
Predictors of Acute Kidney Disease Severity in Hospitalized Patients with Acute Kidney Injury


 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Definition and Staging of AKI and AKD
2.3. Demographic Profiles, Clinical Characteristics, and Outcomes Collection
2.4. Assessment of Hematologic and Biochemical Profiles
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Enrolled Patients
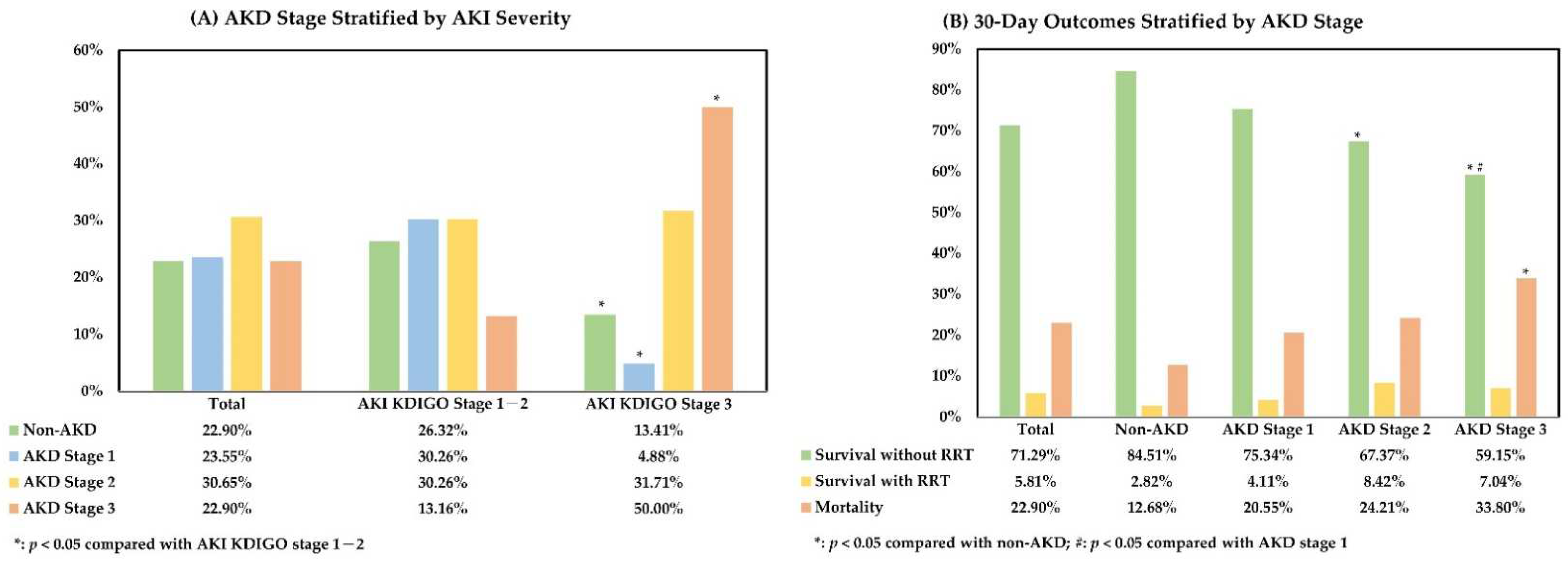
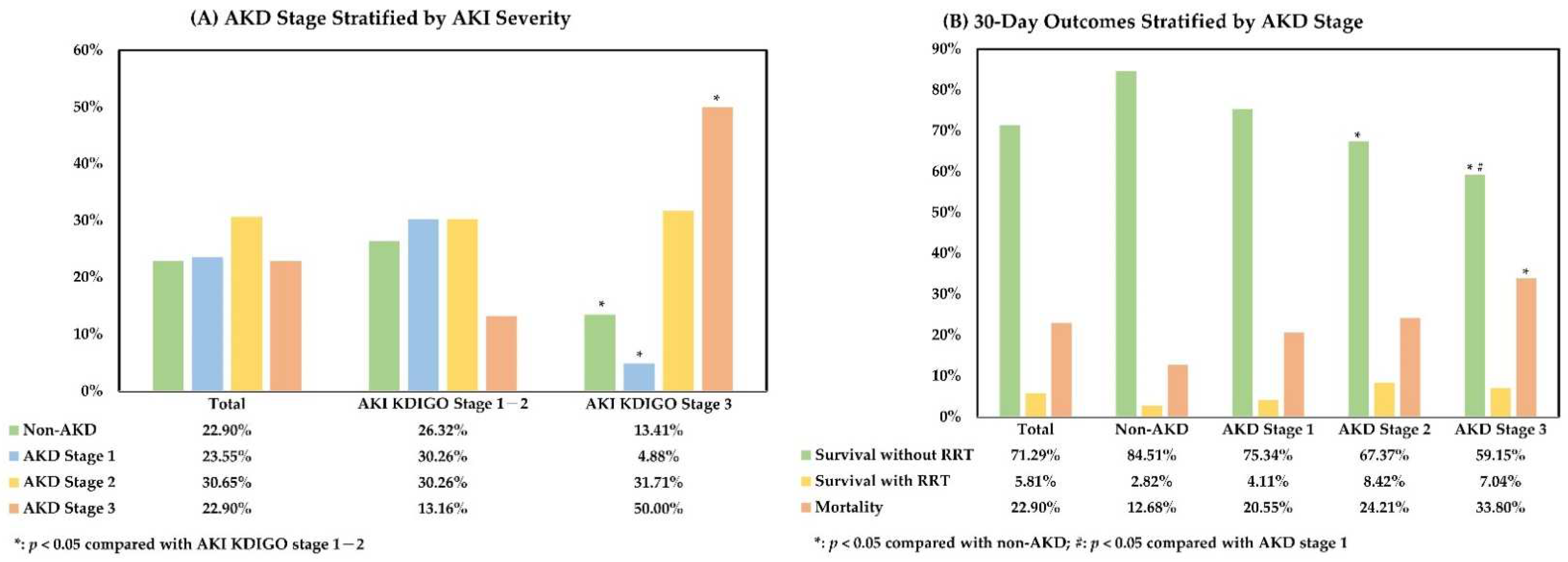
3.2. Relationship between AKI Severity, AKD Stage, and 30-Day Outcome after AKI
3.3. Factors Associated with AKD Severity in Patients with AKI
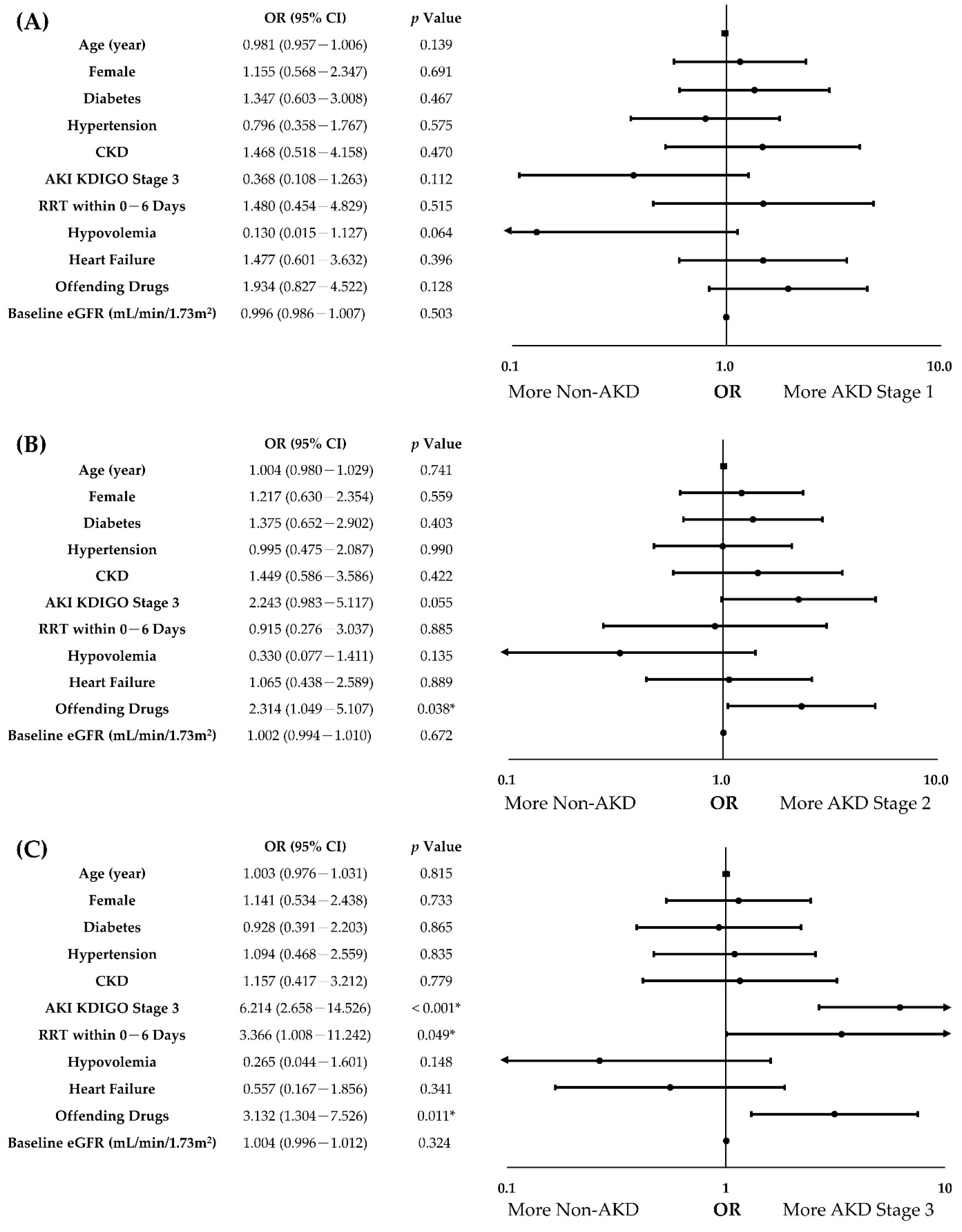
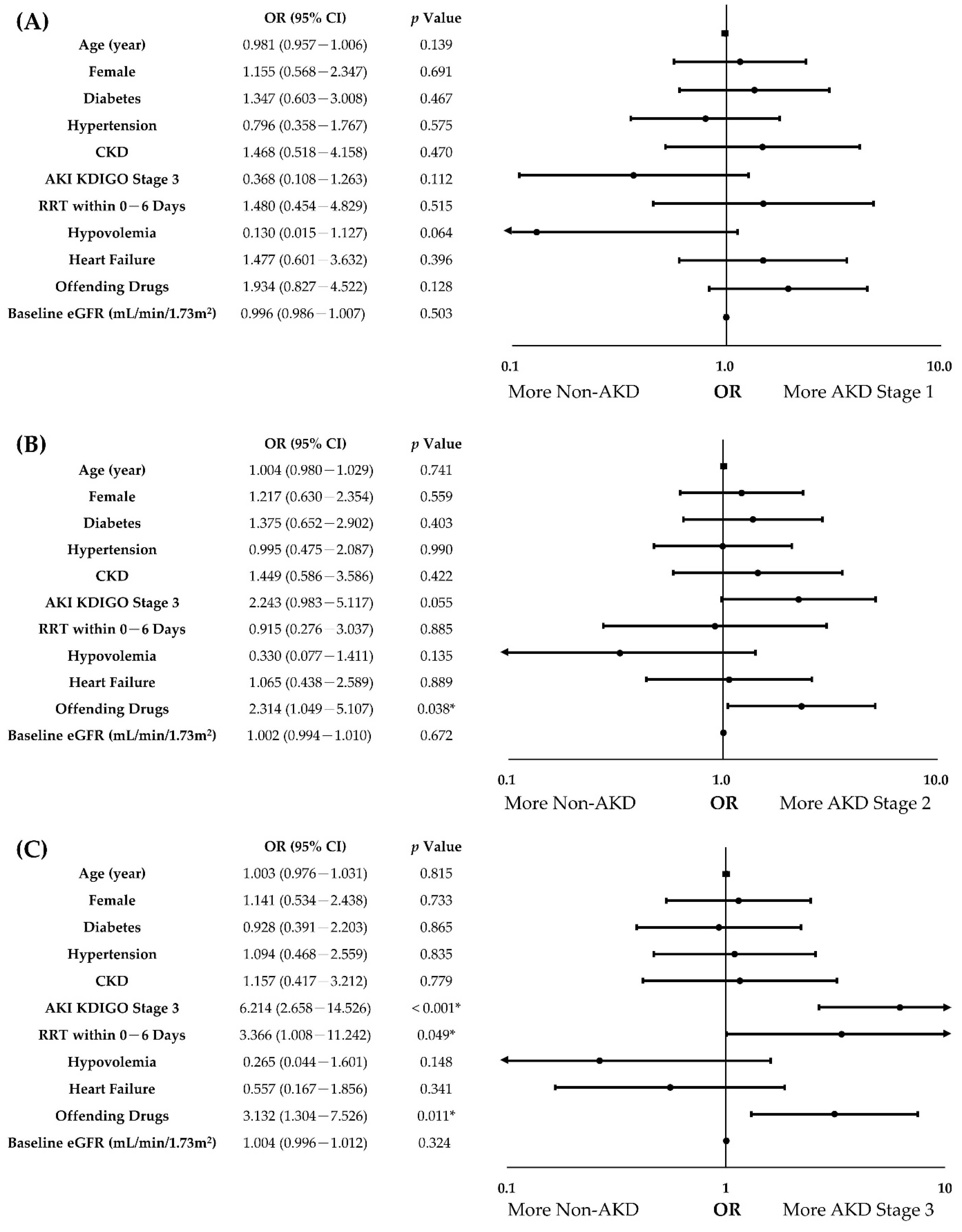
3.4. Independent Predictors of AKD Severity in Patients with AKI
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hoste, E.A.; Kellum, J.A.; Selby, N.M.; Zarbock, A.; Palevsky, P.M.; Bagshaw, S.M.; Goldstein, S.L.; Cerdá, J.; Chawla, L.S. Global epidemiology and outcomes of acute kidney injury. Nat. Rev. Nephrol. 2018, 14, 607–625. [Google Scholar] [CrossRef] [PubMed]
- Odutayo, A.; Wong, C.X.; Farkouh, M.; Altman, D.G.; Hopewell, S.; Emdin, C.A.; Hunn, B.H. AKI and long-term risk for cardiovascular events and mortality. J. Am. Soc. Nephrol. 2017, 28, 377–387. [Google Scholar] [CrossRef] [PubMed]
- Silver, S.A.; Long, J.; Zheng, Y.; Chertow, G.M. Cost of acute kidney injury in hospitalized patients. J. Hosp. Med. 2017, 12, 70–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoste, E.A.; Bagshaw, S.M.; Bellomo, R.; Cely, C.M.; Colman, R.; Cruz, D.N.; Edipidis, K.; Forni, L.G.; Gomersall, C.D.; Govil, D.; et al. Epidemiology of acute kidney injury in critically ill patients: The multinational AKI-EPI study. Intensive Care Med. 2015, 41, 1411–1423. [Google Scholar] [CrossRef]
- Ronco, C.; Bellomo, R.; Kellum, J.A. Acute kidney injury. Lancet 2019, 394, 1949–1964. [Google Scholar] [CrossRef]
- Ponce, D.; de Andrade, L.G.M.; Claure-Del Granado, R.; Ferreiro-Fuentes, A.; Lombardi, R. Development of a prediction score for in-hospital mortality in COVID-19 patients with acute kidney injury: A machine learning approach. Sci. Rep. 2021, 11, 24439. [Google Scholar] [CrossRef]
- Levin, A.; Stevens, P.E.; Bilous, R.W.; Coresh, J.; De Francisco, A.L.; De Jong, P.E.; Griffith, K.E.; Hemmelgarn, B.R.; Iseki, K.; Lamb, E.J. Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. Suppl. 2013, 3, 1–150. [Google Scholar]
- Kellum, J.A.; Lameire, N.; Aspelin, P.; Barsoum, R.S.; Burdmann, E.A.; Goldstein, S.L.; Herzog, C.A.; Joannidis, M.; Kribben, A.; Levey, A.S. Kidney disease: Improving global outcomes (KDIGO) acute kidney injury work group. KDIGO clinical practice guideline for acute kidney injury. Kidney Int. Suppl. 2012, 2, 1–138. [Google Scholar]
- Kaballo, M.A.; Elsayed, M.E.; Stack, A.G. Linking acute kidney injury to chronic kidney disease: The missing links. J. Nephrol. 2017, 30, 461–475. [Google Scholar] [CrossRef]
- Chawla, L.S.; Bellomo, R.; Bihorac, A.; Goldstein, S.L.; Siew, E.D.; Bagshaw, S.M.; Bittleman, D.; Cruz, D.; Endre, Z.; Fitzgerald, R.L.; et al. Acute kidney disease and renal recovery: Consensus report of the Acute Disease Quality Initiative (ADQI) 16 Workgroup. Nat. Rev. Nephrol. 2017, 13, 241–257. [Google Scholar] [CrossRef] [Green Version]
- Gameiro, J.; Carreiro, C.; Fonseca, J.A.; Pereira, M.; Jorge, S.; Gouveia, J.; Lopes, J.A. Acute kidney disease and long-term outcomes in critically ill acute kidney injury patients with sepsis: A cohort analysis. Clin. Kidney J. 2021, 14, 1379–1387. [Google Scholar] [CrossRef] [PubMed]
- Yan, P.; Duan, X.J.; Liu, Y.; Wu, X.; Zhang, N.Y.; Yuan, F.; Tang, H.; Liu, Q.; Deng, Y.H.; Wang, H.S.; et al. Acute kidney disease in hospitalized acute kidney injury patients. Peer J. 2021, 9, e11400. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Y.-Q.; Cheng, W.; Wu, X.; Yan, P.; Feng, L.-X.; Zhang, N.-Y.; Li, X.-W.; Duan, X.-J.; Wang, H.-S.; Peng, J.-C.; et al. Novel risk models to predict acute kidney disease and its outcomes in a Chinese hospitalized population with acute kidney injury. Sci. Rep. 2020, 10, 15636. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Liang, L.; Pan, S.; Liu, Z.; Liang, Y.; Qiao, Y.; Liu, D.; Liu, Z. Diabetes Mellitus as a Risk Factor for Progression from Acute Kidney Injury to Acute Kidney Disease: A Specific Prediction Model. Diabetes Metab. Syndr. Obes. 2021, 14, 2367–2379. [Google Scholar] [CrossRef]
- Holmes, J.; Rainer, T.; Geen, J.; Roberts, G.; May, K.; Wilson, N.; Williams, J.D.; Phillips, A.O. Acute kidney injury in the era of the AKI E-alert. Clin. J. Am. Soc. Nephrol. 2016, 11, 2123–2131. [Google Scholar] [CrossRef]
- Porter, C.J.; Juurlink, I.; Bisset, L.H.; Bavakunji, R.; Mehta, R.L.; Devonald, M.A. A real-time electronic alert to improve detection of acute kidney injury in a large teaching hospital. Nephrol. Dial. Transplant. 2014, 29, 1888–1893. [Google Scholar] [CrossRef] [Green Version]
- Levey, A.S.; Bosch, J.P.; Lewis, J.B.; Greene, T.; Rogers, N.; Roth, D. A more accurate method to estimate glomerular filtration rate from serum creatinine: A new prediction equation. Modification of Diet in Renal Disease Study Group. Ann. Intern. Med. 1999, 130, 461–470. [Google Scholar] [CrossRef]
- Matsuura, R.; Iwagami, M.; Moriya, H.; Ohtake, T.; Hamasaki, Y.; Nangaku, M.; Doi, K.; Kobayashi, S.; Noiri, E. The Clinical Course of Acute Kidney Disease after Cardiac Surgery: A Retrospective Observational Study. Sci. Rep. 2020, 10, 6490. [Google Scholar] [CrossRef] [Green Version]
- Kofman, N.; Margolis, G.; Gal-Oz, A.; Letourneau-Shesaf, S.; Keren, G.; Rozenbaum, Z.; Shacham, Y. Long-term renal outcomes and mortality following renal injury among myocardial infarction patients treated by primary percutaneous intervention. Coron. Artery Dis. 2019, 30, 87–92. [Google Scholar] [CrossRef]
- Maher, R.L.; Hanlon, J.; Hajjar, E.R. Clinical consequences of polypharmacy in elderly. Expert Opin. Drug Saf. 2014, 13, 57–65. [Google Scholar] [CrossRef] [Green Version]
- Kimura, H.; Tanaka, K.; Saito, H.; Iwasaki, T.; Oda, A.; Watanabe, S.; Kanno, M.; Shimabukuro, M.; Asahi, K.; Watanabe, T.; et al. Association of Polypharmacy with Kidney Disease Progression in Adults with CKD. Clin. J. Am. Soc. Nephrol. 2021, 16, 1797–1804. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.-C.; Lee, Y.-T.; Li, L.-C.; Ng, H.-Y.; Kuo, W.-H.; Lin, P.-T.; Liao, Y.-C.; Chiou, T.-T.; Lee, C.-T. The Number of Comorbidities Predicts Renal Outcomes in Patients with Stage 3–5 Chronic Kidney Disease. J. Clin. Med. 2018, 7, 493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Awdishu, L.; Mehta, R.L. The 6R’s of drug induced nephrotoxicity. BMC Nephrol. 2017, 18, 124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jagieła, J.; Bartnicki, P.; Rysz, J. Nephrotoxicity as a Complication of Chemotherapy and Immunotherapy in the Treatment of Colorectal Cancer, Melanoma and Non-Small Cell Lung Cancer. Int. J. Mol. Sci. 2021, 22, 4618. [Google Scholar] [CrossRef]
- Nelson, D.A.; Marks, E.S.; Deuster, P.A.; O’Connor, F.G.; Kurina, L.M. Association of nonsteroidal anti-inflammatory drug prescriptions with kidney disease among active young and middle-aged adults. JAMA Netw. Open 2019, 2, e187896. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, X.; Donnan, P.T.; Bell, S.; Guthrie, B. Non-steroidal anti-inflammatory drug induced acute kidney injury in the community dwelling general population and people with chronic kidney disease: Systematic review and meta-analysis. BMC Nephrol. 2017, 18, 256. [Google Scholar] [CrossRef] [Green Version]
- Abrahamsson, A.; Oras, J.; Snygg, J.; Block, L. Perioperative COX-2 inhibitors may increase the risk of post-operative acute kidney injury. Acta Anaesthesiol. Scand. 2017, 61, 714–721. [Google Scholar] [CrossRef]
- Whelton, A.; Lefkowith, J.L.; West, C.R.; Verburg, K.M. Cardiorenal effects of celecoxib as compared with the nonsteroidal anti-inflammatory drugs diclofenac and ibuprofen. Kidney Int. 2006, 70, 1495–1502. [Google Scholar] [CrossRef] [Green Version]
- Onuigbo, M. Reno-prevention vs. reno-protection: A critical re-appraisal of the evidence-base from the large RAAS blockade trials after ONTARGET—A call for more circumspection. QJM Int. J. Med. 2009, 102, 155–167. [Google Scholar] [CrossRef]
- Guidi, E.; Minetti, E.E.; Cozzi, M.G. Acute and long-term effects of ACE inhibition on renal haemodynamics in glomerular and interstitial nephropathies. J. Renin-Angiotensin-Aldosterone Syst. 2002, 3, 40–45. [Google Scholar] [CrossRef]
- Bainey, K.R.; Rahim, S.; Etherington, K.; Rokoss, M.L.; Natarajan, M.K.; Velianou, J.L.; Brons, S.; Mehta, S.R.; Investigators, C. Effects of withdrawing vs continuing renin-angiotensin blockers on incidence of acute kidney injury in patients with renal insufficiency undergoing cardiac catheterization: Results from the Angiotensin Converting Enzyme Inhibitor/Angiotensin Receptor Blocker and Contrast Induced Nephropathy in Patients Receiving Cardiac Catheterization (CAPTAIN) trial. Am. Heart J. 2015, 170, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Hines, A.; Li, X.; Ortiz-Soriano, V.; Saleh, S.; Litteral, J.; Ruiz-Conejo, M.; Wald, R.; Silver, S.A.; Neyra, J.A. Use of Angiotensin-Converting Enzyme Inhibitors/Angiotensin Receptor Blockers and Acute Kidney Disease after an Episode of AKI: A Multicenter Prospective Cohort Study. Am. J. Nephrol. 2020, 51, 266–275. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.-Y.; Tsai, I.-J.; Pan, H.-C.; Liao, H.-W.; Neyra, J.A.; Wu, V.-C.; Chueh, J.S. The Impact of Angiotensin-Converting Enzyme Inhibitors or Angiotensin II Receptor Blockers on Clinical Outcomes of Acute Kidney Disease Patients: A Systematic Review and Meta-Analysis. Front. Pharmacol. 2021, 12, 665250. [Google Scholar] [CrossRef] [PubMed]
- Morales-Alvarez, M.C. Nephrotoxicity of Antimicrobials and Antibiotics. Adv. Chronic Kidney Dis. 2020, 27, 31–37. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Lin, J.; Duan, M. Application of Machine Learning to Predict Acute Kidney Disease in Patients with Sepsis Associated Acute Kidney Injury. Front. Med. 2021, 8, 792974. [Google Scholar] [CrossRef]
- Forni, L.; Darmon, M.; Ostermann, M.; Oudemans-van Straaten, H.; Pettilä, V.; Prowle, J.; Schetz, M.; Joannidis, M. Renal recovery after acute kidney injury. Intensive Care Med. 2017, 43, 855–866. [Google Scholar] [CrossRef]
- James, M.T.; Pannu, N.; Hemmelgarn, B.R.; Austin, P.C.; Tan, Z.; McArthur, E.; Manns, B.J.; Tonelli, M.; Wald, R.; Quinn, R.R. Derivation and external validation of prediction models for advanced chronic kidney disease following acute kidney injury. JAMA 2017, 318, 1787–1797. [Google Scholar] [CrossRef]
- Coca, S.G.; Yusuf, B.; Shlipak, M.G.; Garg, A.X.; Parikh, C.R. Long-term risk of mortality and other adverse outcomes after acute kidney injury: A systematic review and meta-analysis. Am. J. Kidney Dis. 2009, 53, 961–973. [Google Scholar] [CrossRef] [Green Version]
- Clark, E.G.; Bagshaw, S.M. Unnecessary Renal Replacement Therapy for Acute Kidney Injury is Harmful for Renal Recovery. Semin. Dial. 2015, 28, 6–11. [Google Scholar] [CrossRef]
- Shiao, C.-C.; Huang, T.-M.; Spapen, H.D.; Honore, P.M.; Wu, V.-C. Optimal timing of renal replacement therapy initiation in acute kidney injury: The elephant felt by the blindmen? Crit. Care 2017, 21, 146. [Google Scholar] [CrossRef]
- Elseviers, M.M.; Lins, R.L.; Van der Niepen, P.; Hoste, E.; Malbrain, M.L.; Damas, P.; Devriendt, J. Renal replacement therapy is an independent risk factor for mortality in critically ill patients with acute kidney injury. Crit. Care 2010, 14, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Gallagher, M.; Li, Q.; Lo, S.; Cass, A.; Finfer, S.; Myburgh, J.; Bouman, C.; Faulhaber-Walter, R.; Kellum, J.A.; et al. Renal replacement therapy intensity for acute kidney injury and recovery to dialysis independence: A systematic review and individual patient data meta-analysis. Nephrol. Dial. Transpl. 2018, 33, 1017–1024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peerapornratana, S.; Priyanka, P.; Wang, S.; Smith, A.; Singbartl, K.; Palevsky, P.M.; Chawla, L.S.; Yealy, D.M.; Angus, D.C.; Kellum, J.A.; et al. Sepsis-Associated Acute Kidney Disease. Kidney Int. Rep. 2020, 5, 839–850. [Google Scholar] [CrossRef] [PubMed]
- Wen, Y.; Parikh, C.R. Current concepts and advances in biomarkers of acute kidney injury. Crit. Rev. Clin. Lab. Sci. 2021, 58, 354–368. [Google Scholar] [CrossRef] [PubMed]
- Tsai, K.-F.; Hsu, P.-C.; Lee, C.-T.; Kung, C.-T.; Chang, Y.-C.; Fu, L.-M.; Ou, Y.-C.; Lan, K.-C.; Yen, T.-H.; Lee, W.-C. Association between Enzyme-Linked Immunosorbent Assay-Measured Kidney Injury Markers and Urinary Cadmium Levels in Chronic Kidney Disease. J. Clin. Med. 2021, 11, 156. [Google Scholar] [CrossRef]
- Jim, B.; Santos, J.; Spath, F.; Cijiang He, J. Biomarkers of diabetic nephropathy, the present and the future. Curr. Diabetes Rev. 2012, 8, 317–328. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Demographic Profiles and Comorbidities | |
| Age (years), median (IQR) | 69 (58–79) |
| Female, n (%) | 125 (40.32) |
| BMI (kg/m2), median (IQR) | 24.73 (21.30–28.73) |
| Baseline SCr (μmol/L), median (IQR) | 83.10 (60.11–127.30) |
| Baseline eGFR (mL/min/1.73 m2), median (IQR) | 71.65 (41.76–105.43) |
| Diabetes, n (%) | 135 (43.55) |
| Hypertension, n (%) | 163 (52.58) |
| Dyslipidemia, n (%) | 47 (15.16) |
| CKD, n (%) | 129 (41.61) |
| Heart Failure, n (%) | 54 (17.42) |
| Vascular Disease, n (%) | 78 (25.16) |
| Liver Disease, n (%) | 93 (30.00) |
| Pulmonary Disease, n (%) | 36 (11.61) |
| Malignancy, n (%) | 142 (45.81) |
| Main Causes of AKI | |
| Sepsis, n (%) | 188 (60.65) |
| Cardiorenal Syndrome, n (%) | 22 (7.10) |
| Hypovolemia, n (%) | 13 (4.19) |
| Obstructive Uropathy, n (%) | 13 (4.19) |
| Intrarenal Causes, n (%) | 74 (23.87) |
| Hematologic and Biochemical Profiles at Diagnosis of AKI | |
| SCr (µmol/L) at AKI Diagnosis, median (IQR) | 228.96 (151.16–375.70) |
| eGFR (mL/min/1.73 m2) at AKI Diagnosis, median (IQR) | 22.53 (12.06–35.38) |
| Hemoglobin (g/L), median (IQR) | 100.00 (88.00–117.00) |
| Platelet (109/L), median (IQR) | 169.50 (101.25–253.75) |
| BUN (mmol/L), median (IQR) | 19.99 (12.50–29.27) |
| K (mmol/L), median (IQR) | 4.20 (3.60–4.90) |
| Albumin (g/L), median (IQR) | 29.00 (25.00–33.90) |
| Lactate (mmol/L), median (IQR) | 1.84 (1.29–3.46) |
| pH, median (IQR) | 7.39 (7.30–7.45) |
| HCO3 (mmol/L), median (IQR) | 21.05 (17.10–25.38) |
| Bil-T (µmol/L), median (IQR) | 17.10 (10.26–51.31) |
| RRT Status and 30-Day Mortality after AKI | |
| RRT within 0–6 Days After AKI, n (%) | 40 (12.90) |
| RRT within 7–14 Days After AKI, n (%) | 38 (12.26) |
| 30-Day Mortality After AKI, n (%) | 71 (22.90) |
| Non-AKD (n = 71) | AKD Stage 1 (n = 73) | AKD Stage 2 (n = 95) | AKD Stage 3 (n = 71) | p-Value | |
| Demographic Profiles and Comorbidities, n (%) or Median (IQR) | |||||
| Age (years) | 68 (60–78) | 66 (56–77) | 71 (60–80) | 68 (56–81) | 0.437 |
| Female | 27 (38.03) | 30 (41.10) | 41 (43.16) | 27 (38.03) | 0.886 |
| BMI (kg/m2) | 24.62 (20.35–27.89) | 25.06 (20.97–29.52) | 24.98 (22.42–29.18) | 24.27 (22.08–28.53) | 0.408 |
| Diabetes | 26 (36.62) | 37 (50.68) | 46 (48.42) | 26 (36.62) | 0.158 |
| Hypertension | 34 (47.89) | 40 (54.79) | 54 (56.84) | 35 (49.30) | 0.621 |
| Dyslipidemia | 11 (15.49) | 11 (15.07) | 15 (15.79) | 10 (14.08) | 0.992 |
| CKD | 25 (35.21) | 40 (54.79) | 41 (43.16) | 23 (32.39) b | 0.029 * |
| Heart Failure | 11 (15.49) | 20 (27.40) | 18 (18.95) | 5 (7.04) b | 0.013 * |
| Vascular Disease | 16 (22.54) | 23 (31.51) | 24 (25.26) | 15 (21.13) | 0.487 |
| Liver Disease | 18 (25.35) | 21 (28.77) | 30 (31.58) | 24 (33.80) | 0.709 |
| Pulmonary Disease | 9 (12.68) | 7 (9.59) | 9 (9.47) | 11 (15.49) | 0.607 |
| Malignancy | 36 (50.70) | 28 (38.36) | 43 (45.26) | 35 (49.30) | 0.444 |
| Main Causes of AKI, n (%) | |||||
| Sepsis | 39 (54.93) | 45 (61.64) | 60 (63.16) | 44 (61.97) | 0.728 |
| Cardiorenal Syndrome | 5 (7.04) | 8 (10.96) | 6 (6.32) | 3 (4.23) | 0.453 |
| Hypovolemia | 7 (9.86) | 1 (1.37) | 3 (3.16) | 2 (2.82) | 0.052 # |
| Obstructive Uropathy | 2 (2.82) | 2 (2.74) | 4 (4.21) | 5 (7.04) | 0.541 |
| Intrarenal Causes †† | 18 (25.35) | 17 (23.29) | 22 (23.16) | 17 (23.94) | 0.989 |
| Aggravating Factors at Diagnosis of AKI, n (%) | |||||
| Shock Status | 12 (16.90) | 10 (13.70) | 7 (7.37) | 10 (14.08) | 0.286 |
| Offending Drugs † | 12 (16.90) | 24 (32.88) | 33 (34.74) | 26 (36.62) a | 0.038 * |
| Contrast Exposure | 9 (12.68) | 15 (20.55) | 22 (23.16) | 13 (18.31) | 0.385 |
| AKI Severity and RRT Status at Diagnosis of AKI, n (%) | |||||
| AKI KDIGO Stage 1–2 | 60 (84.51) | 69 (94.52) | 69 (72.63) b | 30 (42.25) a,b,c | <0.001 * |
| AKI KDIGO Stage 3 | 11 (15.49) | 4 (5.48) | 26 (27.37) b | 41 (57.75) a,b,c | <0.001 * |
| RRT within 0–6 Days | 6 (8.45) | 11 (15.07) | 8 (8.42) | 15 (21.13) | 0.057 # |
| Non-AKD (n = 71) | AKD Stage 1 (n = 73) | AKD Stage 2 (n = 95) | AKD Stage 3 (n = 71) | p-Value | |
| Hematologic and Biochemical Profiles at Diagnosis of AKI, Median (IQR) | |||||
| eGFR (mL/min/1.73 m2) | |||||
| Baseline | 81.31 (50.28–107.18) | 56.90 (27.82–90.71) | 70.18 (38.76–101.99) | 85.14 (57.32–127.95) b | 0.003 * |
| At AKI Diagnosis | 26.92 (16.00–40.00) | 20.21 (12.00–34.24) | 21.00 (13.00–36.70) | 19.83 (9.19–32.25) | 0.134 |
| Hemoglobin (g/L) | 103.00 (86.80–124.50) | 98.00 (86.00–111.50) | 100.50 (88.00–118.30) | 99.00 (89.00–113.00) | 0.380 |
| Platelet (109/L) | 159.50 (87.50–259.00) | 165.00 (104.00–273.50) | 169.50 (107.50–255.50) | 183.00 (106.00–236.00) | 0.924 |
| BUN (mmol/L) | 17.49 (10.17–26.15) | 21.78 (13.74–31.42) | 19.99 (12.05–29.01) | 19.99 (13.21–30.70) | 0.592 |
| K (mmol/L) | 4.20 (3.78–4.80) | 4.10 (3.60–4.65) | 4.15 (3.60–5.33) | 4.10 (3.70–5.00) | 0.507 |
| Albumin (g/L) | 30.00 (26.90–35.00) | 29.30 (24.90–33.00) | 29.00 (25.40–33.00) | 28.00 (24.40–33.00) | 0.285 |
| Lactate (mmol/L) | 2.46 (1.37–5.13) | 1.83 (1.35–2.73) | 1.69 (1.08–4.75) | 1.68 (1.25–2.96) | 0.327 |
| pH | 7.42 (7.31–7.49) | 7.41 (7.34–7.45) | 7.37 (7.29–7.45) | 7.37 (7.30–7.43) | 0.106 |
| HCO3 (mmol/L) | 21.10 (17.90–25.48) | 21.20 (17.30–24.10) | 20.90 (16.40–27.23) | 19.80 (15.80–25.30) | 0.907 |
| Bil-T (µmol/L) | 17.10 (10.26–35.92) | 15.39 (9.07–37.63) | 18.81 (10.26–119.73) | 18.81 (9.41–54.73) | 0.688 |
| AKD Stage 1 vs. Non-AKD | AKD Stage 2 vs. Non-AKD | AKD Stage 3 vs. Non-AKD | ||||
| Adjusted OR (95% CI) | p-Value | Adjusted OR (95% CI) | p-Value | Adjusted OR (95% CI) | p-Value | |
| Age (years) | 0.981 (0.957–1.006) | 0.139 | 1.004 (0.980–1.029) | 0.741 | 1.003 (0.976–1.031) | 0.815 |
| Female | 1.155 (0.568–2.347) | 0.691 | 1.217 (0.630–2.354) | 0.559 | 1.141 (0.534–2.438) | 0.733 |
| Diabetes | 1.347 (0.603–3.008) | 0.467 | 1.375 (0.652–2.902) | 0.403 | 0.928 (0.391–2.203) | 0.865 |
| Hypertension | 0.796 (0.358–1.767) | 0.575 | 0.995 (0.475–2.087) | 0.990 | 1.094 (0.468–2.559) | 0.835 |
| CKD | 1.468 (0.518–4.158) | 0.470 | 1.449 (0.586–3.586) | 0.422 | 1.157 (0.417–3.212) | 0.779 |
| AKI KDIGO Stage 1–2 | Reference | Reference | Reference | |||
| AKI KDIGO Stage 3 | 0.368 (0.108–1.263) | 0.112 | 2.243 (0.983–5.117) | 0.055 | 6.214 (2.658–14.526) | <0.001 * |
| RRT within 0–6 Days | 1.480 (0.454–4.829) | 0.515 | 0.915 (0.276–3.037) | 0.885 | 3.366 (1.008–11.242) | 0.049 * |
| Hypovolemia | 0.130 (0.015–1.127) | 0.064 | 0.330 (0.077–1.411) | 0.135 | 0.265 (0.044–1.601) | 0.148 |
| Heart Failure | 1.477 (0.601–3.632) | 0.396 | 1.065 (0.438–2.589) | 0.889 | 0.557 (0.167–1.856) | 0.341 |
| Offending Drugs | 1.934 (0.827–4.522) | 0.128 | 2.314 (1.049–5.107) | 0.038 * | 3.132 (1.304–7.526) | 0.011 * |
| Baseline eGFR (mL/min/1.73 m2) | 0.996 (0.986–1.007) | 0.503 | 1.002 (0.994–1.010) | 0.672 | 1.004 (0.996–1.012) | 0.324 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, P.-C.; Liu, C.-H.; Lee, W.-C.; Wu, C.-H.; Lee, C.-T.; Su, C.-H.; Wang, Y.-C.L.; Tsai, K.-F.; Chiou, T.T.-Y. Predictors of Acute Kidney Disease Severity in Hospitalized Patients with Acute Kidney Injury. Biomedicines 2022, 10, 1081. https://doi.org/10.3390/biomedicines10051081
Hsu P-C, Liu C-H, Lee W-C, Wu C-H, Lee C-T, Su C-H, Wang Y-CL, Tsai K-F, Chiou TT-Y. Predictors of Acute Kidney Disease Severity in Hospitalized Patients with Acute Kidney Injury. Biomedicines. 2022; 10(5):1081. https://doi.org/10.3390/biomedicines10051081
Chicago/Turabian StyleHsu, Pai-Chin, Chih-Han Liu, Wen-Chin Lee, Chien-Hsing Wu, Chien-Te Lee, Chien-Hao Su, Yu-Chin Lily Wang, Kai-Fan Tsai, and Terry Ting-Yu Chiou. 2022. "Predictors of Acute Kidney Disease Severity in Hospitalized Patients with Acute Kidney Injury" Biomedicines 10, no. 5: 1081. https://doi.org/10.3390/biomedicines10051081
APA StyleHsu, P.-C., Liu, C.-H., Lee, W.-C., Wu, C.-H., Lee, C.-T., Su, C.-H., Wang, Y.-C. L., Tsai, K.-F., & Chiou, T. T.-Y. (2022). Predictors of Acute Kidney Disease Severity in Hospitalized Patients with Acute Kidney Injury. Biomedicines, 10(5), 1081. https://doi.org/10.3390/biomedicines10051081