

Obeticholic Acid for Primary Biliary Cholangitis



Abstract
1. Introduction
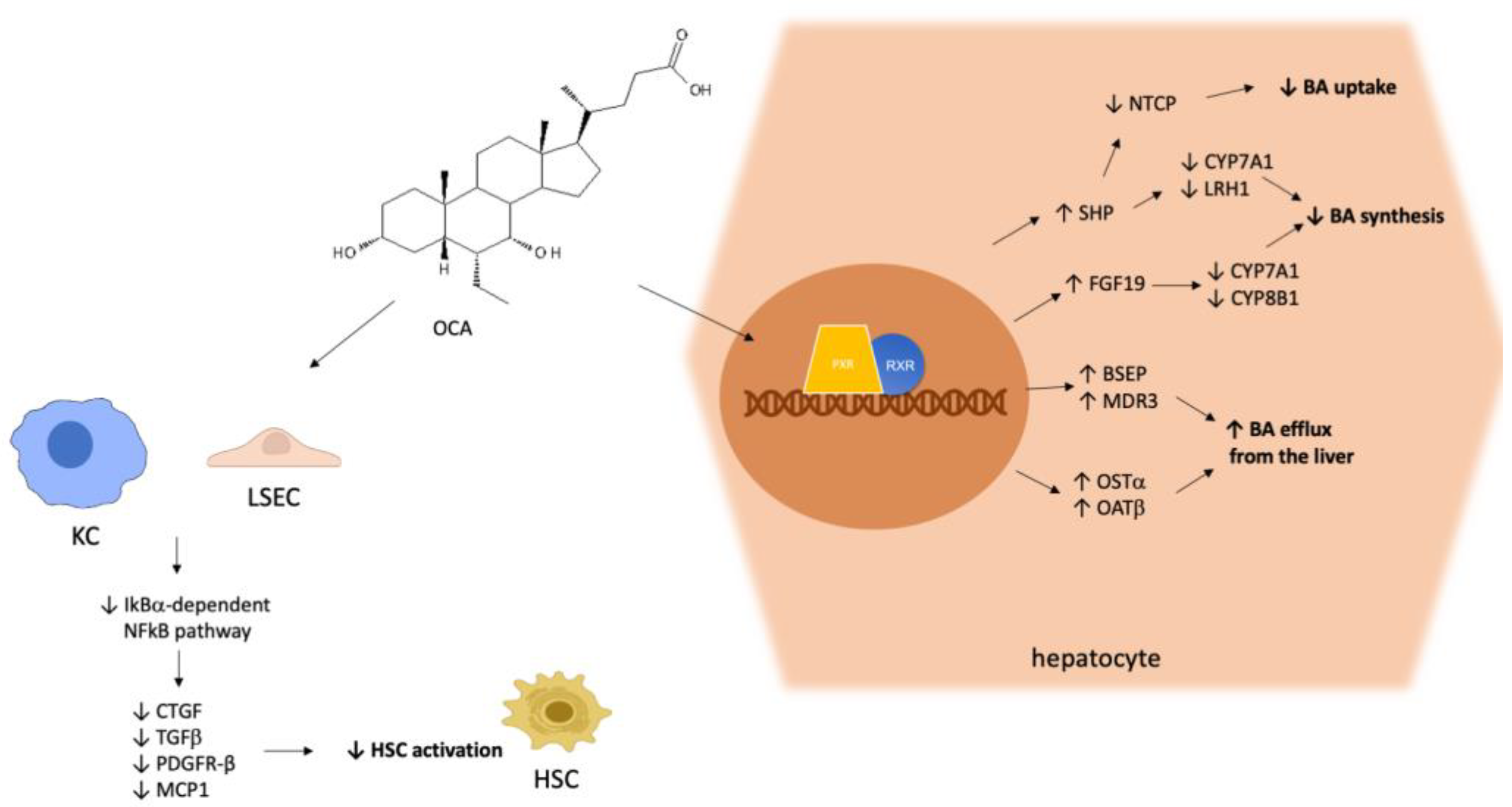
2. Pharmacological Actions of OCA
3. Pre-Registration Studies
4. Real-World Data on OCA
5. Combined Therapy with OCA and Fibrates
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Gulamhusein, A.F.; Hirschfield, G.M. Primary Biliary Cholangitis: Pathogenesis and Therapeutic Opportunities. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 93–110. [Google Scholar] [CrossRef] [PubMed]
- Lv, T.; Chen, S.; Li, M.; Zhang, D.; Kong, Y.; Jia, J. Regional Variation and Temporal Trend of Primary Biliary Cholangitis Epidemiology: A Systematic Review and Meta-analysis. J. Gastroenterol. Hepatol. 2021, 36, 1423–1434. [Google Scholar] [CrossRef] [PubMed]
- Murillo Perez, C.F.; Goet, J.C.; Lammers, W.J.; Gulamhusein, A.; van Buuren, H.R.; Ponsioen, C.Y.; Carbone, M.; Mason, A.; Corpechot, C.; Invernizzi, P.; et al. Milder Disease Stage in Patients with Primary Biliary Cholangitis over a 44-year Period: A Changing Natural History. Hepatology 2018, 67, 1920–1930. [Google Scholar] [CrossRef] [PubMed]
- Prince, M.I. Asymptomatic Primary Biliary Cirrhosis: Clinical Features, Prognosis, and Symptom Progression in a Large Population Based Cohort. Gut 2004, 53, 865–870. [Google Scholar] [CrossRef] [PubMed]
- Invernizzi, P.; Lleo, A.; Podda, M. Interpreting Serological Tests in Diagnosing Autoimmune Liver Diseases. Semin. Liver Dis. 2007, 27, 161–172. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver; Hirschfield, G.M.; Beuers, U.; Corpechot, C.; Invernizzi, P.; Jones, D.; Marzioni, M.; Schramm, C. EASL Clinical Practice Guidelines: The Diagnosis and Management of Patients with Primary Biliary Cholangitis. J. Hepatol. 2017, 67, 145–172. [Google Scholar] [CrossRef] [PubMed]
- Harms, M.H.; van Buuren, H.R.; Corpechot, C.; Thorburn, D.; Janssen, H.L.A.; Lindor, K.D.; Hirschfield, G.M.; Parés, A.; Floreani, A.; Mayo, M.J.; et al. Ursodeoxycholic Acid Therapy and Liver Transplant-Free Survival in Patients with Primary Biliary Cholangitis. J. Hepatol. 2019, 71, 357–365. [Google Scholar] [CrossRef]
- Selmi, C.; Bowlus, C.L.; Gershwin, M.E.; Coppel, R.L. Primary Biliary Cirrhosis. Lancet 2011, 377, 1600–1609. [Google Scholar] [CrossRef]
- Carbone, M.; Mells, G.F.; Pells, G.; Dawwas, M.F. Sex and age are determinants of the clinical phenotype of primary biliary cirrhosis and response to ursodeoxycholic acid. Gastroenterology 2013, 144, 560–569. [Google Scholar] [CrossRef]
- Cheung, A.C.; Lammers, W.J.; Murillo Perez, C.F.; van Buuren, H.R.; Gulamhusein, A.; Trivedi, P.J.; Lazaridis, K.N. Effects of age and sex on response to ursodeoxycholic acid and transplant-free survival in patients with primary biliary cholangitis. Clin. Gastreonetrol. Hepatol. 2019, 17, 2076–2084. [Google Scholar] [CrossRef]
- Beuers, U.; Trauner, M.; Jansen, P.; Poupon, R. New Paradigms in the Treatment of Hepatic Cholestasis: From UDCA to FXR, PXR and Beyond. J. Hepatol. 2015, 62, S25–S37. [Google Scholar] [CrossRef] [PubMed]
- Pellicciari, R.; Costantino, G.; Camaioni, E.; Sadeghpour, B.M.; Entrena, A.; Willson, T.M.; Fiorucci, S.; Clerici, C.; Gioiello, A. Bile Acid Derivatives as Ligands of the Farnesoid X Receptor. Synthesis, Evaluation, and Structure-Activity Relationship of a Series of Body and Side Chain Modified Analogues of Chenodeoxycholic Acid. J. Med. Chem. 2004, 47, 4559–4569. [Google Scholar] [CrossRef] [PubMed]
- Chiang, J.Y.L. Bile Acid Metabolism and Signaling in Liver Disease and Therapy. Liver Res. 2017, 1, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Sayaf, K.; Zanotto, I.; Russo, F.P.; Gabbia, D.; De Martin, S. The Nuclear Receptor PXR in Chronic Liver Disease. Cells 2021, 11, 61. [Google Scholar] [CrossRef]
- Gabbia, D.; Dalla Pozza, A.; Albertoni, L.; Lazzari, R.; Zigiotto, G.; Carrara, M.; Baldo, V.; Baldovin, T.; Floreani, A.; De Martin, S. Pregnane X Receptor and Constitutive Androstane Receptor Modulate Differently CYP3A-Mediated Metabolism in Early- and Late-Stage Cholestasis. World J. Gastroenterol. 2017, 23, 7519–7530. [Google Scholar] [CrossRef]
- Goodwin, B.; Jones, S.A.; Price, R.R.; Watson, M.A.; McKee, D.D.; Moore, L.B.; Galardi, C.; Wilson, J.G.; Lewis, M.C.; Roth, M.E.; et al. A Regulatory Cascade of the Nuclear Receptors FXR, SHP-1, and LRH-1 Represses Bile Acid Biosynthesis. Mol. Cell 2000, 6, 517–526. [Google Scholar] [CrossRef]
- Sun, Y.; Demagny, H.; Schoonjans, K. Emerging Functions of the Nuclear Receptor LRH-1 in Liver Physiology and Pathology. Biochim. Biophys. Acta (BBA)—Mol. Basis Dis. 2021, 1867, 166145. [Google Scholar] [CrossRef]
- Maliha, S.; Guo, G.L. Farnesoid X Receptor and Fibroblast Growth Factor 15/19 as Pharmacological Targets. Liver Res. 2021, 5, 142–150. [Google Scholar] [CrossRef]
- Salhab, A.; Amer, J.; Lu, Y.; Safadi, R. Sodium +/Taurocholate Cotransporting Polypeptide as Target Therapy for Liver Fibrosis. Gut 2022, 71, 1373–1385. [Google Scholar] [CrossRef]
- Halilbasic, E.; Claudel, T.; Trauner, M. Bile Acid Transporters and Regulatory Nuclear Receptors in the Liver and Beyond. J. Hepatol. 2013, 58, 155–168. [Google Scholar] [CrossRef]
- Cariello, M.; Piccinin, E.; Garcia-Irigoyen, O.; Sabbà, C.; Moschetta, A. Nuclear Receptor FXR, Bile Acids and Liver Damage: Introducing the Progressive Familial Intrahepatic Cholestasis with FXR Mutations. Biochim. Biophys. Acta (BBA)—Mol. Basis Dis. 2018, 1864, 1308–1318. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Huang, X.; Yi, T.; Yen, Y.; Moore, D.D.; Huang, W. Spontaneous Development of Liver Tumors in the Absence of the Bile Acid Receptor Farnesoid X Receptor. Cancer Res. 2007, 67, 863–867. [Google Scholar] [CrossRef] [PubMed]
- Fiorucci, S.; Antonelli, E.; Rizzo, G.; Renga, B.; Mencarelli, A.; Riccardi, L.; Orlandi, S.; Pellicciari, R.; Morelli, A. The Nuclear Receptor SHP Mediates Inhibition of Hepatic Stellate Cells by FXR and Protects against Liver Fibrosis. Gastroenterology 2004, 127, 1497–1512. [Google Scholar] [CrossRef] [PubMed]
- Fickert, P.; Hirschfield, G.M.; Denk, G.; Marschall, H.-U.; Altorjay, I.; Färkkilä, M.; Schramm, C.; Spengler, U.; Chapman, R.; Bergquist, A.; et al. NorUrsodeoxycholic Acid Improves Cholestasis in Primary Sclerosing Cholangitis. J. Hepatol. 2017, 67, 549–558. [Google Scholar] [CrossRef] [PubMed]
- Fickert, P.; Fuchsbichler, A.; Moustafa, T.; Wagner, M.; Zollner, G.; Halilbasic, E.; Stöger, U.; Arrese, M.; Pizarro, M.; Solís, N.; et al. Farnesoid X Receptor Critically Determines the Fibrotic Response in Mice but Is Expressed to a Low Extent in Human Hepatic Stellate Cells and Periductal Myofibroblasts. Am. J. Pathol. 2009, 175, 2392–2405. [Google Scholar] [CrossRef]
- Verbeke, L.; Mannaerts, I.; Schierwagen, R.; Govaere, O.; Klein, S.; Vander Elst, I.; Windmolders, P.; Farre, R.; Wenes, M.; Mazzone, M.; et al. FXR Agonist Obeticholic Acid Reduces Hepatic Inflammation and Fibrosis in a Rat Model of Toxic Cirrhosis. Sci. Rep. 2016, 6, 33453. [Google Scholar] [CrossRef]
- Friedman, S.L. Hepatic Stellate Cells: Protean, Multifunctional, and Enigmatic Cells of the Liver. Physiol. Rev. 2008, 88, 125–172. [Google Scholar] [CrossRef]
- Gabbia, D.; Cannella, L.; De Martin, S. The Role of Oxidative Stress in NAFLD–NASH–HCC Transition—Focus on NADPH Oxidases. Biomedicines 2021, 9, 687. [Google Scholar] [CrossRef]
- Modica, S.; Petruzzelli, M.; Bellafante, E.; Murzilli, S.; Salvatore, L.; Celli, N.; Di Tullio, G.; Palasciano, G.; Moustafa, T.; Halilbasic, E.; et al. Selective Activation of Nuclear Bile Acid Receptor FXR in the Intestine Protects Mice Against Cholestasis. Gastroenterology 2012, 142, 355–365.e4. [Google Scholar] [CrossRef]
- Chapman, R.W.; Lynch, K.D. Obeticholic Acid—A New Therapy in PBC and NASH. Br. Med. Bull. 2020, 133, 95–104. [Google Scholar] [CrossRef]
- Kowdley, K.V.; Luketic, V.; Chapman, R.; Hirschfield, G.M.; Poupon, R.; Schramm, C. A randomized trial of obeticholic acid monotherapy in patients with primary biliary cholangitis. Hepatology 2018, 67, 1890–1902. [Google Scholar] [CrossRef] [PubMed]
- Nevens, F.; Andreone, P.; Mazzella, G.; Strasser, S.I.; Bowlus, C.; Invernizzi, P.; Drenth, J.P.H.; Pockros, P.J.; Regula, J.; Beuers, U.; et al. A Placebo-Controlled Trial of Obeticholic Acid in Primary Biliary Cholangitis. N. Engl. J. Med. 2016, 375, 631–643. [Google Scholar] [CrossRef] [PubMed]
- Trauner, M.; Nevens, F.; Shiffman, M.L.; Drenth, J.P.H.; Bowlus, C.L.; Vargas, V.; Andreone, P.; Hirschfield, G.M.; Pencek, R.; Malecha, E.S.; et al. Long-Term Efficacy and Safety of Obeticholic Acid for Patients with Primary Biliary Cholangitis: 3-Year Results of an International Open-Label Extension Study. Lancet Gastroenterol. Hepatol. 2019, 4, 445–453. [Google Scholar] [CrossRef]
- Parés, A.; Shiffman, M.; Vargas, V.; Invernizzi, P.; Malecha, E.S.; Liberman, A.; MacConell, L.; Hirschfield, G. Reduction and Stabilization of Bilirubin with Obeticholic Acid Treatment in Patients with Primary Biliary Cholangitis. Liver Int. 2020, 40, 1121–1129. [Google Scholar] [CrossRef] [PubMed]
- Bowlus, C.L.; Pockros, P.J.; Kremer, A.E.; Parés, A.; Forman, L.M.; Drenth, J.P.H.; Ryder, S.D.; Terracciano, L.; Jin, Y.; Liberman, A.; et al. Long-Term Obeticholic Acid Therapy Improves Histological Endpoints in Patients With Primary Biliary Cholangitis. Clin. Gastroenterol. Hepatol. 2020, 18, 1170–1178.e6. [Google Scholar] [CrossRef]
- Hirschfield, G.M.; Floreani, A.; Tivedi, P.J.; Pencek, R.; Liberman, A.; Marmon, T.; MacConell, L. Long-term effect of obeticholic acid on transient elastography and AST to platelet ratio index in patients with PBC. Gut 2017, 66 (Suppl. 2), A98–A99. [Google Scholar]
- Younossi, Z.M.; Ratziu, V.; Loombar, R.; Rinella, M.; Anstee, Q.M.; Goodman, Z.; Bedossa, P. Obeticholic acid for the treatment of non-alcoholic steatohepatitis: Interim analysis from a multicentre, randomised, placebo-controlled phase 3 trial. Lancet 2019, 394, 2184–2196. [Google Scholar] [CrossRef]
- Kjærgaard, K.; Frisch, K.; Sørensen, M.; Munk, O.L.; Hofmann, A.F.; Horsager, J.; Schacht, A.C.; Erickson, M.; Shapiro, D.; Keiding, S. Obeticholic Acid Improves Hepatic Bile Acid Excretion in Patients with Primary Biliary Cholangitis. J. Hepatol. 2021, 74, 58–65. [Google Scholar] [CrossRef]
- Hirschfield, G.M.; Mason, A.; Luketic, V.; Lindor, K.; Gordon, S.C.; Mayo, M.; Kowdley, K.V.; Vincent, C.; Bodhenheimer, H.C.; Parés, A.; et al. Efficacy of Obeticholic Acid in Patients With Primary Biliary Cirrhosis and Inadequate Response to Ursodeoxycholic Acid. Gastroenterology 2015, 148, 751–761.e8. [Google Scholar] [CrossRef]
- Obeticholic Acid. No author listed. In LiverTox: Clinical and Research Information on Drug-Induced Liver Injury; National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2012. [Google Scholar]
- Roberts, S.B.; Ismail, M.; Kanagalingam, G.; Mason, A.L.; Swain, M.G.; Vincent, C.; Yoshida, E.M.; Tsien, C.; Flemming, J.A.; Janssen, H.L.A.; et al. Real-World Effectiveness of Obeticholic Acid in Patients with Primary Biliary Cholangitis. Hepatol. Commun. 2020, 4, 1332–1345. [Google Scholar] [CrossRef]
- Gomez, E.; Garcia Buey, L.; Molina, E.; Casado, M.; Conde, I.; Berenguer, M.; Jorquera, F.; Simón, M.-A.; Olveira, A.; Hernández-Guerra, M.; et al. Effectiveness and Safety of Obeticholic Acid in a Southern European Multicentre Cohort of Patients with Primary Biliary Cholangitis and Suboptimal Response to Ursodeoxycholic Acid. Aliment. Pharmacol. Ther. 2021, 53, 519–530. [Google Scholar] [CrossRef] [PubMed]
- D’Amato, D.; De Vincentis, A.; Malinverno, F.; Viganò, M.; Alvaro, D.; Pompili, M.; Picciotto, A.; Palitti, V.P.; Russello, M.; Storato, S.; et al. Real-World Experience with Obeticholic Acid in Patients with Primary Biliary Cholangitis. JHEP Rep. 2021, 3, 100248. [Google Scholar] [CrossRef] [PubMed]
- Corpechot, C.; Chazouilleres, O.; Poupon, R. Early primary biliary cirrhosis: Biochemical response to treatment and prediction of long-term outcome. J. Hepatol. 2011, 55, 1361–1367. [Google Scholar] [CrossRef] [PubMed]
- De Vincentis, A.; D’Amato, D.; Cristoferi, L.; Gerussi, A.; Malinverno, F.; Lleo, A.; Colapietro, F. Predictors of serious adverse events and non-response in cirrhotic patients with primary biliary cholangitis treated with obeticholic acid. Liver Int. 2022, in press. [Google Scholar] [CrossRef] [PubMed]
- Gulamhusein, A.F.; Roberts, S.B.; Hallidey, N.; Carbone, M.; Yimam, K.; Namphurong, T. Real World Effectiveness of Obeticholic Acid in Patients with Primary Biliary Cholangitis: The Global Experience. Hepatology 2020, S1, 1267. [Google Scholar]
- Gish, R.G.; Law, A.; Adekunle, F.; Wheeler, D.; Lingohr-Smith, M.; Bassanelli, C. Real-World Effectiveness of Obeticholic Acid in Patients with Primary Biliary Cholangitis. Hepatology 2020, S1, 1268. [Google Scholar]
- Kumagi, T.; Guindi, M.; Fischer, S.E.; Arenovich, T.; Abdalian, R.; Coltescu, C.; Heathcote, J.E.; Hirschfield, G.M. Baseline ductopenia and treatment response predict long-term histological progression in primary biliary cirrhosis. Am. J. Gastroenterol. 2010, 105, 2186–2194. [Google Scholar] [CrossRef]
- Abbass, N.; Culver, E.L.; Thornburn, D.; Halliday, N.; Crothers, H.; Dyson, J.K.; Phaw, A.; Aspinall, R.; Khakoo, S.I.; Kallis, Y.; et al. UK-wide multicenter evaluation of second-line therapies in primary biliary cholangitis. Clin. Gastroenterol. Hepatol. 2022, in press. [Google Scholar] [CrossRef]
- Murillo Perez, C.F.; Fisher, H.; Hin, S.; Kareithi, D.; Adekunle, F.; Mayne, T.; Malecha, E.; Ness, E.; van der Meer, A.J.; Lammers, W.J.; et al. Greater Transplant-Free Survival in Patients Receiving Obeticholic Acid for Primary Biliary Cholangitis in a Clinical Trial Setting Compared to Real-World External Controls. Gastroenterology 2022, S0016-5085(22)01060-5. [Google Scholar] [CrossRef]
- Ghonem, N.S.; Ananthanarayanan, M.; Soroka, C.J.; Boyer, J.L. Peroxisome Proliferator-Activated Receptor α Activates Human Multidrug Resistance Transporter 3/ATP-Binding Cassette Protein Subfamily B4 Transcription and Increases Rat Biliary Phosphatidylcholine Secretion. Hepatology 2014, 59, 1030–1042. [Google Scholar] [CrossRef]
- Honda, A.; Ikegami, T.; Nakamuta, M.; Miyazaki, T.; Iwamoto, J.; Hirayama, T.; Saito, Y.; Takikawa, H.; Imawari, M.; Matsuzaki, Y. Anticholestatic Effects of Bezafibrate in Patients with Primary Biliary Cirrhosis Treated with Ursodeoxycholic Acid. Hepatology 2013, 57, 1931–1941. [Google Scholar] [CrossRef] [PubMed]
- Corpechot, C.; Chazouillères, O.; Rousseau, A.; Le Gruyer, A.; Habersetzer, F.; Mathurin, P.; Goria, O.; Potier, P.; Minello, A.; Silvain, C.; et al. A Placebo-Controlled Trial of Bezafibrate in Primary Biliary Cholangitis. N. Engl. J. Med. 2018, 378, 2171–2181. [Google Scholar] [CrossRef] [PubMed]
- Summerfield, J.A.; Elias, E.; Sherlock, S. Effects of Clofibrate in Primary Biliary Cirrhosis Hypercholesterolemia and Gallstones. Gastroenterology 1975, 69, 998–1000. [Google Scholar] [CrossRef]
- Soret, P.-A.; Lam, L.; Carrat, F.; Smets, L.; Berg, T.; Carbone, M.; Invernizzi, P.; Leroy, V.; Trivedi, P.; Cazzagon, N.; et al. Combination of Fibrates with Obeticholic Acid Is Able to Normalise Biochemical Liver Tests in Patients with Difficult-to-Treat Primary Biliary Cholangitis. Aliment. Pharmacol. Ther. 2021, 53, 1138–1146. [Google Scholar] [CrossRef] [PubMed]
- Lindor, K.D.; Bowlus, C.L.; Boyer, J.; Levy, C.; Mayo, M. Primary Biliary Cholangitis: 2021 Practice Guidance Update from the American Association for the Study of Liver Diseases. Hepatology 2022, 75, 1012–1013. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| NCT Number [Ref] | Type of Study | Therapeutic Scheme | Population | Outcome | Adverse Events |
|---|---|---|---|---|---|
| NCT00570765 [31] | Phase II study, 3-month randomized, double-blind, placebo-controlled, parallel group phase, followed by a long-term safety extension (LTSE) | OCA monotherapy (10 or 50 mg) | 60 PBC patients (18–70 years) | ALP reduction at both dosages after a 3-month treatment. Improvement of GGT, ALT, conjugated bilirubin, IgG | Pruritus (placebo 35%, OCA 10 70%, 94% OCA 50 |
| NCT01473524 [32,33] | Phase III study, international 12-month randomized, double-blind (DB), placebo-controlled, parallel group phase, followed by a long-term safety extension (LTSE) phase of up to 5 years | OCA 5 mg (6 months) up to 10 mg or 10 mg vs. placebo | 217 patients (≥18 years) | ALP reduction only after 12-month treatment with combination Reduction in total and direct bilirubin | Pruritus (56% in the 5–10% group and 68% in the 10 mg group vs. 38% placebo |
| NCT03253276 [38] | Early phase I, double-blind placebo-controlled crossover study | OCA vs. placebo | 8 PBC patients | OCA reduced the time hepatocytes are exposed to potentially cytotoxic bile acids. | 1 patient dropped for pruritus |
| NCT00550862 [39] | Phase II, randomized, double-blind study | OCA (10, 25, 50 mg) plus UDCA combination | 165 patients (18–75 years) | Significant reduction in ALP, γ-GT, and ALT compared with placebo, in patients with PBC experiencing an inadequate response to UDCA | 13% discontinuation for pruritus |
| NCT Number | Type of Study | Therapeutic Scheme | Estimated Enrollment | Primary Endpoints |
|---|---|---|---|---|
| NCT05450887 | Randomized, double-blind, multicenter, placebo-controlled phase III clinical trial | OCA (5 mg titrated to 10 mg) ± UDCA vs. placebo ± UDCA (13~15 mg/kg/day) | 156 PBC patients (18–75 years) | Percentage of PBC patients reaching ALP < 1.67× Upper Limit of Normal, and ALP decrease ≥ 15% from baseline, and total bilirubin ≤ ULN after 12-month treatment |
| NCT03703076 | Post-authorization non-interventional observational, multi-site study | OCA (5 or 10 mg) | 150 patients | Response to Ocaliva® after 12-month treatment (monotherapy or combination) assessed by Paris II response criteria |
| NCT05293938 | Retrospective study | OCA (5 or 10 mg) and UDCA | 2544 participants | Time to the first occurrence of the composite endpoint of all-cause death, liver transplant, or hospitalization for hepatic decompensation after 67 months |
| NCT05292872 (HEROES PBC) | Retrospective study | OCA (5 or 10 mg) and UDCA | 3156 participants | Time to the first occurrence of all-cause death, liver transplant, or hospitalization for hepatic decompensation after 67 months |
| NCT05239468 | Phase IIa, double-blind, randomized, active-controlled, parallel group study | Bezafibrate 100 or 200 mg, OCA 5 mg, Bezafibrate placebo, OCA placebo | 60 patients | ALP change after 12 weeks vs. baseline |
| NCT04594694 | Phase II, double-blind, randomized, parallel group study | Bezafibrate 200 or 400 mg, OCA mg, Bezafibrate placebos, OCA placebo | 75 patients | ALP change after 12 weeks vs. baseline |
| NCT04076527 | Prospective, multicenter cohort study | OCA vs. UDCA | 1200 patients | Construction of a systematic registry to describe the characteristics and the recent state of usual clinical care of the respective population |
| NCT04956328 | Multicenter, randomized, double-blind trial | OCA (5 to 10 mg) + UDCA, or placebo + UDCA | 120 patients | Percentage of PBC patients reaching ALP < 1.67× ULN, and ALP decrease ≥ 15% from baseline, and total bilirubin ≤ ULN after 48week-treatment |
| Author | Country | N. of Patients | Inclusion Criteria | % of Cirrhosis | % of pts with AIH/PBC Overlap | % of Response According to POISE |
|---|---|---|---|---|---|---|
| Roberts | Canada | 64 | Hepatologist’s discretion | 23.7 | 6.3 | 18 |
| Gomez | Spain/Portugal | 120 | Lack of response to Paris II criteria | 21.7 | 10 | 29.5 |
| D’Amato | Italy | 191 | ALP > 1.5 UNL | 32 | 15 | 51.9 |
| Outcome | Baseline Dual | Baseline Triple | Last Follow-Up Triple |
|---|---|---|---|
| ALP (xULN) | 2.5 | 1.8 | 1.1 |
| Normal ALP (%) | 0.7 | 10.3 | 47.4 |
| Absence of pruritus | 41.1 | 51.8 | 66.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Floreani, A.; Gabbia, D.; De Martin, S. Obeticholic Acid for Primary Biliary Cholangitis. Biomedicines 2022, 10, 2464. https://doi.org/10.3390/biomedicines10102464
Floreani A, Gabbia D, De Martin S. Obeticholic Acid for Primary Biliary Cholangitis. Biomedicines. 2022; 10(10):2464. https://doi.org/10.3390/biomedicines10102464
Chicago/Turabian StyleFloreani, Annarosa, Daniela Gabbia, and Sara De Martin. 2022. "Obeticholic Acid for Primary Biliary Cholangitis" Biomedicines 10, no. 10: 2464. https://doi.org/10.3390/biomedicines10102464
APA StyleFloreani, A., Gabbia, D., & De Martin, S. (2022). Obeticholic Acid for Primary Biliary Cholangitis. Biomedicines, 10(10), 2464. https://doi.org/10.3390/biomedicines10102464