
Immunogenicity, Effectiveness, and Safety of COVID-19 Vaccines in Rheumatic Patients: An Updated Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
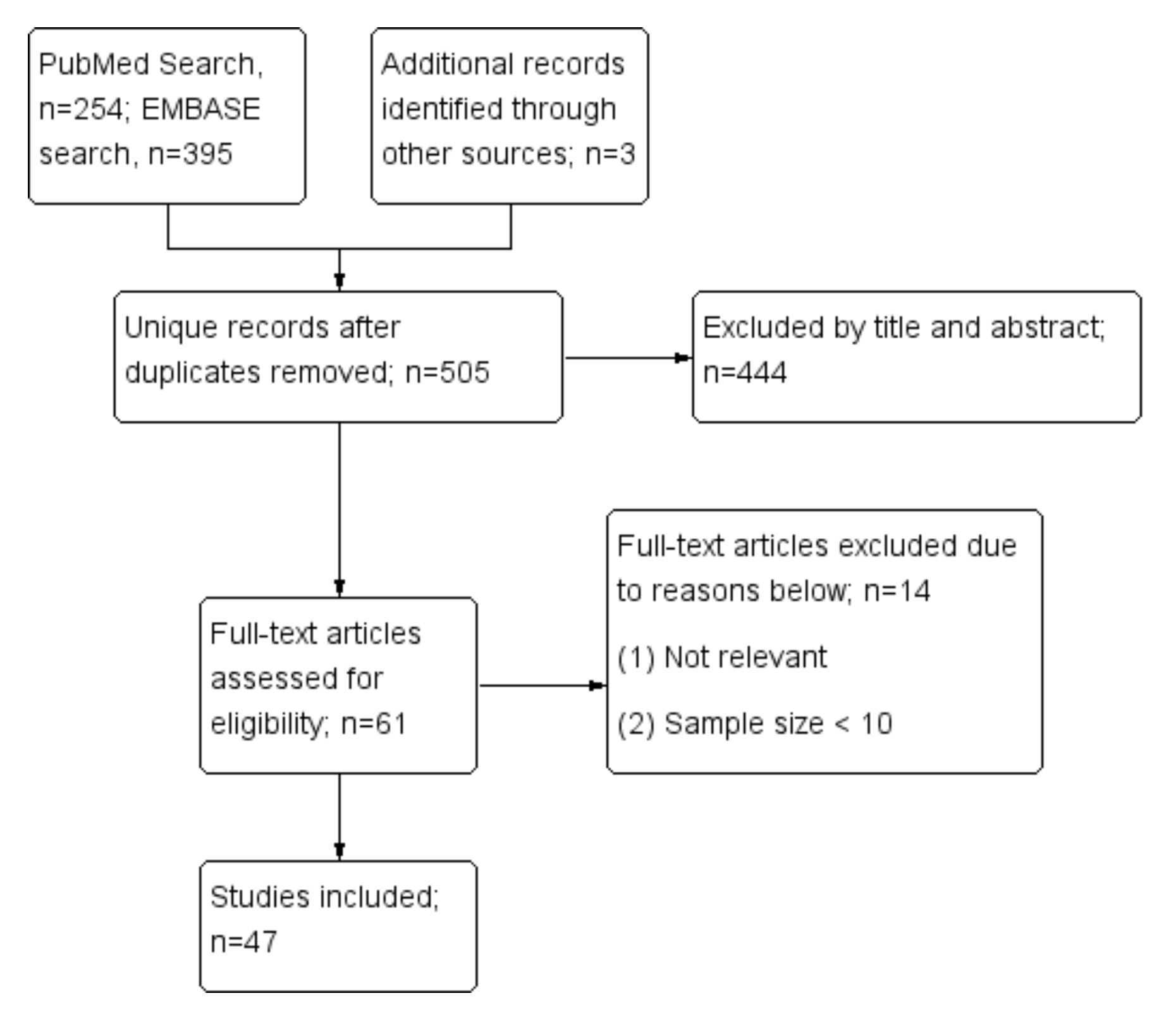
2.1. Literature Search
2.2. Study Selection
2.3. Data Extraction
2.4. Statistical Analysis
3. Results
3.1. Study Characteristics
3.2. Immunogenicity of COVID-19 Vaccines in Rheumatic Patients
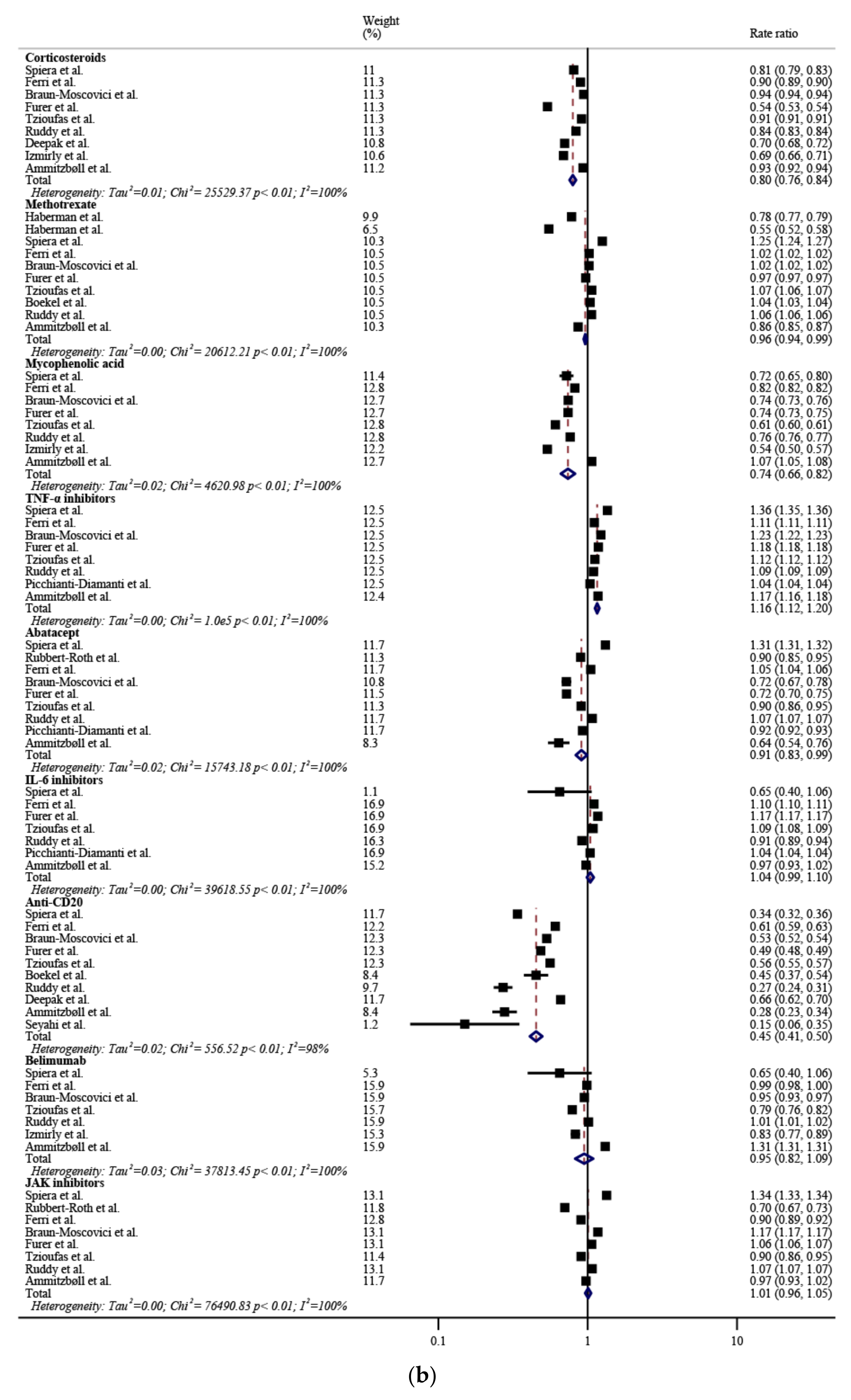
3.3. Influencing Factors of Immunogenicity after COVID-19 Vaccination in Rheumatic Patients
3.4. Effectiveness of COVID-19 Vaccines in Rheumatic Patients
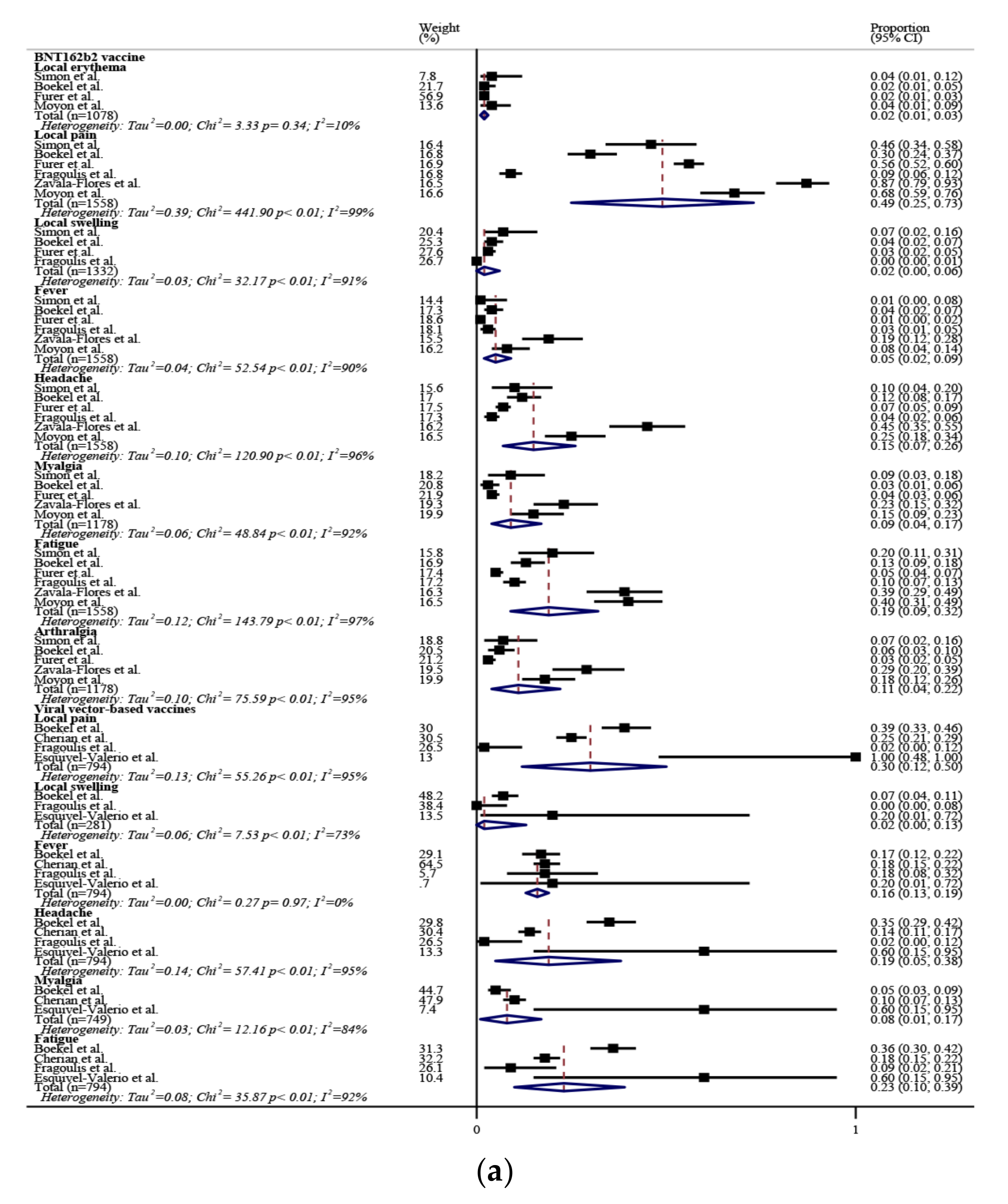
3.5. Adverse Events of COVID-19 Vaccines in Rheumatic Patients
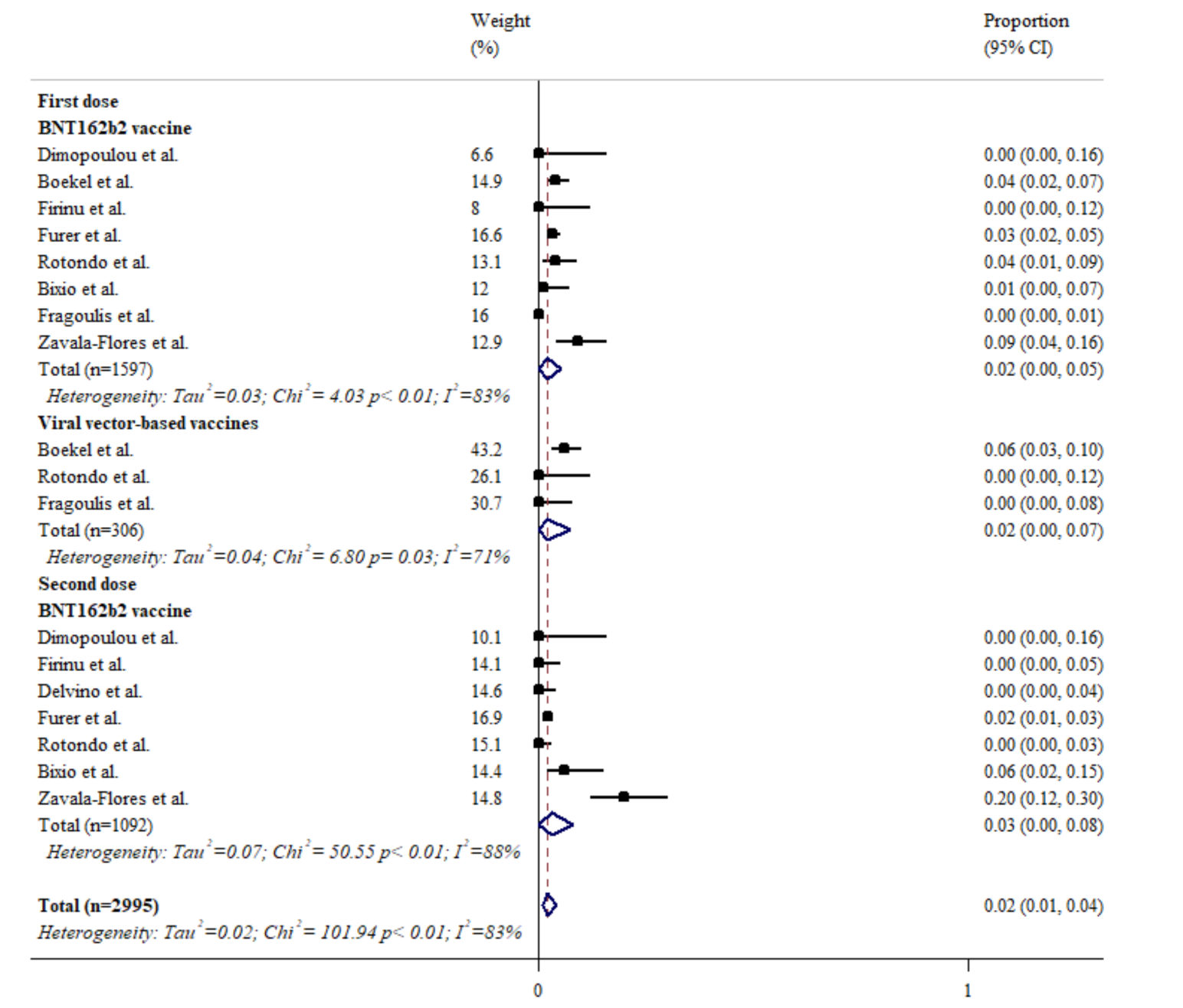
3.6. The Influence of COVID-19 Vaccines on Disease Activity of Rheumatic Diseases
3.7. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sadarangani, M.; Marchant, A.; Kollmann, T.R. Immunological mechanisms of vaccine-induced protection against COVID-19 in humans. Nat. Rev. Immunol. 2021, 21, 475–484. [Google Scholar] [CrossRef] [PubMed]
- Folegatti, P.M.; Ewer, K.J.; Aley, P.K.; Angus, B.; Becker, S.; Belij-Rammerstorfer, S.; Bellamy, D.; Bibi, S.; Bittaye, M.; Clutterbuck, E.A.; et al. Safety and immunogenicity of the ChAdOx1 nCoV-19 vaccine against SARS-CoV-2: A preliminary report of a phase 1/2, single-blind, randomised controlled trial. Lancet 2020, 396, 467–478. [Google Scholar] [CrossRef]
- Jackson, L.A.; Anderson, E.J.; Rouphael, N.G.; Roberts, P.C.; Makhene, M.; Coler, R.N.; McCullough, M.P.; Chappell, J.D.; Denison, M.R.; Stevens, L.J.; et al. An mRNA Vaccine against SARS-CoV-2—Preliminary Report. N. Engl. J. Med. 2020, 383, 1920–1931. [Google Scholar] [CrossRef] [PubMed]
- Zhu, F.-C.; Guan, X.-H.; Li, Y.-H.; Huang, J.-Y.; Jiang, T.; Hou, L.-H.; Li, J.-X.; Yang, B.-F.; Wang, L.; Wang, W.-J.; et al. Immunogenicity and safety of a recombinant adenovirus type-5-vectored COVID-19 vaccine in healthy adults aged 18 years or older: A randomised, double-blind, placebo-controlled, phase 2 trial. Lancet 2020, 396, 479–488. [Google Scholar] [CrossRef]
- Mulligan, M.J.; Lyke, K.E.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Raabe, V.; Bailey, R.; Swanson, K.A.; et al. Phase I/II study of COVID-19 RNA vaccine BNT162b1 in adults. Nature 2020, 586, 589–593. [Google Scholar] [CrossRef] [PubMed]
- Bos, R.; Rutten, L.; van der Lubbe, J.E.M.; Bakkers, M.J.G.; Hardenberg, G.; Wegmann, F.; Zuijdgeest, D.; de Wilde, A.H.; Koornneef, A.; Verwilligen, A.; et al. Ad26 vector-based COVID-19 vaccine encoding a prefusion-stabilized SARS-CoV-2 Spike immunogen induces potent humoral and cellular immune responses. NPJ Vaccines 2020, 5, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Stephenson, K.E.; Le Gars, M.; Sadoff, J.; de Groot, A.M.; Heerwegh, D.; Truyers, C.; Atyeo, C.; Loos, C.; Chandrashekar, A.; McMahan, K.; et al. Immunogenicity of the Ad26.COV2.S Vaccine for COVID. JAMA 2021, 325, 1535. [Google Scholar] [CrossRef] [PubMed]
- Sadoff, J.; Le Gars, M.; Shukarev, G.; Heerwegh, D.; Truyers, C.; de Groot, A.M.; Stoop, J.; Tete, S.; Van Damme, W.; Leroux-Roels, I.; et al. Interim Results of a Phase 1–2a Trial of Ad26.COV2.S Covid-19 Vaccine. N. Engl. J. Med. 2021, 384, 1824–1835. [Google Scholar] [CrossRef] [PubMed]
- Anderson, E.J.; Rouphael, N.G.; Widge, A.T.; Jackson, L.A.; Roberts, P.C.; Makhene, M.; Chappell, J.D.; Denison, M.R.; Stevens, L.J.; Pruijssers, A.J.; et al. Safety and Immunogenicity of SARS-CoV-2 mRNA-1273 Vaccine in Older Adults. N. Engl. J. Med. 2020, 383, 2427–2438. [Google Scholar] [CrossRef]
- Walsh, E.E.; Frenck, R.W., Jr.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R.; et al. Safety and Immunogenicity of Two RNA-Based COVID-19 Vaccine Candidates. N. Engl. J. Med. 2020, 383, 2439–2450. [Google Scholar] [CrossRef]
- Lazarus, R.; Baos, S.; Cappel-Porter, H.; Carson-Stevens, A.; Clout, M.; Culliford, L.; Emmett, S.R.; Garstang, J.; Gbadamoshi, L.; Hallis, B.; et al. Safety and immunogenicity of concomitant administration of COVID-19 vaccines (ChAdOx1 or BNT162b2) with seasonal influenza vaccines in adults in the UK (ComFluCOV): A multicentre, randomised, controlled, phase 4 trial. Lancet 2021, 398, 2277–2287. [Google Scholar] [CrossRef]
- Medeiros-Ribeiro, A.C.; Aikawa, N.E.; Saad, C.G.S.; Yuki, E.F.N.; Pedrosa, T.; Fusco, S.R.G.; Rojo, P.T.; Pereira, R.M.R.; Shinjo, S.K.; Andrade, D.C.O.; et al. Immunogenicity and safety of the CoronaVac inactivated vaccine in patients with autoimmune rheumatic diseases: A phase 4 trial. Nat. Med. 2021, 27, 1744–1751. [Google Scholar] [CrossRef] [PubMed]
- Furer, V.; Eviatar, T.; Zisman, D.; Peleg, H.; Paran, D.; Levartovsky, D.; Zisapel, M.; Elalouf, O.; Kaufman, I.; Meidan, R.; et al. Immunogenicity and safety of the BNT162b2 mRNA COVID-19 vaccine in adult patients with autoimmune inflammatory rheumatic diseases and in the general population: A multicentre study. Ann. Rheum. Dis. 2021, 80, 1330–1338. [Google Scholar] [CrossRef] [PubMed]
- Shinjo, S.K.; de Souza, F.H.C.; Borges, I.B.P.; dos Santos, A.M.; Miossi, R.; Misse, R.G.; Medeiros-Ribeiro, A.C.; Saad, C.G.S.; Yuki, E.F.N.; Pasoto, S.G.; et al. Systemic autoimmune myopathies: A prospective phase 4 controlled trial of an inactivated virus vaccine against SARS-CoV-2. Rheumatology 2021. Epub ahead of print. [Google Scholar] [CrossRef]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Rutherford, M.A.; Scott, J.; Karabayas, M.; Antonelou, M.; Gopaluni, S.; Gray, D.; Barrett, J.; Brix, S.R.; Dhaun, N.; McAdoo, S.P.; et al. Risk Factors for Severe Outcomes in Patients with Systemic Vasculitis and COVID-19: A Binational, Registry-Based Cohort Study. Arthritis Rheumatol. 2021, 73, 1713–1719. [Google Scholar] [CrossRef]
- Ahmed, S.; Gasparyan, A.Y.; Zimba, O. Comorbidities in rheumatic diseases need special consideration during the COVID-19 pandemic. Rheumatol. Int. 2021, 41, 243–256. [Google Scholar] [CrossRef]
- Arnold, J.; Winthrop, K.; Emery, P. COVID-19 vaccination and antirheumatic therapy. Rheumatology 2021, 60, 3496–3502. [Google Scholar] [CrossRef]
- Prendecki, M.; Clarke, C.; Edwards, H.; McIntyre, S.; Mortimer, P.; Gleeson, S.; Martin, P.; Thomson, T.; Randell, P.; Shah, A.; et al. Humoral and T-cell responses to SARS-CoV-2 vaccination in patients receiving immunosuppression. Ann. Rheum. Dis. 2021, 80, 1322–1329. [Google Scholar] [CrossRef]
- Malipiero, G.; Moratto, A.; Infantino, M.; D’Agaro, P.; Piscianz, E.; Manfredi, M.; Grossi, V.; Benvenuti, E.; Bulgaresi, M.; Benucci, M.; et al. Assessment of humoral and cellular immunity induced by the BNT162b2 SARS-CoV-2 vaccine in healthcare workers, elderly people, and immunosuppressed patients with autoimmune disease. Immunol. Res. 2021, 69, 576–583. [Google Scholar] [CrossRef]
- Vijenthira, A.; Gong, I.; Betschel, S.D.; Cheung, M.; Hicks, L.K. Vaccine response following anti-CD20 therapy: A systematic review and meta-analysis of 905 patients. Blood Adv. 2021, 5, 2624–2643. [Google Scholar] [CrossRef] [PubMed]
- Geisen, U.M.; Berner, D.K.; Tran, F.; Sümbül, M.; Vullriede, L.; Ciripoi, M.; Reid, H.M.; Schaffarzyk, A.; Longardt, A.C.; Franzenburg, J.; et al. Immunogenicity and safety of anti-SARS-CoV-2 mRNA vaccines in patients with chronic inflammatory conditions and immunosuppressive therapy in a monocentric cohort. Ann. Rheum. Dis. 2021, 80, 1306–1311. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Dimopoulou, D.; Spyridis, N.; Vartzelis, G.; Tsolia, M.N.; Maritsi, D.N. Safety and tolerability of the COVID -19 messenger RNA vaccine in adolescents with juvenile idiopathic arthritis treated with tumor necrosis factor inhibitors. Arthritis Rheumatol. 2021, 74, 365–366. [Google Scholar] [CrossRef]
- Ammitzbøll, C.; Bartels, L.E.; Andersen, J.B.; Vils, S.R.; Mistegård, C.E.; Johannsen, A.D.; Hermansen, M.-L.F.; Thomsen, M.K.; Hauge, E.; Troldborg, A. Impaired Antibody Response to the BNT162b2 Messenger RNA Coronavirus Disease 2019 Vaccine in Patients with Systemic Lupus Erythematosus and Rheumatoid Arthritis. ACR Open Rheumatol. 2021, 3, 622–628. [Google Scholar] [CrossRef]
- Dimopoulou, D.; Vartzelis, G.; Dasoula, F.; Tsolia, M.; Maritsi, D. Immunogenicity of the COVID-19 mRNA vaccine in adolescents with juvenile idiopathic arthritis on treatment with TNF inhibitors. Ann. Rheum. Dis. 2021, 81, 592–593. [Google Scholar] [CrossRef]
- Bartels, L.E.; Ammitzbøll, C.; Andersen, J.B.; Vils, S.R.; Mistegaard, C.E.; Johannsen, A.D.; Hermansen, M.-L.F.; Thomsen, M.K.; Erikstrup, C.; Hauge, E.-M.; et al. Local and systemic reactogenicity of COVID-19 vaccine BNT162b2 in patients with systemic lupus erythematosus and rheumatoid arthritis. Rheumatol. Int. 2021, 41, 1925–1931. [Google Scholar] [CrossRef]
- Benucci, M.; Damiani, A.; Infantino, M.; Manfredi, M.; Grossi, V.; Lari, B.; Gobbi, F.L.; Sarzi-Puttini, P. Presence of specific T cell response after SARS-CoV-2 vaccination in rheumatoid arthritis patients receiving rituximab. Immunol. Res. 2021, 69, 309–311. [Google Scholar] [CrossRef]
- Bixio, R.; Bertelle, D.; Masia, M.; Pistillo, F.; Carletto, A.; Rossini, M. Incidence of Disease Flare After BNT162b2 Coronavirus Disease 2019 Vaccination in Patients with Rheumatoid Arthritis in Remission. ACR Open Rheumatol. 2021, 3, 832–833. [Google Scholar] [CrossRef]
- Boekel, L.; Kummer, L.Y.; van Dam, K.P.J.; Hooijberg, F.; van Kempen, Z.; Vogelzang, E.H.; Wieske, L.; Eftimov, F.; van Vollenhoven, R.; Kuijpers, T.W.; et al. Adverse events after first COVID-19 vaccination in patients with autoimmune diseases. Lancet Rheumatol. 2021, 3, e542–e545. [Google Scholar] [CrossRef]
- Boekel, L.; Steenhuis, M.; Hooijberg, F.; Besten, Y.R.; van Kempen, Z.L.E.; Kummer, L.Y.; van Dam, K.P.J.; Stalman, E.W.; Vogelzang, E.H.; Cristianawati, O.; et al. Antibody development after COVID-19 vaccination in patients with autoimmune diseases in the Netherlands: A substudy of data from two prospective cohort studies. Lancet Rheumatol. 2021, 3, e778–e788. [Google Scholar] [CrossRef]
- Boyarsky, B.J.; Ruddy, J.A.; Connolly, C.M.; Ou, M.T.; Werbel, W.A.; Garonzik-Wang, J.M.; Segev, D.L.; Paik, J.J. Antibody response to a single dose of SARS-CoV-2 mRNA vaccine in patients with rheumatic and musculoskeletal diseases. Ann. Rheum. Dis. 2021, 80, 1098–1099. [Google Scholar] [CrossRef] [PubMed]
- Braun-Moscovici, Y.; Kaplan, M.; Braun, M.; Markovits, D.; Giryes, S.; Toledano, K.; Tavor, Y.; Dolnikov, K.; Balbir-Gurman, A. Disease activity and humoral response in patients with inflammatory rheumatic diseases after two doses of the Pfizer mRNA vaccine against SARS-CoV-2. Ann. Rheum. Dis. 2021, 80, 1317–1321. [Google Scholar] [CrossRef] [PubMed]
- Bugatti, S.; De Stefano, L.; Balduzzi, S.; Greco, M.I.; Luvaro, T.; Cassaniti, I.; Bogliolo, L.; Mazzucchelli, I.; D’Onofrio, B.; di Lernia, M.; et al. Methotrexate and glucocorticoids, but not anticytokine therapy, impair the immunogenicity of a single dose of the BNT162b2 mRNA COVID-19 vaccine in patients with chronic inflammatory arthritis. Ann. Rheum. Dis. 2021, 80, 17–19. [Google Scholar] [CrossRef] [PubMed]
- Cherian, S.; Paul, A.; Ahmed, S.; Alias, B.; Manoj, M.; Santhosh, A.K.; Varghese, D.R.; Krishnan, N.; Shenoy, P. Safety of the ChAdOx1 nCoV-19 and the BBV152 vaccines in 724 patients with rheumatic diseases: A post-vaccination cross-sectional survey. Rheumatol. Int. 2021, 41, 1441–1445. [Google Scholar] [CrossRef] [PubMed]
- Chiang, T.P.-Y.; Connolly, C.M.; Ruddy, J.A.; Boyarsky, B.J.; Alejo, J.L.; Werbel, W.A.; Massie, A.; Christopher-Stine, L.; Garonzik-Wang, J.; Segev, D.L.; et al. Antibody response to the Janssen/Johnson & Johnson SARS-CoV-2 vaccine in patients with rheumatic and musculoskeletal diseases. Ann. Rheum. Dis. 2021, 80, 1365–1366. [Google Scholar] [CrossRef]
- Connolly, C.M.; Ruddy, J.A.; Boyarsky, B.J.; Barbur, I.; Werbel, W.A.; Geetha, D.; Garonzik-Wang, J.M.; Segev, D.L.; Christopher-Stine, L.; Paik, J.J. Disease Flare and Reactogenicity in Patients with Rheumatic and Musculoskeletal Diseases Following Two-Dose SARS & CoV -2 Messenger RNA Vaccination. Arthritis Rheumatol. 2021, 74, 28–32. [Google Scholar] [CrossRef] [PubMed]
- Atteno, M.; Raimondo, M.; Mangiacapra, S.; Cannavacciuolo, F.; Nunziata, M.; Iorio, V.; Iuliano, N.; Tibullo, L.; Mastroianni, M.; Amitrano, M. Safety profile of pfizer-biontech covid-19 vaccine in patients with rheumatic diseases: Preliminary assessment. Ann. Rheum. Dis. 2021, 80, 907–908. [Google Scholar]
- Deepak, M.P.; Kim, W.; Paley, M.A.; Yang, M.; Carvidi, B.A.B.; Demissie, B.E.G.; El-Qunni, B.A.A.; Haile, B.A.; Huang, B.K.; Kinnett, B.B.; et al. Effect of Immunosuppression on the Immunogenicity of mRNA Vaccines to SARS-CoV-2: A Prospective Cohort Study. Ann. Intern. Med. 2021, 174, 1572–1585. [Google Scholar] [CrossRef] [PubMed]
- Delvino, P.; Bozzalla Cassione, E.; Biglia, A.; Quadrelli, V.S.; Bartoletti, A.; Montecucco, C.; Monti, S. Safety of BNT162b2 mRNA COVID-19 vaccine in a cohort of elderly, immunocompromised patients with systemic vasculitis. Clin. Exp. Rheumatol. 2021. Available online: https://pubmed.ncbi.nlm.nih.gov/34528506/ (accessed on 10 February 2022).
- Embi, P.J.; Levy, M.E.; Naleway, A.L.; Patel, P.; Gaglani, M.; Natarajan, K.; Dascomb, K.; Ong, T.C.; Klein, N.P.; Liao, I.-C.; et al. Effectiveness of 2-Dose Vaccination with mRNA COVID-19 Vaccines Against COVID-19–Associated Hospitalizations Among Immunocompromised Adults—Nine States, January–September 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 1553–1559. [Google Scholar] [CrossRef]
- Esquivel-Valerio, J.A.; Skinner-Taylor, C.M.; Moreno-Arquieta, I.A.; la Garza, J.A.C.-D.; Garcia-Arellano, G.; Gonzalez-Garcia, P.L.; Almaraz-Juarez, F.d.R.; Galarza-Delgado, D.A. Adverse events of six COVID-19 vaccines in patients with autoimmune rheumatic diseases: A cross-sectional study. Rheumatol. Int. 2021, 41, 2105–2108. [Google Scholar] [CrossRef] [PubMed]
- Ferri, C.; Ursini, F.; Gragnani, L.; Raimondo, V.; Giuggioli, D.; Foti, R.; Caminiti, M.; Olivo, D.; Cuomo, G.; Visentini, M.; et al. Impaired immunogenicity to COVID-19 vaccines in autoimmune systemic diseases. High prevalence of non-response in different patients’ subgroups. J. Autoimmun. 2021, 125, 102744. [Google Scholar] [CrossRef] [PubMed]
- Firinu, D.; Perra, A.; Campagna, M.; Littera, R.; Fenu, G.; Meloni, F.; Cipri, S.; Sedda, F.; Conti, M.; Miglianti, M.; et al. Evaluation of antibody response to BNT162b2 mRNA COVID-19 vaccine in patients affected by immune-mediated inflammatory diseases up to 5 months after vaccination. Clin. Exp. Med. 2021. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Fragoulis, G.E.; Bournia, V.-K.; Mavrea, E.; Evangelatos, G.; Fragiadaki, K.; Karamanakos, A.; Kravariti, E.; Laskari, K.; Panopoulos, S.; Pappa, M.; et al. COVID-19 vaccine safety and nocebo-prone associated hesitancy in patients with systemic rheumatic diseases: A cross-sectional study. Rheumatol. Int. 2021, 42, 31–39. [Google Scholar] [CrossRef]
- Haberman, R.H.; Herati, R.; Simon, D.; Samanovic, M.; Blank, R.B.; Tuen, M.; Koralov, S.B.; Atreya, R.; Tascilar, K.; Allen, J.R.; et al. Methotrexate hampers immunogenicity to BNT162b2 mRNA COVID-19 vaccine in immune-mediated inflammatory disease. Ann. Rheum. Dis. 2021, 80, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Izmirly, P.M.; Kim, M.Y.; Samanovic, M.; Fernandez-Ruiz, R.; Ohana, S.; Deonaraine, K.K.; Engel, A.J.; Masson, M.; Xie, X.; Cornelius, A.R.; et al. Evaluation of Immune Response and Disease Status in Systemic Lupus Erythematosus Patients Following SARS – CoV -2 Vaccination. Arthritis Rheumatol. 2021, 74, 284–294. [Google Scholar] [CrossRef]
- Kant, S.; Ravi, S.; Geetha, D. The SARS-CoV-2 Vaccine Response in ANCA-Associated Vasculitis. J. Am. Soc. Nephrol. 2021, 32, PO0148. [Google Scholar]
- Li, X.; Tong, X.; Yeung, W.W.Y.; Kuan, P.; Yum, S.H.H.; Chui, C.S.L.; Lai, F.T.T.; Wan, E.Y.F.; Wong, C.K.H.; Chan, E.W.Y.; et al. Two-dose COVID-19 vaccination and possible arthritis flare among patients with rheumatoid arthritis in Hong Kong. Ann. Rheum. Dis. 2021, 81, 564–568. [Google Scholar] [CrossRef] [PubMed]
- Machado, P.M.; Lawson-Tovey, S.; Hyrich, K.; Carmona, L.; Gossec, L.; Mateus, E.; Strangfeld, A.; Raffeiner, B.; Goulenok, T.; Brocq, O.; et al. Mariette COVID-19 vaccine safety in patients with rheumatic and musculoskeletal disease. Ann. Rheum. Dis. 2021, 80, 199–200. [Google Scholar] [CrossRef]
- Moyon, Q.; Sterlin, D.; Miyara, M.; Anna, F.; Mathian, A.; Lhote, R.; Ghillani-Dalbin, P.; Breillat, P.; Mudumba, S.; de Alba, S.; et al. BNT162b2 vaccine-induced humoral and cellular responses against SARS-CoV-2 variants in systemic lupus erythematosus. Ann. Rheum. Dis. 2021, 81, 575–583. [Google Scholar] [CrossRef]
- Mrak, D.; Tobudic, S.; Koblischke, M.; Graninger, M.; Radner, H.; Sieghart, D.; Hofer, P.; Perkmann, T.; Haslacher, H.; Thalhammer, R.; et al. SARS-CoV-2 vaccination in rituximab-treated patients: B cells promote humoral immune responses in the presence of T-cell-mediated immunity. Ann. Rheum. Dis. 2021, 80, 1345–1350. [Google Scholar] [CrossRef] [PubMed]
- Papagoras, C.; Fragoulis, G.E.; Zioga, N.; Simopoulou, T.; Deftereou, K.; Kalavri, E.; Zampeli, E.; Gerolymatou, N.; Kataxaki, E.; Melissaropoulos, K.; et al. Better outcomes of COVID-19 in vaccinated compared to unvaccinated patients with systemic rheumatic diseases. Ann. Rheum. Dis. Epub ahead of print. 2021. [Google Scholar] [CrossRef] [PubMed]
- Picchianti-Diamanti, A.; Aiello, A.; Laganà, B.; Agrati, C.; Castilletti, C.; Meschi, S.; Farroni, C.; Lapa, D.; Fard, S.N.; Cuzzi, G.; et al. ImmunosuppressiveTherapies Differently Modulate Humoral- and T-Cell-Specific Responses to COVID-19 mRNA Vaccine in Rheumatoid Arthritis Patients. Front. Immunol. 2021, 12, 740249. [Google Scholar] [CrossRef]
- Rotondo, C.; Cantatore, F.; Fornaro, M.; Colia, R.; Busto, G.; Rella, V.; Sciacca, S.; Lops, L.; Cici, D.; Maruotti, N.; et al. Preliminary Data on Post Market Safety Profiles of COVID 19 Vaccines in Rheumatic Diseases: Assessments on Various Vaccines in Use, Different Rheumatic Disease Subtypes, and Immunosuppressive Therapies: A Two-Centers Study. Vaccines 2021, 9, 730. [Google Scholar] [CrossRef] [PubMed]
- Rubbert-Roth, A.; Vuilleumier, N.; Ludewig, B.; Schmiedeberg, K.; Haller, C.; von Kempis, J. Anti-SARS-CoV-2 mRNA vaccine in patients with rheumatoid arthritis. Lancet Rheumatol. 2021, 3, e470–e472. [Google Scholar] [CrossRef]
- Ruddy, J.A.; Connolly, C.M.; Boyarsky, B.J.; Werbel, W.A.; Christopher-Stine, L.; Garonzik-Wang, J.; Segev, D.L.; Paik, J.J. High antibody response to two-dose SARS-CoV-2 messenger RNA vaccination in patients with rheumatic and musculoskeletal diseases. Ann. Rheum. Dis. 2021, 80, 1351–1352. [Google Scholar] [CrossRef]
- Sattui, S.E.; Liew, J.W.; Kennedy, K.; Sirotich, E.; Putman, M.; Moni, T.T.; Akpabio, A.; Alpízar-Rodríguez, D.; Berenbaum, F.; Bulina, I.; et al. Early experience of COVID-19 vaccination in adults with systemic rheumatic diseases: Results from the COVID-19 Global Rheumatology Alliance Vaccine Survey. RMD Open 2021, 7, e001814. [Google Scholar] [CrossRef]
- Schmiedeberg, K.; Vuilleumier, N.; Pagano, S.; Albrich, W.C.; Ludewig, B.; von Kempis, J.; Rubbert-Roth, A. Efficacy and tolerability of a third dose of an mRNA anti-SARS-CoV-2 vaccine in patients with rheumatoid arthritis with absent or minimal serological response to two previous doses. Lancet Rheumatol. 2021, 4, e11–e13. [Google Scholar] [CrossRef]
- Sciascia, S.; Costanzo, P.; Radin, M.; Schreiber, K.; Pini, M.; Vaccarino, A.; Cecchi, I.; Baldovino, S.; Roccatello, D. Safety and tolerability of mRNA COVID-19 vaccines in people with antiphospholipid antibodies. Lancet Rheumatol. 2021, 3, e832. [Google Scholar] [CrossRef]
- Seyahi, E.; Bakhdiyarli, G.; Oztas, M.; Kuskucu, M.A.; Tok, Y.; Sut, N.; Ozcifci, G.; Ozcaglayan, A.; Balkan, I.I.; Saltoglu, N.; et al. Antibody response to inactivated COVID-19 vaccine (CoronaVac) in immune-mediated diseases: A controlled study among hospital workers and elderly. Rheumatol. Int. 2021, 41, 1429–1440. [Google Scholar] [CrossRef]
- Simon, D.; Tascilar, K.; Krönke, G.; Kleyer, A.; Zaiss, M.M.; Heppt, F.; Meder, C.; Atreya, R.; Klenske, E.; Dietrich, P.; et al. Patients with immune-mediated inflammatory diseases receiving cytokine inhibitors have low prevalence of SARS-CoV-2 seroconversion. Nat. Commun. 2020, 11, 3774. [Google Scholar] [CrossRef] [PubMed]
- Tzioufas, A.G.; Bakasis, A.-D.; Goules, A.V.; Bitzogli, K.; Cinoku, I.I.; Chatzis, L.G.; Argyropoulou, O.D.; Venetsanopoulou, A.I.; Mavrommati, M.; Stergiou, I.E.; et al. A prospective multicenter study assessing humoral immunogenicity and safety of the mRNA SARS-CoV-2 vaccines in Greek patients with systemic autoimmune and autoinflammatory rheumatic diseases. J. Autoimmun. 2021, 125, 102743. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Katz, P.; Paez, D.; Carvidi, A.; Matloubian, M.; Nakamura, M.; Gensler, L.S. Gensler Reactogenicity of SARS-COV-2 vaccines in patients with autoimmune and inflammatory disease. Ann. Rheum. Dis. 2021, 80, 911. [Google Scholar] [CrossRef]
- Zavala-Flores, E.; Salcedo-Matienzo, J.; Quiroz-Alva, A.; Berrocal-Kasay, A. Side effects and flares risk after SARS-CoV-2 vaccination in patients with systemic lupus erythematosus. Clin. Rheumatol. 2021, 1–9. [Google Scholar] [CrossRef]
- Attauabi, M.; Seidelin, J.B.; Felding, O.K.; Wewer, M.D.; Arp, L.K.V.; Sarikaya, M.Z.; Egeberg, A.; Vladimirova, N.; Bendtsen, F.; Burisch, J. Coronavirus disease 2019, immune-mediated inflammatory diseases and immunosuppressive therapies – A Danish population-based cohort study. J. Autoimmun. 2021, 118, 102613. [Google Scholar] [CrossRef] [PubMed]
- Curtis, J.R.; Johnson, S.R.; Anthony, D.D.; Arasaratnam, R.J.; Baden, L.R.; Bass, A.R.; Calabrese, C.; Gravallese, E.M.; Harpaz, R.; Kroger, A.; et al. American College of Rheumatology Guidance for COVID-19 Vaccination in Patients with Rheumatic and Musculoskeletal Diseases: Version 3. Arthritis Rheumatol. 2021, 73, e60–e75. [Google Scholar] [CrossRef] [PubMed]
- Furer, V.; Rondaan, C.; Heijstek, M.W.; Agmon-Levin, N.; Van Assen, S.; Bijl, M.; Breedveld, F.C.; D’Amelio, R.; Dougados, M.; Kapetanovic, M.C.; et al. 2019 update of EULAR recommendations for vaccination in adult patients with autoimmune inflammatory rheumatic diseases. Ann. Rheum. Dis. 2020, 79, 39–52. [Google Scholar] [CrossRef]
- Hua, C.; Barnetche, T.; Combe, B.; Morel, J. Effect of Methotrexate, Anti-Tumor Necrosis Factor α, and Rituximab on the Immune Response to Influenza and Pneumococcal Vaccines in Patients with Rheumatoid Arthritis: A Systematic Review and Meta-Analysis. Arthritis Care Res. 2014, 66, 1016–1026. [Google Scholar] [CrossRef]
- Grupper, A.; Rabinowich, L.; Schwartz, D.; Schwartz, I.F.; Ben-Yehoyada, M.; Shashar, M.; Katchman, E.; Halperin, T.; Turner, D.; Goykhman, Y.; et al. Reduced humoral response to mRNA SARS-CoV-2 BNT162b2 vaccine in kidney transplant recipients without prior exposure to the virus. Arab. Archaeol. Epigr. 2021, 21, 2719–2726. [Google Scholar] [CrossRef]
- Peled, Y.; Ram, E.; Lavee, J.; Sternik, L.; Segev, A.; Wieder-Finesod, A.; Mandelboim, M.; Indenbaum, V.; Levy, I.; Raanani, E.; et al. BNT162b2 vaccination in heart transplant recipients: Clinical experience and antibody response. J. Heart Lung Transplant. 2021, 40, 759–762. [Google Scholar] [CrossRef]
- Felten, R.; Dubois, M.; Ugarte-Gil, M.F.; Chaudier, A.; Kawka, L.; Bergier, H.; Costecalde, C.; Pijnenburg, L.; Fort, J.; Chatelus, E.; et al. Vaccination against COVID-19: Expectations and concerns of patients with autoimmune and rheumatic diseases. Lancet Rheumatol. 2021, 3, e243–e245. [Google Scholar] [CrossRef]
- Wu, Q.; Dudley, M.Z.; Chen, X.; Bai, X.; Dong, K.; Zhuang, T.; Salmon, D.; Yu, H. Evaluation of the safety profile of COVID-19 vaccines: A rapid review. BMC Med. 2021, 19, 173. [Google Scholar] [CrossRef] [PubMed]
- Capone, F.; Lucchini, M.; Ferraro, E.; Bianco, A.; Rossi, M.; Cicia, A.; Cortese, A.; Cruciani, A.; De Arcangelis, V.; De Giglio, L.; et al. Immunogenicity and safety of mRNA COVID-19 vaccines in people with multiple sclerosis treated with different disease-modifying therapies. Neurotherapeutics 2021, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Sormani, M.P.; Schiavetti, I.; Landi, D.; Carmisciano, L.; De Rossi, N.; Cordioli, C.; Moiola, L.; Radaelli, M.; Immovilli, P.; Capobianco, M.; et al. SARS-CoV-2 serology after COVID-19 in multiple sclerosis: An international cohort study. Mult. Scler. J. 2021, 13524585211035318. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Country | Sample Size of Rheumatic Patients (n) | Proportion of Female | Mean/Median Age (Years) | Vaccine | Rheumatic Diseases | Humoral Immunogenecity Measurement | Cellular Immunogenecity Measurement | Documentation of Adverse Events |
|---|---|---|---|---|---|---|---|---|---|
| Ammitzbøll et al. [25] | Denmark | 134 | 72% | 66 | BNT | RA 54%, and SLE 46% | Anti-SARS-CoV-2 antibody CLIA (Ortho Clinical Diagnostics) | N.A. | N.A. |
| Barbhaiya et al. [26] | USA | 1101 | 81% | 61 | BNT 54%, Moderna 44%, J&J 2%, and AZ 0.3% | N.A. | N.A. | N.A. | Online survey |
| Bartels et al. [27] | Denmark | 282 | 79% | 59 | BNT | RA 55%, and SLE 45% | N.A. | N.A. | Questionnaire |
| Benucci et al. [28] | Italy | 14 | N.A. | 57 | BNT | RA | Anti-RBD IgG antibodies FEIA (ThermoFisher) | IGRA (Euroimmun) | N.A. |
| Bixio et al. [29] | Italy | 77 | 81% | 62 | BNT | RA | N.A. | N.A. | Clinical record |
| Boekel et al. [30] | Netherlands | 505 | 65% | 64 | AZ 46%, BNT 41%, and Moderna 13% | RA 40%, PsA 10%, and MS 16% | N.A. | N.A. | Online questionnaire |
| Boekel et al. [31] | Netherlands | 632 | 67% | 63 | AZ 54%, BNT 38%, and Moderna 8% | RA 41%, PsA 11%, AS 11%, and MS 9% | Anti-RBD IgG antibody ELISA (in-house) | N.A. | N.A. |
| Boyarsky et al. [32] | USA | 123 | 95% | 50 | BNT 52%, and Moderna 48% | Inflammatory arthritis 28%, overlap syndrome 29%, SLE 20%, and PSS 13% | Anti-RBD antibody ECLIA (Roche) | N.A. | N.A. |
| Braun-Moscovici et al. [33] | Isreal | 264 | 76% | 58 | BNT | RA 37%, PsA 12%, and SpA 8% | Anti-RBD IgG CLIA (Abbott) | N.A. | Clinical record |
| Bugatti et al. [34] | Italy | 140 | 68% | 56 | BNT | RA 59%, PsA 21%, and SpA 20% | Anti-S1/S2 protein antibodys IgG CLIA (DiaSorin) | N.A. | N.A. |
| Cherian et al. [35] | India | 513 | 83% | 58 | AZ 87%, and Covaxin 10% | RA 44%, inflammatory arthritis 16%, SpA 13%, and SLE 10%, | N.A. | N.A. | Clinical record |
| Chiang et al. [36] | USA | 1039 | 94% | 46 | mRNA vaccines 96%, and J&J 4% | Inflammatory arthritis 44%, overlap syndrome 21%, SLE 21%, and PSS 5% | Anti-RBD antibody ECLIA (Roche) | N.A. | N.A. |
| Connolly et al. [37] | USA | 1377 | 92% | 47 | BNT 55%, and Moderna 45% | Inflammatory arthriitis 47%, SLE 20%, and overlap syndrome 20% | N.A. | N.A. | Online questionnaire |
| Cuomo et al. [38] | Italy | 27 | 78% | 49 | BNT | Inflammaory arthritis 48%, RA 22%, and SSc 19% | N.A. | N.A. | Telephone interview |
| Deepak et al. [39] | USA | 133 | 74% | 46 | mRNA vaccines | IBD 32%, RA 29%, SpA 15%, and SLE 11% | Anti-S protein IgG ELISA (in-house) | N.A. | N.A. |
| Delvino et al. [40] | Italy | 81 | 68% | 76 | BNT | GCA | N.A. | N.A. | Written questionnaire |
| Dimopoulou et al. [24] | Greece | 21 | 76% | 17 | BNT | JIA | N.A. | N.A. | N.A. |
| Embi et al. [41] | USA | 5024 | N.A. | N.A. | Moderna 40%, and BNT 60% | Rheumatic or inflammatory disorders | N.A. | N.A. | N.A. |
| Esquivel-Valerio et al. [42] | Mexico | 225 | 95% | 51 | BNT 48%, Convidecia 13%, Moderna 13%, AZ 12%, CoronaVac 10%, and J&J 2% | RA 59%, SLE 11%, and axial SpA 10% | N.A. | N.A. | Survey |
| Ferri et al. [43] | Italy | 478 | 84% | 59 | BNT 94%, and Moderna 6% | SSc 55%, RA 21%, CV 13%, and SLE 8%, | Anti- S1/S2 protein antibodys IgG CLIA (Abbott) | N.A. | Telephone interview |
| Firinu et al. [44] | Italy | 95 | 73% | 56 | BNT | SLE 24%, RA 24%, PsA, PsO and AS 25% | Anti-RBD IgG CLIA (Snibe Diagnostics) | N.A. | N.A. |
| Fragoulis et al. [45] | Greece | 441 | 76% | 56 | BNT 86%, AZ 10%, Moderna 3%, and J&J 1% | Inflammatory arthritis 59%, CTD 27%, and vasculitis 11% | N.A. | N.A. | Telephone interview |
| Furer et al. [13] | Isreal | 686 | 69% | 59 | BNT | RA 38%, PsA 24%, SLE 15%, vasculitis 10%, and SpA 10% | Anti-S1/S2 protein antibodys IgG CLIA (DiaSorin) | N.A. | Telephone questionnaire |
| Geisen et al. [22] | Germany | 26 | 64% | 51 | 81% BNT, and Moderna 19% | RA 31%, PsO 12%, SpA 12%, and IBD 12% | Anti-SARS-CoV-2 ELISA (Euroimmun) | N.A. | Online survey |
| Haberman et al. [46] | USA | 51 | 71% | 56 | BNT | RA 43%, and PsO/PsA 47% | Anti-S1 protein antibody ELISA (in-house) | N.A. | N.A. |
| Germany | 31 | 71% | 51 | BNT | GCA and PMR | Anti-S1 protein antibody ELISA (Euroimmun) | N.A. | N.A. | |
| Izmirly et al. [47] | USA | 90 | 88% | 46 | BNT 68%, Moderna 15%, and J&J 5.5% | SLE | Anti-RBD IgG ELISA (in-house) | IFN-γ ELISpot assay (in-house) | N.A. |
| Kant et al. [48] | USA | 48 | 35% | 67 | Moderna 52%, BNT 40%, and J&J 8% | AAV | N.A. | N.A. | N.A. |
| Li et al. [49] | Hong Kong | 1324 | 75% | 58 | CoronaVac 51%, and BNT 49%, | RA | N.A. | N.A. | Clinical record |
| Machado et al. [50] | EULAR COVID-19 Vaccination Registry | 1519 | 68% | 63 | BNT 78%, AZ 16%, and Moderna 5% | Inflammatory arthritis 51%, CTD 19%, and vasculitis 16% | N.A. | N.A. | Clinical record |
| Medeiros-Ribeiro et al. [12] | Brazil | 910 | 77% | 51 | CoronaVac | Inflammatory arthritis 50% | Anti-S1/S2 protein antibodys IgG CLIA (DiaSorin) | N.A. | Diary |
| Moyon et al. [51] | France | 126 | 91% | 47 | BNT | SLE | SARS-CoV-2 multi-antigenphotonic ring immunoassay(Genalyte) | IGRA (Qiagen) | Clinical record |
| Mrak et al. [52] | Austria | 45 | 78% | 64 | BNT 82%, and Moderna 18% | RA 53%, CTD 27%, and vasculitis 16% | N.A. | IFN-γ ELISpot assay (in-house) | N.A. |
| Papagoras et al. [53] | Greece | 48 | 69% | 51 | BNT 79%, and AZ 21% | Inflammatory arthritis 58%, CTD and vasculitis 40% | N.A. | N.A. | N.A. |
| Picchianti-Diamanti et al. [54] | Italy | 35 | 77% | 59 | BNT | RA | Anti-RBD IgG CLIA (Abbott) | IFN-γ whole-blood assay (in-house) | N.A. |
| Prendecki et al. [19] | UK | 119 | 48% | 53 | mRNA vaccines 71%, and AZ 29%, | AAV/anti-GBM 38%, MCD/FSGS 24%, MGN 19%, and SLE 16% | Anti-S1/S2 protein antibodys IgG CLIA (Abbott) | T SPOT (Oxford Immunotec) | N.A. |
| Rotondo et al. [55] | Italy | 137 | 70% | 57 | BNT 78%, and AZ 22% | Arthritis 78%, and CTD 18% | N.A. | N.A. | Questionnaire |
| Rubbert-Roth et al. [56] | Switzerland | 53 | 55% | 65 | BNT 83%, and Moderna 17% | RA | Anti-RBD antibody ECLIA (Roche) | N.A. | N.A. |
| Ruddy et al. [57] | USA | 404 | 96% | 44 | Moderna 51%, and BNT 49% | Inflammatory arthritis 45%, and SLE 22% | Anti-RBD antibody ECLIA (Roche) | N.A. | N.A. |
| Sattui et al. [58] | Global RheumatologyAlliance | 2860 | 87% | 55 | BNT 53%, AZ 23%, Moderna 21%, and J&J 2% | RA 42%, IIM 17%, PSS 15%, and SLE 14% | N.A. | N.A. | Online survey |
| Schmiedeberg et al. [59] | Switzerland | 17 | 47% | 67 | BNT 82%, and Moderna 12% | RA | Anti-RBD antibody ECLIA (Roche) | N.A. | N.A. |
| Sciascia et al. [60] | Italy | 102 | 85% | 52 | BNT 66%, and Moderna 34% | APS 51%, and aPL 49% | N.A. | N.A. | Clinical record |
| Seyahi et al. [61] | Turkey | 104 | 66% | 48 | CoronaVac | SpA 23%, RA 18%, CTD 16%, BS 14%, and FMF 10% | Anti-RBD antibody ECLIA (Roche) | N.A. | N.A. |
| Simon et al. [62] | Germany | 84 | 66% | 53 | BNT | SpA 32%, RA 30%, IBD 10%, and PsO 10% | Anti-S1 protein antibody ELISA (Euroimmun) | N.A. | Clinical record |
| Spiera et al. [59] | USA | 89 | 76% | 61 | BNT 57%, and Moderna 43% | RA 26%, GPA 13%, PSS 11%, and SLE 10% | Anti-RBD antibody ECLIA (Roche) | N.A. | N.A. |
| Tzioufas et al. [63] | Greece | 605 | 71% | 58 | BNT 95%, and Moderna 5% | RA 28%, seronegative arthritis 21%, SLE 20%, and vasculitis 11%, | Anti-S1 protein antibody ELISA (Euroimmun) | N.A. | Questionnaire |
| Yang et al. [64] | USA | 70 | 69% | 48 | mRNA vaccines | RA 30%, SpA 30%, SLE 11%, and IBD 10% | N.A. | N.A. | Clinical record |
| Zavala-Flores et al. [65] | Peru | 100 | 94% | 39 | BNT | SLE | N.A. | N.A. | Clinical record |
| Factors |
|---|
| Older age |
| Lower B lymphocyte count |
| Lower serum IgG |
| Shorter interval between vaccination and last infusion of anti-CD20 therapy |
| Not achieving B cell reconstitution after anti-CD20 therapy |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tang, K.-T.; Hsu, B.-C.; Chen, D.-Y. Immunogenicity, Effectiveness, and Safety of COVID-19 Vaccines in Rheumatic Patients: An Updated Systematic Review and Meta-Analysis. Biomedicines 2022, 10, 834. https://doi.org/10.3390/biomedicines10040834
Tang K-T, Hsu B-C, Chen D-Y. Immunogenicity, Effectiveness, and Safety of COVID-19 Vaccines in Rheumatic Patients: An Updated Systematic Review and Meta-Analysis. Biomedicines. 2022; 10(4):834. https://doi.org/10.3390/biomedicines10040834
Chicago/Turabian StyleTang, Kuo-Tung, Bo-Chueh Hsu, and Der-Yuan Chen. 2022. "Immunogenicity, Effectiveness, and Safety of COVID-19 Vaccines in Rheumatic Patients: An Updated Systematic Review and Meta-Analysis" Biomedicines 10, no. 4: 834. https://doi.org/10.3390/biomedicines10040834
APA StyleTang, K.-T., Hsu, B.-C., & Chen, D.-Y. (2022). Immunogenicity, Effectiveness, and Safety of COVID-19 Vaccines in Rheumatic Patients: An Updated Systematic Review and Meta-Analysis. Biomedicines, 10(4), 834. https://doi.org/10.3390/biomedicines10040834