed]
- Geuna, S.; Tos, P.; Raimondo, S.; Lee, J.M.; Gambarotta, G.; Nicolino, S.; Fornaro, M.; Papalia, I.; Perroteau, I.; Battiston, B. Functional, morphological and biomolecular assessment of posttraumatic neuro-muscular recovery in the rat forelimb model. Acta Neurochir. Suppl. 2007, 100, 173–177. [Google Scholar]
- Hamers, F.P.; Lankhorst, A.J.; van Laar, T.J.; Veldhuis, W.B.; Gispen, W.H. Automated quantitative gait analysis during overground locomotion in the rat: Its application to spinal cord contusion and transection injuries. J. Neurotrauma 2001, 18, 187–201. [Google Scholar] [CrossRef] [PubMed]
- Joosten, E.A.; Veldhuis, W.B.; Hamers, F.P. Collagen containing neonatal astrocytes stimulates regrowth of injured fibers and promotes modest locomotor recovery after spinal cord injury. J. Neurosci. Res. 2004, 77, 127–142. [Google Scholar] [CrossRef] [PubMed]
- Datto, J.P.; Shah, A.K.; Bastidas, J.C.; Arheart, K.L.; Marcillo, A.E.; Dietrich, W.D.; Pearse, D.D. Use of the CatWalk Gait Device to Assess Differences in Locomotion between Genders in Rats Inherently and following Spinal Cord Injury. Dataset Pap. Sci. 2016, 2016, 11. [Google Scholar] [CrossRef]
- Deumens, R.; Jaken, R.J.; Marcus, M.A.; Joosten, E.A. The CatWalk gait analysis in assessment of both dynamic and static gait changes after adult rat sciatic nerve resection. J. Neurosci. Methods 2007, 164, 120–130. [Google Scholar] [CrossRef]
- Bozkurt, A.; Deumens, R.; Scheffel, J.; O'Dey, D.M.; Weis, J.; Joosten, E.A.; Fuhrmann, T.; Brook, G.A.; Pallua, N. CatWalk gait analysis in assessment of functional recovery after sciatic nerve injury. J. Neurosci. Methods 2008, 173, 91–98. [Google Scholar] [CrossRef]
- Cobianchi, S.; de Cruz, J.; Navarro, X. Assessment of sensory thresholds and nociceptive fiber growth after sciatic nerve injury reveals the differential contribution of collateral reinnervation and nerve regeneration to neuropathic pain. Exp. Neurol. 2014, 255, 1–11. [Google Scholar] [CrossRef]
- Casal, D.; Mota-Silva, E.; Iria, I.; Alves, S.; Farinho, A.; Pen, C.; Lourenco-Silva, N.; Mascarenhas-Lemos, L.; Silva-Ferreira, J.; Ferraz-Oliveira, M.; et al. Reconstruction of a 10-mm-long median nerve gap in an ischemic environment using autologous conduits with different patterns of blood supply: A comparative study in the rat. PLoS ONE 2018, 13, e0195692. [Google Scholar] [CrossRef]
- Mittermayr, R.; Antonic, V.; Hartinger, J.; Kaufmann, H.; Redl, H.; Teot, L.; Stojadinovic, A.; Schaden, W. Extracorporeal shock wave therapy (ESWT) for wound healing: Technology, mechanisms, and clinical efficacy. Wound Repair Regen. 2012, 20, 456–465. [Google Scholar] [CrossRef] [PubMed]
- Hausdorf, J.; Lemmens, M.A.; Heck, K.D.; Grolms, N.; Korr, H.; Kertschanska, S.; Steinbusch, H.W.; Schmitz, C.; Maier, M. Selective loss of unmyelinated nerve fibers after extracorporeal shockwave application to the musculoskeletal system. Neuroscience 2008, 155, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Arcilla, C.K.; Tadi, P. Neuroanatomy, Unmyelinated Nerve Fibers. In StatPearls; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2022. [Google Scholar]
- Ohtori, S.; Inoue, G.; Mannoji, C.; Saisu, T.; Takahashi, K.; Mitsuhashi, S.; Wada, Y.; Takahashi, K.; Yamagata, M.; Moriya, H. Shock wave application to rat skin induces degeneration and reinnervation of sensory nerve fibres. Neurosci. Lett. 2001, 315, 57–60. [Google Scholar] [CrossRef]
- Zucal, I.; Mihic-Probst, D.; Pignet, A.L.; Calcagni, M.; Giovanoli, P.; Frueh, F.S. Intraneural fibrosis and loss of microvascular architecture—Key findings investigating failed human nerve allografts. Ann. Anat. 2022, 239, 151810. [Google Scholar] [CrossRef]
- Saffari, S.; Saffari, T.M.; Ulrich, D.J.O.; Hovius, S.E.R.; Shin, A.Y. The interaction of stem cells and vascularity in peripheral nerve regeneration. Neural Regen. Res. 2021, 16, 1510–1517. [Google Scholar] [CrossRef]
- Masgutov, R.; Zeinalova, A.; Bogov, A.; Masgutova, G.; Salafutdinov, I.; Garanina, E.; Syromiatnikova, V.; Idrisova, K.; Mullakhmetova, A.; Andreeva, D.; et al. Angiogenesis and nerve regeneration induced by local administration of plasmid pBud-coVEGF165-coFGF2 into the intact rat sciatic nerve. Neural Regen. Res. 2021, 16, 1882–1889. [Google Scholar] [CrossRef] [PubMed]
- Prahm, C.; Heinzel, J.; Kolbenschlag, J. Blood Supply and Microcirculation of the Peripheral Nerve. In Peripheral Nerve Tissue Engineering and Regeneration; Phillips, J., Hercher, D., Hausner, T., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 1–46. [Google Scholar]
- Saffari, T.M.; Mathot, F.; Friedrich, P.F.; Bishop, A.T.; Shin, A.Y. Surgical Angiogenesis of Decellularized Nerve Allografts Improves Early Functional Recovery in a Rat Sciatic Nerve Defect Model. Plast. Reconstr. Surg. 2021, 148, 561–570. [Google Scholar] [CrossRef]
- Saffari, T.M.; Mathot, F.; Thaler, R.; van Wijnen, A.J.; Bishop, A.T.; Shin, A.Y. Microcomputed analysis of nerve angioarchitecture after combined stem cell delivery and surgical angiogenesis to nerve allograft. J. Plast. Reconstr. Aesthetic Surg. 2021, 74, 1919–1930. [Google Scholar] [CrossRef]
- Saffari, T.M.; Badreldin, A.; Mathot, F.; Bagheri, L.; Bishop, A.T.; van Wijnen, A.J.; Shin, A.Y. Surgical angiogenesis modifies the cellular environment of processed nerve allografts in a rat sciatic nerve defect model. Gene 2020, 751, 144711. [Google Scholar] [CrossRef]
- Saffari, T.M.; Mathot, F.; Bishop, A.T.; Shin, A.Y. New methods for objective angiogenesis evaluation of rat nerves using microcomputed tomography scanning and conventional photography. Microsurgery 2020, 40, 370–376. [Google Scholar] [CrossRef]
- Saffari, T.M.; Mathot, F.; Friedrich, P.F.; Bishop, A.T.; Shin, A.Y. Revascularization patterns of nerve allografts in a rat sciatic nerve defect model. J. Plast. Reconstr. Aesthetic Surg. 2020, 73, 460–468. [Google Scholar] [CrossRef] [PubMed]
- Saffari, T.M.; Bedar, M.; Hundepool, C.A.; Bishop, A.T.; Shin, A.Y. The role of vascularization in nerve regeneration of nerve graft. Neural Regen. Res. 2020, 15, 1573–1579. [Google Scholar] [CrossRef] [PubMed]
- Mathot, F.; Rbia, N.; Bishop, A.T.; Hovius, S.E.R.; Shin, A.Y. Adipose derived mesenchymal stem cells seeded onto a decellularized nerve allograft enhances angiogenesis in a rat sciatic nerve defect model. Microsurgery 2020, 40, 585–592. [Google Scholar] [CrossRef] [PubMed]
- Muangsanit, P.; Shipley, R.J.; Phillips, J.B. Vascularization Strategies for Peripheral Nerve Tissue Engineering. Anat. Rec. 2018, 301, 1657–1667. [Google Scholar] [CrossRef]
- Harwood, A.E.; Green, J.; Cayton, T.; Raza, A.; Wallace, T.; Carradice, D.; Chetter, I.C.; Smith, G.E. A feasibility double-blind randomized placebo-controlled trial of extracorporeal shockwave therapy as a novel treatment for intermittent claudication. J. Vasc. Surg. 2018, 67, 514–521.e2. [Google Scholar] [CrossRef]
- Cayton, T.; Harwood, A.; Smith, G.E.; Chetter, I. A Systematic Review of Extracorporeal Shockwave Therapy as a Novel Treatment for Intermittent Claudication. Ann. Vasc. Surg. 2016, 35, 226–233. [Google Scholar] [CrossRef]
- Leu, S.; Huang, T.H.; Chen, Y.L.; Yip, H.K. Effect of Extracorporeal Shockwave on Angiogenesis and Anti-Inflammation: Molecular-Cellular Signaling Pathways. Transl. Res. Biomed. 2017, 6, 109–116. [Google Scholar] [CrossRef]
- Frueh, F.S.; Gousopoulos, E.; Power, D.M.; Ampofo, E.; Giovanoli, P.; Calcagni, M.; Laschke, M.W. A potential role of lymphangiogenesis for peripheral nerve injury and regeneration. Med. Hypotheses 2020, 135, 109470. [Google Scholar] [CrossRef]
- Meng, F.W.; Jing, X.N.; Song, G.H.; Jie, L.L.; Shen, F.F. Prox1 induces new lymphatic vessel formation and promotes nerve reconstruction in a mouse model of sciatic nerve crush injury. J. Anat. 2020, 237, 933–940. [Google Scholar] [CrossRef]
- Chen, B.; Chen, Q.; Parkinson, D.B.; Dun, X.-P. Analysis of Schwann Cell Migration and Axon Regeneration Following Nerve Injury in the Sciatic Nerve Bridge. Front. Mol. Neurosci. 2019, 12, 308. [Google Scholar] [CrossRef]
- Saio, S.; Konishi, K.; Hohjoh, H.; Tamura, Y.; Masutani, T.; Iddamalgoda, A.; Ichihashi, M.; Hasegawa, H.; Mizutani, K.I. Extracellular Environment-Controlled Angiogenesis, and Potential Application for Peripheral Nerve Regeneration. Int. J. Mol. Sci. 2021, 22, 11169. [Google Scholar] [CrossRef] [PubMed]
- Geuna, S.; Tos, P.; Battiston, B.; Giacobini-Robecchi, M.G. Bridging peripheral nerve defects with muscle-vein combined guides. Neurol. Res. 2004, 26, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Schuh, C.M.; Hercher, D.; Stainer, M.; Hopf, R.; Teuschl, A.H.; Schmidhammer, R.; Redl, H. Extracorporeal shockwave treatment: A novel tool to improve Schwann cell isolation and culture. Cytotherapy 2016, 18, 760–770. [Google Scholar] [CrossRef] [PubMed]
- Park, K.D.; Lee, W.Y.; Park, M.H.; Ahn, J.K.; Park, Y. High- versus low-energy extracorporeal shock-wave therapy for myofascial pain syndrome of upper trapezius: A prospective randomized single blinded pilot study. Medicine 2018, 97, e11432. [Google Scholar] [CrossRef] [PubMed]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| WPO1 | |||||||
| Ability | 1/3 | 2/3 | 3/3 | vs. ANG | vs. MVC | vs. ANG + ESWT | vs. MVC + ESWT |
| ANG | 3/3 (100%) | 0/3 (0%) | 0/3 (0%) | n. s. | n. s. | n. s. | |
| MVC | 5/5 (100%) | 0/5 (0%) | 0/5 (0%) | n. s. | n. s. | n. s. | |
| ANG + ESWT | 6/6 (100%) | 0/6 (0%) | 0/6 (0%) | n. s. | n. s. | n. s. | |
| MVC + ESWT | 7/7 (100%) | 0/7 (0%) | 0/7 (0%) | n. s. | n. s. | n. s. | |
| WPO2 | |||||||
| Ability | 1/3 | 2/3 | 3/3 | vs. ANG | vs. MVC | vs. ANG + ESWT | vs. MVC + ESWT |
| ANG | 3/3 (100%) | 0/3 (0%) | 0/3 (0%) | n. s. | n. s. | n. s. | |
| MVC | 5/5 (100%) | 0/5 (0%) | 0/5 (0%) | n. s. | n. s. | n. s. | |
| ANG + ESWT | 6/6 (100%) | 0/6 (0%) | 0/6 (0%) | n. s. | n. s. | n. s. | |
| MVC + ESWT | 7/7 (100%) | 0/7 (0%) | 0/7 (0%) | n. s. | n. s. | n. s. | |
| WPO3 | |||||||
| Ability | 1/3 | 2/3 | 3/3 | vs. ANG | vs. MVC | vs. ANG + ESWT | vs. MVC + ESWT |
| ANG | 3/3 (100%) | 0/3 (0%) | 0/3 (0%) | n. s. | n. s. | n. s. | |
| MVC | 5/5 (100%) | 0/5 (0%) | 0/5 (0%) | n. s. | n. s. | n. s. | |
| ANG + ESWT | 5/6 (83.3%) | 1/6 (16.7%) | 0/6 (0%) | n. s. | n. s. | n. s. | |
| MVC + ESWT | 7/7 (100%) | 0/7 (0%) | 0/7 (0%) | n. s. | n. s. | n. s. | |
| WPO4 | |||||||
| Ability | 1/3 | 2/3 | 3/3 | vs. ANG | vs. MVC | vs. ANG + ESWT | vs. MVC + ESWT |
| ANG | 0/3 (0%) | 2/3 (66%) | 1/3 (33%) | p < 0.05 | n. s. | p < 0.05 | |
| MVC | 5/5 (100%) | 0/5 (0%) | 0/5 (0%) | p < 0.05 | n. s. | n. s. | |
| ANG + ESWT | 3/6 (50%) | 2/6 (33.3%) | 1/6 (16.7%) | n. s. | n. s. | n. s. | |
| MVC + ESWT | 7/7 (100%) | 0/7 (0%) | 0/7 (0%) | p < 0.05 | n. s. | n. s. | |
| WPO5 | |||||||
| Ability | 1/3 | 2/3 | 3/3 | vs. ANG | vs. MVC | vs. ANG + ESWT | vs. MVC + ESWT |
| ANG | 0/3 (0%) | 1/3 (33.3%) | 2/3 (66.7%) | p < 0.05 | n. s. | p < 0.05 | |
| MVC | 5/5 (100%) | 0/5 (0%) | 0/5 (0%) | p < 0.05 | n. s. | n. s. | |
| ANG + ESWT | 2/6 (33.3%) | 2/6 (33.3%) | 2/6 (33.3%) | n. s. | n. s. | n. s. | |
| MVC + ESWT | 6/7 (85.7%) | 1/7 (14.3%) | 0/7 (0%) | n. s. | n. s. | p< 0.05 | |
| WPO6 | |||||||
| Ability | 1/3 | 2/3 | 3/3 | vs. ANG | vs. MVC | vs. ANG + ESWT | vs. MVC + ESWT |
| ANG | 0/3 (0%) | 0/3 (0%) | 3/3 (100%) | p < 0.05 | n. s. | p < 0.05 | |
| MVC | 5/5 (100%) | 0/5 (0%) | 0/5 (0%) | p < 0.05 | p < 0.05 | n. s. | |
| ANG + ESWT | 0/6 (0%) | 2/6 (33.3%) | 4/6 (66.7%) | n. s. | p< 0.05 | p < 0.05 | |
| MVC + ESWT | 6/7 (85.7%) | 1/7 (14.3%) | 0/7 (0%) | p < 0.05 | n. s. | p < 0.05 | |
| WPO7 | |||||||
| Ability | 1/3 | 2/3 | 3/3 | vs. ANG | vs. MVC | vs. ANG + ESWT | vs. MVC + ESWT |
| ANG | 0/3 (0%) | 0/3 (0%) | 3/3 (100%) | p < 0.05 | n. s. | n. s. | |
| MVC | 5/5 (100%) | 0/5 (0%) | 0/5 (0%) | p < 0.05 | p < 0.05 | n. s. | |
| ANG + ESWT | 0/6 (0%) | 2/6 (33.3%) | 4/6 (66.7%) | n. s. | p < 0.05 | n. s. | |
| MVC + ESWT | 5/7 (71.4%) | 1/7 (14.3%) | 1/7 (14.3%) | n. s. | n. s. | n. s. | |
| WPO8 | |||||||
| Ability | 1/3 | 2/3 | 3/3 | vs. ANG | vs. MVC | vs. ANG + ESWT | vs. MVC + ESWT |
| ANG | 0/3 (0%) | 0/3 (0%) | 3/3 (100%) | n. s. | n. s. | n. s. | |
| MVC | 4/5 (80%) | 1/5 (20%) | 0/5 (0%) | n. s. | p < 0.05 | n. s. | |
| ANG + ESWT | 0/6 (0%) | 1/6 (16.7%) | 5/6 (83.3%) | n. s. | p < 0.05 | n. s. | |
| MVC + ESWT | 4/7 (57.1%) | 1/7 (14.3%) | 2/7 (28.6%) | n. s. | n. s. | n. s. | |
| WPO9 | |||||||
| Ability | 1/3 | 2/3 | 3/3 | vs. ANG | vs. MVC | vs. ANG + ESWT | vs. MVC + ESWT |
| ANG | 0/3 (0%) | 0/3 (0%) | 3/3 (100%) | n. s. | n. s. | n. s. | |
| MVC | 4/5 (80%) | 1/5 (20%) | 0/5 (0%) | n. s. | p < 0.05 | n. s. | |
| ANG + ESWT | 0/6 (0%) | 0/6 (0%) | 6/6 (100%) | n. s. | p < 0.05 | n. s. | |
| MVC + ESWT | 4/7 (57.1%) | 0/7 (0%) | 33/7 (42.9%) | n. s. | n. s. | n. s. | |
| WPO10 | |||||||
| Ability | 1/3 | 2/3 | 3/3 | vs. ANG | vs. MVC | vs. ANG + ESWT | vs. MVC + ESWT |
| ANG | 0/3 (0%) | 0/3 (0%) | 3/3 (100%) | n. s. | n. s. | n. s. | |
| MVC | 3/5 (60%) | 1/5 (20%) | 1/5 (20%) | n. s. | n. s. | n. s. | |
| ANG + ESWT | 0/6 (0%) | 0/6 (0%) | 6/6 (100%) | n. s. | n. s. | n. s. | |
| MVC + ESWT | 4/7 (57.1%) | 0/7 (0%) | 33/7 (42.9%) | n. s. | n. s. | n. s. | |
| WPO11 | |||||||
| Ability | 1/3 | 2/3 | 3/3 | vs. ANG | vs. MVC | vs. ANG + ESWT | vs. MVC + ESWT |
| ANG | 0/3 (0%) | 0/3 (0%) | 3/3 (100%) | n. s. | n. s. | n. s. | |
| MVC | 3/5 (60%) | 0/5 (20%) | 2/5 (40%) | n. s. | n. s. | n. s. | |
| ANG + ESWT | 0/6 (0%) | 0/6 (0%) | 6/6 (100%) | n. s. | n. s. | n. s. | |
| MVC + ESWT | 3/7 (42.9%) | 1/7 (14.3%) | 3/7 (42.9%) | n. s. | n. s. | n. s. | |
| WPO12 | |||||||
| Ability | 1/3 | 2/3 | 3/3 | vs. ANG | vs. MVC | vs. ANG + ESWT | vs. MVC + ESWT |
| ANG | 0/3 (0%) | 0/3 (0%) | 3/3 (100%) | n. s. | n. s. | n. s. | |
| MVC | 3/5 (60%) | 0/5 (20%) | 2/5 (40%) | n. s. | n. s. | n. s. | |
| ANG + ESWT | 0/6 (0%) | 0/6 (0%) | 6/6 (100%) | n. s. | n. s. | n. s. | |
| MVC + ESWT | 1/7 (14.3%) | 3/7 (42.9%) | 3/7 (42.9%) | n. s. | n. s. | n. s. | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heinzel, J.C.; Oberhauser, V.; Keibl, C.; Schädl, B.; Swiadek, N.V.; Längle, G.; Frick, H.; Slezak, C.; Prahm, C.; Grillari, J.; et al. ESWT Diminishes Axonal Regeneration following Repair of the Rat Median Nerve with Muscle-In-Vein Conduits but Not after Autologous Nerve Grafting. Biomedicines 2022, 10, 1777. https://doi.org/10.3390/biomedicines10081777
Heinzel JC, Oberhauser V, Keibl C, Schädl B, Swiadek NV, Längle G, Frick H, Slezak C, Prahm C, Grillari J, et al. ESWT Diminishes Axonal Regeneration following Repair of the Rat Median Nerve with Muscle-In-Vein Conduits but Not after Autologous Nerve Grafting. Biomedicines. 2022; 10(8):1777. https://doi.org/10.3390/biomedicines10081777
Chicago/Turabian StyleHeinzel, Johannes C., Viola Oberhauser, Claudia Keibl, Barbara Schädl, Nicole V. Swiadek, Gregor Längle, Helen Frick, Cyrill Slezak, Cosima Prahm, Johannes Grillari, and et al. 2022. "ESWT Diminishes Axonal Regeneration following Repair of the Rat Median Nerve with Muscle-In-Vein Conduits but Not after Autologous Nerve Grafting" Biomedicines 10, no. 8: 1777. https://doi.org/10.3390/biomedicines10081777
APA StyleHeinzel, J. C., Oberhauser, V., Keibl, C., Schädl, B., Swiadek, N. V., Längle, G., Frick, H., Slezak, C., Prahm, C., Grillari, J., Kolbenschlag, J., & Hercher, D. (2022). ESWT Diminishes Axonal Regeneration following Repair of the Rat Median Nerve with Muscle-In-Vein Conduits but Not after Autologous Nerve Grafting. Biomedicines, 10(8), 1777. https://doi.org/10.3390/biomedicines10081777