
Cardiovascular Disease-Associated MicroRNA Dysregulation during the First Trimester of Gestation in Women with Chronic Hypertension and Normotensive Women Subsequently Developing Gestational Hypertension or Preeclampsia with or without Fetal Growth Restriction



Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients Cohort
2.2. First Trimester Risk Analysis
2.3. Processing of Samples
2.4. Statistical Analysis
3. Results
3.1. Cardiovascular Disease-Associated MicroRNAs Are Dysregulated in Early Stages of Gestation in Women with Chronic Hypertension and Normotensive Women Subsequently Developing GH or PE wo/w FGR
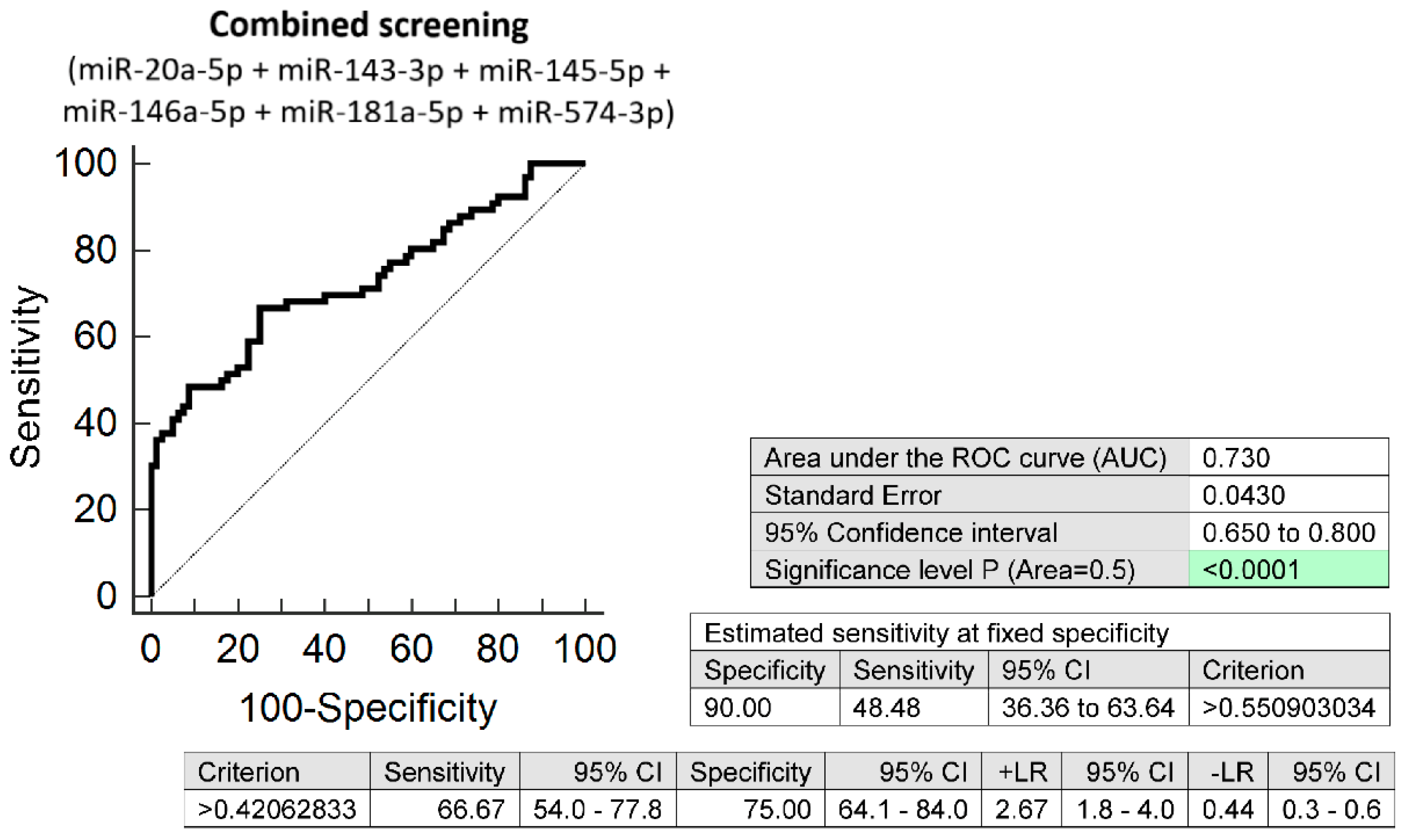
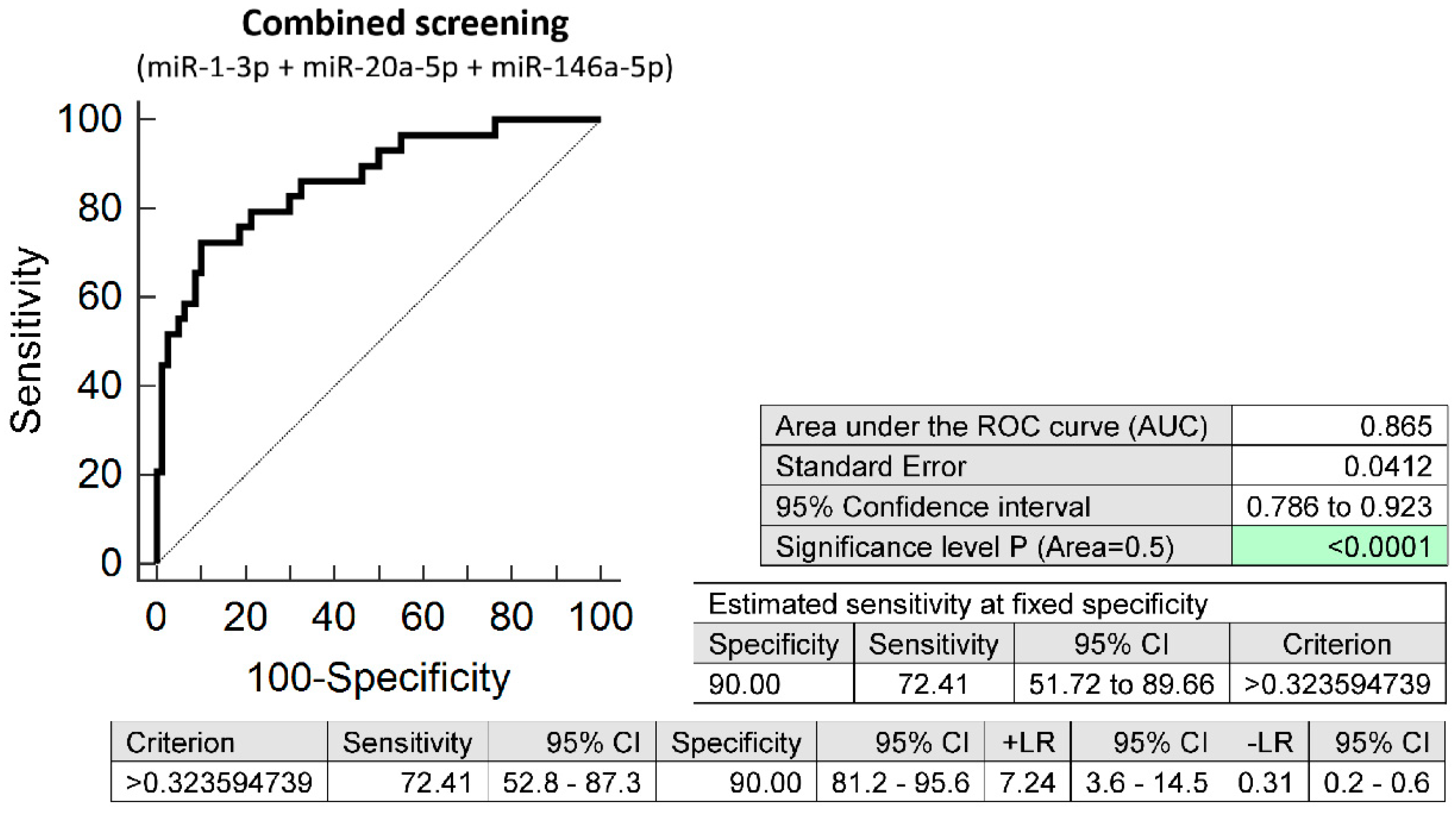
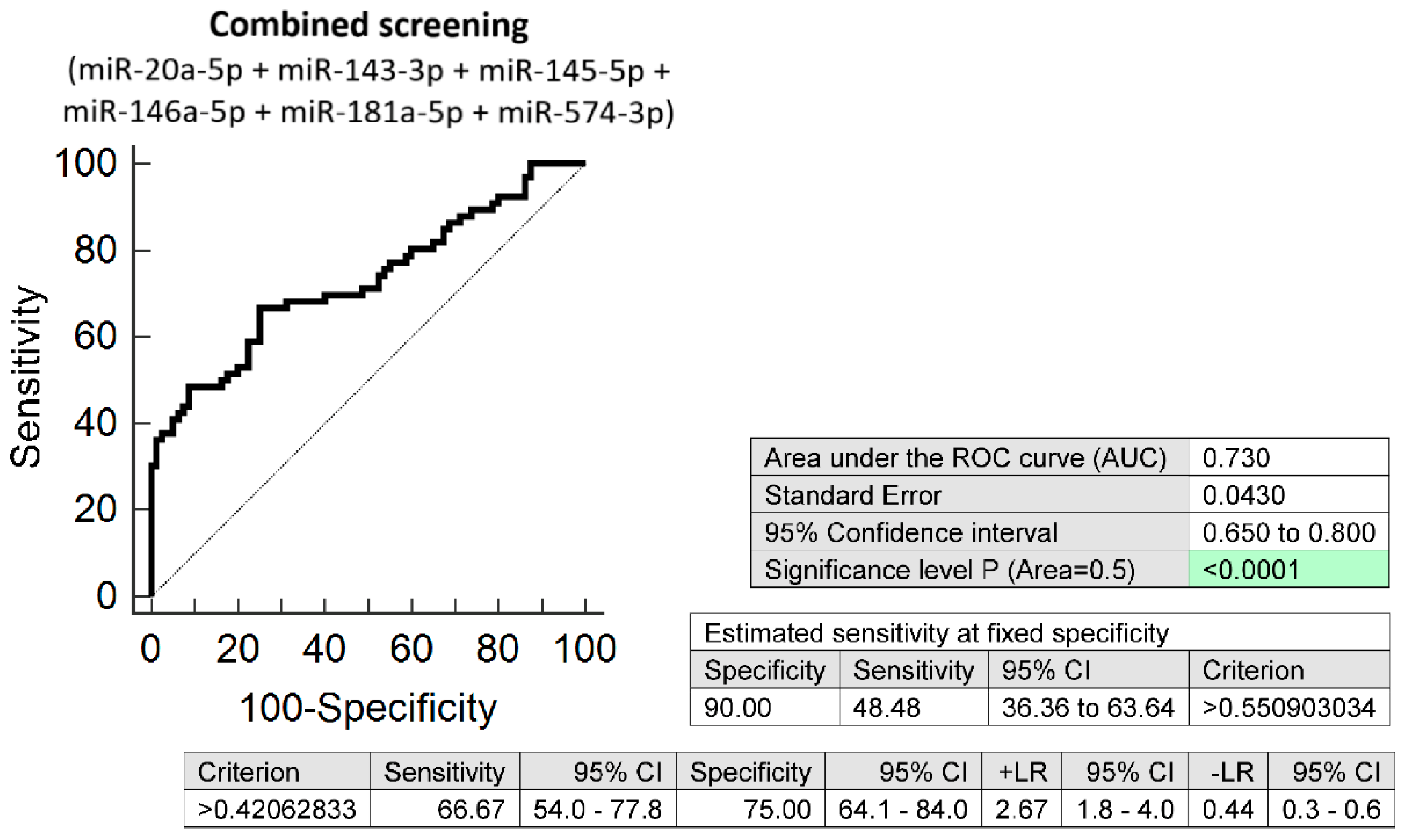
3.2. The High Accuracy of First Trimester Combined MicroRNA Screening to Differentiate between Women with Chronic Hypertension and Normotensive Women with Normal Course of Gestation
3.3. The Very Good Accuracy of First Trimester Combined MicroRNA Screening to Differentiate between Normotensive Women with Subsequent Development of PE wo/w FGR and Normal Course of Gestation
3.4. Correlation between First Trimester MicroRNA Screening and the Routine First Trimester Predictive Markers for PE and/or FGR
4. Discussion
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- ACOG Committee Opinion No. 743. Low-Dose Aspirin Use During Pregnancy. Obstet. Gynecol. 2018, 132, e44–e52.
- National Institute for Health and Care Excellence. Hypertension in Pregnancy: Diagnosis and Management. Available online: www.nice.org.uk/guidance/ng133 (accessed on 4 October 2021).
- Tong, S.; Mol, B.W.; Walker, S.P. Preventing preeclampsia with aspirin: Does dose or timing matter? Am. J. Obstet. Gynecol. 2017, 216, 95–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peres, G.M.; Mariana, M.; Cairrão, E. Pre-Eclampsia and Eclampsia: An Update on the Pharmacological Treatment Applied in Portugal. J. Cardiovasc. Dev. Dis. 2018, 5, 3. [Google Scholar] [CrossRef] [Green Version]
- Meher, S.; Duley, L.; Hunter, K.; Askie, L. Antiplatelet therapy before or after 16 weeks’ gestation for preventing preeclampsia: An individual participant data meta-analysis. Am. J. Obstet. Gynecol. 2017, 216, 121–128.e2. [Google Scholar] [CrossRef] [PubMed]
- National Collaborating Centre for Women’s and Children’s Health. Hypertension in Pregnancy: The Management of Hypertensive Disorders during Pregnancy—NICE Clinical Guideline; Royal College of Obstetricans and Gynaecologist: London, UK, 2010. [Google Scholar]
- Giannakou, K. Prediction of pre-eclampsia. Obstet. Med. 2021, 14, 220–224. [Google Scholar] [CrossRef] [PubMed]
- O’Gorman, N.; Wright, D.; Poon, L.C.; Rolnik, D.L.; Syngelaki, A.; de Alvarado, M.; Carbone, I.F.; Dutemeyer, V.; Fiolna, M.; Frick, A.; et al. Multicenter screening for pre-eclampsia by maternal factors and biomarkers at 11–13 weeks’ gestation: Comparison with NICE guidelines and ACOG recommendations. Ultrasound Obstet. Gynecol. 2017, 49, 756–760. [Google Scholar] [CrossRef]
- O’Gorman, N.; Wright, D.; Syngelaki, A.; Akolekar, R.; Wright, A.; Poon, L.C.; Nicolaides, K.H. Competing risks model in screening for preeclampsia by maternal factors and biomarkers at 11–13 weeks gestation. Am. J. Obstet. Gynecol. 2016, 214, 103.e1–103.e12. [Google Scholar] [CrossRef] [Green Version]
- The Fetal Medicine Foundation. Stratification of Pregnancy Management 11–13 Weeks’ Gestation. Available online: www.courses.fetalmedicine.com/fmf/show/861?locale=en (accessed on 4 October 2021).
- Mazer Zumaeta, A.; Wright, A.; Syngelaki, A.; Maritsa, V.A.; Da Silva, A.B.; Nicolaides, K.H. Screening for pre-eclampsia at 11–13 weeks’ gestation: Use of pregnancy-associated plasma protein-A, placental growth factor or both. Ultrasound Obstet. Gynecol. 2020, 56, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Tan, M.Y.; Syngelaki, A.; Poon, L.C.; Rolnik, D.L.; O’Gorman, N.; Delgado, J.L.; Akolekar, R.; Konstantinidou, L.; Tsavdaridou, M.; Galeva, S.; et al. Screening for pre-eclampsia by maternal factors and biomarkers at 11–13 weeks’ gestation. Ultrasound Obstet. Gynecol. 2018, 52, 186–195. [Google Scholar] [CrossRef] [Green Version]
- Rolnik, D.L.; Wright, D.; Poon, L.C.; O’Gorman, N.; Syngelaki, A.; de Paco Matallana, C.; Akolekar, R.; Cicero, S.; Janga, D.; Singh, M.; et al. Aspirin versus Placebo in Pregnancies at High Risk for Preterm Preeclampsia. N. Engl. J. Med. 2017, 377, 613–622. [Google Scholar] [CrossRef]
- Wright, D.; Poon, L.C.; Rolnik, D.L.; Syngelaki, A.; Delgado, J.L.; Vojtassakova, D.; de Alvarado, M.; Kapeti, E.; Rehal, A.; Pazos, A.; et al. Aspirin for Evidence-Based Preeclampsia Prevention trial: Influence of compliance on beneficial effect of aspirin in prevention of preterm preeclampsia. Am. J. Obstet. Gynecol. 2017, 217, 685.e1–685.e5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.; Xie, Z.; Wang, X.; Xiao, Q.; Lu, X.; Lu, S.; Shi, Y.; Lv, S. A risk model of prenatal screening markers in first trimester for predicting hypertensive disorders of pregnancy. EPMA J. 2020, 11, 343–353. [Google Scholar] [CrossRef] [PubMed]
- Hromadnikova, I.; Kotlabova, K.; Krofta, L. Association Analysis in Young and Middle-Aged Mothers-Relation between Expression of Cardiovascular Disease Associated MicroRNAs and Abnormal Clinical Findings. J. Pers. Med. 2021, 11, 39. [Google Scholar] [CrossRef] [PubMed]
- Hromadnikova, I.; Kotlabova, K.; Dvorakova, L.; Krofta, L. Postpartum profiling of microRNAs involved in pathogenesis of cardiovascular/cerebrovascular diseases in women exposed to pregnancy-related complications. Int. J. Cardiol. 2019, 291, 158–167. [Google Scholar] [CrossRef]
- Winger, E.E.; Reed, J.L.; Ji, X. First trimester PBMC microRNA predicts adverse pregnancy outcome. Am. J. Reprod. Immunol. 2014, 72, 515–526. [Google Scholar] [CrossRef] [PubMed]
- Winger, E.E.; Reed, J.L.; Ji, X. First-trimester maternal cell microRNA is a superior pregnancy marker to immunological testing for predicting adverse pregnancy outcome. J. Reprod. Immunol. 2015, 110, 22–35. [Google Scholar] [CrossRef]
- Winger, E.E.; Reed, J.L.; Ji, X.; Nicolaides, K. Peripheral blood cell microRNA quantification during the first trimester predicts preeclampsia: Proof of concept. PLoS ONE 2018, 13, e0190654. [Google Scholar]
- Livak, K.J.; Schmittgen, T.D. Analysis of relative gene expression data using real-time quantitative PCR and the 2(-Delta Delta C(T)) Method. Methods 2001, 25, 402–408. [Google Scholar] [CrossRef]
- Vandesompele, J.; De Preter, K.; Pattyn, F.; Poppe, B.; Van Roy, N.; De Paepe, A.; Speleman, F. Accurate normalization of real-time quantitative RT-PCR data by geometric averaging of multiple internal control genes. Genome Biol. 2002, 3, research0034.1. [Google Scholar] [CrossRef] [Green Version]
- Benjamini, Y.; Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Stat. Soc. Ser. B 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Haynes, W. Benjamini–Hochberg Method. In Encyclopedia of Systems Biology; Dubitzky, W., Wolkenhauer, O., Cho, K.H., Yokota, H., Eds.; Springer: New York, NY, USA, 2013. [Google Scholar]
- Ura, B.; Feriotto, G.; Monasta, L.; Bilel, S.; Zweyer, M.; Celeghini, C. Potential role of circulating microRNAs as early markers of preeclampsia. Taiwan J. Obstet. Gynecol. 2014, 53, 232–234. [Google Scholar] [CrossRef] [Green Version]
- Jiang, L.; Long, A.; Tan, L.; Hong, M.; Wu, J.; Cai, L.; Li, Q. Elevated microRNA-520g in pre-eclampsia inhibits migration and invasion of trophoblasts. Placenta 2017, 51, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Huang, G.; Zhang, Y.; Yang, H.; Long, Y.; Liang, Q.; Zheng, Z. MiR-942 decreased before 20 weeks gestation in women with preeclampsia and was associated with the pathophysiology of preeclampsia in vitro. Clin. Exp. Hypertens. 2017, 39, 108–113. [Google Scholar] [CrossRef] [PubMed]
- Hromadnikova, I.; Kotlabova, K.; Ivankova, K.; Krofta, L. First trimester screening of circulating C19MC microRNAs and the evaluation of their potential to predict the onset of preeclampsia and IUGR. PLoS ONE 2017, 12, e0171756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Timofeeva, A.V.; Gusar, V.A.; Kan, N.E.; Prozorovskaya, K.N.; Karapetyan, A.O.; Bayev, O.R.; Chagovets, V.V.; Kliver, S.F.; Iakovishina, D.Y.; Frankevich, V.E.; et al. Identification of potential early biomarkers of preeclampsia. Placenta 2018, 61, 61–71. [Google Scholar] [CrossRef] [PubMed]
- Yoffe, L.; Gilam, A.; Yaron, O.; Polsky, A.; Farberov, L.; Syngelaki, A.; Nicolaides, K.; Hod, M.; Shomron, N. Early Detection of Preeclampsia Using Circulating Small non-coding RNA. Sci. Rep. 2018, 8, 3401. [Google Scholar] [CrossRef]
- Mavreli, D.; Lykoudi, A.; Lambrou, G.; Papaioannou, G.; Vrachnis, N.; Kalantaridou, S.; Papantoniou, N.; Kolialexi, A. Deep Sequencing Identified Dysregulated Circulating MicroRNAs in Late Onset Preeclampsia. In Vivo 2020, 34, 2317–2324. [Google Scholar] [CrossRef]
- Licini, C.; Avellini, C.; Picchiassi, E.; Mensà, E.; Fantone, S.; Ramini, D.; Tersigni, C.; Tossetta, G.; Castellucci, C.; Tarquini, F.; et al. Pre-eclampsia predictive ability of maternal miR-125b: A clinical and experimental study. Transl. Res. 2021, 228, 13–27. [Google Scholar] [CrossRef]
- Hromadnikova, I.; Dvorakova, L.; Kotlabova, K.; Krofta, L. The Prediction of Gestational Hypertension, Preeclampsia and Fetal Growth Restriction via the First Trimester Screening of Plasma Exosomal C19MC microRNAs. Int. J. Mol. Sci. 2019, 20, 2972. [Google Scholar] [CrossRef]
- Kontaraki, J.E.; Marketou, M.E.; Zacharis, E.A.; Parthenakis, F.I.; Vardas, P.E. Differential expression of vascular smooth muscle-modulating microRNAs in human peripheral blood mononuclear cells: Novel targets in essential hypertension. J. Hum. Hypertens. 2014, 28, 510–516. [Google Scholar] [CrossRef]
- Kontaraki, J.E.; Marketou, M.E.; Parthenakis, F.I.; Maragkoudakis, S.; Zacharis, E.A.; Petousis, S.; Kochiadakis, G.E.; Vardas, P.E. Hypertrophic and antihypertrophic microRNA levels in peripheral blood mononuclear cells and their relationship to left ventricular hypertrophy in patients with essential hypertension. J. Am. Soc. Hypertens. 2015, 9, 802–810. [Google Scholar] [CrossRef] [PubMed]
- Dluzen, D.F.; Noren Hooten, N.; Zhang, Y.; Kim, Y.; Glover, F.E.; Tajuddin, S.M.; Jacob, K.D.; Zonderman, A.B.; Evans, M.K. Racial differences in microRNA and gene expression in hypertensive women. Sci. Rep. 2016, 6, 35815. [Google Scholar] [CrossRef] [PubMed]
- Kriegel, A.J.; Baker, M.A.; Liu, Y.; Liu, P.; Cowley, A.W., Jr.; Liang, M. Endogenous microRNAs in human microvascular endothelial cells regulate mRNAs encoded by hypertension-related genes. Hypertension 2015, 66, 793–799. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hijmans, J.G.; Diehl, K.J.; Bammert, T.D.; Kavlich, P.J.; Lincenberg, G.M.; Greiner, J.J.; Stauffer, B.L.; DeSouza, C.A. Association between hypertension and circulating vascular-related microRNAs. J. Hum. Hypertens. 2018, 32, 440–447. [Google Scholar] [CrossRef]
- Roganović, J. Downregulation of microRNA-146a in diabetes, obesity and hypertension may contribute to severe COVID-19. Med. Hypotheses 2021, 146, 110448. [Google Scholar] [CrossRef]
- Klimczak, D.; Kuch, M.; Pilecki, T.; Żochowska, D.; Wirkowska, A.; Pączek, L. Plasma microRNA-155-5p is increased among patients with chronic kidney disease and nocturnal hypertension. J. Am. Soc. Hypertens. 2017, 11, 831–841.e4. [Google Scholar] [CrossRef]
- Hu, Y.; Li, Q.; Zhang, L.; Zhong, L.; Gu, M.; He, B.; Qu, Q.; Lao, Y.; Gu, K.; Zheng, B.; et al. Serum miR-195-5p Exhibits Clinical Significance in the Diagnosis of Essential Hypertension with Type 2 Diabetes Mellitus by Targeting DRD1. Clinics (Sao Paulo) 2021, 76, e2502. [Google Scholar] [CrossRef]
- Salem, M.A.A.; Ammar, I.M.M. First-Trimester Uterine Artery Pulsatility Index and Maternal Serum PAPP-A and PlGF in Prediction of Preeclampsia in Primigravida. J. Obstet. Gynaecol. India 2018, 68, 192–196. [Google Scholar] [CrossRef]
- Park, H.J.; Shim, S.S.; Cha, D.H. Combined Screening for Early Detection of Pre-Eclampsia. Int. J. Mol. Sci. 2015, 16, 17952–17974. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Normal Pregnancies (n = 80) | CHH (n = 29) | GH (n = 83) | PE wo/w FGR (n = 66) | p-Value 1 | p-Value 2 | p-Value 3 | |
|---|---|---|---|---|---|---|---|
| Maternal characteristics | |||||||
| Maternal age (years) | 32.0 (29.0–34.25) | 34.0 (32.0–39.0) | 34.0 (30.0–36.5) | 31.0 (28.25–36.0) | 0.032 | 0.445 | 1.000 |
| Advanced maternal age (≥35 years old) | 20 (25%) | 14 (48.28%) | 34 (40.96%) | 22 (33.33%) | 0.020 | 0.030 | 0.268 |
| Caucasian ethnic group | 80 (100%) | 29 (100%) | 83 (100%) | 66 (100%) | - | - | - |
| Prepregnancy BMI (kg/m2) | 21.28 (20.54–23.55) | 25.56 (21.67–31.31) | 24.8 (22.65–30.76) | 23.98 (21.37–28.17) | <0.001 | <0.001 | <0.001 |
| Diabetes mellitus (T1DM, T2DM) | 0 (0%) | 2 (6.90%) | 6 (7.23%) | 4 (6.06%) | - | - | - |
| Autoimmune diseases (SLE/APS/RA) | 0 (0%) | 1 (3.45%) | 3 (3.61%) | 2 (3.03%) | - | - | - |
| Parity | |||||||
| Nulliparous | 40 (50.0%) | 15 (51.72%) | 55 (66.26%) | 52 (78.79%) | 1.000 | 0.035 | <0.001 |
| Parous with no previous PE | 40 (50.0%) | 11 (37.93%) | 26 (31.33%) | 8 (12.12%) | - | - | - |
| Parous with previous PE | 0 (0%) | 3 (10.34%) | 2 (2.41%) | 6 (9.09%) | - | - | - |
| ART (IVF/ICSI/other) | 2 (2.5%) | 7 (24.14%) | 15 (18.07%) | 17 (25.76%) | <0.001 | 0.001 | <0.001 |
| Smoking during pregnancy | 2 (2.5%) | 2 (6.90%) | 3 (3.61%) | 3 (4.55%) | 0.281 | 0.680 | 0.499 |
| Pregnancy details (First trimester of gestation) | |||||||
| Gestational age at sampling (weeks) | 10.29 (10.14–10.57) | 10.57 (10.14–10.71) | 10.29 (10.0–10.71) | 10.43 (10.03–11.0) | 0.468 | 1.000 | 1.000 |
| MAP (mmHg) | 88.75 (84.54–95.04) | 100.83 (96.5–112.75) | 99.67 (95.62–104.83) | 96.0 (91.0–100.08) | <0.001 | <0.001 | <0.001 |
| MAP (MoM) | 1.05 (1.01–1.10) | 1.16 (1.11–1.24) | 1.14 (1.11–1.19) | 1.13 (1.07–1.17) | <0.001 | <0.001 | 0.017 |
| Mean UtA-PI | 1.39 (1.11–1.68) | 1.38 (1.15–1.78) | 1.54 (1.24–1.95) | 1.55 (1.13–1.94) | 0.195 | 1.000 | 1.000 |
| Mean UtA-PI (MoM) | 0.90 (0.73–1.10) | 0.92 (0.70–1.16) | 1.02 (0.82–1.27) | 1.0 (0.71–1.26) | 0.111 | 1.000 | 1.000 |
| PIGF serum levels (pg/mL) | 27.1 (21.6–34.3) | 24.6 (19.45–36.37) | 25.0 (20.8–29.6) | 22.8 (17.8–29.2) | 1.000 | 0.442 | 0.040 |
| PIGF serum levels (MoM) | 1.04 (0.85–1.31) | 0.94 (0.82–1.19) | 1.06 (0.87–1.23) | 0.96 (0.7–1.20) | 1.000 | 1.000 | 0.294 |
| PAPP-A serum levels (IU/L) | 1.49 (1.09–2.36) | 1.19 (0.60–2.66) | 1.10 (0.65–1.95) | 1.28 (0.73–2.05) | 0.575 | 0.016 | 0.214 |
| PAPP-A serum levels (MoM) | 1.17 (0.82–1.54) | 0.92 (0.66–1.35) | 1.07 (0.70–1.54) | 0.93 (0.61–1.38) | 0.917 | 1.000 | 0.118 |
| Screen-positive for PE and/or FGR by FMF algorithm | 0 (0%) | 16 (55.17%) | 29 (34.94%) | 22 (33.33%) | - | - | - |
| Aspirin intake during pregnancy | 0 (0%) | 15 (51.72%) | 26 (31.33%) | 22 (33.33%) | - | - | - |
| Pregnancy details (At delivery) | |||||||
| Systolic blood pressure (mmHg) | 122 (115–131) | 136.5 (126.75–146.25) | 147.5 (137.75–154.75) | 155 (145–165.75) | <0.001 | <0.001 | <0.001 |
| Diastolic blood pressure (mmHg) | 76.5 (70.75–81.25) | 85.0 (80–95.25) | 94.5 (89–99) | 100 (92.25–103) | <0.001 | <0.001 | <0.001 |
| Gestational age at delivery (weeks) | 40.07 (39.10–40.60) | 38.78 (37.82–40.03) | 39.14 (38.36–40.07) | 37.07 (34.75–38.25) | 0.002 | 0.005 | <0.001 |
| Delivery at gestational age < 37 weeks | 0 (0%) | 4 (13.79%) | 10 (12.05%) | 33 (50.0%) | - | - | - |
| BMI (kg/m2) | 26.66 (25.11–28.81) | 29.81 (26.27–33.10) | 30.67 (28.07–35.66) | 29.83 (26.64–33.96) | 0.007 | <0.001 | <0.001 |
| Weight gain during pregnancy (kg) | 14 (12–17.75) | 10 (7.75–12.725) | 14 (10–18) | 14 (10–19) | 0.001 | 1.000 | 1.000 |
| Fetal birth weight (grams) | 3470 (3290–3690) | 3240 (2965–3475) | 3370 (3110–3785) | 2645 (2065–3222.5) | 0.996 | 0.076 | <0.001 |
| Fetal sex | |||||||
| Boy | 40 (50.0%) | 16 (55.17%) | 47 (56.63%) | 29 (43.94%) | 0.633 | 0.396 | 0.465 |
| Girl | 40 (50.0%) | 13 (44.83%) | 36 (43.37%) | 37 (56.06%) | |||
| Mode of delivery | |||||||
| Vaginal | 69 (86.25%) | 14 (48.28%) | 48 (57.83%) | 18 (27.27%) | <0.001 | <0.001 | <0.001 |
| CS | 11 (13.75%) | 15 (51.72%) | 35 (42.17%) | 48 (72.73%) | |||
| K | i | Alpha = 0.05 | Alpha = 0.01 | Alpha = 0.001 |
|---|---|---|---|---|
| 6 | 0.05 | 0.01 | 0.001 | |
| 1 | 0.008 | 0.002 | 0.000 | |
| 2 | 0.017 | 0.003 | 0.000 | |
| 3 | 0.025 | 0.005 | 0.001 | |
| 4 | 0.033 | 0.007 | 0.001 | |
| 5 | 0.042 | 0.008 | 0.001 | |
| 6 | 0.050 | 0.010 | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hromadnikova, I.; Kotlabova, K.; Krofta, L. Cardiovascular Disease-Associated MicroRNA Dysregulation during the First Trimester of Gestation in Women with Chronic Hypertension and Normotensive Women Subsequently Developing Gestational Hypertension or Preeclampsia with or without Fetal Growth Restriction. Biomedicines 2022, 10, 256. https://doi.org/10.3390/biomedicines10020256
Hromadnikova I, Kotlabova K, Krofta L. Cardiovascular Disease-Associated MicroRNA Dysregulation during the First Trimester of Gestation in Women with Chronic Hypertension and Normotensive Women Subsequently Developing Gestational Hypertension or Preeclampsia with or without Fetal Growth Restriction. Biomedicines. 2022; 10(2):256. https://doi.org/10.3390/biomedicines10020256
Chicago/Turabian StyleHromadnikova, Ilona, Katerina Kotlabova, and Ladislav Krofta. 2022. "Cardiovascular Disease-Associated MicroRNA Dysregulation during the First Trimester of Gestation in Women with Chronic Hypertension and Normotensive Women Subsequently Developing Gestational Hypertension or Preeclampsia with or without Fetal Growth Restriction" Biomedicines 10, no. 2: 256. https://doi.org/10.3390/biomedicines10020256
APA StyleHromadnikova, I., Kotlabova, K., & Krofta, L. (2022). Cardiovascular Disease-Associated MicroRNA Dysregulation during the First Trimester of Gestation in Women with Chronic Hypertension and Normotensive Women Subsequently Developing Gestational Hypertension or Preeclampsia with or without Fetal Growth Restriction. Biomedicines, 10(2), 256. https://doi.org/10.3390/biomedicines10020256