
The Characteristics and Obstetric Outcomes of Type II Vasa Previa: Systematic Review and Meta-Analysis
 ,
,  ,
,
Abstract
1. General Overview
2. Systematic Literature Search
2.1. Approach for Systematic Review
2.2. Article Retrieval and Search Strategy
2.3. Study Selection
2.4. Data Extraction
2.5. Analysis of Outcome Measures and Assessment of Bias Risk
2.6. Meta-Analysis Plan
2.7. Statistical Analysis
3. Results
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk of Bias of Included Studies
3.4. Number of Studies: Primary Outcome
3.4.1. Primary Outcome: The Incidence of Type II Vasa Previa
3.4.2. Co-Primary Outcome: Number of Studies Comparing Type I and II Vasa Previa
3.4.3. Co-Primary Outcome: Characteristics and Obstetric Outcomes Comparing Type I and II Vasa Previa
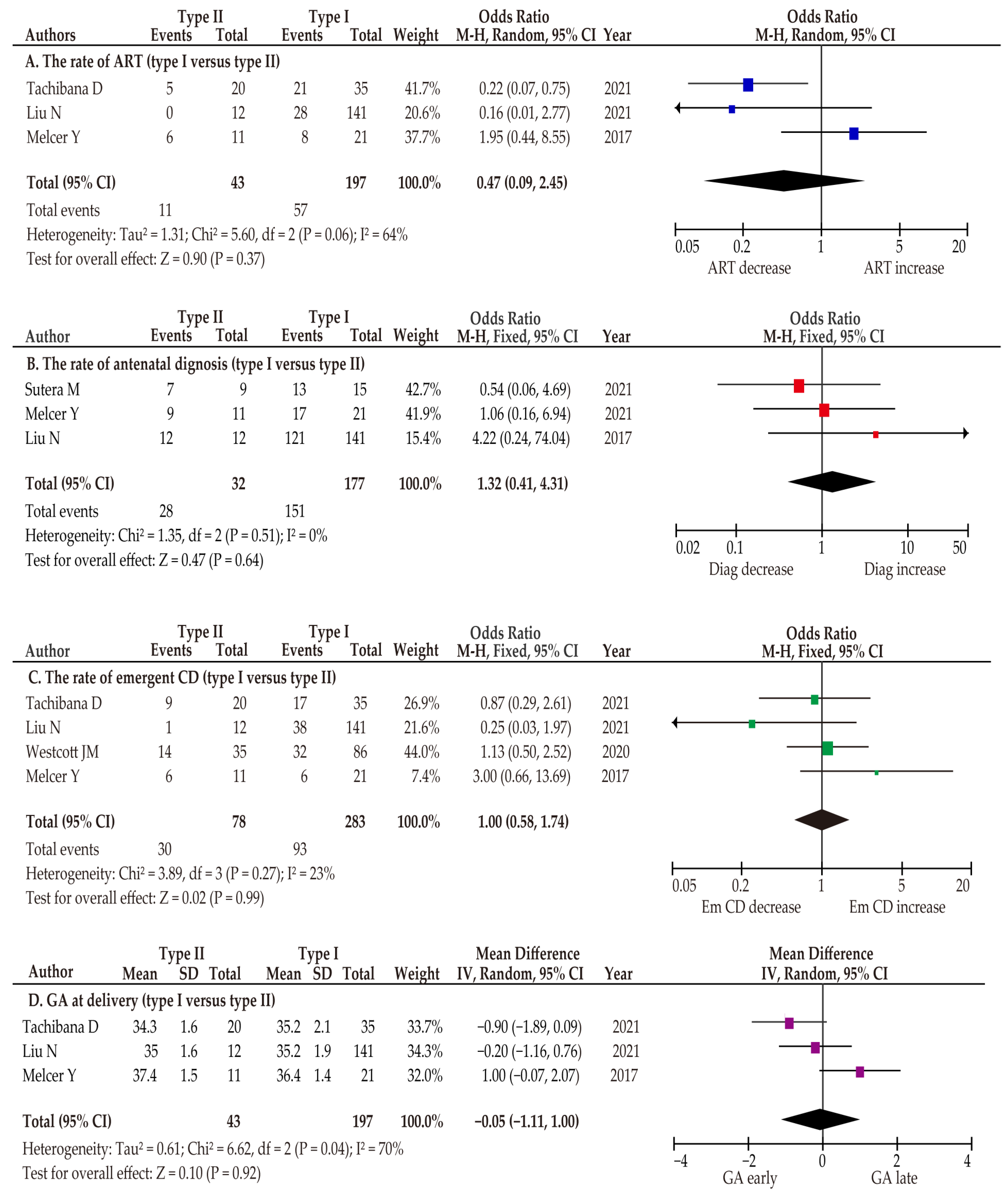
3.4.4. Co-Primary Outcome: The Rate of ART
3.4.5. Co-Primary Outcome: The Rate of Antenatal Diagnosis
3.4.6. Co-Primary Outcome: The Rate of Emergent Cesarean Delivery
3.4.7. Co-Primary Outcome: Gestational Age at Delivery
3.4.8. Co-Primary Outcome: Maternal and Neonatal Outcomes
3.5. Number of Studies: Secondary Outcome
3.5.1. Secondary Outcome: The Rate of Vasa Previa in Abnormal Placenta
3.5.2. Secondary Outcome: The Association between ART and Abnormal Placenta
3.6. Number of Studies: Sensitivity Analysis
The Rate of Abnormal Placenta According to the Type of ART
4. Discussion
4.1. Principal Findings
4.2. Strengths and Limitations
4.3. Comparison with Existing Literature
4.3.1. The Incidence of Type II Vasa Previa
4.3.2. The Different Characteristics between Type I and Type II Vasa Previa
4.3.3. The Association between ART and Abnormal Placenta
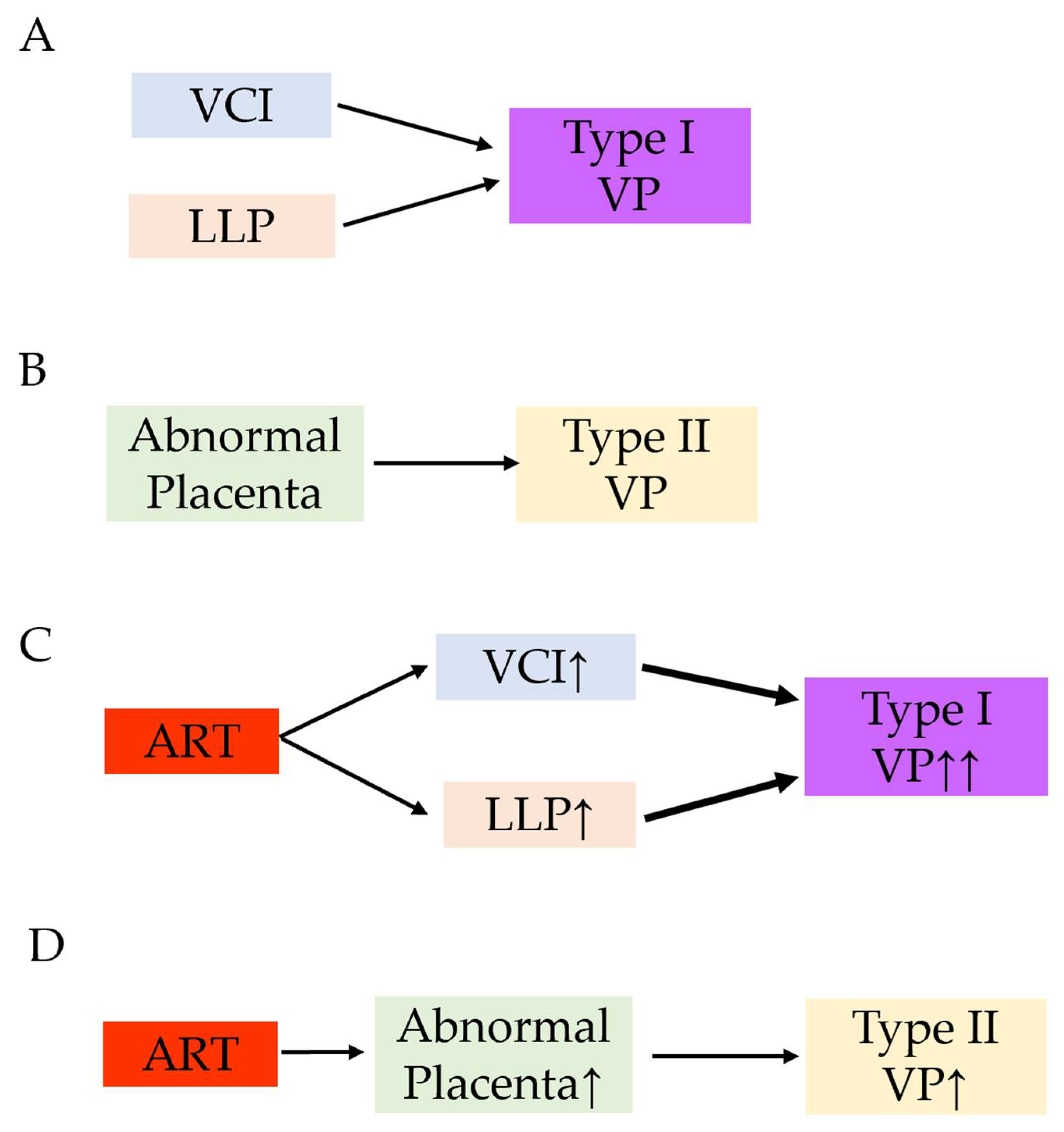
4.3.4. The Mechanism of Developing Type II Vasa Previa
4.3.5. The Association between ART and Vasa Previa
5. Conclusions and Implications
5.1. Implications for Practice
5.2. Implications for Clinical Research
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Transparency
References
- Mitchell, S.J.; Ngo, G.; Maurel, K.A.; Hasegawa, J.; Arakaki, T.; Melcer, Y.; Maymon, R.; Vendittelli, F.; Shamshirsaz, A.A.; Erfani, H.; et al. Timing of birth and adverse pregnancy outcomes in cases of prenatally diagnosed vasa previa: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2022, 227, 173–181.e24. [Google Scholar] [CrossRef] [PubMed]
- Pavalagantharajah, S.; Villani, L.A.; D’Souza, R. Vasa previa and associated risk factors: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. MFM 2020, 2, 100117. [Google Scholar] [CrossRef] [PubMed]
- Melcer, Y.; Maymon, R.; Jauniaux, E. Vasa previa: Prenatal diagnosis and management. Curr. Opin. Obstet. Gynecol. 2018, 30, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Jauniaux, E.; Melcer, Y.; Maymon, R. Prenatal diagnosis and management of vasa previa in twin pregnancies: A case series and systematic review. Am. J. Obstet. Gynecol. 2017, 216, 568–575. [Google Scholar] [CrossRef] [PubMed]
- Matsuzaki, S.; Endo, M.; Kimura, T. Vasa previa with an intact amniotic membrane. Am. J. Obstet. Gynecol. 2017, 216, 616.e1–616.e2. [Google Scholar] [CrossRef]
- Society of Maternal-Fetal (SMFM) Publications Committee; Sinkey, R.G.; Odibo, A.O.; Dashe, J.S. #37: Diagnosis and management of vasa previa. Am. J. Obstet. Gynecol. 2015, 213, 615–619. [Google Scholar] [CrossRef]
- Swank, M.L.; Garite, T.J.; Maurel, K.; Das, A.; Perlow, J.H.; Combs, C.A.; Fishman, S.; Vanderhoeven, J.; Nageotte, M.; Bush, M.; et al. Vasa previa: Diagnosis and management. Am. J. Obstet. Gynecol. 2016, 215, 223.e1–223.e6. [Google Scholar] [CrossRef]
- Klahr, R.; Fox, N.S.; Zafman, K.; Hill, M.B.; Connolly, C.T.; Rebarber, A. Frequency of spontaneous resolution of vasa previa with advancing gestational age. Am. J. Obstet. Gynecol. 2019, 221, 646.e1–646.e7. [Google Scholar] [CrossRef]
- Sinkey, R.G.; Odibo, A.O. Vasa previa screening strategies: Decision and cost-effectiveness analysis. Ultrasound Obs. Gynecol 2018, 52, 522–529. [Google Scholar] [CrossRef]
- Green, A.; Chiu, S.; Manor, E.; Smith, L.; Oyelese, Y. The association of gestational age at delivery with neonatal outcomes in prenatally diagnosed vasa previa. J. Matern. Fetal Neonatal Med. 2022, 35, 10162–10167. [Google Scholar] [CrossRef]
- Gagnon, R. No. 231-Guidelines for the Management of Vasa Previa. J. Obstet. Gynaecol. Can. JOGC J. D’obstetrique Et Gynecol. Du Can. JOGC 2017, 39, e415–e421. [Google Scholar] [CrossRef] [PubMed]
- Tsakiridis, I.; Mamopoulos, A.; Athanasiadis, A.; Dagklis, T. Diagnosis and Management of Vasa Previa: A Comparison of 4 National Guidelines. Obs. Gynecol. Surv. 2019, 74, 436–442. [Google Scholar] [CrossRef]
- Jauniaux, E.; Alfirevic, Z.; Bhide, A.G.; Burton, G.J.; Collins, S.L.; Silver, R. Vasa Praevia: Diagnosis and Management: Green-top Guideline No. 27b. Bjog 2019, 126, e49–e61. [Google Scholar] [CrossRef]
- Catanzarite, V.; Maida, C.; Thomas, W.; Mendoza, A.; Stanco, L.; Piacquadio, K.M. Prenatal sonographic diagnosis of vasa previa: Ultrasound findings and obstetric outcome in ten cases. Ultrasound Obs. Gynecol. 2001, 18, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Ruiter, L.; Kok, N.; Limpens, J.; Derks, J.B.; de Graaf, I.M.; Mol, B.W.; Pajkrt, E. Systematic review of accuracy of ultrasound in the diagnosis of vasa previa. Ultrasound Obs. Gynecol 2015, 45, 516–522. [Google Scholar] [CrossRef] [PubMed]
- Rebarber, A.; Dolin, C.; Fox, N.S.; Klauser, C.K.; Saltzman, D.H.; Roman, A.S. Natural history of vasa previa across gestation using a screening protocol. J. Ultrasound Med. 2014, 33, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Bręborowicz, G.H.; Markwitz, W.; Szpera-Goździewicz, A.; Dera-Szymanowska, A.; Ropacka-Lesiak, M.; Szymański, P.; Kubiaczyk-Paluch, B. Prenatal diagnosis of vasa previa. J. Matern. Fetal Neonatal Med. 2015, 28, 1806–1808. [Google Scholar] [CrossRef]
- Baumfeld, Y.; Gutvirtz, G.; Shoham, I.; Sheiner, E. Fetal heart rate patterns of pregnancies with vasa previa and velamentous cord insertion. Arch. Gynecol. Obstet. 2016, 293, 361–367. [Google Scholar] [CrossRef]
- Ibirogba, E.R.; Shazly, S.A.; Chmait, R.H.; Ruano, R. Is there a role for fetoscopic laser ablation therapy in Type-2 vasa previa? Ultrasound Obs. Gynecol. 2019, 54, 696. [Google Scholar] [CrossRef]
- Siargkas, A.; Tsakiridis, I.; Pachi, C.; Mamopoulos, A.; Athanasiadis, A.; Dagklis, T. Impact of velamentous cord insertion on perinatal outcomes: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. MFM 2022, 5, 100812. [Google Scholar] [CrossRef]
- Zhang, W.; Geris, S.; Al-Emara, N.; Ramadan, G.; Sotiriadis, A.; Akolekar, R. Perinatal outcome of pregnancies with prenatal diagnosis of vasa previa: Systematic review and meta-analysis. Ultrasound Obs. Gynecol. 2021, 57, 710–719. [Google Scholar] [CrossRef] [PubMed]
- Ruiter, L.; Kok, N.; Limpens, J.; Derks, J.B.; de Graaf, I.M.; Mol, B.; Pajkrt, E. Incidence of and risk indicators for vasa praevia: A systematic review. BJOG 2016, 123, 1278–1287. [Google Scholar] [CrossRef] [PubMed]
- Kamijo, K.; Miyamoto, T.; Ando, H.; Tanaka, Y.; Kikuchi, N.; Shinagawa, M.; Yamada, S.; Asaka, R.; Fuseya, C.; Ohira, S.; et al. Clinical characteristics of a novel “Type 3” vasa previa: Case series at a single center. J. Matern. Fetal Neonatal Med. 2021, 35, 7730–7736. [Google Scholar] [CrossRef] [PubMed]
- Schachter, M.; Tovbin, Y.; Arieli, S.; Friedler, S.; Ron-El, R.; Sherman, D. In vitro fertilization is a risk factor for vasa previa. Fertil. Steril. 2002, 78, 642–643. [Google Scholar] [CrossRef]
- Pirtea, L.C.; Grigoraş, D.; Sas, I.; Ilie, A.C.; Stana, L.G.; Motoc, A.G.; Jianu, A.M.; Mazilu, O. In vitro fertilization represents a risk factor for vasa praevia. Rom. J. Morphol. Embryol. Rev. Roum. Morphol. Embryol. 2016, 57, 627–632. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Moher, D. Updating guidance for reporting systematic reviews: Development of the PRISMA 2020 statement. J. Clin. Epidemiol. 2021, 134, 103–112. [Google Scholar] [CrossRef]
- Matsuzaki, S.; Lee, M.; Nagase, Y.; Jitsumori, M.; Matsuzaki, S.; Maeda, M.; Takiuchi, T.; Kakigano, A.; Mimura, K.; Ueda, Y.; et al. A systematic review and meta-analysis of obstetric and maternal outcomes after prior uterine artery embolization. Sci. Rep. 2021, 11, 16914. [Google Scholar] [CrossRef]
- Matsuzaki, S.; Endo, M.; Ueda, Y.; Mimura, K.; Kakigano, A.; Egawa-Takata, T.; Kumasawa, K.; Yoshino, K.; Kimura, T. A case of acute Sheehan’s syndrome and literature review: A rare but life-threatening complication of postpartum hemorrhage. BMC Pregnancy Childbirth 2017, 17, 188. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernan, M.A.; Reeves, B.C.; Savovic, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Danna, S.M.; Graham, E.; Burns, R.J.; Deschenes, S.S.; Schmitz, N. Association between Depressive Symptoms and Cognitive Function in Persons with Diabetes Mellitus: A Systematic Review. PLoS ONE 2016, 11, e0160809. [Google Scholar] [CrossRef]
- ROBINS-I Detailed Guidance. 2016. Available online: https://www.riskofbias.info/welcome/home/current-version-of-robins-i/robins-i-detailed-guidance-2016 (accessed on 30 September 2022).
- Matsuzaki, S.; Nagase, Y.; Ueda, Y.; Lee, M.; Matsuzaki, S.; Maeda, M.; Takiuchi, T.; Kakigano, A.; Mimura, K.; Endo, M.; et al. The association of endometriosis with placenta previa and postpartum hemorrhage: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. MFM 2021, 3, 100417. [Google Scholar] [CrossRef] [PubMed]
- Chapter 10: Analysing Data and Undertaking Meta-Analyses. In Cochrane Handbook for Systematic Reviews of Interventions, Version 6.1 ed; Cochrane: London, UK, 2020; Available online: https://training.cochrane.org/handbook/current/chapter-10 (accessed on 30 September 2022).
- Volodarsky-Perel, A.; Ton Nu, T.N.; Buckett, W.; Machado-Gedeon, A.; Cui, Y.; Shaul, J.; Dahan, M.H. Effect of embryo stage at transfer on placental histopathology features in singleton live births resulting from fresh embryo transfers. Fertil. Steril. 2021, 115, 673–682. [Google Scholar] [CrossRef] [PubMed]
- Sacha, C.R.; Harris, A.L.; James, K.; Basnet, K.; Freret, T.S.; Yeh, J.; Kaimal, A.; Souter, I.; Roberts, D.J. Placental pathology in live births conceived with in vitro fertilization after fresh and frozen embryo transfer. Am. J. Obstet. Gynecol. 2020, 222, 360.e1–360.e16. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, S.; Igarashi, M.; Inde, Y.; Miyake, H. Abnormally shaped placentae in twin pregnancy. Arch. Gynecol. Obstet. 2010, 281, 65–69. [Google Scholar] [CrossRef]
- Suzuki, S.; Igarashi, M. Clinical significance of pregnancies with succenturiate lobes of placenta. Arch. Gynecol. Obstet. 2008, 277, 299–301. [Google Scholar] [CrossRef] [PubMed]
- Degirmenci, Y.; Steetskamp, J.; Macchiella, D.; Hasenburg, A.; Hasenburg, A. Vasa previa: A rare obstetric complication-A case series and a literature review. Clin. Case Rep. 2022, 10, e05608. [Google Scholar] [CrossRef] [PubMed]
- Tachibana, D.; Misugi, T.; Pooh, R.K.; Kitada, K.; Kurihara, Y.; Tahara, M.; Hamuro, A.; Nakano, A.; Koyama, M. Placental Types and Effective Perinatal Management of Vasa Previa: Lessons from 55 Cases in a Single Institution. Diagnostics 2021, 11, 1369. [Google Scholar] [CrossRef]
- Gross, A.; Markota Ajd, B.; Specht, C.; Scheier, M. Systematic screening for vasa previa at the 20-week anomaly scan. Acta Obstet. Et Gynecol. Scand. 2021, 100, 1694–1699. [Google Scholar] [CrossRef]
- Sutera, M.; Garofalo, A.; Pilloni, E.; Parisi, S.; Alemanno, M.G.; Menato, G.; Sciarrone, A.; Viora, E. Vasa previa: When antenatal diagnosis can change fetal prognosis. J. Perinat. Med. 2021, 49, 915–922. [Google Scholar] [CrossRef]
- Liu, N.; Hu, Q.; Liao, H.; Wang, X.; Yu, H. Vasa previa: Perinatal outcomes in singleton and multiple pregnancies. Biosci. Trends 2021, 15, 118–125. [Google Scholar] [CrossRef]
- Westcott, J.M.; Simpson, S.; Chasen, S.; Vieira, L.; Stone, J.; Doulaveris, G.; Dar, P.; Bernstein, P.S.; Atallah, F.; Dolin, C.D.; et al. Prenatally diagnosed vasa previa: Association with adverse obstetrical and neonatal outcomes. Am. J. Obstet. Gynecol. MFM 2020, 2, 100206. [Google Scholar] [CrossRef] [PubMed]
- Melcer, Y.; Maymon, R.; Pekar-Zlotin, M.; Levinsohn-Tavor, O.; Tovbin, J.; Jauniaux, E. Evaluation of the impact of vasa previa on feto-placental hormonal synthesis and fetal growth. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 215, 193–196. [Google Scholar] [CrossRef]
- Nohuz, E.; Boulay, E.; Gallot, D.; Lemery, D.; Vendittelli, F. Can we perform a prenatal diagnosis of vasa previa to improve its obstetrical and neonatal outcomes? J. Gynecol. Obstet. Hum. Reprod. 2017, 46, 373–377. [Google Scholar] [CrossRef] [PubMed]
- Carnide, C.; Jerónimo, M.; Faria, D.; Silva, I.S. Twin pregnancy complicated by vasa previa. BMJ Case Rep. 2012, 2012, bcr2012006484. [Google Scholar] [CrossRef]
- Kikuchi, A.; Uemura, R.; Serikawa, T.; Takakuwa, K.; Tanaka, K. Clinical significances of magnetic resonance imaging in prenatal diagnosis of vasa previa in a woman with bilobed placentas. J. Obstet. Gynaecol. Res. 2011, 37, 75–78. [Google Scholar] [CrossRef]
- Hasegawa, J.; Farina, A.; Nakamura, M.; Matsuoka, R.; Ichizuka, K.; Sekizawa, A.; Okai, T. Analysis of the ultrasonographic findings predictive of vasa previa. Prenat. Diagn. 2010, 30, 1121–1125. [Google Scholar] [CrossRef]
- Chmait, R.H.; Chavira, E.; Kontopoulos, E.V.; Quintero, R.A. Third trimester fetoscopic laser ablation of type II vasa previa. J. Matern. -Fetal Neonatal Med. 2010, 23, 459–462. [Google Scholar] [CrossRef]
- Fung, T.Y.; Lau, T.K. Poor perinatal outcome associated with vasa previa: Is it preventable? A report of three cases and review of the literature. Ultrasound Obs. Gynecol. 1998, 12, 430–433. [Google Scholar] [CrossRef]
- Baschat, A.A.; Gembruch, U. Ante- and intrapartum diagnosis of vasa praevia in singleton pregnancies by colour coded Doppler sonography. Eur. J. Obstet. Gynecol. Reprod. Biol. 1998, 79, 19–25. [Google Scholar] [CrossRef]
- Catanzarite, V.; Cousins, L.; Daneshmand, S.; Schwendemann, W.; Casele, H.; Adamczak, J.; Tith, T.; Patel, A. Prenatally Diagnosed Vasa Previa: A Single-Institution Series of 96 Cases. Obstet. Gynecol. 2016, 128, 1153–1161. [Google Scholar] [CrossRef]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed]
- Matsuzaki, S.; Ueda, Y.; Matsuzaki, S.; Nagase, Y.; Kakuda, M.; Lee, M.; Maeda, M.; Kurahashi, H.; Hayashida, H.; Hisa, T.; et al. Assisted Reproductive Technique and Abnormal Cord Insertion: A Systematic Review and Meta-Analysis. Biomedicines 2022, 10, 1722. [Google Scholar] [CrossRef] [PubMed]
- de Los Reyes, S.; Henderson, J.; Eke, A.C. A systematic review and meta-analysis of velamentous cord insertion among singleton pregnancies and the risk of preterm delivery. Int. J. Gynaecol. Obstet. 2018, 142, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Ismail, K.I.; Hannigan, A.; O’Donoghue, K.; Cotter, A. Abnormal placental cord insertion and adverse pregnancy outcomes: A systematic review and meta-analysis. Syst. Rev. 2017, 6, 242. [Google Scholar] [CrossRef]
- Vahanian, S.A.; Lavery, J.A.; Ananth, C.V.; Vintzileos, A. Placental implantation abnormalities and risk of preterm delivery: A systematic review and metaanalysis. Am. J. Obstet. Gynecol. 2015, 213, S78–S90. [Google Scholar] [CrossRef]
- Society for Maternal-Fetal Medicine (SMFM); Ghidini, A.; Gandhi, M.; McCoy, J.; Kuller, J.A.; Publications Committee. Society for Maternal-Fetal Medicine Consult Series #60: Management of pregnancies resulting from in vitro fertilization. Am. J. Obstet. Gynecol. 2022, 226, B2–B12. [Google Scholar] [CrossRef]
- Jauniaux, E.; Englert, Y.; Vanesse, M.; Hiden, M.; Wilkin, P. Pathologic features of placentas from singleton pregnancies obtained by in vitro fertilization and embryo transfer. Obstet. Gynecol. 1990, 76, 61–64. [Google Scholar]
- Yanaihara, A.; Hatakeyama, S.; Ohgi, S.; Motomura, K.; Taniguchi, R.; Hirano, A.; Takenaka, S.; Yanaihara, T. Difference in the size of the placenta and umbilical cord between women with natural pregnancy and those with IVF pregnancy. J. Assist. Reprod. Genet. 2018, 35, 431–434. [Google Scholar] [CrossRef]
- Gavriil, P.; Jauniaux, E.; Leroy, F. Pathologic examination of placentas from singleton and twin pregnancies obtained after in vitro fertilization and embryo transfer. Pediatr. Pathol. 1993, 13, 453–462. [Google Scholar] [CrossRef]
- Hasegawa, J.; Iwasaki, S.; Matsuoka, R.; Ichizuka, K.; Sekizawa, A.; Okai, T. Velamentous cord insertion caused by oblique implantation after in vitro fertilization and embryo transfer. J. Obstet. Gynaecol. Res. 2011, 37, 1698–1701. [Google Scholar] [CrossRef]
- Sinha, P.; Kaushik, S.; Kuruba, N.; Beweley, S. Vasa praevia: A missed diagnosis. J. Obstet. Gynaecol. 2008, 28, 600–603. [Google Scholar] [CrossRef]
- Jansen, C.; Kleinrouweler, C.E.; Kastelein, A.W.; Ruiter, L.; van Leeuwen, E.; Mol, B.W.; Pajkrt, E. Follow-up ultrasound in second-trimester low-positioned anterior and posterior placentae: Prospective cohort study. Ultrasound Obs. Gynecol. 2020, 56, 725–731. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, J.; Matsuoka, R.; Ichizuka, K.; Otsuki, K.; Sekizawa, A.; Farina, A.; Okai, T. Cord insertion into the lower third of the uterus in the first trimester is associated with placental and umbilical cord abnormalities. Ultrasound Obs. Gynecol 2006, 28, 183–186. [Google Scholar] [CrossRef]
- Silver, R.M. Abnormal Placentation: Placenta Previa, Vasa Previa, and Placenta Accreta. Obstet. Gynecol. 2015, 126, 654–668. [Google Scholar] [CrossRef] [PubMed]
- Baergen, R.N.; Matrai, C. Placental Shape Aberrations. In Benirschke’s Pathology of the Human Placenta; Baergen, R.N., Burton, G.J., Kaplan, C.G., Eds.; Springer International Publishing: Cham, Switzerland, 2022; pp. 403–411. [Google Scholar]
- Monie, I.W. Velamentous Insertion of the Cord in Early Pregnancy. Am. J. Obstet. Gynecol. 1965, 93, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, J.; Farina, A.; Simonazzi, G.; Bisulli, M.; Puccetti, C.; Pilu, G.; Gabrielli, S.; Rizzo, N. Umbilical cord insertion into the lower segment of the uterus at 11 to 13 weeks’ gestation is associated with maternal serum PAPP-A. Prenat. Diagn. 2011, 31, 434–438. [Google Scholar] [CrossRef]
- Tsakiridis, I.; Dagklis, T.; Athanasiadis, A.; Dinas, K.; Sotiriadis, A. Impact of Marginal and Velamentous Cord Insertion on Uterine Artery Doppler Indices, Fetal Growth, and Preeclampsia. J. Ultrasound Med. 2021, 41, 2011–2018. [Google Scholar] [CrossRef]
- Hasegawa, J. Sonoembryological evaluations of the development of placenta previa and velamentous cord insertion. J. Obstet. Gynaecol. Res. 2015, 41, 1–5. [Google Scholar] [CrossRef]
- Matsuzaki, S.; Nagase, Y.; Takiuchi, T.; Kakigano, A.; Mimura, K.; Lee, M.; Matsuzaki, S.; Ueda, Y.; Tomimatsu, T.; Endo, M.; et al. Antenatal diagnosis of placenta accreta spectrum after in vitro fertilization-embryo transfer: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 9205. [Google Scholar] [CrossRef]
- Baulies, S.; Maiz, N.; Muñoz, A.; Torrents, M.; Echevarría, M.; Serra, B. Prenatal ultrasound diagnosis of vasa praevia and analysis of risk factors. Prenat. Diagn. 2007, 27, 595–599. [Google Scholar] [CrossRef]
- Yang, M.; Zheng, Y.; Li, M.; Li, W.; Li, X.; Zhang, X.; Wang, R.; Zhang, J.; Zhou, F.; Yang, Q.; et al. Clinical features of velamentous umbilical cord insertion and vasa previa: A retrospective analysis based on 501 cases. Medicine 2020, 99, e23166. [Google Scholar] [CrossRef] [PubMed]
- Cochrane, E.; Pando, C.; Kirschen, G.W.; Soucier, D.; Fuchs, A.; Garry, D.J. Assisted reproductive technologies (ART) and placental abnormalities. J. Perinat. Med. 2020, 48, 825–828. [Google Scholar] [CrossRef] [PubMed]
- O’Quinn, C.; Cooper, S.; Tang, S.; Wood, S. Antenatal Diagnosis of Marginal and Velamentous Placental Cord Insertion and Pregnancy Outcomes. Obstet. Gynecol. 2020, 135, 953–959. [Google Scholar] [CrossRef]
- Kalafat, E.; Thilaganathan, B.; Papageorghiou, A.; Bhide, A.; Khalil, A. Significance of placental cord insertion site in twin pregnancy. Ultrasound Obs. Gynecol. 2018, 52, 378–384. [Google Scholar] [CrossRef]
- Ebbing, C.; Johnsen, S.L.; Albrechtsen, S.; Sunde, I.D.; Vekseth, C.; Rasmussen, S. Velamentous or marginal cord insertion and the risk of spontaneous preterm birth, prelabor rupture of the membranes, and anomalous cord length, a population-based study. Acta Obstet. Et Gynecol. Scand. 2017, 96, 78–85. [Google Scholar] [CrossRef]
- Wang, J.; Liu, Q.; Deng, B.; Chen, F.; Liu, X.; Cheng, J. Pregnancy outcomes of Chinese women undergoing IVF with embryonic cryopreservation as compared to natural conception. BMC Pregnancy Childbirth 2021, 21, 39. [Google Scholar] [CrossRef]
- Qin, J.; Sheng, X.; Wu, D.; Gao, S.; You, Y.; Yang, T.; Wang, H. Adverse Obstetric Outcomes Associated With In Vitro Fertilization in Singleton Pregnancies. Reprod. Sci. 2017, 24, 595–608. [Google Scholar] [CrossRef]
- Healy, D.L.; Breheny, S.; Halliday, J.; Jaques, A.; Rushford, D.; Garrett, C.; Talbot, J.M.; Baker, H.W. Prevalence and risk factors for obstetric haemorrhage in 6730 singleton births after assisted reproductive technology in Victoria Australia. Hum. Reprod. 2010, 25, 265–274. [Google Scholar] [CrossRef]
- Sabban, H.; Zakhari, A.; Patenaude, V.; Tulandi, T.; Abenhaim, H.A. Obstetrical and perinatal morbidity and mortality among in-vitro fertilization pregnancies: A population-based study. Arch. Gynecol. Obstet. 2017, 296, 107–113. [Google Scholar] [CrossRef]
- Matsuzaki, S.; Ueda, Y.; Nagase, Y.; Matsuzaki, S.; Kakuda, M.; Kakuda, S.; Sakaguchi, H.; Hisa, T.; Kamiura, S. Placenta Accreta Spectrum Disorder Complicated with Endometriosis: Systematic Review and Meta-Analysis. Biomedicines 2022, 10, 390. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author | Year | Location | Type | Total | VP | N | Frequency | ART | Outcome | Type I vs. II |
|---|---|---|---|---|---|---|---|---|---|---|
| Degirmenci Y [38] | 2022 | GER | Series | -- | 5 | 3 | -- | -- | Yes | -- |
| Tachibana D [39] | 2021 | JPN | Original | -- | 55 | 13 | 13/55 (23.6%) | Yes | Yes | Yes |
| Gross A [40] | 2021 | AUS | Original | 5905 | 21 | 3 | 3/21 (14.3%) | -- | -- | Yes |
| Sutera M [41] | 2021 | ITA | Original | 89,600 | 24 | 9 | 9/24 (37.5%) | -- | -- | Yes |
| Liu N [42] | 2021 | CHN | Original | 79,647 | 157 | 12 | 12/157 (7.6%) | Yes | Yes | Yes |
| Westcott JM [43] | 2020 | USA | Original | -- | 122 | 35 | 35/122 (28.7%) | -- | -- | Yes |
| Melcer Y [44] | 2017 | GBR | Original | -- | 32 | 11 | 11/32 (34.4%) | Yes | Yes | Yes |
| Nohuz E [45] | 2017 | FRN | Series | -- | 8 | 5 | -- | -- | -- | -- |
| Catanzarite V [52] | 2016 | USA | Original | -- | 96 | 25 | 25/96 (26.0%) | -- | -- | -- |
| Carnide C [46] | 2012 | PRT | Case | -- | 1 | 1 | -- | -- | Yes | -- |
| Kikuchi A [47] | 2011 | JPN | Case | -- | 1 | 1 | -- | -- | Yes | -- |
| Hasegawa J [48] | 2010 | JPN | Series | -- | 10 | 4 | -- | -- | Yes | -- |
| Chmait RH [49] | 2010 | USA | Case | -- | 2 | 2 | -- | -- | Yes | -- |
| Catanzarite V [14] | 2001 | USA | Series | -- | 10 | 8 | -- | -- | Yes | -- |
| Fung TY [50] | 1998 | HKG | Series | -- | 3 | 1 | -- | -- | Yes | -- |
| Baschat AA [51] | 1998 | GER | Series | -- | 5 | 4 | -- | -- | Yes | -- |
| Author | Year | Total | N | Type I | Type II | OR (95%CI) |
|---|---|---|---|---|---|---|
| ART | ||||||
| Tachibana D [39] | 2021 | 55 | 20 # | 21/35 (60.0%) | 5/20 (25.0%) | 0.22 (0.07–0.75) |
| Liu N [42] | 2021 | 157 | 12 | 28/141 (19.9%) | 0/12 (0%) | 0.16 (0.01–2.77) |
| Melcer Y [44] | 2017 | 32 | 11 | 8/21 (38.1%) | 6/11 (54.5%) | 1.95 (0.09–2.45) |
| Antenatal Diagnosis | ||||||
| Sutera M [41] | 2021 | 24 | 9 | 13/15 (86.7%) | 7/9 (77.8%) | 0.54 (0.06–4.69) |
| Liu N [42] | 2021 | 157 | 12 | 121/141 (85.8%) | 12/12 (100%) | 1.06 (0.16–6.94) |
| Melcer Y [44] | 2017 | 32 | 11 | 17/21 (81.0%) | 9/11 (81.8%) | 4.22 (0.24–74.04) |
| Emergent cesarean delivery | ||||||
| Tachibana D [39] | 2021 | 55 | 20 # | 17/35 (48.6%) | 9/20 (45.0%) | 0.87 (0.29–2.61) |
| Liu N [42] | 2021 | 157 | 12 | 38/141 (27.0%) | 1/12 (8.3%) | 0.25 (0.03–1.97) |
| Westcott JM [43] | 2020 | 122 | 35 | 32/86 (37.2%) | 14/35 (40%) | 1.81 (0.84–3.91) |
| Melcer Y [44] | 2017 | 32 | 11 | 6/21 (28.6%) | 6/11 (54.5%) | 3.00 (0.66–13.69) |
| GA at delivery | ||||||
| Tachibana D [39] | 2021 | 55 | 20 # | 35.2 ± 2.1 $ | 34.3 ± 1.6 | 0.90 (−0.09–1.89) |
| Liu N [42] | 2021 | 157 | 12 | 35.2 ± 1.9 | 35.0 ± 1.6 | 0.20 (−0.76–1.16) |
| Melcer Y [44] | 2017 | 32 | 11 | 36.4 ± 1.4 | 37.4 ± 1.5 | −1.00 (−2.07–0.07) |
| Maternal Transfusion | ||||||
| Tachibana D [39] | 2021 | 55 | 20 # | 11/35 (31.4%) | 10/20 (50.0%) | 2.18 (0.70–6.76) |
| Neonatal Death | ||||||
| Tachibana D [39] | 2021 | 55 | 20 # | 0/35 (0%) | 0/20 (0%) | -- |
| Liu N [42] | 2021 | 157 | 12 | 3/141 (2.1%) | 2/12 (16.7%) | 9.20 (1.37–61.56) |
| Gross A [40] | 2021 | 21 | 3 | 0/18 (0%) | 0/3 (0%) | -- |
| Author | Year | N | VP | Placenta |
| The rate of vasa previa in women with succenturiate lobes | ||||
| Gross A [40] | 2021 | 68 | 3 | Succenturiate lobes, bilobed |
| Suzuki S [36] | 2010 | 83 | 1 | Succenturiate lobes |
| Author | Year | N | Ab | Type of ART |
| ART and abnormal placenta | ||||
| Volodarsky A [34] | 2021 | 677 | 17 | Blastocyst versus Cleavage |
| Sacha CR [35] | 2020 | 1140 | 70 | Frozen versus Fresh |
| Suzuki S [37] | 2008 | 7713 | 47 | ART versus non-ART |
| Author | Year | Total | N | Placenta | Exp | Cont | Unadjusted OR (95%CI) | Adjusted OR (95%CI) |
|---|---|---|---|---|---|---|---|---|
| ART vs. non-ART | ||||||||
| Suzuki S [37] | 2008 | 7713 | 47 | Suc | 4/105 (3.8%) | 43/7608 (0.6%) | 6.97 (2.45–19.78) | -- |
| Blastocyst vs. Cleavage (Fresh) | ||||||||
| Volodarsky A [34] | 2021 | 677 | 17 | Bil, Suc | 12/425 (3.3%) | 5/252 (2.0%) | 1.44 (0.50–4.12) | -- |
| Frozen vs. Fresh | ||||||||
| Sacha CR [35] | 2020 | 1140 | 70 | Suc | 22/211 (10.4%) | 48/929 (5.2%) | 2.50 (1.08–5.76) | 2.97 (1.10–7.96) |
| Day 5 Frozen vs. Fresh | ||||||||
| Sacha CR [35] | 2020 | 630 | 39 | Suc | 20/184 (10.9%) | 19/466 (4.1%) | 6.72 (1.62–27.77) | 5.32 (1.54–18.38) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsuzaki, S.; Ueda, Y.; Matsuzaki, S.; Kakuda, M.; Lee, M.; Takemoto, Y.; Hayashida, H.; Maeda, M.; Kakubari, R.; Hisa, T.; et al. The Characteristics and Obstetric Outcomes of Type II Vasa Previa: Systematic Review and Meta-Analysis. Biomedicines 2022, 10, 3263. https://doi.org/10.3390/biomedicines10123263
Matsuzaki S, Ueda Y, Matsuzaki S, Kakuda M, Lee M, Takemoto Y, Hayashida H, Maeda M, Kakubari R, Hisa T, et al. The Characteristics and Obstetric Outcomes of Type II Vasa Previa: Systematic Review and Meta-Analysis. Biomedicines. 2022; 10(12):3263. https://doi.org/10.3390/biomedicines10123263
Chicago/Turabian StyleMatsuzaki, Shinya, Yutaka Ueda, Satoko Matsuzaki, Mamoru Kakuda, Misooja Lee, Yuki Takemoto, Harue Hayashida, Michihide Maeda, Reisa Kakubari, Tsuyoshi Hisa, and et al. 2022. "The Characteristics and Obstetric Outcomes of Type II Vasa Previa: Systematic Review and Meta-Analysis" Biomedicines 10, no. 12: 3263. https://doi.org/10.3390/biomedicines10123263
APA StyleMatsuzaki, S., Ueda, Y., Matsuzaki, S., Kakuda, M., Lee, M., Takemoto, Y., Hayashida, H., Maeda, M., Kakubari, R., Hisa, T., Mabuchi, S., & Kamiura, S. (2022). The Characteristics and Obstetric Outcomes of Type II Vasa Previa: Systematic Review and Meta-Analysis. Biomedicines, 10(12), 3263. https://doi.org/10.3390/biomedicines10123263