
Significantly Altered Serum Levels of NAD, AGE, RAGE, CRP, and Elastin as Potential Biomarkers of Psoriasis and Aging—A Case-Control Study

 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Groups and Clinical Examinations
2.2. Collection of the Blood Samples
2.3. Analysis of AGE
2.4. Analysis of RAGE
2.5. Analysis of CRP
2.6. Analysis of Elastin
2.7. Analysis of NAD
2.8. Statistical Analysis
3. Results
3.1. Participant’s Data
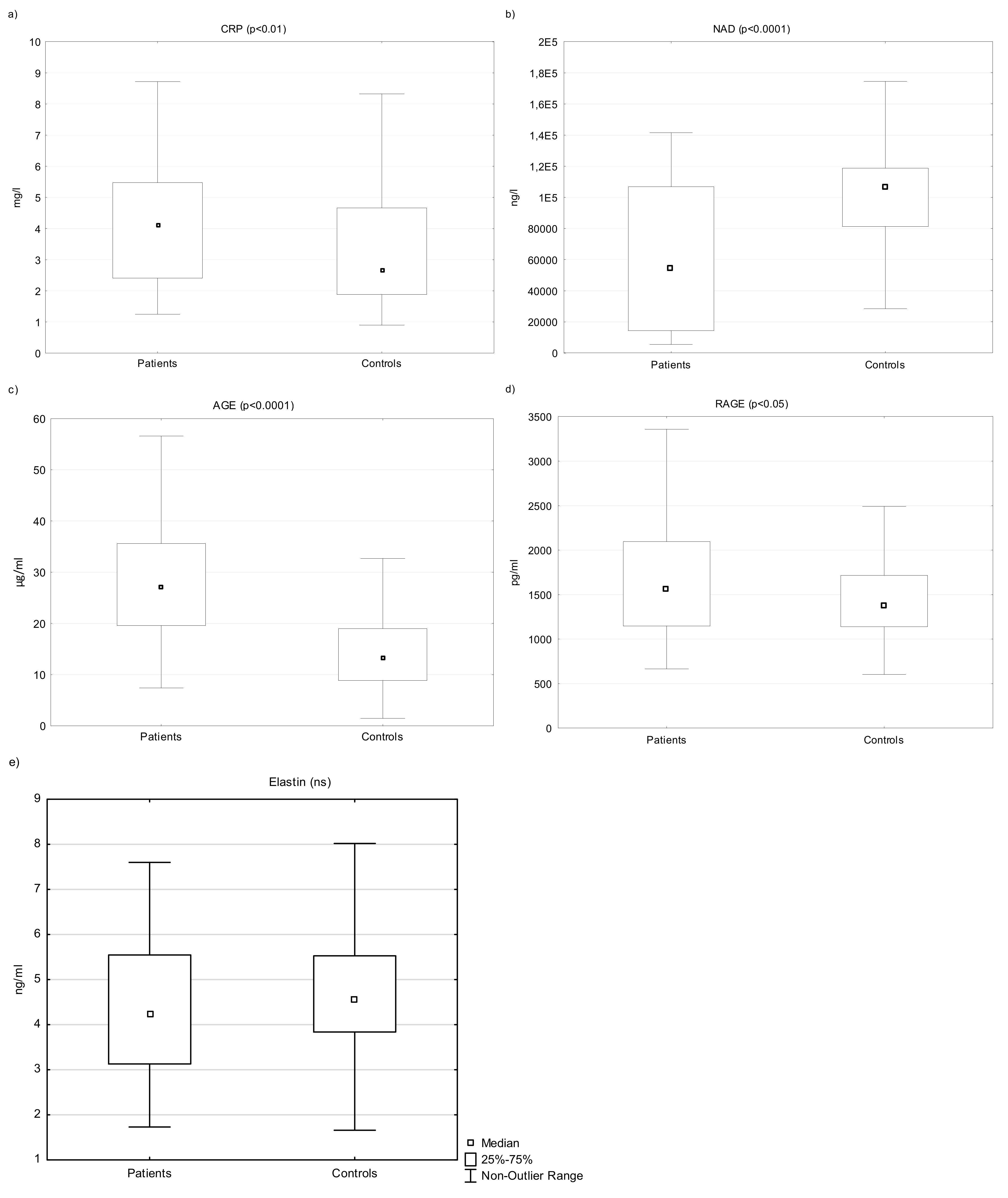
3.2. The Levels of Selected Parameters (CRP, NAD, AGE and RAGE, Elastin)
3.3. Correlation among Measured Parameters
3.4. Sex Differences between Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Baker, K.F.; Isaacs, J.D. Novel therapies for immune-mediated inflammatory diseases: What can we learn from their use in rheumatoid arthritis, spondyloarthritis, systemic lupus erythematosus, psoriasis, Crohn’s disease and ulcerative colitis? Ann. Rheum. Dis. 2018, 77, 175–187. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, A.W.; Read, C. Pathophysiology, Clinical Presentation, and Treatment of Psoriasis: A Review. JAMA—J. Am. Med. Assoc. 2020, 323, 1945–1960. [Google Scholar] [CrossRef] [PubMed]
- Baş, Y.; Seçkin, H.Y.; Kalkan, G.; Takci, Z.; Çitil, R.; Önder, Y.; Şahin, Ş.; DEMİR, A.K. Prevalence and related factors of psoriasis and seborrheic dermatitis: A communitybased study. Turk. J. Med. Sci. 2016, 46, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Schonmann, Y.; Ashcroft, D.M.; Iskandar, I.Y.K.; Parisi, R.; Sde-Or, S.; Comaneshter, D.; Batat, E.; Shani, M.; Vinker, S.; Griffiths, C.E.; et al. Incidence and prevalence of psoriasis in Israel between 2011 and 2017. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 2075–2081. [Google Scholar] [CrossRef] [PubMed]
- Beranek, M.; Fiala, Z.; Kremlacek, J.; Andrys, C.; Krejsek, J.; Hamakova, K.; Chmelarova, M.; Palicka, V.; Borska, L. Changes in circulating cell-free DNA and nucleosomes in patients with exacerbated psoriasis. Arch. Dermatol. Res. 2017, 309, 815–821. [Google Scholar] [CrossRef] [PubMed]
- Cannavò, S.P.; Riso, G.; Casciaro, M.; Di Salvo, E.; Gangemi, S. Oxidative stress involvement in psoriasis: A systematic review. Free Radic. Res. 2019, 53, 829–840. [Google Scholar] [CrossRef] [PubMed]
- Biswas, S.K. Does the Interdependence between Oxidative Stress and Inflammation Explain the Antioxidant Paradox? Oxid. Med. Cell. Longev. 2016, 2016, 5698931. [Google Scholar] [CrossRef]
- Borsky, P.; Chmelarova, M.; Fiala, Z.; Hamakova, K.; Palicka, V.; Krejsek, J.; Andrys, C.; Kremlacek, J.; Rehacek, V.; Beranek, M.; et al. Aging in psoriasis vulgaris: Female patients are epigenetically older than healthy controls. Immun. Ageing 2021, 18, 10. [Google Scholar] [CrossRef]
- Holmannova, D.; Borsky, P.; Borska, L.; Andrys, C.; Hamakova, K.; Rehacek, V.; Svadlakova, T.; Malkova, A.; Beranek, M.; Palicka, V.; et al. Metabolic Syndrome, Clusterin and Elafin in Patients with Psoriasis Vulgaris. Int. J. Mol. Sci. 2020, 21, 5617. [Google Scholar] [CrossRef]
- BBorska, L.; Kremlacek, J.; Andrys, C.; Krejsek, J.; Hamakova, K.; Borsky, P.; Palicka, V.; Rehacek, V.; Malkova, A.; Fiala, Z. Systemic Inflammation, Oxidative Damage to Nucleic Acids, and Metabolic Syndrome in the Pathogenesis of Psoriasis. Int. J. Mol. Sci. 2017, 18, 2238. [Google Scholar] [CrossRef]
- Mehta, N.N.; Azfar, R.S.; Shin, D.B.; Neimann, A.L.; Troxel, A.B.; Gelfand, J.M. Patients with severe psoriasis are at increased risk of cardiovascular mortality: Cohort study using the general practice research database. Eur. Heart J. 2010, 31, 1000–1006. [Google Scholar] [CrossRef]
- Howcroft, T.K.; Campisi, J.; Louis, G.B.; Smith, M.T.; Wise, B.; Wyss-Coray, T.; Augustine, A.D.; McElhaney, J.E.; Kohanski, R.; Sierra, F. The role of inflammation in age-related disease. Aging 2013, 5, 84–93. [Google Scholar] [CrossRef]
- Chung, H.Y.; Ki, W.C.; Lee, E.K.; Chung, K.W.; Chung, S.; Lee, B.; Seo, A.Y.; Chung, J.H.; Jung, Y.S.; Im, E.; et al. Redefining Chronic Inflammation in Aging and Age-Related Diseases: Proposal of the Senoinflammation Concept. Aging Dis. 2019, 10, 367–382. [Google Scholar] [CrossRef]
- SSingh, T.; Newman, A.B. Inflammatory markers in population studies of aging. Ageing Res. Rev. 2011, 10, 319–329. [Google Scholar] [CrossRef]
- Covarrubias, A.J.; Perrone, R.; Grozio, A.; Verdin, E. NAD+ metabolism and its roles in cellular processes during ageing. Nat. Rev. Mol. Cell Biol. 2021, 22, 119–141. [Google Scholar] [CrossRef]
- Han, G.; Williams, C.A.; Salter, K.; Garl, P.J.; Li, A.G.; Wang, X.-J. A Role for TGFβ Signaling in the Pathogenesis of Psoriasis. J. Investig. Dermatol. 2010, 130, 371–377. [Google Scholar] [CrossRef]
- Krieglstein, K.; Miyazono, K.; Ten Dijke, P.; Unsicker, K. TGF-β in aging and disease. Cell Tissue Res. 2012, 347, 5–9. [Google Scholar] [CrossRef]
- Mezentsev, A.; Nikolaev, A.; Bruskin, S. Matrix metalloproteinases and their role in psoriasis. Gene 2014, 540, 1–10. [Google Scholar] [CrossRef]
- Hodges, N.A.; Suarez-Martinez, A.D.; Murfee, W.L. Understanding angiogenesis during aging: Opportunities for discoveries and new models. J. Appl. Physiol. 2018, 125, 1843–1850. [Google Scholar] [CrossRef]
- Ahadi, S.; Zhou, W.; Rose, S.M.S.-F.; Sailani, M.R.; Contrepois, K.; Avina, M.; Ashland, M.; Brunet, A.; Snyder, M. Personal aging markers and ageotypes revealed by deep longitudinal profiling. Nat. Med. 2020, 26, 83–90. [Google Scholar] [CrossRef]
- Holmannova, D.; Borska, L.; Andrys, C.; Borsky, P.; Kremlacek, J.; Hamakova, K.; Rehacek, V.; Malkova, A.; Svadlakova, T.; Palicka, V.; et al. The Impact of Psoriasis and Metabolic Syndrome on the Systemic Inflammation and Oxidative Damage to Nucleic Acids. J. Immunol. Res. 2020, 2020, 7352637. [Google Scholar] [CrossRef]
- Rodríguez-Cerdeira, C.; Molares-Vila, A.; Sánchez-Blanco, E.; Sánchez-Blanco, B. Study on Certain Biomarkers of Inflammation in Psoriasis Through “OMICS” Platforms. Open Biochem. J. 2014, 8, 21–34. [Google Scholar] [CrossRef]
- Lennarz, W.J.; Lane, M.D. Encyclopedia of Biological Chemistry, 2nd ed.Academic Press: Cambridge, MA, USA, 2013. [Google Scholar]
- Yan, S.F.; Ramasamy, R.; Naka, Y.; Schmidt, A.M. Glycation, Inflammation, and RAGE: A Scaffold for the Macrovascular Complications of Diabetes and Beyond. Circ. Res. 2003, 93, 1159–1169. [Google Scholar] [CrossRef]
- Papagrigoraki, A.; Maurelli, M.; Del Giglio, M.; Gisondi, P.; Girolomoni, G. Advanced glycation end products in the pathogenesis of psoriasis. Int. J. Mol. Sci. 2017, 18, 2471. [Google Scholar] [CrossRef]
- Palanissami, G.; Paul, S.F.D. RAGE and Its Ligands: Molecular Interplay Between Glycation, Inflammation, and Hallmarks of Cancer—A Review. Horm. Cancer 2018, 9, 295–325. [Google Scholar] [CrossRef]
- Parks, W.C.; Pierce, R.A.; Lee, K.A.; Mecham, R.P. Elastin. Adv. Mol. Cell Biol. 1993, 6, 133–181. [Google Scholar] [CrossRef]
- Heinz, A. Elastases and elastokines: Elastin degradation and its significance in health and disease. Crit. Rev. Biochem. Mol. Biol. 2020, 55, 252–273. [Google Scholar] [CrossRef]
- Scandolera, A.; Odoul, L.; Salesse, S.; Guillot, A.; Blaise, S.; Kawecki, C.; Maurice, P.; El Btaouri, H.; Romier-Crouzet, B.; Martiny, L.; et al. The Elastin Receptor Complex: A Unique Matricellular Receptor with High Anti-tumoral Potential. Front. Pharmacol. 2016, 7, 32. [Google Scholar] [CrossRef]
- Antonicelli, F.; Bellon, G.; Debelle, L.; Hornebeck, W. Elastin-Elastases and Inflamm-Aging. Curr. Top. Dev. Biol. 2007, 79, 99–155. [Google Scholar] [CrossRef]
- Kucich, U.; Rosenbloom, J.C.; Abrams, W.R.; Bashir, M.; Rosenbloom, J. Stabilization of elastin mRNA by TGF-β: Initial characterization of signaling pathway. Pneumologie 1997, 51, 1080. [Google Scholar] [CrossRef]
- Colburn, K.K.; Kelly, G.T.; Malto, M.C.; Sandberg, L.B.; Boucek, R.J. Serum anti-tropo: Anti-alpha-elastin antibody ratio assessing elastin turnover in scleroderma. Clin. Rheumatol. 1992, 11, 206–210. [Google Scholar] [CrossRef] [PubMed]
- Krettek, A.; Sukhova, G.K.; Libby, P. Elastogenesis in human arterial disease: A role for macrophages in disordered elastin synthesis. Arterioscler Thromb. Vasc. Biol. 2003, 23, 582–587. [Google Scholar] [CrossRef] [PubMed]
- Ungerstedt, J.S.; Blombäck, M.; Söderström, T. Nicotinamide is a potent inhibitor of proinflammatory cytokines. Clin. Exp. Immunol. 2003, 131, 48–52. [Google Scholar] [CrossRef] [PubMed]
- Radenkovic, D.; Verdin, E. Clinical evidence for targeting nad therapeutically. Pharmaceuticals 2020, 13, 247. [Google Scholar] [CrossRef]
- Namazi, M.R. Nicotinamide: A potential addition to the anti-psoriatic weaponry. FASEB J. 2003, 17, 1377–1379. [Google Scholar] [CrossRef]
- Gustafson, C.J.; Watkins, C.; Hix, E.; Feldman, S.R. Combination therapy in psoriasis: An evidence-based review. Am. J. Clin. Dermatol. 2013, 14, 9–25. [Google Scholar] [CrossRef]
- Rinnerthaler, M.; Streubel, M.K.; Bischof, J.; Richter, K. Skin aging, gene expression and calcium. Exp. Gerontol. 2015, 68, 59–65. [Google Scholar] [CrossRef]
- Boehncke, W.H.; Schön, M.P. Psoriasis. Lancet 2015, 386, 983–994. [Google Scholar] [CrossRef]
- Beygi, S.; Lajevardi, V.; Abedini, R. C-reactive protein in psoriasis: A review of the literature. J. Eur. Acad. Dermatol. Venereol. 2014, 28, 700–711. [Google Scholar] [CrossRef]
- Okan, G.; Baki, A.M.; Yorulmaz, E.; Dogru-Abbasoglu, S.; Vural, P. Fibroblast growth factor 23 and placental growth factor in patients with psoriasis and their relation to disease severity. Ann. Clin. Lab. Sci. 2016, 46, 174–179. [Google Scholar]
- Choi, J.; Joseph, L.; Pilote, L. Obesity and C-reactive protein in various populations: A systematic review and meta-analysis. Obes. Rev. 2013, 14, 232–244. [Google Scholar] [CrossRef]
- Oikarinen, A.; Tamminen, M.; Karvonen, J.; Reunala, T.; Kallioinen, M.; Hannuksela, M.; Ala-Kokko, L. Effect of long-term PUVA treatment of psoriasis on the collagen and elastin gene expression and growth of skin fibroblasts in vitro. Br. J. Dermatol. 1990, 123, 621–630. [Google Scholar] [CrossRef]
- Mora Huertas, A.C.; Schmelzer, C.E.H.; Hoehenwarter, W.; Heyroth, F.; Heinz, A. Molecular-level insights into aging processes of skin elastin. Biochimie 2016, 128–129, 163–173. [Google Scholar] [CrossRef]
- Nackman, G.B.; Karkowski, F.J.; Halpern, V.J.; Gaetz, H.P.; Tilson, M.D. Elastin degradation products induce adventitial angiogenesis in the Anidjar/Dobrin rat aneurysm model. Surgery 1997, 122, 39–44. [Google Scholar] [CrossRef]
- Chua, R.A.; Arbiser, J.L. The role of angiogenesis in the pathogenesis of psoriasis. Autoimmunity 2009, 42, 574–579. [Google Scholar] [CrossRef]
- Socha, M.; Kicinski, P.; Feldo, M.; Zubilewicz, T.; Pietrzak, A. Assessment of selected angiogenesis markers in the serum of middle-aged male patients with plaque psoriasis. Dermatol. Ther. 2021, 34, e14727. [Google Scholar] [CrossRef]
- Van Lammeren, G.W.; Moll, F.L.; De Borst, G.J.; De Kleijn, D.P.; De Vries, J.-P.P.; Pasterkamp, G. Atherosclerotic Plaque Biomarkers: Beyond the Horizon of the Vulnerable Plaque. Curr. Cardiol. Rev. 2011, 7, 22–27. [Google Scholar] [CrossRef][Green Version]
- Nockowski, P.; Szepietowski, J.C.; Ziarkiewicz, M.; Baran, E. Serum concentrations of transforming growth factor beta 1 in patients with psoriasis vulgaris. Acta Dermatovenerol. Croat. 2004, 12, 2–6. [Google Scholar]
- Flisiak, I.; Zaniewski, P.; Chodynicka, B. Plasma TGF-β1, TIMP-1, MMP-1 and IL-18 as a combined biomarker of psoriasis activity. Biomarkers 2008, 13, 549–556. [Google Scholar] [CrossRef]
- Nallasamy, S.; Yoshida, K.; Akins, M.; Myers, K.; Iozzo, R.; Mahendroo, M. Steroid Hormones Are Key Modulators of Tissue Mechanical Function via Regulation of Collagen and Elastic Fibers. Endocrinology 2017, 158, 950–962. [Google Scholar] [CrossRef]
- Lephart, E.D.; Naftolin, F. Menopause and the Skin: Old Favorites and New Innovations in Cosmeceuticals for Estrogen-Deficient Skin. Dermatol. Ther. 2020, 11, 53–69. [Google Scholar] [CrossRef]
- Clarke, R.E.; Dordevic, A.L.; Tan, S.M.; Ryan, L.; Coughlan, M.T. Dietary Advanced Glycation End Products and Risk Factors for Chronic Disease: A Systematic Review of Randomised Controlled Trials. Nutrients 2016, 8, 125. [Google Scholar] [CrossRef]
- Ramasamy, R.; Yan, S.F.; Schmidt, A.M. RAGE: Therapeutic target and biomarker of the inflammatory response-the evidence mounts. J. Leukoc. Biol. 2009, 86, 505–512. [Google Scholar] [CrossRef]
- Papagrigoraki, A.; Del Giglio, M.; Cosma, C.; Maurelli, M.; Girolomoni, G.; Lapolla, A. Advanced glycation end products are increased in the skin and blood of patients with severe psoriasis. Acta Derm. Venereol. 2017, 97, 782–787. [Google Scholar] [CrossRef] [PubMed]
- Jaisson, S.; Gillery, P. Evaluation of nonenzymatic posttranslational modification-derived products as biomarkers of molecular aging of proteins. Clin. Chem. 2010, 56, 1401–1412. [Google Scholar] [CrossRef] [PubMed]
- Mezentsev, A.V.; Bruskin, S.A.; Soboleva, A.G.; Sobolev, V.V.; Piruzian, E.S. Pharmacological control of receptor of ddvanced glycation end-products and its biological effects in psoriasis. Int. J. Biomed. Sci. 2013, 9, 112–122. [Google Scholar] [PubMed]
- Sparvero, L.J.; Asafu-Adjei, D.; Kang, R.; Tang, D.; Amin, N.; Im, J.; Rutledge, R.; Lin, B.; Amoscato, A.A.; Zeh, H.J.; et al. RAGE (Receptor for Advanced Glycation Endproducts), RAGE Ligands, and their role in Cancer and Inflammation. J. Transl. Med. 2009, 7, 17. [Google Scholar] [CrossRef] [PubMed]
- Yaku, K.; Okabe, K.; Nakagawa, T. NAD metabolism: Implications in aging and longevity. Ageing Res. Rev. 2018, 47, 1–17. [Google Scholar] [CrossRef]
- Li, L.; Renier, G. Activation of nicotinamide adenine dinucleotide phosphate (reduced form) oxidase by advanced glycation end products links oxidative stress to altered retinal vascular endothelial growth factor expression. Metabolism 2006, 55, 1516–1523. [Google Scholar] [CrossRef]
- Shi, X.Y.; Hou, F.F.; Niu, H.X.; Wang, G.B.; Xie, D.; Guo, Z.J.; Zhou, Z.M.; Yang, F.; Tian, J.W.; Zhang, X. Advanced Oxidation Protein Products Promote Inflammation in Diabetic Kidney through Activation of Renal Nicotinamide Adenine Dinucleotide Phosphate Oxidase. Endocrinology 2008, 149, 1829–1839. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Patients (PP) | Controls (CG) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| N | Median | Q1 | Q3 | N | Median | Q1 | Q3 | p-Value | |
| Age | 60 | 45.8 | 34.6 | 58.5 | 100 | 48.7 | 39.1 | 56.1 | NS |
| Weight | 60 | 80.0 | 67.0 | 90.0 | 100 | 83.5 | 68.5 | 95.0 | NS |
| BMI | 60 | 26.9 | 23.7 | 30.7 | 100 | 26.1 | 23.7 | 29.7 | NS |
| Variable | Valid N | Median | Q1 | Q3 | p-Value |
|---|---|---|---|---|---|
| Elastin | |||||
| Patients | 60 | 4.24 | 3.13 | 5.50 | NS |
| Controls | 100 | 4.60 | 3.84 | 5.50 | |
| NAD | |||||
| Patients | 60 | 54,485 | 14,368 | 106,776 | <0.0001 |
| Controls | 100 | 106,465 | 81,208 | 118,608 | |
| CRP | |||||
| Patients | 60 | 4.12 | 2.41 | 5.50 | <0.01 |
| Controls | 100 | 2.70 | 1.88 | 4.70 | |
| AGEs | |||||
| Patients | 60 | 27.15 | 19.60 | 35.60 | <0.0001 |
| Controls | 100 | 13.40 | 8.85 | 19.00 | |
| RAGE | |||||
| Patients | 60 | 1564 | 1146 | 2096 | <0.05 |
| Controls | 100 | 1375 | 1140 | 1718 | |
| Pair of Variables | Patients (PP) | Controls (CG) | All Groups | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Valid | Spearman | p-Value | Valid | Spearman | p-Value | Valid | Spearman | p-Value | |
| Age & PASI | 60 | −0.27214 | <0.05 | ||||||
| Age & BMI | 60 | 0.39711 | <0.01 | 100 | 0.130206 | NS | 160 | 0.259092 | <0.001 |
| Age & AGE | 60 | −0.0252 | NS | 100 | 0.283483 | <0.01 | 160 | 0.151202 | NS |
| Age & Elastin | 60 | 0.7995 | <0.0001 | 100 | 0.275487 | <0.01 | 160 | 0.53016 | <0.0001 |
| Age & NAD | 60 | −0.11512 | NS | 100 | −0.36829 | <0.05 | 160 | −0.23827 | <0.05 |
| Age & CRP | 60 | 0.283301 | <0.05 | 100 | 0.061266 | NS | 160 | 0.141147 | NS |
| PASI & Elastin | 60 | −0.28479 | <0.05 | ||||||
| AGE & NAD | 60 | −0.4014 | <0.05 | 100 | −0.3729 | <0.05 | 160 | −0.50575 | <0.05 |
| Variable | Valid N | Median | Q1 | Q3 | p-Value |
|---|---|---|---|---|---|
| Elastin | |||||
| Men | 89 | 4.30 | 3.18 | 5.20 | p < 0.01 |
| Women | 71 | 4.84 | 3.97 | 6.60 | |
| NAD | |||||
| Men | 89 | 105,270 | 48,587 | 115,360 | NS |
| Women | 71 | 98,250 | 52,730 | 43,477 | |
| CRP | |||||
| Men | 89 | 3.00 | 2.04 | 4.70 | NS |
| Women | 71 | 2.94 | 2.05 | 5.30 | |
| AGEs | |||||
| Men | 89 | 16.50 | 10.90 | 25.90 | NS |
| Women | 71 | 18.20 | 10.30 | 29.20 | |
| RAGE | |||||
| Men | 89 | 1368 | 1126 | 1769 | NS |
| Women | 71 | 1485 | 1185 | 2032 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karas, A.; Holmannova, D.; Borsky, P.; Fiala, Z.; Andrys, C.; Hamakova, K.; Svadlakova, T.; Palicka, V.; Krejsek, J.; Rehacek, V.; et al. Significantly Altered Serum Levels of NAD, AGE, RAGE, CRP, and Elastin as Potential Biomarkers of Psoriasis and Aging—A Case-Control Study. Biomedicines 2022, 10, 1133. https://doi.org/10.3390/biomedicines10051133
Karas A, Holmannova D, Borsky P, Fiala Z, Andrys C, Hamakova K, Svadlakova T, Palicka V, Krejsek J, Rehacek V, et al. Significantly Altered Serum Levels of NAD, AGE, RAGE, CRP, and Elastin as Potential Biomarkers of Psoriasis and Aging—A Case-Control Study. Biomedicines. 2022; 10(5):1133. https://doi.org/10.3390/biomedicines10051133
Chicago/Turabian StyleKaras, Adam, Drahomira Holmannova, Pavel Borsky, Zdenek Fiala, Ctirad Andrys, Kvetoslava Hamakova, Tereza Svadlakova, Vladimir Palicka, Jan Krejsek, Vit Rehacek, and et al. 2022. "Significantly Altered Serum Levels of NAD, AGE, RAGE, CRP, and Elastin as Potential Biomarkers of Psoriasis and Aging—A Case-Control Study" Biomedicines 10, no. 5: 1133. https://doi.org/10.3390/biomedicines10051133
APA StyleKaras, A., Holmannova, D., Borsky, P., Fiala, Z., Andrys, C., Hamakova, K., Svadlakova, T., Palicka, V., Krejsek, J., Rehacek, V., Esterkova, M., Kovarikova, H., & Borska, L. (2022). Significantly Altered Serum Levels of NAD, AGE, RAGE, CRP, and Elastin as Potential Biomarkers of Psoriasis and Aging—A Case-Control Study. Biomedicines, 10(5), 1133. https://doi.org/10.3390/biomedicines10051133