
Novel Biomarkers Detected by Proteomics Predict Death and Cardiovascular Events in Hemodialysis Patients

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
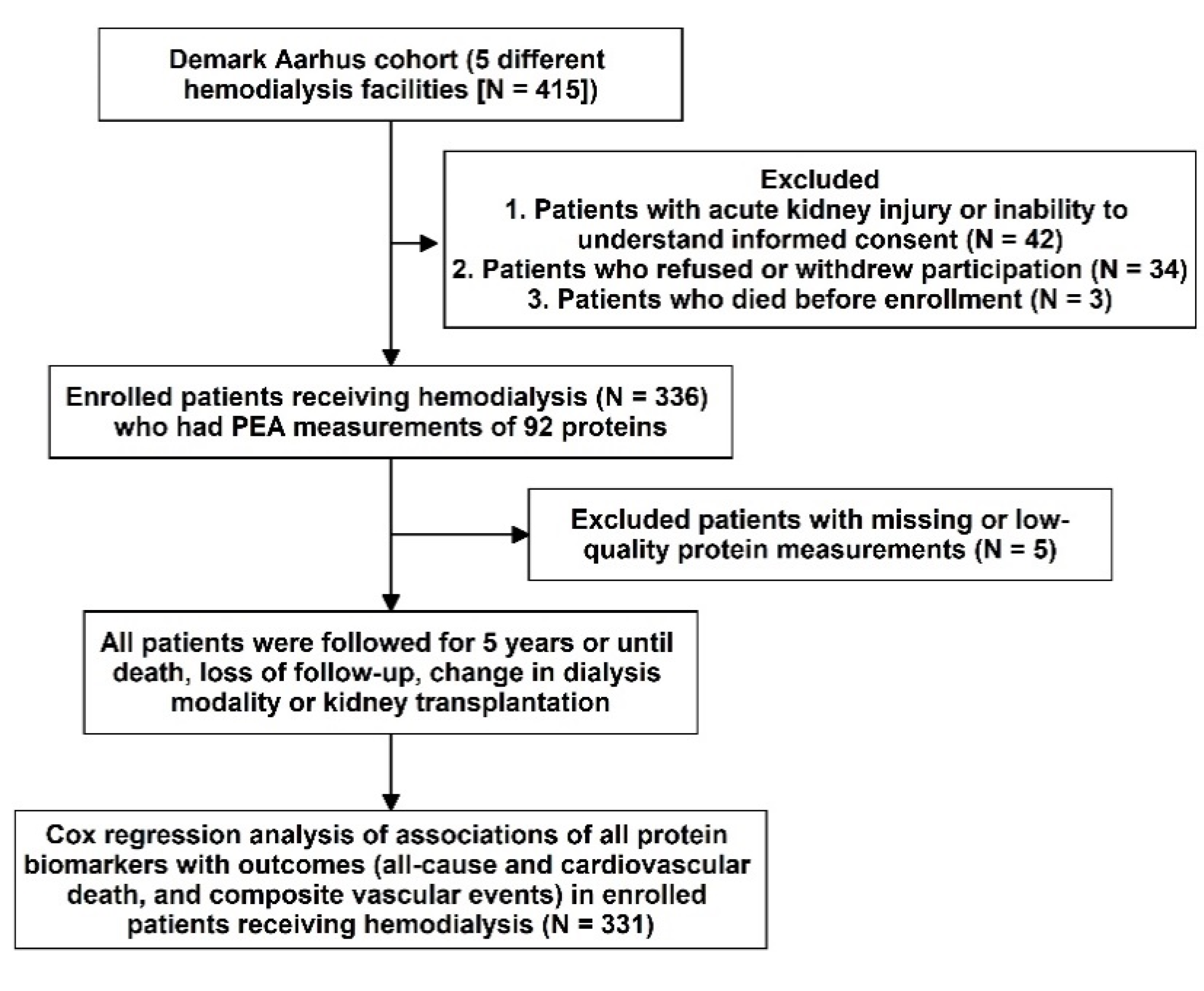
2.1. Subjects, Study Design, and Follow-Up Events
2.2. Clinical Biochemistry and PEA Proteomics Biomarkers Profiling
2.3. Statistical Analyses
3. Results
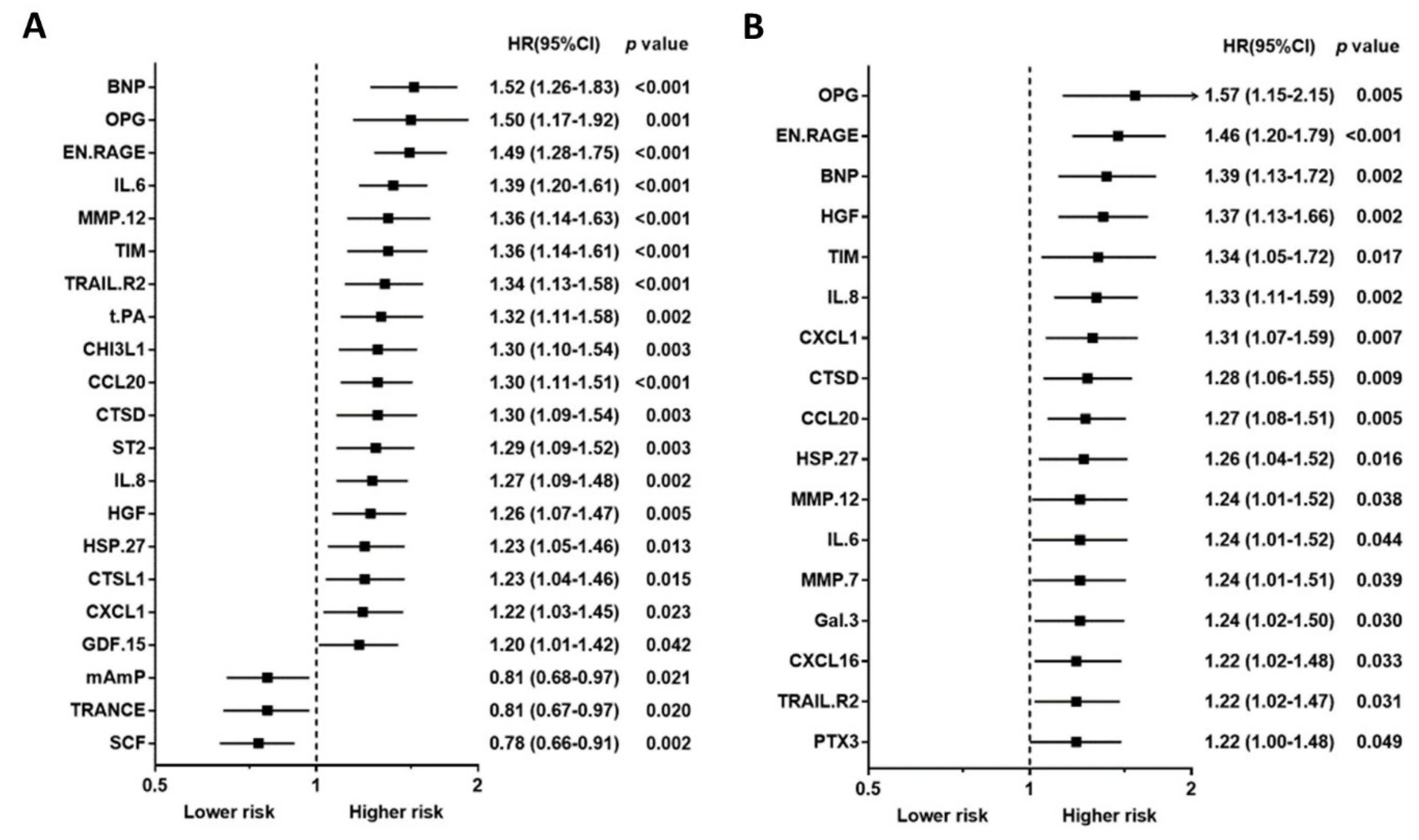
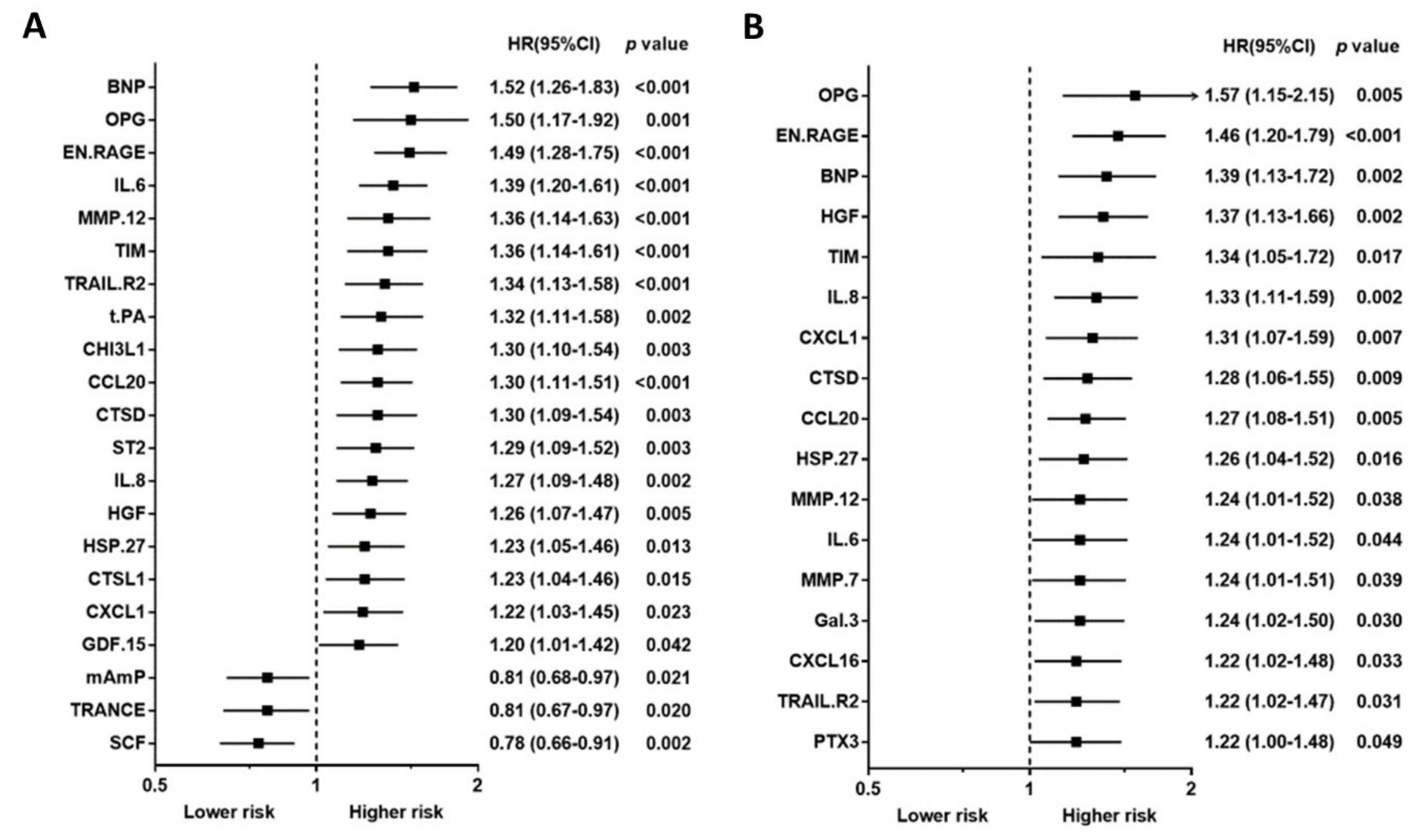
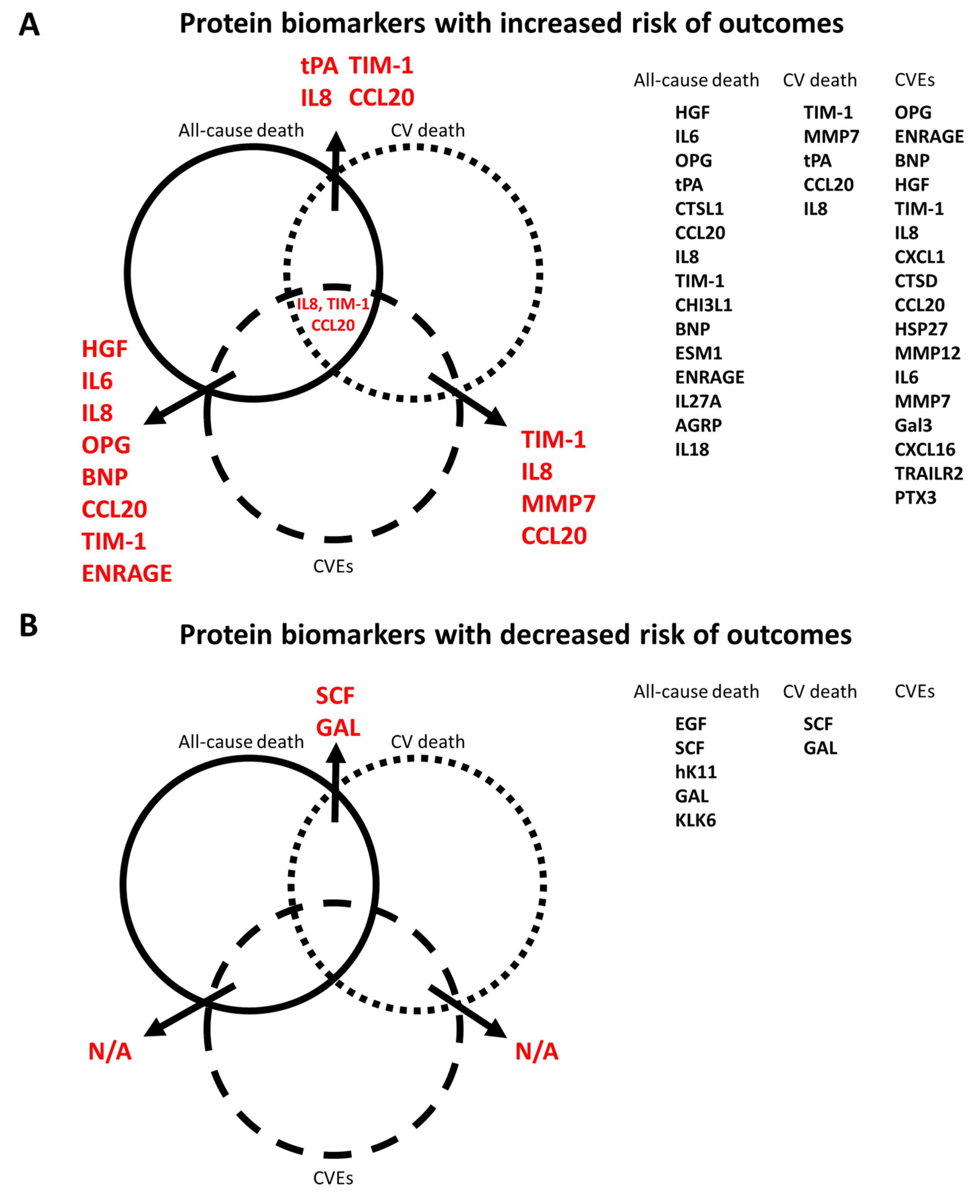
3.1. Associations between Proteins and Outcome Events
3.2. Relationship between Clinical Factors and PEA-Based Proteins
4. Discussion
4.1. Comparison with Other PEA-Based Proteomics Studies in Patients with Kidney Disease
4.2. Comparison with Other Biomarker Studies in Patients with Kidney Disease
4.3. Potential Mechanisms and Clinical Studies of Novel Biomarkers
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Go, A.S.; Chertow, G.M.; Fan, D.; McCulloch, C.E.; Hsu, C.Y. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N. Engl. J. Med. 2004, 351, 1296–1305. [Google Scholar] [CrossRef] [PubMed]
- Cozzolino, M.; Mangano, M.; Stucchi, A.; Ciceri, P.; Conte, F.; Galassi, A. Cardiovascular disease in dialysis patients. Nephrol. Dial. Transplant. 2018, 33, iii28–iii34. [Google Scholar] [CrossRef] [PubMed]
- Vickery, S.; Webb, M.C.; Price, C.P.; John, R.I.; Abbas, N.A.; Lamb, E.J. Prognostic value of cardiac biomarkers for death in a non-dialysis chronic kidney disease population. Nephrol. Dial. Transplant. 2008, 23, 3546–3553. [Google Scholar] [CrossRef] [Green Version]
- Matsushita, K.; Sang, Y.; Ballew, S.H.; Shlipak, M.; Katz, R.; Rosas, S.E.; Peralta, C.A.; Woodward, M.; Kramer, H.J.; Jacobs, D.R.; et al. Subclinical atherosclerosis measures for cardiovascular prediction in CKD. J. Am. Soc. Nephrol. 2015, 26, 439–447. [Google Scholar] [CrossRef] [Green Version]
- de Filippi, C.; Wasserman, S.; Rosanio, S.; Tiblier, E.; Sperger, H.; Tocchi, M.; Christenson, R.; Uretsky, B.; Smiley, M.; Gold, J.; et al. Cardiac troponin T and C-reactive protein for predicting prognosis, coronary atherosclerosis, and cardiomyopathy in patients undergoing long-term hemodialysis. JAMA 2003, 290, 353–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Honda, H.; Qureshi, A.R.; Heimburger, O.; Barany, P.; Wang, K.; Pecoits-Filho, R.; Stenvinkel, P.; Lindholm, B. Serum albumin, C-reactive protein, interleukin 6, and fetuin a as predictors of malnutrition, cardiovascular disease, and mortality in patients with ESRD. Am. J. Kidney Dis. 2006, 47, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Rao, M.; Guo, D.; Perianayagam, M.C.; Tighiouart, H.; Jaber, B.L.; Pereira, B.J.; Balakrishnan, V.S. Plasma interleukin-6 predicts cardiovascular mortality in hemodialysis patients. Am. J. Kidney Dis. 2005, 45, 324–333. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, O.M.; Mannstadt, M.; Isakova, T.; Rauh-Hain, J.A.; Tamez, H.; Shah, A.; Smith, K.; Lee, H.; Thadhani, R.; Juppner, H.; et al. Fibroblast growth factor 23 and mortality among patients undergoing hemodialysis. N. Engl. J. Med. 2008, 359, 584–592. [Google Scholar] [CrossRef] [Green Version]
- Chonchol, M.; Greene, T.; Zhang, Y.; Hoofnagle, A.N.; Cheung, A.K. Low Vitamin D and High Fibroblast Growth Factor 23 Serum Levels Associate with Infectious and Cardiac Deaths in the HEMO Study. J. Am. Soc. Nephrol. 2016, 27, 227–237. [Google Scholar] [CrossRef] [Green Version]
- Zoccali, C.; Mallamaci, F.; Benedetto, F.A.; Tripepi, G.; Parlongo, S.; Cataliotti, A.; Cutrupi, S.; Giacone, G.; Bellanuova, I.; Cottini, E.; et al. Cardiac natriuretic peptides are related to left ventricular mass and function and predict mortality in dialysis patients. J. Am. Soc. Nephrol. 2001, 12, 1508–1515. [Google Scholar] [CrossRef]
- Winkler, K.; Wanner, C.; Drechsler, C.; Lilienthal, J.; Marz, W.; Krane, V.; German, D.; Dialysis Study, I. Change in N-terminal-pro-B-type-natriuretic-peptide and the risk of sudden death, stroke, myocardial infarction, and all-cause mortality in diabetic dialysis patients. Eur. Heart J. 2008, 29, 2092–2099. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dubin, R.F.; Li, Y.; He, J.; Jaar, B.G.; Kallem, R.; Lash, J.P.; Makos, G.; Rosas, S.E.; Soliman, E.Z.; Townsend, R.R.; et al. Predictors of high sensitivity cardiac troponin T in chronic kidney disease patients: A cross-sectional study in the chronic renal insufficiency cohort (CRIC). BMC Nephrol. 2013, 14, 229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michos, E.D.; Wilson, L.M.; Yeh, H.C.; Berger, Z.; Suarez-Cuervo, C.; Stacy, S.R.; Bass, E.B. Prognostic value of cardiac troponin in patients with chronic kidney disease without suspected acute coronary syndrome: A systematic review and meta-analysis. Ann. Intern. Med. 2014, 161, 491–501. [Google Scholar] [CrossRef] [Green Version]
- Lind, L.; Arnlov, J.; Lindahl, B.; Siegbahn, A.; Sundstrom, J.; Ingelsson, E. Use of a proximity extension assay proteomics chip to discover new biomarkers for human atherosclerosis. Atherosclerosis 2015, 242, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Nowak, C.; Carlsson, A.C.; Ostgren, C.J.; Nystrom, F.H.; Alam, M.; Feldreich, T.; Sundstrom, J.; Carrero, J.J.; Leppert, J.; Hedberg, P.; et al. Multiplex proteomics for prediction of major cardiovascular events in type 2 diabetes. Diabetologia 2018, 61, 1748–1757. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feldreich, T.; Nowak, C.; Fall, T.; Carlsson, A.C.; Carrero, J.J.; Ripsweden, J.; Qureshi, A.R.; Heimburger, O.; Barany, P.; Stenvinkel, P.; et al. Circulating proteins as predictors of cardiovascular mortality in end-stage renal disease. J. Nephrol. 2019, 32, 111–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Assarsson, E.; Lundberg, M.; Holmquist, G.; Bjorkesten, J.; Thorsen, S.B.; Ekman, D.; Eriksson, A.; Rennel Dickens, E.; Ohlsson, S.; Edfeldt, G.; et al. Homogenous 96-plex PEA immunoassay exhibiting high sensitivity, specificity, and excellent scalability. PLoS ONE 2014, 9, e95192. [Google Scholar] [CrossRef] [Green Version]
- Feldreich, T.; Nowak, C.; Carlsson, A.C.; Ostgren, C.J.; Nystrom, F.H.; Sundstrom, J.; Carrero-Roig, J.J.; Leppert, J.; Hedberg, P.; Giedraitis, V.; et al. The association between plasma proteomics and incident cardiovascular disease identifies MMP-12 as a promising cardiovascular risk marker in patients with chronic kidney disease. Atherosclerosis 2020, 307, 11–15. [Google Scholar] [CrossRef]
- Panichi, V.; Rizza, G.M.; Paoletti, S.; Bigazzi, R.; Aloisi, M.; Barsotti, G.; Rindi, P.; Donati, G.; Antonelli, A.; Panicucci, E.; et al. Chronic inflammation and mortality in haemodialysis: Effect of different renal replacement therapies. Results from the RISCAVID study. Nephrol. Dial. Transplant. 2008, 23, 2337–2343. [Google Scholar] [CrossRef] [Green Version]
- Panichi, V.; Taccola, D.; Rizza, G.M.; Consani, C.; Ghiadoni, L.; Filippi, C.; Cristofani, R.; Panicucci, E.; Migliori, M.; Sidoti, A.; et al. Interleukin-8 is a powerful prognostic predictor of all-cause and cardiovascular mortality in dialytic patients. Nephron Clin. Pract. 2006, 102, c51–c58. [Google Scholar] [CrossRef]
- Shiotsu, Y.; Mori, Y.; Nishimura, M.; Sakoda, C.; Tokoro, T.; Hatta, T.; Maki, N.; Iida, K.; Iwamoto, N.; Ono, T.; et al. Plasma S100A12 level is associated with cardiovascular disease in hemodialysis patients. Clin. J. Am. Soc. Nephrol. 2011, 6, 718–723. [Google Scholar] [CrossRef] [PubMed]
- Morena, M.; Terrier, N.; Jaussent, I.; Leray-Moragues, H.; Chalabi, L.; Rivory, J.P.; Maurice, F.; Delcourt, C.; Cristol, J.P.; Canaud, B.; et al. Plasma osteoprotegerin is associated with mortality in hemodialysis patients. J. Am. Soc. Nephrol. 2006, 17, 262–270. [Google Scholar] [CrossRef] [PubMed]
- Speer, G.; Fekete, B.C.; El Hadj Othmane, T.; Szabo, T.; Egresits, J.; Fodor, E.; Kiss, I.; Logan, A.G.; Nemcsik, J.; Szabo, A.; et al. Serum osteoprotegerin level, carotid-femoral pulse wave velocity and cardiovascular survival in haemodialysis patients. Nephrol. Dial. Transplant. 2008, 23, 3256–3262. [Google Scholar] [CrossRef] [PubMed]
- Winther, S.; Christensen, J.H.; Flyvbjerg, A.; Schmidt, E.B.; Jorgensen, K.A.; Skou-Jorgensen, H.; Svensson, M. Osteoprotegerin and mortality in hemodialysis patients with cardiovascular disease. Clin. Nephrol. 2013, 80, 161–167. [Google Scholar] [CrossRef] [Green Version]
- Schoppet, M.; Al-Fakhri, N.; Franke, F.E.; Katz, N.; Barth, P.J.; Maisch, B.; Preissner, K.T.; Hofbauer, L.C. Localization of osteoprotegerin, tumor necrosis factor-related apoptosis-inducing ligand, and receptor activator of nuclear factor-kappaB ligand in Monckeberg’s sclerosis and atherosclerosis. J. Clin. Endocrinol. Metab. 2004, 89, 4104–4112. [Google Scholar] [CrossRef] [Green Version]
- Libetta, C.; Esposito, P.; Martinelli, C.; Grosjean, F.; Gregorini, M.; Rampino, T.; Dal Canton, A. Hepatocyte growth factor (HGF) and hemodialysis: Physiopathology and clinical implications. Clin. Exp. Nephrol. 2016, 20, 371–378. [Google Scholar] [CrossRef]
- Lonn, J.; Starkhammar Johansson, C.; Kalvegren, H.; Brudin, L.; Skoglund, C.; Garvin, P.; Sarndahl, E.; Ravald, N.; Richter, A.; Bengtsson, T.; et al. Hepatocyte growth factor in patients with coronary artery disease and its relation to periodontal condition. Results Immunol. 2011, 2, 7–12. [Google Scholar] [CrossRef] [Green Version]
- Rajpathak, S.N.; Wang, T.; Wassertheil-Smoller, S.; Strickler, H.D.; Kaplan, R.C.; McGinn, A.P.; Wildman, R.P.; Rosenbaum, D.; Rohan, T.E.; Scherer, P.E.; et al. Hepatocyte growth factor and the risk of ischemic stroke developing among postmenopausal women: Results from the Women’s Health Initiative. Stroke 2010, 41, 857–862. [Google Scholar] [CrossRef] [Green Version]
- Malatino, L.S.; Cataliotti, A.; Benedetto, F.A.; Stancanelli, B.; Bellanuova, I.; Belluardo, P.; Bonaiuto, L.; Tripepi, G.; Mallamaci, F.; Castellino, P.; et al. Hepatocyte growth factor and left ventricular geometry in end-stage renal disease. Hypertension 2003, 41, 88–92. [Google Scholar] [CrossRef] [Green Version]
- Anan, F.; Shimomura, T.; Imagawa, M.; Masaki, T.; Nawata, T.; Takahashi, N.; Yonemochi, H.; Eshima, N.; Saikawa, T.; Yoshimatsu, H. Predictors for silent cerebral infarction in patients with chronic renal failure undergoing hemodialysis. Metabolism 2007, 56, 593–598. [Google Scholar] [CrossRef]
- Rampino, T.; Libetta, C.; De Simone, W.; Ranghino, A.; Soccio, G.; Gregorini, M.; Guallini, P.; Tamagnone, L.; Dal Canton, A. Hemodialysis stimulates hepatocyte growth factor release. Kidney Int. 1998, 53, 1382–1388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lebherz-Eichinger, D.; Klaus, D.A.; Reiter, T.; Horl, W.H.; Haas, M.; Ankersmit, H.J.; Krenn, C.G.; Roth, G.A. Increased chemokine excretion in patients suffering from chronic kidney disease. Transl. Res. 2014, 164, 433–443.e2. [Google Scholar] [CrossRef] [PubMed]
- Safa, A.; Rashidinejad, H.R.; Khalili, M.; Dabiri, S.; Nemati, M.; Mohammadi, M.M.; Jafarzadeh, A. Higher circulating levels of chemokines CXCL10, CCL20 and CCL22 in patients with ischemic heart disease. Cytokine 2016, 83, 147–157. [Google Scholar] [CrossRef] [PubMed]
- Calvayrac, O.; Rodriguez-Calvo, R.; Alonso, J.; Orbe, J.; Martin-Ventura, J.L.; Guadall, A.; Gentile, M.; Juan-Babot, O.; Egido, J.; Beloqui, O.; et al. CCL20 is increased in hypercholesterolemic subjects and is upregulated by LDL in vascular smooth muscle cells: Role of NF-kappaB. Arterioscler. Thromb. Vasc. Biol. 2011, 31, 2733–2741. [Google Scholar] [CrossRef] [Green Version]
- Elnabawi, Y.A.; Garshick, M.S.; Tawil, M.; Barrett, T.J.; Fisher, E.A.; Lo Sicco, K.; Neimann, A.L.; Scher, J.U.; Krueger, J.; Berger, J.S. CCL20 in psoriasis: A potential biomarker of disease severity, inflammation, and impaired vascular health. J. Am. Acad. Dermatol. 2021, 84, 913–920. [Google Scholar] [CrossRef]
- Tesmer, L.A.; Lundy, S.K.; Sarkar, S.; Fox, D.A. Th17 cells in human disease. Immunol. Rev. 2008, 223, 87–113. [Google Scholar] [CrossRef]
- Taleb, S.; Tedgui, A.; Mallat, Z. IL-17 and Th17 cells in atherosclerosis: Subtle and contextual roles. Arterioscler. Thromb. Vasc. Biol. 2015, 35, 258–264. [Google Scholar] [CrossRef] [Green Version]
- Wan, W.; Lim, J.K.; Lionakis, M.S.; Rivollier, A.; McDermott, D.H.; Kelsall, B.L.; Farber, J.M.; Murphy, P.M. Genetic deletion of chemokine receptor Ccr6 decreases atherogenesis in ApoE-deficient mice. Circ. Res. 2011, 109, 374–381. [Google Scholar] [CrossRef] [Green Version]
- de Bono, D. Significance of raised plasma concentrations of tissue-type plasminogen activator and plasminogen activator inhibitor in patients at risk from ischaemic heart disease. Br. Heart J. 1994, 71, 504–507. [Google Scholar] [CrossRef] [Green Version]
- Lowe, G.D.; Danesh, J.; Lewington, S.; Walker, M.; Lennon, L.; Thomson, A.; Rumley, A.; Whincup, P.H. Tissue plasminogen activator antigen and coronary heart disease. Prospective study and meta-analysis. Eur. Heart J. 2004, 25, 252–259. [Google Scholar] [CrossRef]
- Segarra, A.; Chacon, P.; Martinez-Eyarre, C.; Argelaguer, X.; Vila, J.; Ruiz, P.; Fort, J.; Bartolome, J.; Camps, J.; Moliner, E.; et al. Circulating levels of plasminogen activator inhibitor type-1, tissue plasminogen activator, and thrombomodulin in hemodialysis patients: Biochemical correlations and role as independent predictors of coronary artery stenosis. J. Am. Soc. Nephrol. 2001, 12, 1255–1263. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Cabiale, Z.; Parrado, C.; Narvaez, M.; Millon, C.; Puigcerver, A.; Fuxe, K.; Narvaez, J.A. Neurochemical modulation of central cardiovascular control: The integrative role of galanin. Exp. Suppl. 2010, 102, 113–131. [Google Scholar] [CrossRef] [PubMed]
- Palkeeva, M.; Studneva, I.; Molokoedov, A.; Serebryakova, L.; Veselova, O.; Ovchinnikov, M.; Sidorova, M.; Pisarenko, O. Galanin/GalR1-3 system: A promising therapeutic target for myocardial ischemia/reperfusion injury. Biomed. Pharmacother. 2019, 109, 1556–1562. [Google Scholar] [CrossRef] [PubMed]
- Martinelli, I.; Timotin, A.; Moreno-Corchado, P.; Marsal, D.; Kramar, S.; Loy, H.; Joffre, C.; Boal, F.; Tronchere, H.; Kunduzova, O. Galanin promotes autophagy and alleviates apoptosis in the hypertrophied heart through FoxO1 pathway. Redox Biol. 2021, 40, 101866. [Google Scholar] [CrossRef] [PubMed]
- Bjorkbacka, H.; Yao Mattisson, I.; Wigren, M.; Melander, O.; Fredrikson, G.N.; Bengtsson, E.; Goncalves, I.; Almgren, P.; Lagerstedt, J.O.; Orho-Melander, M.; et al. Plasma stem cell factor levels are associated with risk of cardiovascular disease and death. J. Intern. Med. 2017, 282, 508–521. [Google Scholar] [CrossRef]
- Wallentin, L.; Eriksson, N.; Olszowka, M.; Grammer, T.B.; Hagstrom, E.; Held, C.; Kleber, M.E.; Koenig, W.; Marz, W.; Stewart, R.A.H.; et al. Plasma proteins associated with cardiovascular death in patients with chronic coronary heart disease: A retrospective study. PLoS Med. 2021, 18, e1003513. [Google Scholar] [CrossRef]
- Lennartsson, J.; Ronnstrand, L. Stem cell factor receptor/c-Kit: From basic science to clinical implications. Physiol. Rev. 2012, 92, 1619–1649. [Google Scholar] [CrossRef] [Green Version]
- Lutz, M.; Rosenberg, M.; Kiessling, F.; Eckstein, V.; Heger, T.; Krebs, J.; Ho, A.D.; Katus, H.A.; Frey, N. Local injection of stem cell factor (SCF) improves myocardial homing of systemically delivered c-kit + bone marrow-derived stem cells. Cardiovasc. Res. 2008, 77, 143–150. [Google Scholar] [CrossRef] [Green Version]
- Block, G.A.; Klassen, P.S.; Lazarus, J.M.; Ofsthun, N.; Lowrie, E.G.; Chertow, G.M. Mineral metabolism, mortality, and morbidity in maintenance hemodialysis. J. Am. Soc. Nephrol. 2004, 15, 2208–2218. [Google Scholar] [CrossRef] [Green Version]
- Floege, J.; Kim, J.; Ireland, E.; Chazot, C.; Drueke, T.; de Francisco, A.; Kronenberg, F.; Marcelli, D.; Passlick-Deetjen, J.; Schernthaner, G.; et al. Serum iPTH, calcium and phosphate, and the risk of mortality in a European haemodialysis population. Nephrol. Dial. Transplant. 2011, 26, 1948–1955. [Google Scholar] [CrossRef] [Green Version]
- Sobsey, C.A.; Ibrahim, S.; Richard, V.R.; Gaspar, V.; Mitsa, G.; Lacasse, V.; Zahedi, R.P.; Batist, G.; Borchers, C.H. Targeted and untargeted proteomics approaches in biomarker development. Proteomics 2020, 20, e1900029. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All-Cause Death | Cardiovascular Death | Composite Vascular Event | No Event | Significance | |
|---|---|---|---|---|---|
| Patients (n) | 167 | 62 | 140 | 122 | |
| Age, years | 68.9 ± 12.5 | 68.1 ± 11.9 | 67.5 ± 12.0 | 58.9 ± 16.3 | ***, ###, ††† |
| Males, n (%) | 115 (69%) | 47 (76%) | 96 (69%) | 74 (61%) | NS, NS, NS |
| Smoking | NS, NS, † | ||||
| Current smoker, n (%) | 39 (23%) | 18 (29%) | 43 (31%) | 33 (27%) | |
| Never smoker, n (%) | 55 (33%) | 17 (27%) | 33 (24%) | 48 (39%) | |
| Former smoker, n (%) | 73 (44%) | 27 (44%) | 64 (46%) | 41 (34%) | |
| Cause of end-stage kidney disease | *, ###, ††† | ||||
| Hypertension, n (%) | 24 (14%) | 13 (21%) | 22 (16%) | 15 (12%) | |
| Diabetes mellitus, n (%) | 36 (22%) | 18 (29%) | 39 (28%) | 14 (12%) | |
| Glomerulonephritis, n (%) | 16 (10%) | 3 (5%) | 9 (6%) | 21 (17%) | |
| Cystic disease, n (%) | 10 (6%) | 2 (3%) | 9 (6%) | 17 (14%) | |
| Others, n (%) | 81 (49%) | 26 (42%) | 61 (44%) | 55 (45%) | |
| Hemodialysis vintage, days | 1533 ± 1592 | 1366 ± 1427 | 1468 ± 1505 | 1337 ± 1714 | NS, NS, NS |
| Renal replacement therapy vintage, days | 2041 ± 2385 | 1706 ± 1934 | 2032 ± 2473 | 2344 ± 2955 | NS, NS, NS |
| Previous kidney transplant, n (%) | 8 (5%) | 3 (5%) | 7 (5%) | 11 (9%) | NS, NS, NS |
| Residual renal function of daily urine amount | NS, NS, NS | ||||
| <50 mL/day, n (%) | 63 (38%) | 23 (37%) | 53 (38%) | 41 (34%) | |
| 50–500 mL/day, n (%) | 28 (17%) | 9 (15%) | 24 (17%) | 28 (23%) | |
| >500 mL/day, n (%) | 76 (46%) | 30 (48%) | 63 (45%) | 53 (43%) | |
| Dialysis modality | NS, NS, NS | ||||
| Hemodialysis, n (%) | 145 (87%) | 55 (89%) | 116 (83%) | 106 (87%) | |
| Hemodiafiltration, n (%) | 22 (13%) | 7 (11%) | 24 (17%) | 16 (13%) | |
| Dialysis treatment time per week, hours | 11.1 ± 2.6 | 11.4 ± 2.5 | 11.3 ± 2.7 | 11.2 ± 2.6 | NS, NS, NS |
| Time interval between subjects’ inclusion and prior dialysis session, hours | 59.7 ± 23.0 | 57.5 ± 23.8 | 58.9 ± 22.0 | 57.5 ± 20.7 | NS, NS, NS |
| Comorbidities | |||||
| Diabetes mellitus, n (%) | 53 (32%) | 24 (39%) | 53 (38%) | 22 (18%) | *, ##, ††† |
| Type 1 diabetes mellitus, n (%) | 10 (6%) | 6 (10%) | 12 (9%) | 9 (7%) | |
| Type 2 diabetes mellitus, n (%) | 43 (26%) | 18 (29%) | 41 (29%) | 13 (11%) | |
| Previous myocardial infarction, n (%) | 40 (24%) | 17 (27%) | 30 (21%) | 16 (13%) | *, #, NS |
| Previous unstable angina, n (%) | 54 (32%) | 23 (37%) | 44 (31%) | 20 (16%) | **, ##, †† |
| Previous cerebrovascular disease, n (%) | 38 (23%) | 19 (31%) | 42 (30%) | 16 (13%) | NS, ##, †† |
| Previous peripheral artery disease, n (%) | 43 (26%) | 20 (32%) | 43 (31%) | 15 (12%) | **, ##, ††† |
| Statin treatment, n (%) | 61 (37%) | 22 (36%) | 58 (41%) | 37 (30%) | NS, NS, NS |
| Clinical laboratory data | |||||
| Albumin, (g/L) | 38.17 ± 4.09 | 38.56 ± 4.19 | 38.29 ± 4.02 | 40.11 ± 3.13 | ***, #, ††† |
| C-reactive protein (mg/L) | 7.56 (16.20) | 7.02 (12.72) | 7.08 (14.52) | 4.46 (7.68) | ***, ##, ††† |
| Phosphate (mmol/L) | 1.55 ± 0.33 | 1.59 ± 0.32 | 1.61 ± 0.40 | 1.64 ± 0.41 | NS, NS, NS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, P.-H.; Glerup, R.I.; Svensson, M.H.S.; Eriksson, N.; Christensen, J.H.; Laval, P.d.; Soveri, I.; Westerlund, M.; Linde, T.; Ljunggren, Ö.; et al. Novel Biomarkers Detected by Proteomics Predict Death and Cardiovascular Events in Hemodialysis Patients. Biomedicines 2022, 10, 740. https://doi.org/10.3390/biomedicines10040740
Wu P-H, Glerup RI, Svensson MHS, Eriksson N, Christensen JH, Laval Pd, Soveri I, Westerlund M, Linde T, Ljunggren Ö, et al. Novel Biomarkers Detected by Proteomics Predict Death and Cardiovascular Events in Hemodialysis Patients. Biomedicines. 2022; 10(4):740. https://doi.org/10.3390/biomedicines10040740
Chicago/Turabian StyleWu, Ping-Hsun, Rie Io Glerup, My Hanna Sofia Svensson, Niclas Eriksson, Jeppe Hagstrup Christensen, Philip de Laval, Inga Soveri, Magnus Westerlund, Torbjörn Linde, Östen Ljunggren, and et al. 2022. "Novel Biomarkers Detected by Proteomics Predict Death and Cardiovascular Events in Hemodialysis Patients" Biomedicines 10, no. 4: 740. https://doi.org/10.3390/biomedicines10040740
APA StyleWu, P.-H., Glerup, R. I., Svensson, M. H. S., Eriksson, N., Christensen, J. H., Laval, P. d., Soveri, I., Westerlund, M., Linde, T., Ljunggren, Ö., & Fellström, B. (2022). Novel Biomarkers Detected by Proteomics Predict Death and Cardiovascular Events in Hemodialysis Patients. Biomedicines, 10(4), 740. https://doi.org/10.3390/biomedicines10040740