
Percutaneous Endoscopic Interbody Debridement and Fusion (PEIDF) Decreases Risk of Sepsis and Mortality in Treating Infectious Spondylodiscitis for Patients with Poor Physical Status, a Retrospective Cohort Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
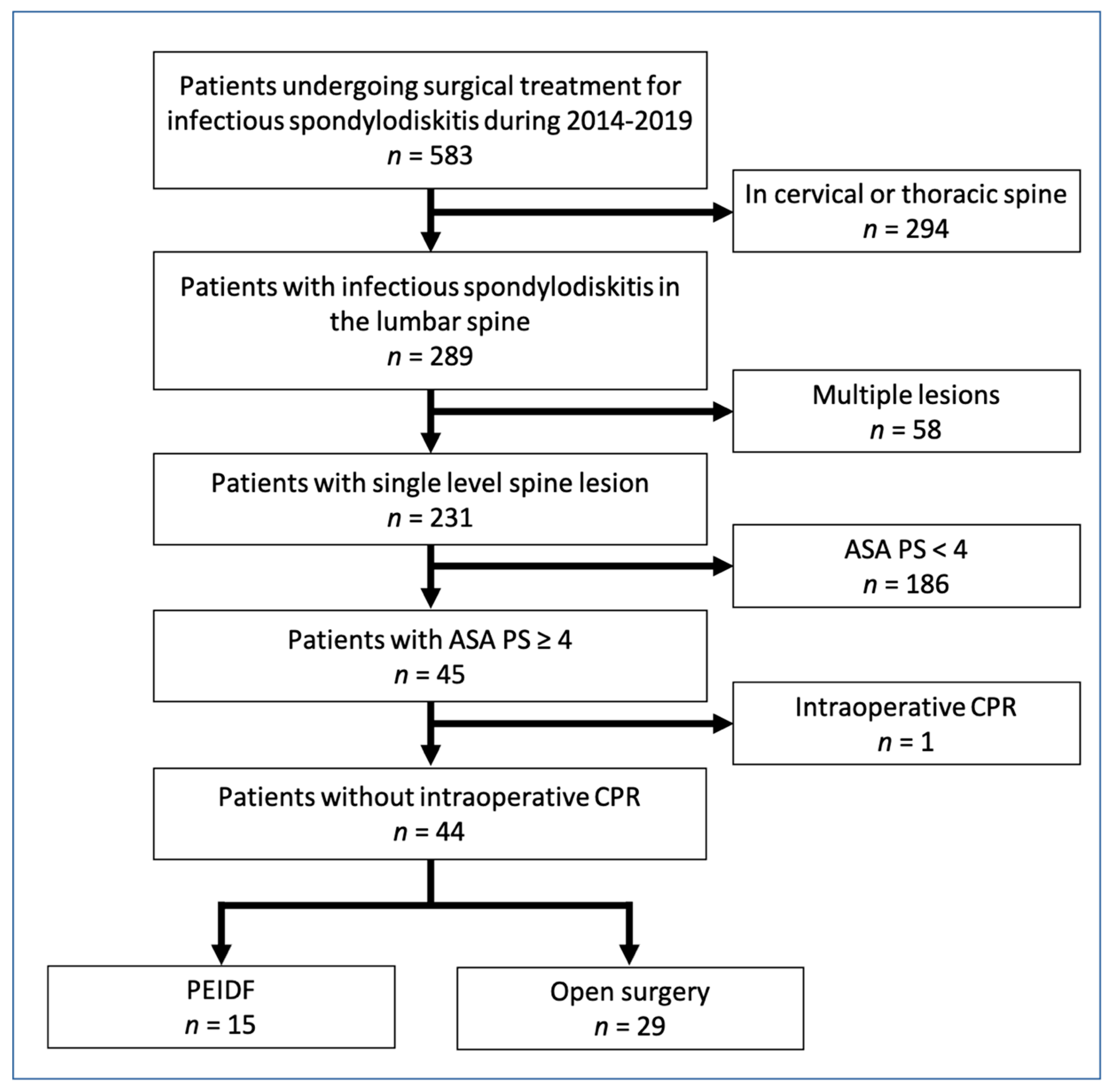
2.1. Study Population
2.2. Outcome Measurement and Data Collection
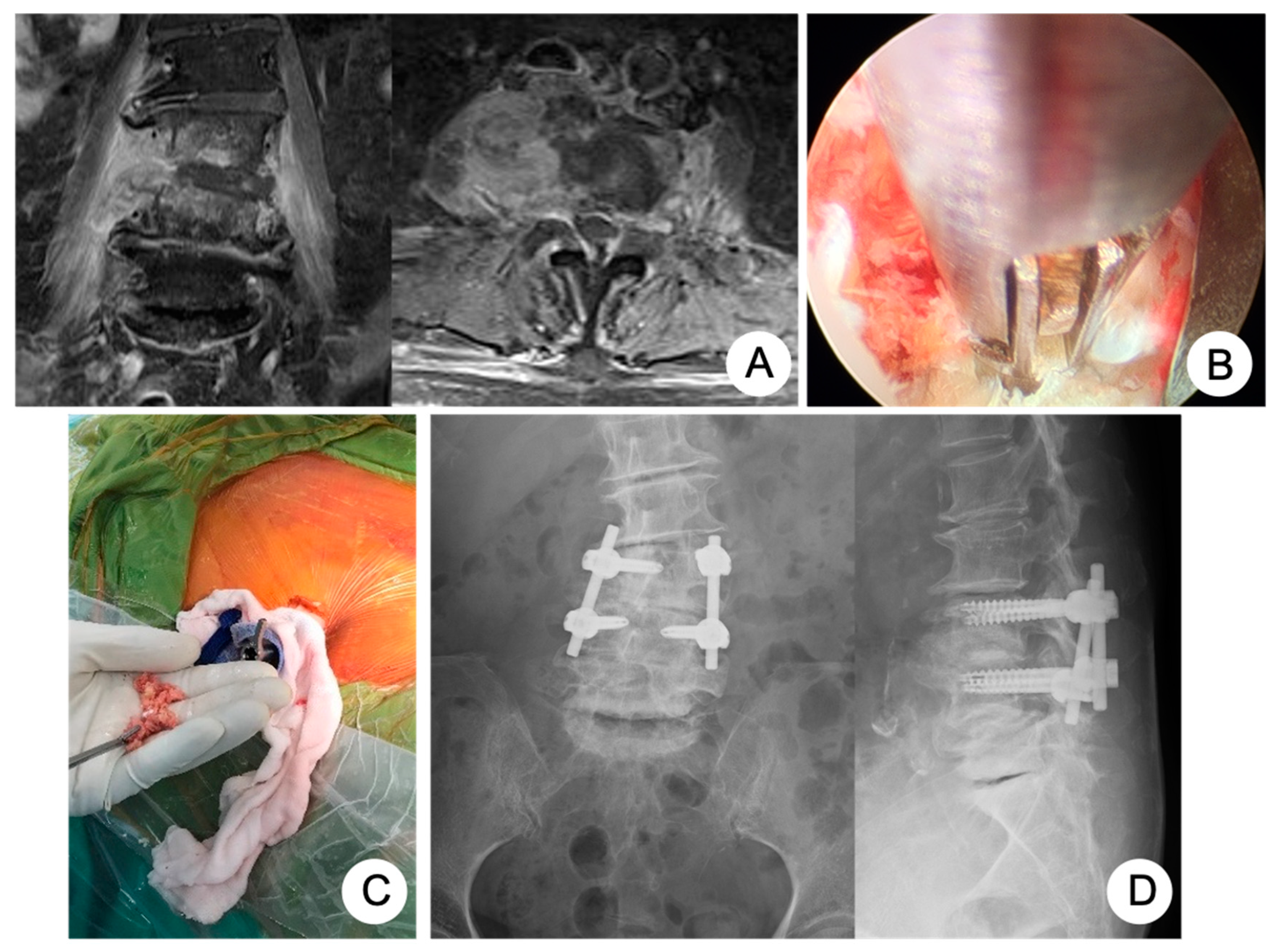
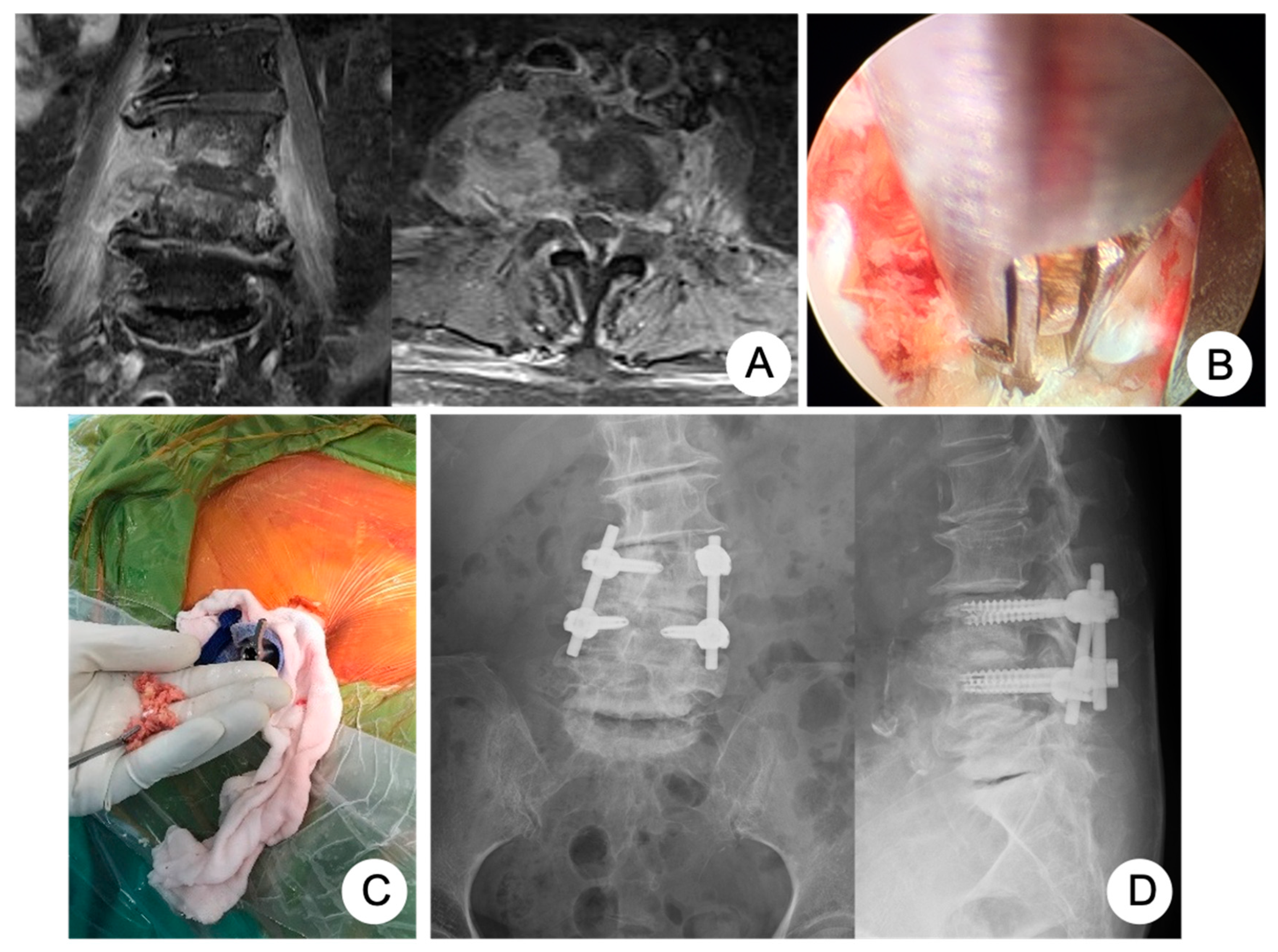
2.3. Surgical Techniques
2.3.1. PEIDF
2.3.2. Posterior Open Surgery
2.3.3. Anterior Open Surgery
2.3.4. Statistical Analysis
3. Results
3.1. Study Objects
3.2. Demographic and Clinical Data
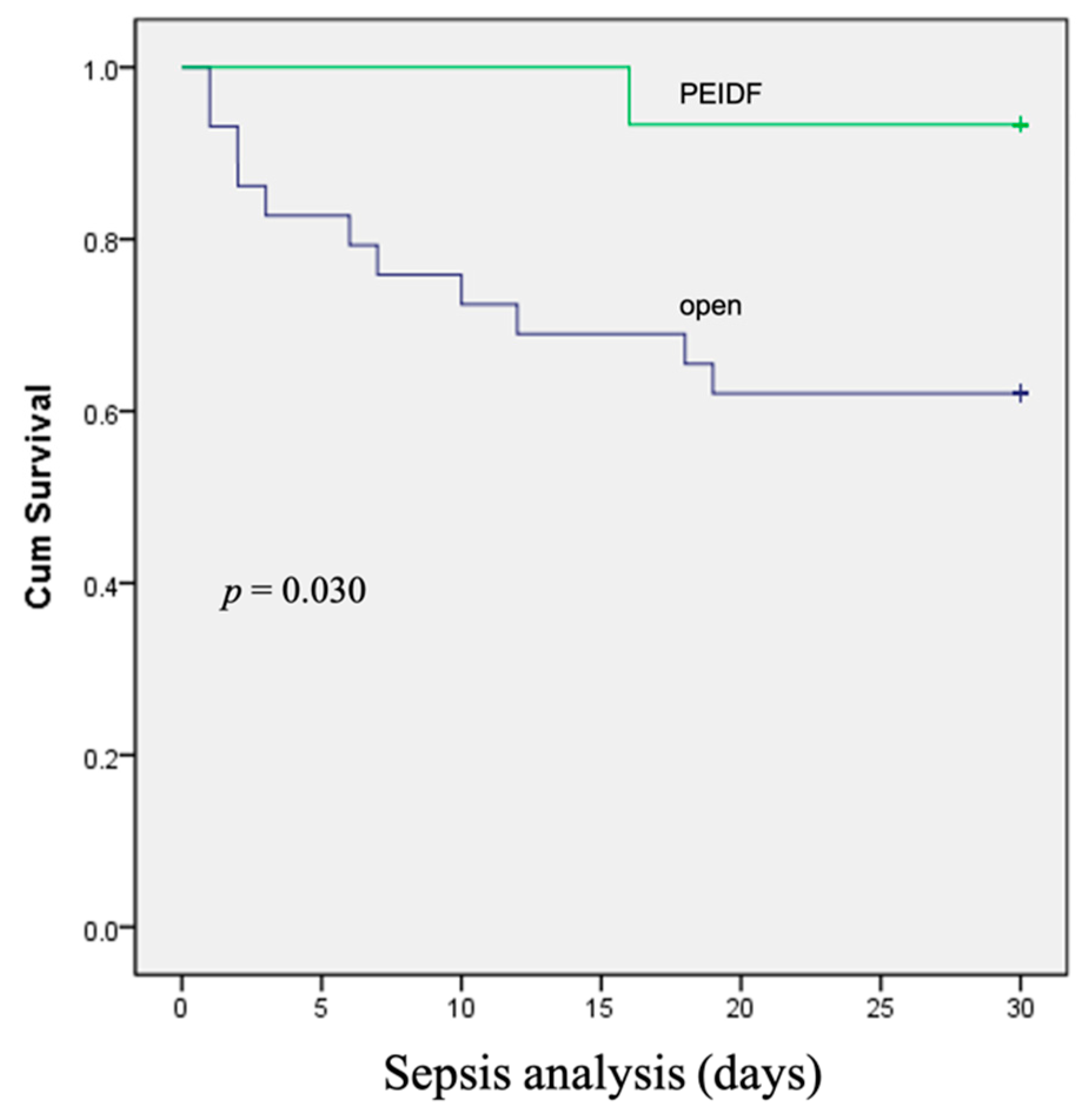
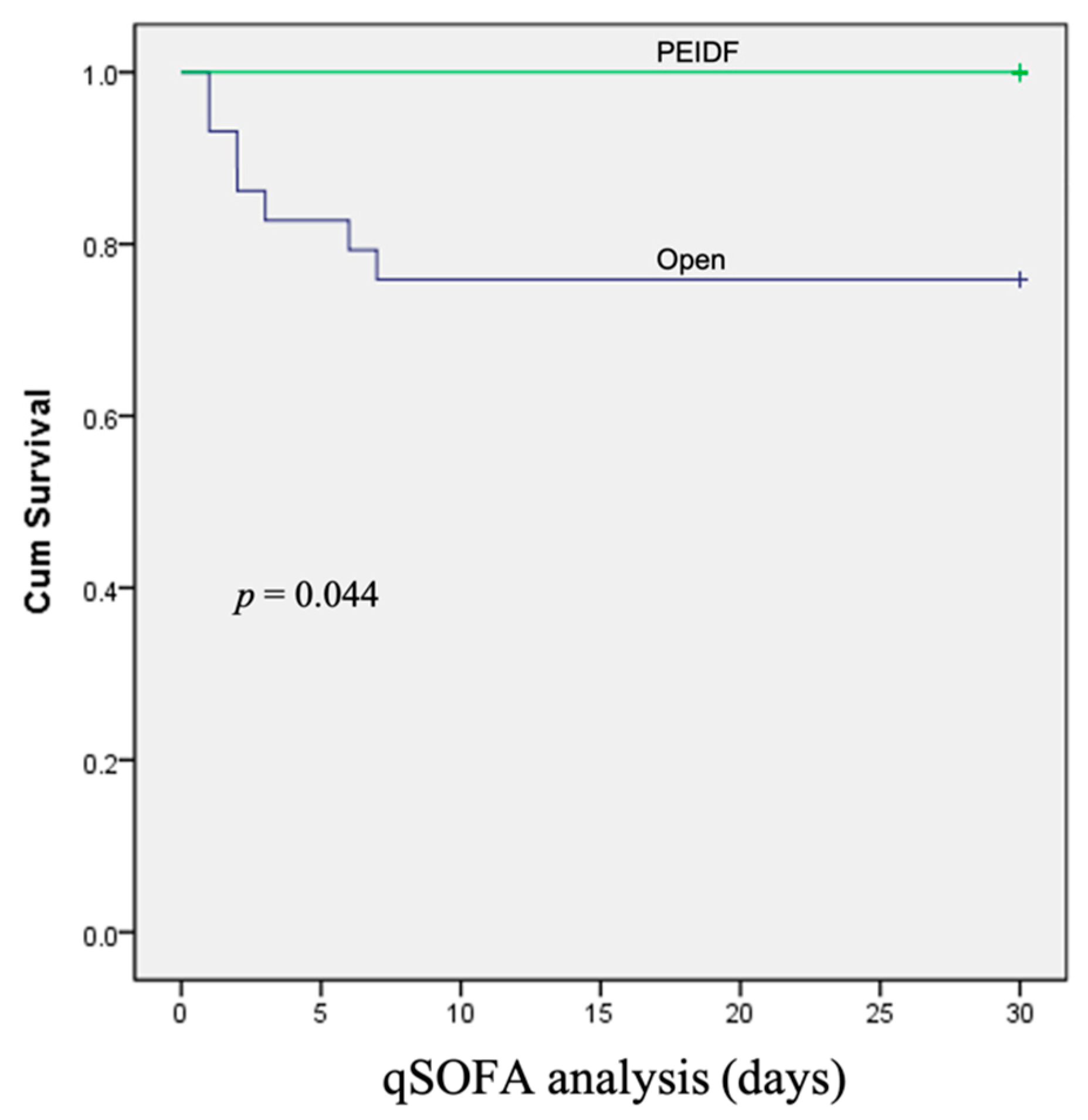
3.3. Outcome Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vogel, T.; Dombrovskiy, V.Y.; Carson, J.L.; Graham, A.M.; Lowry, S.F. Postoperative Sepsis in the United States. Ann. Surg. 2010, 252, 1065–1071. [Google Scholar] [CrossRef] [PubMed]
- Cecconi, M.; Evans, L.; Levy, M.; Rhodes, A. Sepsis and septic shock. Lancet 2018, 392, 75–87. [Google Scholar] [CrossRef]
- Faist, E.; Wichmann, M.; Kim, C. Immunosuppression and immunomodulation in surgical patients. Curr. Opin. Crit. Care 1997, 3, 293–298. [Google Scholar] [CrossRef]
- Glance, L.G.; Dick, A.W.; Mukamel, D.B.; Fleming, F.J.; Zollo, R.A.; Wissler, R.; Salloum, R.; Meredith, U.W.; Osler, T.M. Association between Intraoperative Blood Transfusion and Mortality and Morbidity in Patients Undergoing Noncardiac Surgery. Anesthesiology 2011, 114, 283–292. [Google Scholar] [CrossRef] [PubMed]
- Hotchkiss, R.S.; Karl, I.E. The Pathophysiology and Treatment of Sepsis. N. Engl. J. Med. 2003, 348, 138–150. [Google Scholar] [CrossRef] [PubMed]
- Fu, T.-S.; Yang, S.-C.; Tsai, T.-T.; Chen, L.-H.; Lai, P.-L.; Niu, C.-C.; Chen, W.-J. Percutaneous endoscopic debridement and drainage in immunocompromised patients with complicated infectious spondylitis. Minim. Invasive Ther. Allied Technol. 2010, 19, 42–47. [Google Scholar] [CrossRef]
- Griffith-Jones, W.; Nasto, L.A.; Pola, E.; Stokes, O.M.; Mehdian, H. Percutaneous suction and irrigation for the treatment of recalcitrant pyogenic spondylodiscitis. J. Orthop. Traumatol. 2018, 19, 10. [Google Scholar] [CrossRef]
- Lin, G.-X.; Kim, J.-S.; Sharma, S.; Sun, L.-W.; Wu, H.-H.; Chang, K.-S.; Chen, Y.-C.; Chen, C.-M. Full Endoscopic Discectomy, Debridement, and Drainage for High-Risk Patients with Spondylodiscitis. World Neurosurg. 2019, 127, e202–e211. [Google Scholar] [CrossRef]
- Lai, P.J.; Wang, S.F.; Tsai, T.T.; Li, Y.D.; Chiu, P.Y.; Hsieh, M.K.; Kao, F.C. Percutaneous Endoscopic Interbody Debridement and Fusion for Pyogenic Lumbar Spondylodiskitis: Surgical Technique and the Comparison With Percutaneous Endoscopic Drainage and Debridement. Neurospine 2021, 18, 891–902. [Google Scholar] [CrossRef]
- Mayhew, D.; Mendonca, V.; Murthy, B.V.S. A review of ASA physical status-historical perspectives and modern developments. Anaesthesia 2019, 74, 373–379. [Google Scholar] [CrossRef]
- Koch, C.; Edinger, F.; Fischer, T.; Brenck, F.; Hecker, A.; Katzer, C.; Markmann, M.; Sander, M.; Schneck, E. Comparison of qSOFA score, SOFA score, and SIRS criteria for the prediction of infection and mortality among surgical intermediate and intensive care patients. World J. Emerg. Surg. 2020, 15, 63. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.-C.; Chen, W.-J.; Chen, H.-S.; Kao, Y.-H.; Yu, S.-W.; Tu, Y.-K. Extended indications of percutaneous endoscopic lavage and drainage for the treatment of lumbar infectious spondylitis. Eur. Spine J. 2014, 23, 846–853. [Google Scholar] [CrossRef] [PubMed]
- Menges, P.; Kessler, W.; Kloecker, C.; Feuerherd, M.; Gaubert, S.; Diedrich, S.; van der Linde, J.; Hegenbart, A.; Busemann, A.; Traeger, T.; et al. Surgical Trauma and Postoperative Immune Dysfunction. Eur. Surg. Res. 2012, 48, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Schömig, F.; Bürger, J.; Hu, Z.; Pruß, A.; Klotz, E.; Pumberger, M.; Hipfl, C. Intraoperative blood loss as indicated by haemoglobin trend is a predictor for the development of postoperative spinal implant infection—A matched-pair analysis. J. Orthop. Surg. Res. 2021, 16, 393. [Google Scholar] [CrossRef]
- Veenhof, A.A.; Vlug, M.S.; van der Pas, M.H.; Sietses, C.; van der Peet, D.L.; De Lange-De Klerk ES, M.; Cuesta, M.A. Surgical stress response and postoperative immune function after laparoscopy or open surgery with fast track or standard perioperative care: A randomized trial. Ann. Surg. 2012, 255, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Zhou, K.; Lai, Y.; Shen, C.; Wu, Y.; Che, G. Estimated intraoperative blood loss correlates with postoperative cardiopulmonary complications and length of stay in patients undergoing video-assisted thoracoscopic lung cancer lobectomy: A retrospective cohort study. BMC Surg. 2018, 18, 29. [Google Scholar] [CrossRef]
- Dhabhar, F.S.; Miller, A.H.; McEwen, B.S.; Spencer, R.L. Stress-induced changes in blood leukocyte distribution. Role of adrenal steroid hormones. J. Immunol. 1996, 157, 1638–1644. [Google Scholar]
- Bartal, I.; Melamed, R.; Greenfeld, K.; Atzil, S.; Glasner, A.; Domankevich, V.; Naor, R.; Beilin, B.; Yardeni, I.Z.; Ben-Eliyahu, S. Immune perturbations in patients along the perioperative period: Alterations in cell surface markers and leukocyte subtypes before and after surgery. Brain Behav. Immun. 2010, 24, 376–386. [Google Scholar] [CrossRef]
- Angele, M.K.; Faist, E. Clinical review: Immunodepression in the surgical patient and increased susceptibility to infection. Crit. Care 2002, 6, 298–305. [Google Scholar] [CrossRef]
- Malone, D.L.; Dunne, J.; Tracy, J.K.; Putnam, A.T.; Scalea, T.M.; Napolitano, L.M. Blood Transfusion, Independent of Shock Severity, Is Associated with Worse Outcome in Trauma. J. Trauma 2003, 54, 898–907. [Google Scholar] [CrossRef]
- Vamvakas, E.C.; Blajchman, M.A. Transfusion-related immunomodulation (TRIM): An update. Blood Rev. 2007, 21, 327–348. [Google Scholar] [CrossRef]
- Hod, E.A.; Zhang, N.; Sokol, S.A.; Wojczyk, B.S.; Francis, R.O.; Ansaldi, D.; Francis, K.P.; Della-Latta, P.; Whittier, S.; Sheth, S.; et al. Transfusion of red blood cells after prolonged storage produces harmful effects that are mediated by iron and inflammation. Blood 2010, 115, 4284–4292. [Google Scholar] [CrossRef] [PubMed]
- Ganz, T. Iron and infection. Int. J. Hematol. 2018, 107, 7–15. [Google Scholar] [CrossRef]
- Kaufmann, S.H.; Dorhoi, A. Molecular Determinants in Phagocyte-Bacteria Interactions. Immunity 2016, 44, 476–491. [Google Scholar] [CrossRef] [PubMed]
- Kirkley, S.; Cowles, J.; Pellegrini, V.; Harris, C.; Boyd, A.; Blumberg, N. Cytokine secretion after allogeneic or autologous blood transfusion. Lancet 1995, 345, 527. [Google Scholar] [CrossRef]
- Lowery, G.L.; Kulkarni, S.S. Posterior percutaneous spine instrumentation. Eur. Spine J. 2000, 9 (Suppl. S1), S126–S130. [Google Scholar] [CrossRef]
- Hong, S.-H.; Suh, S.-P.; Yeom, J.; Kim, J.-Y.; Lee, S.G.; Han, J.-W. Minimally Invasive Spine Surgery versus Open Posterior Instrumentation Surgery for Unstable Thoracolumbar Burst Fracture. Asian Spine J. 2021, 15, 761–768. [Google Scholar] [CrossRef]
- Foley, K.T.; Holly, L.T.; Schwender, J.D. Minimally Invasive Lumbar Fusion. Spine 2003, 28 (Suppl. S15), S26–S35. [Google Scholar] [CrossRef] [PubMed]
- Nasto, L.A.; Colangelo, D.; Mazzotta, V.; Di Meco, E.; Neri, V.; Nasto, R.A.; Fantoni, M.; Pola, E. Is posterior percutaneous screw-rod instrumentation a safe and effective alternative approach to TLSO rigid bracing for single-level pyogenic spondylodiscitis? Results of a retrospective cohort analysis. Spine J. 2014, 14, 1139–1146. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PEIDF | Open | p-Value | |
|---|---|---|---|
| Number of patients | 15 | 29 | |
| Age (year) | 68.93 ± 14.09 | 70.83 ± 7.96 | 0.635 |
| Sex (Male/Female) | 8/7 | 12/17 | 0.450 |
| Comorbidity | |||
| Diabetic Mellitus | 5 | 13 | 0.462 |
| ESRD | 3 | 14 | 0.092 |
| COPD | 5 | 8 | 0.692 |
| Malignancy history | 3 | 4 | 0.594 |
| Pyogenic burden | |||
| Psoas abscess | 8 | 11 | 0.328 |
| Epidural abscess | 2 | 10 | 0.135 |
| Surgical data | |||
| Surgical time (minute) | 120.80 ± 25.79 | 128.49 ± 39.95 | 0.506 |
| Blood loss (mL) | <50 | 662.07 ± 489.47 | <0.001 * |
| Intraoperative transfusion | 0 | 16 | <0.001 * |
| Preoperative laboratory data | |||
| Albumin (g/dL) | 2.89 ± 0.73 | 3.14 ± 0.78 | 0.345 |
| CRP (mg/L) | 137.31 ± 78.21 | 140.66 ± 69.87 | 0.885 |
| WBC count (1000/μL) | 9.85 ± 2.95 | 12.49 ± 6.27 | 0.065 |
| Segment (%) | 75.47 ± 9.02 | 78.55 ± 9.89 | 0.320 |
| Platelet (1000/μL) | 257.33 ± 126.34 | 310.10 ± 162.97 | 0.280 |
| Hemoglobin (g/dL) | 9.85 ± 1.07 | 9.27 ± 1.76 | 0.177 |
| Postoperative laboratory data | |||
| CRP (mg/L) | 17.87 ± 19.96 | 41.73 ± 8.13 | 0.017 * |
| WBC count (1000/μL) | 6.67 ± 2.56 | 7.12 ± 2.17 | 0.451 |
| Segment (%) | 61.13 ± 8.04 | 62.47 ± 10.39 | 0.665 |
| Platelet (1000/μL) | 266.20 ± 63.59 | 263.13 ± 82.41 | 0.901 |
| D1 Hemoglobin (g/dL) | 9.81 ± 1.22 | 9.03 ± 1.27 | 0.059 |
| Culture rate (%) | 12 (80.0%) | 18 (62.1%) | 0.226 |
| Revision within one month | 0 | 5 | 0.135 |
| VAS score | |||
| Preoperative | 7.87 ± 1.06 | 7.66 ± 1.289 | 0.588 |
| Postoperative one week | 2.73 ± 0.704 | 4.52 ± 1.661 | <0.001 * |
| PEIDF | Open | p-Value | |
|---|---|---|---|
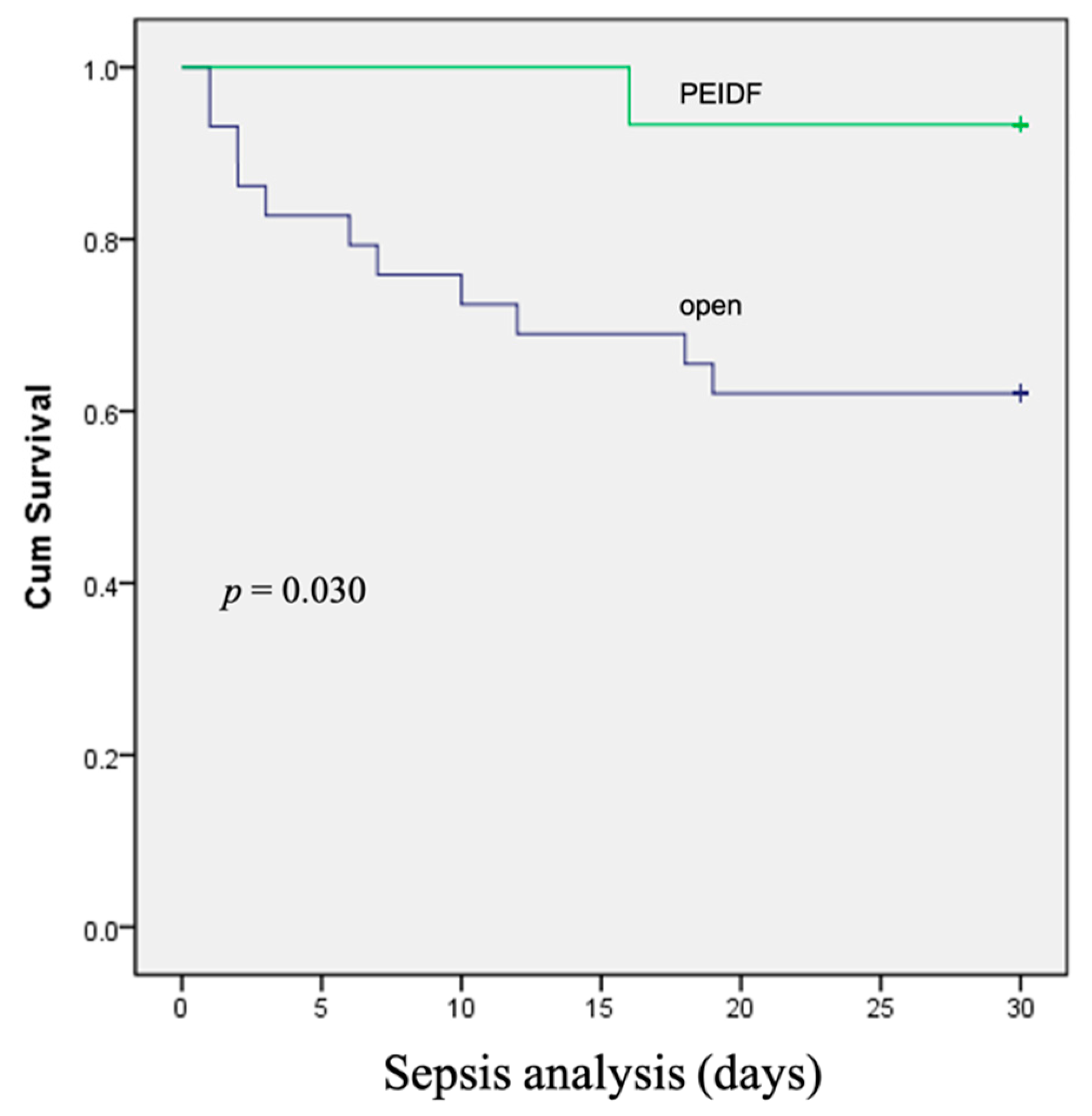
| Sepsis (%) | 1 (6.7) | 11 (37.9) | 0.030 * |
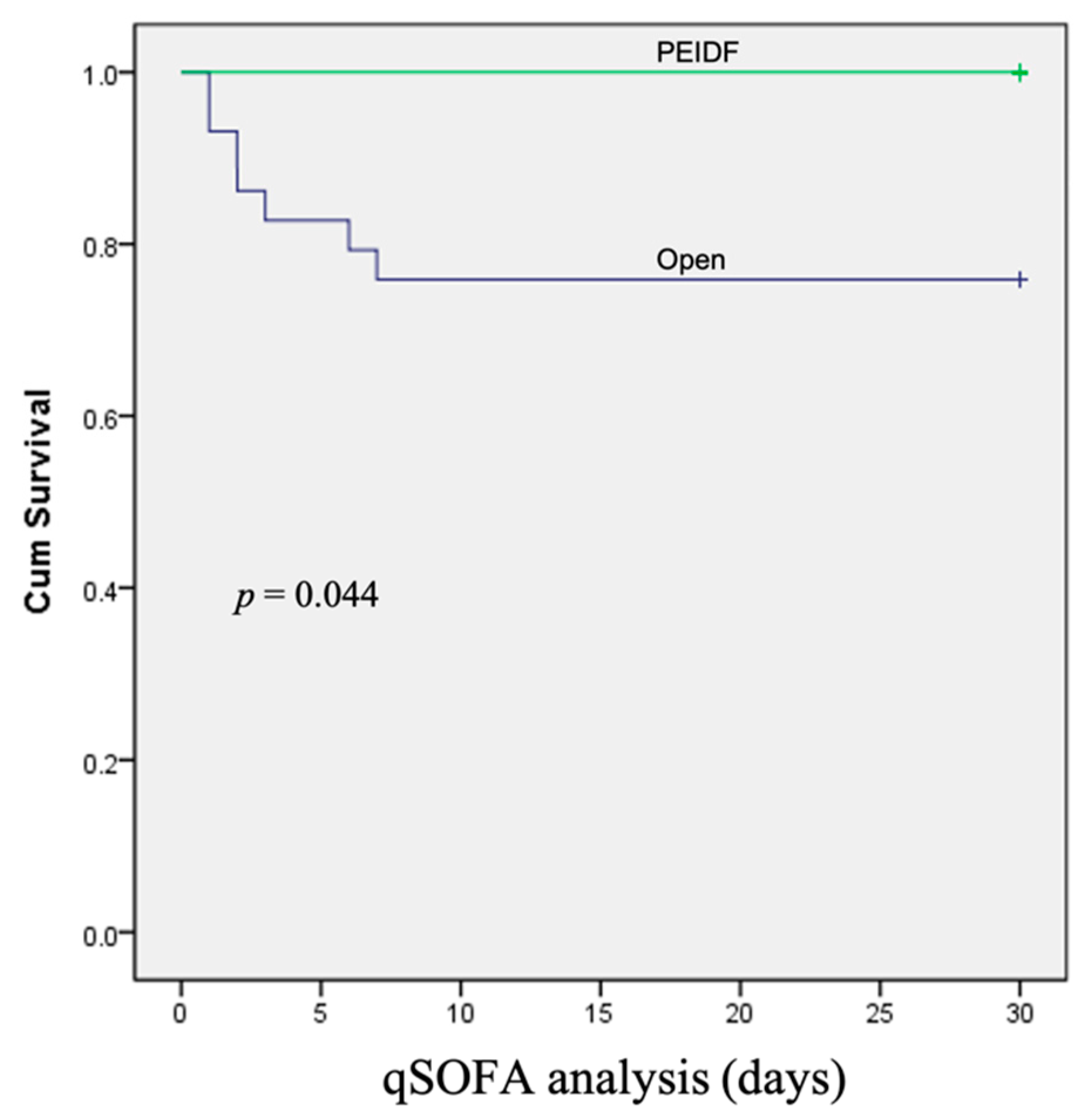
| qSOFA ≥ 2 (%) | 0 (0.0) | 7 (24.1) | 0.044 * |
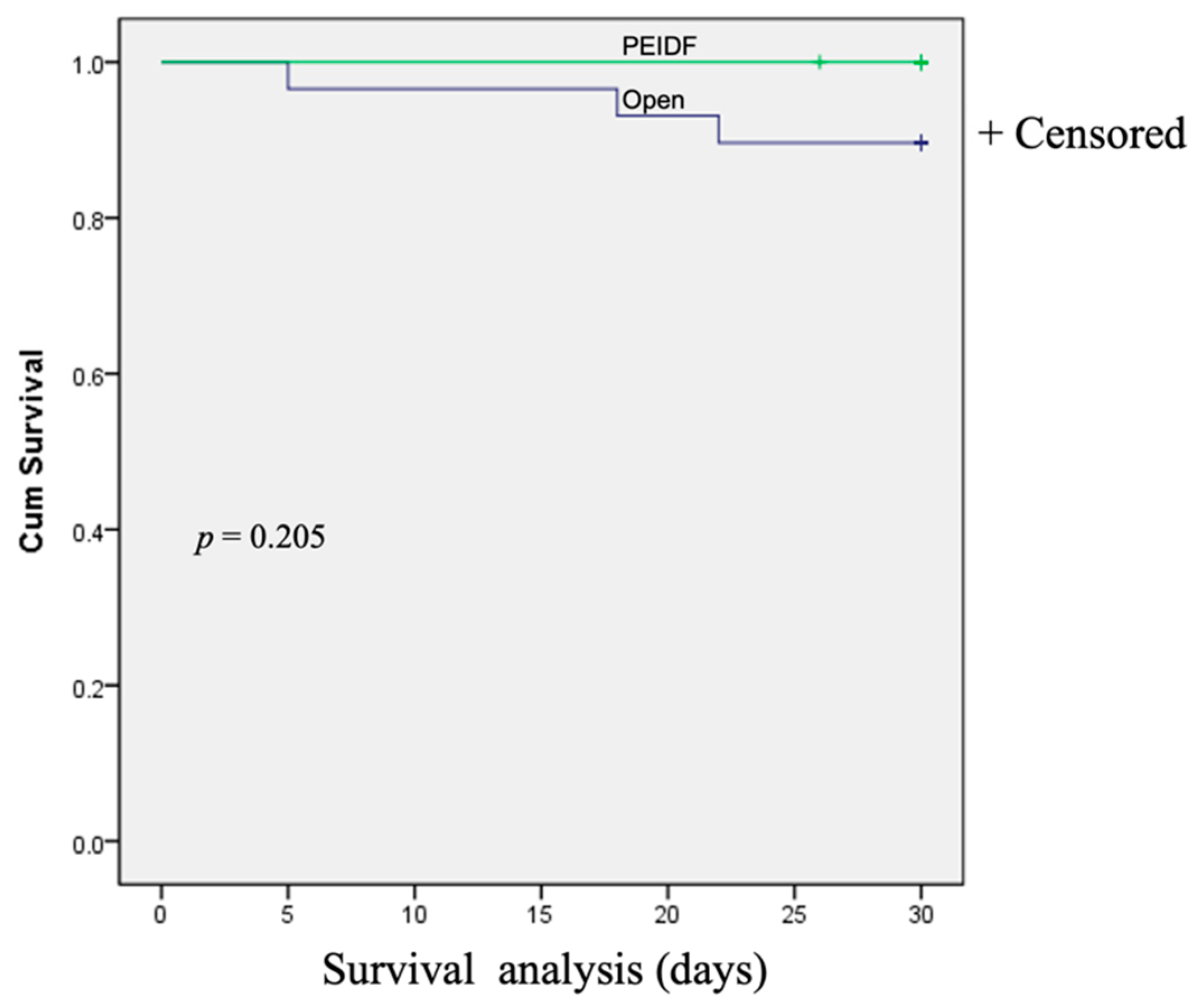
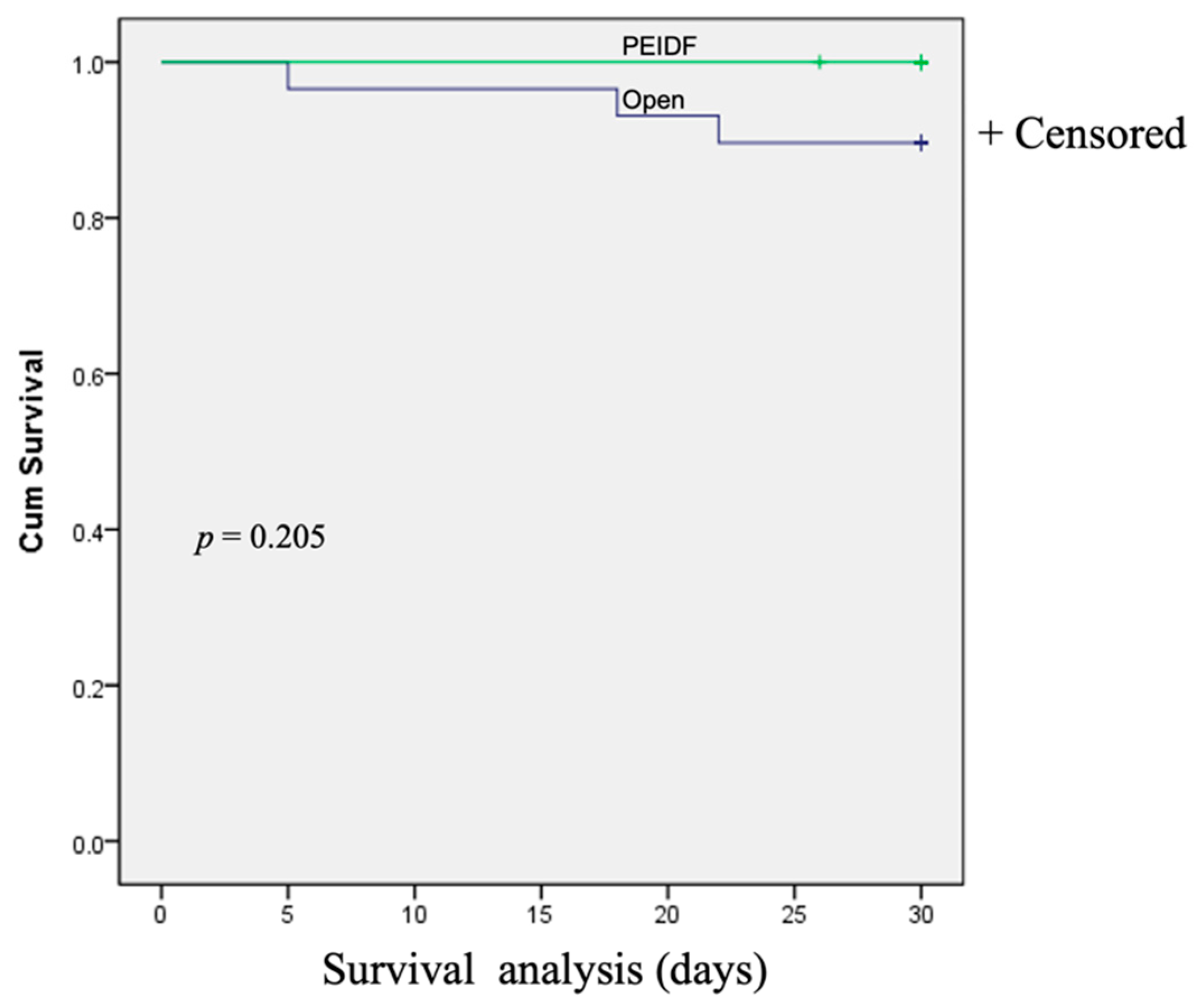
| Death (%) | 1 (6.7) | 3 (10.3) | 0.205 |
| Days to normal CRP level | 26.93 ± 11.55 | 41.31 ± 12.32 | 0.001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, S.-F.; Tsai, T.-T.; Li, Y.-D.; Chiu, P.-Y.; Hsieh, M.-K.; Liao, J.-C.; Lai, P.-L.; Kao, F.-C. Percutaneous Endoscopic Interbody Debridement and Fusion (PEIDF) Decreases Risk of Sepsis and Mortality in Treating Infectious Spondylodiscitis for Patients with Poor Physical Status, a Retrospective Cohort Study. Biomedicines 2022, 10, 1659. https://doi.org/10.3390/biomedicines10071659
Wang S-F, Tsai T-T, Li Y-D, Chiu P-Y, Hsieh M-K, Liao J-C, Lai P-L, Kao F-C. Percutaneous Endoscopic Interbody Debridement and Fusion (PEIDF) Decreases Risk of Sepsis and Mortality in Treating Infectious Spondylodiscitis for Patients with Poor Physical Status, a Retrospective Cohort Study. Biomedicines. 2022; 10(7):1659. https://doi.org/10.3390/biomedicines10071659
Chicago/Turabian StyleWang, Sheng-Fen, Tsung-Ting Tsai, Yun-Da Li, Ping-Yeh Chiu, Ming-Kai Hsieh, Jen-Chung Liao, Po-Liang Lai, and Fu-Cheng Kao. 2022. "Percutaneous Endoscopic Interbody Debridement and Fusion (PEIDF) Decreases Risk of Sepsis and Mortality in Treating Infectious Spondylodiscitis for Patients with Poor Physical Status, a Retrospective Cohort Study" Biomedicines 10, no. 7: 1659. https://doi.org/10.3390/biomedicines10071659
APA StyleWang, S.-F., Tsai, T.-T., Li, Y.-D., Chiu, P.-Y., Hsieh, M.-K., Liao, J.-C., Lai, P.-L., & Kao, F.-C. (2022). Percutaneous Endoscopic Interbody Debridement and Fusion (PEIDF) Decreases Risk of Sepsis and Mortality in Treating Infectious Spondylodiscitis for Patients with Poor Physical Status, a Retrospective Cohort Study. Biomedicines, 10(7), 1659. https://doi.org/10.3390/biomedicines10071659