
A Retrospective Comparison of Three Patient-Controlled Analgesic Strategies: Intravenous Opioid Analgesia Plus Abdominal Wall Nerve Blocks versus Epidural Analgesia versus Intravenous Opioid Analgesia Alone in Open Liver Surgery

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Material and Methods
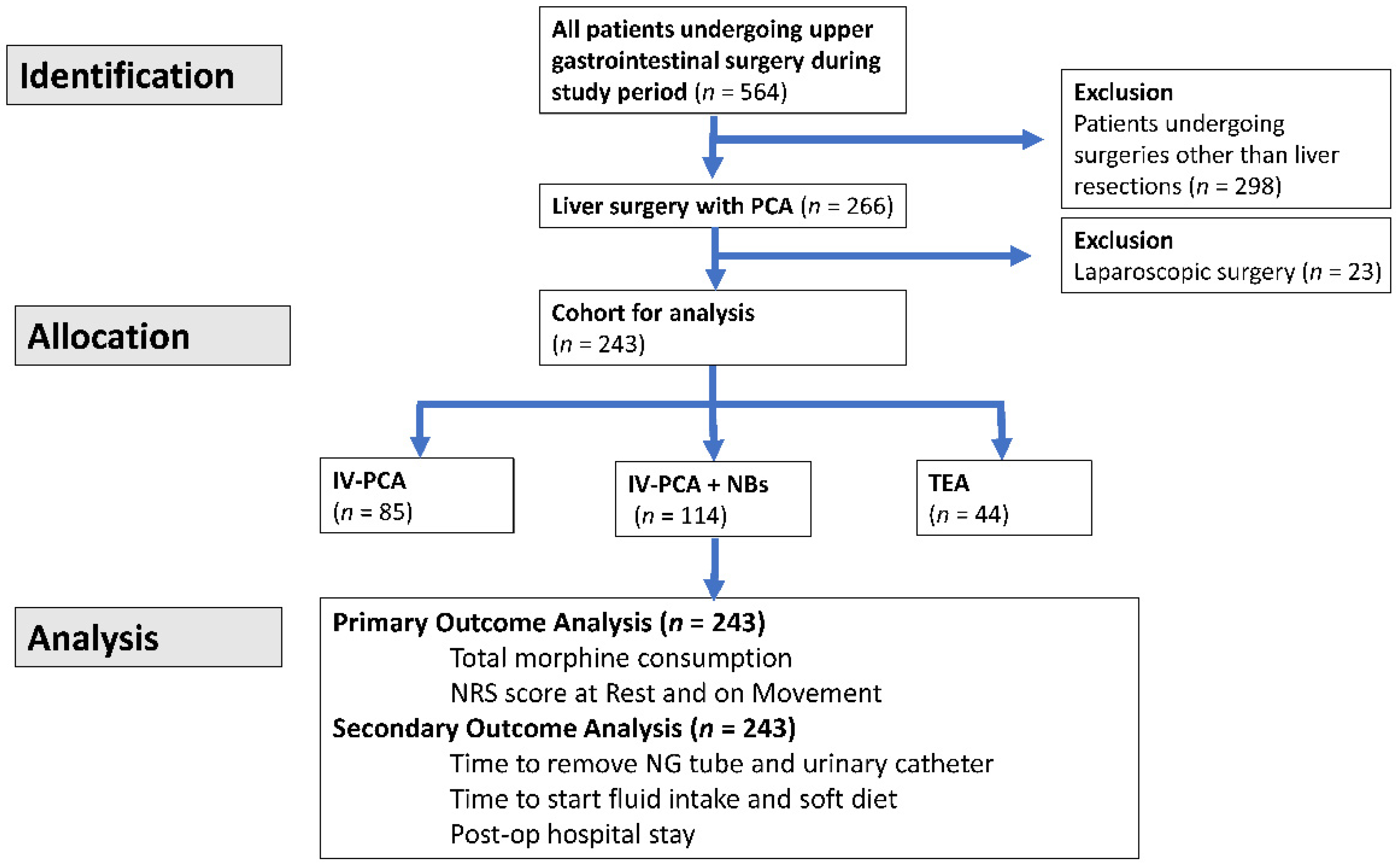
2.1. Data Source and Patient Population
2.2. Procedures of Anesthesia and Postoperative Analgesia
2.3. Statistics
3. Results
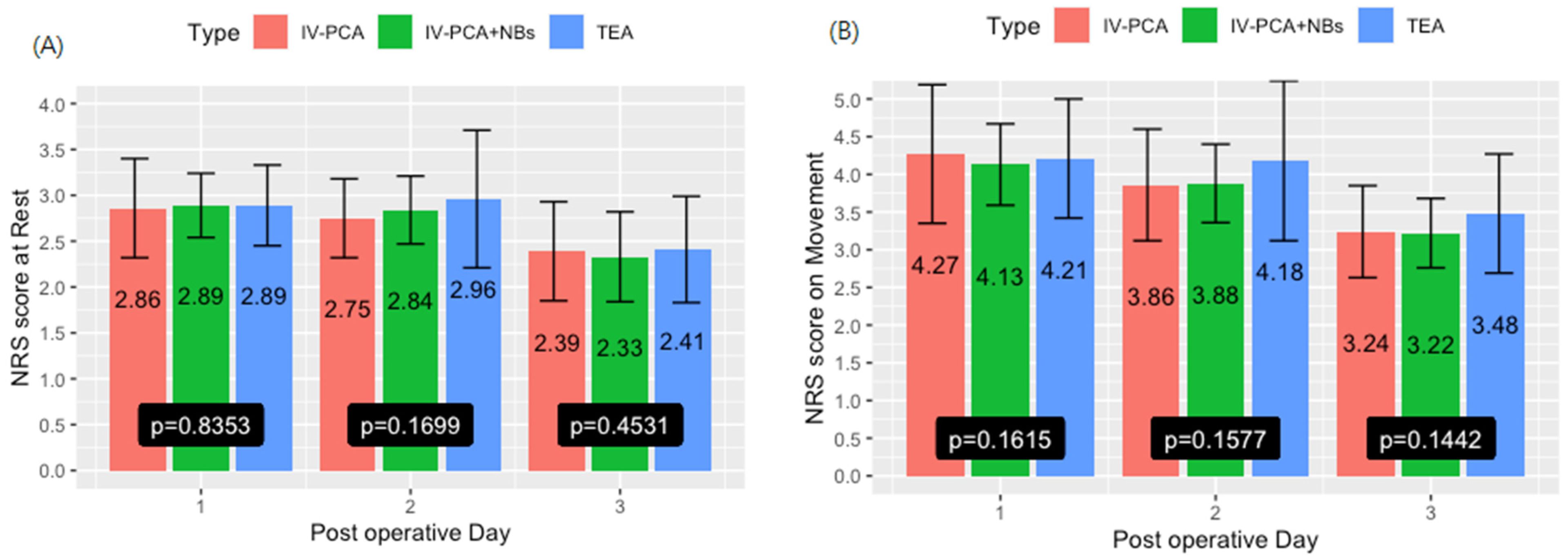
3.1. Primary Outcome
3.2. Secondary Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Pędziwiatr, M.; Mavrikis, J.; Witowski, J.; Adamos, A.; Major, P.; Nowakowski, M.; Budzyński, A. Current status of enhanced recovery after surgery (ERAS) protocol in gastrointestinal surgery. Med. Oncol. 2018, 35, 95. [Google Scholar] [CrossRef]
- Ljungqvist, O. ERAS—Enhanced recovery after surgery: Moving evidence-based perioperative care to practice. JPEN J. Parenter. Enter. Nutr. 2014, 38, 559–566. [Google Scholar] [CrossRef]
- Ljungqvist, O.; Scott, M.; Fearon, K.C. Enhanced Recovery After Surgery: A Review. JAMA Surg. 2017, 152, 292–298. [Google Scholar] [CrossRef]
- Pisarska, M.; Małczak, P.; Major, P.; Wysocki, M.; Budzyński, A.; Pędziwiatr, M. Enhanced recovery after surgery protocol in oesophageal cancer surgery: Systematic review and meta-analysis. PLoS ONE 2017, 12, e0174382. [Google Scholar] [CrossRef]
- Zhou, J.; Du, R.; Wang, L.; Wang, F.; Li, D.; Tong, G.; Wang, W.; Ding, X.; Wang, D. The Application of Enhanced Recovery After Surgery (ERAS) for Patients Undergoing Bariatric Surgery: A Systematic Review and Meta-analysis. Obes. Surg. 2021, 31, 1321–1331. [Google Scholar] [CrossRef]
- Jones, E.L.; Wainwright, T.W.; Foster, J.D.; Smith, J.R.; Middleton, R.G.; Francis, N.K. A systematic review of patient reported outcomes and patient experience in enhanced recovery after orthopaedic surgery. Ann. R. Coll. Surg. Engl. 2014, 96, 89–94. [Google Scholar] [CrossRef]
- de Groot, J.J.; Ament, S.M.; Maessen, J.M.; Dejong, C.H.; Kleijnen, J.M.; Slangen, B.F. Enhanced recovery pathways in abdominal gynecologic surgery: A systematic review and meta-analysis. Acta Obstet. Et Gynecol. Scand. 2016, 95, 382–395. [Google Scholar] [CrossRef]
- Song, W.; Wang, K.; Zhang, R.J.; Dai, Q.X.; Zou, S.B. The enhanced recovery after surgery (ERAS) program in liver surgery: A meta-analysis of randomized controlled trials. Springerplus 2016, 5, 207. [Google Scholar] [CrossRef]
- Ruffolo, L.I.; Nessen, M.F.; Probst, C.P.; Jackson, K.M.; Ruan, D.T.; Schoeniger, L.O.; Moalem, J. Open adrenalectomy through a makuuchi incision: A single institution’s experience. Surgery 2018, 164, 1372–1376. [Google Scholar] [CrossRef]
- Chang, S.B.; Palavecino, M.; Wray, C.J.; Kishi, Y.; Pisters, P.W.; Vauthey, J.N. Modified Makuuchi incision for foregut procedures. Arch. Surg. 2010, 145, 281–284. [Google Scholar] [CrossRef]
- Polat, F.; Atan, A.; Yeşil, S.; Dikmen, K.; Ünsal, A. Modified Makuuchi incision in the surgical treatment of renal tumors: Initial results. Turk. J. Urol. 2019, 45, 467–470. [Google Scholar] [CrossRef]
- Bokka, S.H.; Sreenivasan Kodakkattil, S.; Manikandan, R.; Lalgudi Narayanan, D.; M, H.; Kalra, S.; Biju, P. Usage of Modified Makuuchi Incision for Surgical Management of Complex Renal and Adrenal Lesions. Cureus 2020, 12, e11012. [Google Scholar] [CrossRef]
- Melloul, E.; Hübner, M.; Scott, M.; Snowden, C.; Prentis, J.; Dejong, C.H.; Garden, O.J.; Farges, O.; Kokudo, N.; Vauthey, J.N.; et al. Guidelines for Perioperative Care for Liver Surgery: Enhanced Recovery After Surgery (ERAS) Society Recommendations. World J. Surg. 2016, 40, 2425–2440. [Google Scholar] [CrossRef]
- Kim, B.J.; Soliz, J.M.; Aloia, T.A.; Vauthey, J.N. What Is the Best Pain Control After Major Hepatopancreatobiliary Surgery? Adv. Surg. 2018, 52, 235–246. [Google Scholar] [CrossRef]
- Li, J.; Pourrahmat, M.M.; Vasilyeva, E.; Kim, P.T.; Osborn, J.; Wiseman, S.M. Efficacy and Safety of Patient-controlled Analgesia Compared With Epidural Analgesia After Open Hepatic Resection: A Systematic Review and Meta-analysis. Ann. Surg. 2019, 270, 200–208. [Google Scholar] [CrossRef]
- Esteve, N.; Ferrer, A.; Sansaloni, C.; Mariscal, M.; Torres, M.; Mora, C. Epidural anesthesia and analgesia in liver resection: Safety and effectiveness. Rev. Española De Anestesiol. Reanim. 2017, 64, 86–94. [Google Scholar] [CrossRef]
- Allen, S.; DeRoche, A.; Adams, L.; Slocum, K.V.; Clark, C.J.; Fino, N.F.; Shen, P. Effect of epidural compared to patient-controlled intravenous analgesia on outcomes for patients undergoing liver resection for neoplastic disease. J. Surg. Oncol. 2017, 115, 402–406. [Google Scholar] [CrossRef]
- Aloia, T.A.; Kim, B.J.; Segraves-Chun, Y.S.; Cata, J.P.; Truty, M.J.; Shi, Q.; Holmes, A.; Soliz, J.M.; Popat, K.U.; Rahlfs, T.F.; et al. A Randomized Controlled Trial of Postoperative Thoracic Epidural Analgesia Versus Intravenous Patient-controlled Analgesia After Major Hepatopancreatobiliary Surgery. Ann. Surg. 2017, 266, 545–554. [Google Scholar] [CrossRef]
- Kambakamba, P.; Slankamenac, K.; Tschuor, C.; Kron, P.; Wirsching, A.; Maurer, K.; Petrowsky, H.; Clavien, P.A.; Lesurtel, M. Epidural analgesia and perioperative kidney function after major liver resection. Br. J. Surg. 2015, 102, 805–812. [Google Scholar] [CrossRef]
- Gavriilidis, P.; Roberts, K.J.; Sutcliffe, R.P. Local anaesthetic infiltration via wound catheter versus epidural analgesia in open hepatectomy: A systematic review and meta-analysis of randomised controlled trials. HPB 2019, 21, 945–952. [Google Scholar] [CrossRef]
- Bell, R.; Ward, D.; Jeffery, J.; Toogood, G.J.; Lodge, J.A.; Rao, K.; Lotia, S.; Hidalgo, E. A Randomized Controlled Trial Comparing Epidural Analgesia Versus Continuous Local Anesthetic Infiltration Via Abdominal Wound Catheter in Open Liver Resection. Ann. Surg. 2019, 269, 413–419. [Google Scholar] [CrossRef] [PubMed]
- Qiao, X.F.; Jia, W.D.; Li, Y.Q.; Lv, J.G.; Zhou, H. Effectiveness of Parecoxib Sodium Combined with Transversus Abdominis Plane Block for Pain Management After Hepatectomy for Hepatocellular Carcinoma: A Prospective Controlled Study. Med. Sci. Monit. 2019, 25, 1053–1060. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, V.; Divatia, J.V. Enhanced recovery after surgery in liver resection: Current concepts and controversies. Korean J. Anesthesiol. 2019, 72, 119–129. [Google Scholar] [CrossRef] [PubMed]
- Sakowska, M.; Docherty, E.; Linscott, D.; Connor, S. A change in practice from epidural to intrathecal morphine analgesia for hepato-pancreato-biliary surgery. World J. Surg. 2009, 33, 1802–1808. [Google Scholar] [CrossRef]
- Hausken, J.; Fretland, A.A.; Edwin, B.; Andersen, M.H.; Dagenborg, V.J.; Bjornelv, G.M.W.; Kristiansen, R.; Roysland, K.; Kvarstein, G.; Tonnessen, T.I. Intravenous Patient-controlled Analgesia Versus Thoracic Epidural Analgesia After Open Liver Surgery: A Prospective, Randomized, Controlled, Noninferiority Trial. Ann. Surg. 2019, 270, 193–199. [Google Scholar] [CrossRef]
- Golembiewski, J.; Dasta, J. Evolving Role of Local Anesthetics in Managing Postsurgical Analgesia. Clin. Ther. 2015, 37, 1354–1371. [Google Scholar] [CrossRef]
- Mallan, D.; Sharan, S.; Saxena, S.; Singh, T.K.; Faisal. Anesthetic techniques: Focus on transversus abdominis plane (TAP) blocks. Local Reg. Anesth. 2019, 12, 81–88. [Google Scholar] [CrossRef]
- Rudin, A.; Lundberg, J.F.; Hammarlund-Udenaes, M.; Flisberg, P.; Werner, M.U. Morphine metabolism after major liver surgery. Anesth. Analg. 2007, 104, 1409–1414. [Google Scholar] [CrossRef]
- Page, A.J.; Ejaz, A.; Spolverato, G.; Zavadsky, T.; Grant, M.C.; Galante, D.J.; Wick, E.C.; Weiss, M.; Makary, M.A.; Wu, C.L.; et al. Enhanced recovery after surgery protocols for open hepatectomy—physiology, immunomodulation, and implementation. J. Gastrointest. Surg. 2015, 19, 387–399. [Google Scholar] [CrossRef]
- Hernandez, M.C.; Panchamia, J.; Finnesgard, E.J.; Leiting, J.L.; Franssen, B.; Saleem, H.; Kendrick, M.L.; Nagorney, D.M.; Truty, M.J.; Smoot, R.L. Transversus abdominis plane blocks with liposomal bupivacaine after open major hepatectomy is associated with reduced early patient-reported pain scores and opioid administration. Surgery 2018, 164, 1251–1258. [Google Scholar] [CrossRef]
- Karanicolas, P.J.; Cleary, S.; McHardy, P.; Kiss, A.; Sawyer, J.; Behman, R.; Ladak, S.; McCluskey, S.A.; Srinivas, C.; Katz, J.; et al. Medial Open Transversus Abdominis Plane (MOTAP) Catheters Reduce Opioid Requirements and Improve Pain Control Following Open Liver Resection: A Multicenter, Blinded, Randomized Controlled Trial. Ann. Surg. 2018, 268, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Ayad, S.; Babazade, R.; Elsharkawy, H.; Nadar, V.; Lokhande, C.; Makarova, N.; Khanna, R.; Sessler, D.I.; Turan, A. Comparison of Transversus Abdominis Plane Infiltration with Liposomal Bupivacaine versus Continuous Epidural Analgesia versus Intravenous Opioid Analgesia. PLoS ONE 2016, 11, e0153675. [Google Scholar] [CrossRef]
- Nair, A.; Amula, V.E.; Naik, V.; Kodisharapu, P.K.; Poornachand, A.; Shyam Prasad, M.S.; Saifuddin, M.S.; Rayani, B.K. Comparison of Postoperative Analgesia in Patients Undergoing Ileostomy Closure with and Without Dual Transversus Abdominis Plane (TAP) Block: A Randomized Controlled Trial. Rambam Maimonides Med. J. 2019, 10, e0004. [Google Scholar] [CrossRef] [PubMed]
- Scherrer, V.; Compere, V.; Loisel, C.; Dureuil, B. Cardiac arrest from local anesthetic toxicity after a field block and transversus abdominis plane block: A consequence of miscommunication between the anesthesiologist and surgeon. A A Case Rep. 2013, 1, 75–76. [Google Scholar] [CrossRef] [PubMed]
- Brian, D. O’Donnell, M.; Stephen Mannion, M. A Case of Liver Trauma With a Blunt Regional Anesthesia Needle While Performing Transversus Abdominis Plane Block. Reg. Anesth. Pain Med. 2009, 34, 75. [Google Scholar]
- Lancaster, P.; Chadwick, M. Liver trauma secondary to ultrasound-guided transversus abdominis plane block. Br. J. Anaesth. 2010, 104, 509–510. [Google Scholar] [CrossRef]
- Manatakis, D.K.; Stamos, N.; Agalianos, C.; Karvelis, M.A.; Gkiaourakis, M.; Davides, D. Transient femoral nerve palsy complicating “blind” transversus abdominis plane block. Case Rep. Anesth. 2013, 2013, 874215. [Google Scholar] [CrossRef]
- Hsu, H.Y.; Yu, M.C.; Lee, C.W.; Tsai, H.I.; Sung, C.M.; Chen, C.W.; Huang, S.W.; Lin, C.Y.; Jeng, W.J.; Lee, W.C.; et al. RAM score is an effective predictor for early mortality and recurrence after hepatectomy for hepatocellular carcinoma. BMC Cancer 2017, 17, 742. [Google Scholar] [CrossRef]
- Lee, C.W.; Tsai, H.I.; Sung, C.M.; Chen, C.W.; Huang, S.W.; Jeng, W.J.; Wu, T.H.; Chan, K.M.; Yu, M.C.; Lee, W.C.; et al. Risk factors for early mortality after hepatectomy for hepatocellular carcinoma. Medicine 2016, 95, e5028. [Google Scholar] [CrossRef]
- Dolan, J.; Lucie, P.; Geary, T.; Smith, M.; Kenny, G.N. The rectus sheath block: Accuracy of local anesthetic placement by trainee anesthesiologists using loss of resistance or ultrasound guidance. Reg. Anesth. Pain Med. 2009, 34, 247–250. [Google Scholar] [CrossRef]
- Ganapathy, S.; Sondekoppam, R.V.; Terlecki, M.; Brookes, J.; Das Adhikary, S.; Subramanian, L. Comparison of efficacy and safety of lateral-to-medial continuous transversus abdominis plane block with thoracic epidural analgesia in patients undergoing abdominal surgery: A randomised, open-label feasibility study. Eur. J. Anaesthesiol. 2015, 32, 797–804. [Google Scholar] [CrossRef] [PubMed]
- Gnanasekar, N.; Kumar, G.D.; Kurhekar, P.; Raghuraman, M.S.; Prasad, T.K. Comparative Evaluation of Ropivacaine and Ropivacaine with Dexamethasone in Transverse Abdominis Plane Block for Lower Abdominal Surgeries: A Prospective, Randomized, Double-Blinded Study. Anesth. Essays Res. 2018, 12, 937–942. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.B.; Goldberg, G.R. Chapter 2—How Should Opioids Be Started and Titrated in Hospital or Inpatient Settings? In Evidence-Based Practice in Palliative Medicine; Goldstein, N.E., Morrison, R.S., Eds.; W.B. Saunders: Philadelphia, PA, USA, 2013; pp. 8–13. [Google Scholar]
- Haefeli, M.; Elfering, A. Pain assessment. Eur. Spine J. Off. Publ. Eur. Spine Soc. Eur. Spinal Deform. Soc. Eur. Sect. Cerv. Spine Res. Soc. 2006, 15 (Suppl. S1), S17–S24. [Google Scholar] [CrossRef]
- Williamson, A.; Hoggart, B. Pain: A review of three commonly used pain rating scales. J. Clin. Nurs. 2005, 14, 798–804. [Google Scholar] [CrossRef]
- Chung, K.C.; Barlev, A.; Braun, A.H.; Qian, Y.; Zagari, M. Assessing analgesic use in patients with advanced cancer: Development of a new scale—The Analgesic Quantification Algorithm. Pain Med. 2014, 15, 225–232. [Google Scholar] [CrossRef][Green Version]
- Shaheen, P.E.; Walsh, D.; Lasheen, W.; Davis, M.P.; Lagman, R.L. Opioid equianalgesic tables: Are they all equally dangerous? J. Pain Symptom Manag. 2009, 38, 409–417. [Google Scholar] [CrossRef]
- Qi, S.; Chen, G.; Cao, P.; Hu, J.; He, G.; Luo, J.; He, J.; Peng, X. Safety and efficacy of enhanced recovery after surgery (ERAS) programs in patients undergoing hepatectomy: A prospective randomized controlled trial. J. Clin. Lab. Anal. 2018, 32, e22434. [Google Scholar] [CrossRef] [PubMed]
- Gulur, P.; Tsui, B.; Pathak, R.; Koury, K.M.; Lee, H. Retrospective analysis of the incidence of epidural haematoma in patients with epidural catheters and abnormal coagulation parameters. Br. J. Anaesth. 2015, 114, 808–811. [Google Scholar] [CrossRef]
- Thangamuthu, A.; Russell, I.F.; Purva, M. Epidural failure rate using a standardised definition. Int. J. Obstet. Anesth. 2013, 22, 310–315. [Google Scholar] [CrossRef]
- Rawal, N. Epidural technique for postoperative pain: Gold standard no more? Reg. Anesth. Pain Med. 2012, 37, 310–317. [Google Scholar] [CrossRef]
- Fayed, N.A.; Abo El-Wafa, H.B.; Gab-Alla, N.M.; Yassen, K.A.; Lotfy, M.E. Comparison between intravenous patient controlled analgesia and patient controlled epidural analgesia in cirrhotic patients after hepatic resection. Middle East J. Anaesthesiol. 2014, 22, 467–476. [Google Scholar] [PubMed]
- Salicath, J.H.; Yeoh, E.C.; Bennett, M.H. Epidural analgesia versus patient-controlled intravenous analgesia for pain following intra-abdominal surgery in adults. Cochrane Database Syst. Rev. 2018, 8, Cd010434. [Google Scholar] [CrossRef] [PubMed]
- Viderman, D.; Tapinova, K.; Nabidollayeva, F.; Tankacheev, R.; Abdildin, Y.G. Intravenous versus Epidural Routes of Patient-Controlled Analgesia in Abdominal Surgery: Systematic Review with Meta-Analysis. J. Clin. Med. 2022, 11, 2579. [Google Scholar] [CrossRef] [PubMed]
- Mistry, K.; Hutchins, J.; Leiting, J.; Mangalick, K.; Pruett, T.; Chinnakotla, S. Continuous Paravertebral Infusions as an Effective Adjunct for Postoperative Pain Management in Living Liver Donors: A Retrospective Observational Study. Transplant. Proc. 2017, 49, 309–315. [Google Scholar] [CrossRef]
- Schreiber, K.L.; Chelly, J.E.; Lang, R.S.; Abuelkasem, E.; Geller, D.A.; Marsh, J.W.; Tsung, A.; Sakai, T. Epidural versus paravertebral nerve block for postoperative analgesia in patients undergoing open liver resection: A randomized clinical trial. Reg. Anesth. Pain Med. 2016, 41, 460. [Google Scholar] [CrossRef]
- De Pietri, L.; Siniscalchi, A.; Reggiani, A.; Masetti, M.; Begliomini, B.; Gazzi, M.; Gerunda, G.E.; Pasetto, A. The Use of Intrathecal Morphine for Postoperative Pain Relief After Liver Resection: A Comparison with Epidural Analgesia. Anesth. Analg. 2006, 102, 1157–1163. [Google Scholar] [CrossRef]
- Tang, J.; Churilov, L.; Tan, C.O.; Hu, R.; Pearce, B.; Cosic, L.; Christophi, C.; Weinberg, L. Intrathecal morphine is associated with reduction in postoperative opioid requirements and improvement in postoperative analgesia in patients undergoing open liver resection. BMC Anesthesiol. 2020, 20, 207. [Google Scholar] [CrossRef]
- Petersen, P.L.; Mathiesen, O.; Torup, H.; Dahl, J.B. The transversus abdominis plane block: A valuable option for postoperative analgesia? A topical review. Acta Anaesthesiol. Scand. 2010, 54, 529–535. [Google Scholar] [CrossRef]
- Tsai, H.C.; Yoshida, T.; Chuang, T.Y.; Yang, S.F.; Chang, C.C.; Yao, H.Y.; Tai, Y.T.; Lin, J.A.; Chen, K.Y. Transversus Abdominis Plane Block: An Updated Review of Anatomy and Techniques. Biomed Res. Int. 2017, 2017, 8284363. [Google Scholar] [CrossRef]
- Charlton, S.; Cyna, A.M.; Middleton, P.; Griffiths, J.D. Perioperative transversus abdominis plane (TAP) blocks for analgesia after abdominal surgery. Cochrane Database Syst. Rev. 2010, CD007705. [Google Scholar] [CrossRef]
- Dudek, P.; Zawadka, M.; Andruszkiewicz, P.; Gelo, R.; Pugliese, F.; Bilotta, F. Postoperative Analgesia after Open Liver Surgery: Systematic Review of Clinical Evidence. J. Clin. Med. 2021, 10, 3662. [Google Scholar] [CrossRef] [PubMed]
- Wong-Lun-Hing, E.M.; van Dam, R.M.; Welsh, F.K.; Wells, J.K.; John, T.G.; Cresswell, A.B.; Dejong, C.H.; Rees, M. Postoperative pain control using continuous i.m. bupivacaine infusion plus patient-controlled analgesia compared with epidural analgesia after major hepatectomy. HPB 2014, 16, 601–609. [Google Scholar] [CrossRef] [PubMed]
- Ayad, S.; Babazade, R.; Elsharkawy, H.; Nadar, V.; Lokhande, C.; Makarova, N.; Khanna, R.; Sessler, D.I.; Turan, A. Correction: Comparison of Transversus Abdominis Plane Infiltration with Liposomal Bupivacaine versus Continuous Epidural Analgesia versus Intravenous Opioid Analgesia. PLoS ONE 2016, 11, e0163687. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Total | IV-PCA (n = 85) | IV-PCA + NBs (n = 114) | TEA (n = 44) | p-Value | ||||
|---|---|---|---|---|---|---|---|---|---|
| No. | (%) | No. | (%) | No. | (%) | No. | (%) | ||
| Male gender | 167 | 68.7% | 57 | 67.1% | 78 | 68.4% | 32 | 72.7% | 0.802 |
| Comorbidity | |||||||||
| Diabetes | 66 | 27.2% | 28 | 32.9% | 25 | 21.9% | 13 | 29.5% | 0.208 |
| Hypertension | 105 | 43.2% | 39 | 45.9% | 51 | 44.7% | 15 | 34.1% | 0.397 |
| ESRD | 5 | 2.1% | 1 | 1.2% | 4 | 3.5% | 0 | 0.0% | 0.295 |
| CAD | 10 | 4.1% | 3 | 3.5% | 6 | 5.3% | 1 | 2.3% | 0.659 |
| CVA | 7 | 2.9% | 4 | 4.7% | 3 | 2.6% | 0 | 0.0% | 0.310 |
| Cancer history | 44 | 18.1% | 11 | 12.9% | 27 | 23.7% | 6 | 13.6% | 0.105 |
| HBV infection | 123 | 50.6% | 39 | 45.9% | 58 | 50.9% | 26 | 59.1% | 0.363 |
| HCV infection | 36 | 14.8% | 17 | 20.0% | 18 | 15.8% | 1 | 2.3% | 0.025 |
| Cigarette smoking | 101 | 41.6% | 33 | 38.8% | 52 | 45.6% | 16 | 36.4% | 0.467 |
| Alcohol consumption | 79 | 32.5% | 29 | 34.1% | 38 | 33.3% | 12 | 27.3% | 0.71 |
| Previous surgery | 41 | 16.9% | 17 | 20.0% | 15 | 13.2% | 9 | 20.5% | 0.347 |
| Mean±SD | Mean±SD | Mean±SD | Mean±SD | p-Value | |||||
| Age (years) | 60.90 ± 11.07 | 62.34 ± 11.64 | 60.85 ± 10.75 | 58.25 ± 10.48 | 0.138 | ||||
| Weight (kg) | 66.77 ± 11.99 | 66.22 ± 12.91 | 66.63 ± 10.89 | 68.20 ± 13.01 | 0.665 | ||||
| ICG-15 (%) | 10.09 ± 7.27 | 10.66 ± 7.54 | 10.44 ± 7.62 | 7.86 ± 5.10 | 0.151 | ||||
| Hemoglobin (g/dL) | 13.5 ± 1.81 | 13.67 ± 1.64 | 13.18 ± 1.96 | 14 ± 1.56 | 0.0209 | ||||
| Albumin (g/dL) | 4.22 ± 0.41 | 4.14 ± 0.36 | 4.19 ± 0.44 | 4.44 ± 0.35 | <0.001 | ||||
| Platelet (1000/uL) | 194.07 ± 76.29 | 184.84 ± 73.96 | 202.82 ± 85.34 | 189.23 ± 50.33 | 0.233 | ||||
| ALT (U/L) | 46.41 ± 49.47 | 48.73 ± 47.56 | 45.89 ± 55.04 | 43.27 ± 37.01 | 0.83 | ||||
| Alkaline Phosphatase (U/L) | 90.42 ± 55.43 | 90.75 ± 42.82 | 95.16 ± 68.23 | 77.73 ± 35.62 | 0.21 | ||||
| Total Bilirubin (mg/dL) | 0.74 ± 1.31 | 0.65 ± 0.24 | 0.85 ± 1.9 | 0.62 ± 0.25 | 0.454 | ||||
| α-fetoprotein (ng/mL) | 3244.34 ± 19057.55 | 5958.48 ± 27930.21 | 2097.30 ± 13786.73 | 1034.08 ± 2917.73 | 0.28 | ||||
| Variables | Total | IV-PCA (n = 85) | IV-PCA + NBs (n = 114) | TEA (n = 44) | p-Value | ||||
|---|---|---|---|---|---|---|---|---|---|
| No. | (%) | No. | (%) | No. | (%) | No. | (%) | ||
| Intra-Abdominal Adhesion | 39 | 16.0% | 16 | 18.8% | 15 | 13.2% | 8 | 18.2% | 0.511 |
| Major Resections | 107 | 44% | 36 | 42% | 58 | 51% | 13 | 30% | 0.0495 |
| Intraoperative Blood Transfusion | 116 | 48% | 46 | 54% | 55 | 48% | 15 | 34% | 0.096 |
| Diagnosis | 0.316 | ||||||||
| HCC | 164 | 67.49% | 61 | 71.76% | 76 | 66.67% | 27 | 61.36% | |
| CCC | 27 | 11.11% | 8 | 9.41% | 12 | 10.53% | 7 | 15.91% | |
| Metastatic liver tumor | 23 | 9.47% | 9 | 10.59% | 12 | 10.53% | 2 | 4.55% | |
| Benign disease | 26 | 10.70% | 7 | 8.24% | 11 | 9.65% | 8 | 18.18% | |
| Sarcoma | 3 | 1.23% | 0 | 0.00% | 3 | 2.63% | 0 | 0.00% | |
| Mean±SD | Mean±SD | Mean±SD | Mean±SD | p-Value | |||||
| Operative Time (min) | 314.42 ± 105.69 | 315.51 ± 106.08 | 317.73 ± 102.23 | 303.77 ± 115.21 | 0.755 | ||||
| Intraoperative Fluid Transfusion (mL) | 1537.62 ± 789.97 | 1641.06 ± 814.93 | 1457.46 ± 800.53 | 1545.45 ± 701.72 | 0.269 | ||||
| Intraoperative Urine Output (mL/h/kilograms) | 1.16 ± 0.77 | 1.24 ± 0.79 | 1.09 ± 0.71 | 1.21 ± 0.89 | 0.3612 | ||||
| Intraoperative Blood Loss (mL) | 512.88 ± 614.69 | 604.82 ± 719.57 | 450.44 ± 532.21 | 497.05 ± 585.95 | 0.212 | ||||
| Variables | Total | IV-PCA (n = 85) | IV-PCA + NBs (n = 114) | TEA (n = 44) | p-Value | |||
|---|---|---|---|---|---|---|---|---|
| Mean ± SD | IV-PCA vs. IV-PCA + NBs | IV-PCA vs. TEA | IV-PCA + NBs vs. TEA | |||||
| Total Morphine consumption (mg) | 60.99 ± 44.75 | 83.53 ± 49.51 | 64.17 ± 31.96 | 9.21 ± 4.91 | <0.001 | 0.0008 | <0.001 | <0.001 |
| Total Morphine use/weight (mg/kg) | 0.92 ± 0.64 | 1.26 ± 0.67 | 0.96 ± 0.46 | 0.14 ± 0.07 | <0.0001 | 0.0002 | <0.0001 | <0.0001 |
| Day 1 rest NRS | 2.88 ± 0.44 | 2.86 ± 0.54 | 2.89 ± 0.35 | 2.89 ± 0.44 | 0.8353 | 0.8753 | 0.9020 | 0.9968 |
| Day 2 rest NRS | 2.83 ± 0.48 | 2.75 ± 0.43 | 2.84 ± 0.37 | 2.96 ± 0.75 | 0.1699 | 0.3298 | 0.0780 | 0.4637 |
| Day 3 rest NRS | 2.36 ± 0.52 | 2.39 ± 0.54 | 2.33 ± 0.49 | 2.41 ± 0.58 | 0.4531 | 0.6222 | 0.9537 | 0.5628 |
| Day 1 move NRS | 4.19 ± 0.74 | 4.27 ± 0.92 | 4.13 ± 0.54 | 4.21 ± 0.79 | 0.1615 | 0.3790 | 0.7138 | 0.9775 |
| Day 2 move NRS | 3.93 ± 0.73 | 3.86 ± 0.74 | 3.88 ± 0.52 | 4.18 ± 1.06 | 0.1577 | 0.9928 | 0.1179 | 0.1152 |
| Day 3 move NRS | 3.27 ± 0.59 | 3.24 ± 0.61 | 3.22 ± 0.46 | 3.48 ± 0.79 | 0.1442 | 0.9402 | 0.1145 | 0.0502 |
| Variables | Total | IV-PCA (n = 85) | IV-PCA + NBs (n = 114) | TEA (n = 44) | p-Value | |||
|---|---|---|---|---|---|---|---|---|
| Mean ± SD | IV-PCA vs. IV-PCA + NBs | IV-PCA vs. TEA | IV-PCA + NBs vs. TEA | |||||
| NG tube removal (days) | 1.32 ± 0.92 | 1.3 5 ± 1.09 | 1.29 ± 0.86 | 1.29 ± 0.7 | 0.9430 | 0.9033 | 0.9825 | 0.9888 |
| Urinary catheter removal (days) | 4.21 ± 3.21 | 4.93 ± 5.08 | 3.87 ± 1.31 | 3.70 ± 1.30 | 0.0414 | 0.0461 | 0.2281 | 0.9931 |
| Start on sip of water (days) | 1.42 ± 0.96 | 1.51 ± 1.2 | 1.38 ± 0.86 | 1.36 ± 0.68 | 0.1933 | 0.5913 | 0.7635 | 0.9998 |
| Start on soft diet (days) | 2.81 ± 1.98 | 2.85 ± 1.96 | 2.85 ± 2.18 | 2.66 ± 1.42 | 0.1130 | 0.9998 | 0.9998 | 0.8497 |
| Postoperative hospital stay(days) | 11.79 ± 6.16 | 12.71 ± 7.26 | 11.79 ± 5.71 | 10.02 ± 4.52 | <.0001 | 0.5602 | 0.5724 | 0.9613 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, H.-I.; Lu, Y.-C.; Zheng, C.-W.; Yu, M.-C.; Chou, A.-H.; Lee, C.-H.; Kou, H.-W.; Lin, J.-R.; Lai, Y.-H.; Chang, L.-L.; et al. A Retrospective Comparison of Three Patient-Controlled Analgesic Strategies: Intravenous Opioid Analgesia Plus Abdominal Wall Nerve Blocks versus Epidural Analgesia versus Intravenous Opioid Analgesia Alone in Open Liver Surgery. Biomedicines 2022, 10, 2411. https://doi.org/10.3390/biomedicines10102411
Tsai H-I, Lu Y-C, Zheng C-W, Yu M-C, Chou A-H, Lee C-H, Kou H-W, Lin J-R, Lai Y-H, Chang L-L, et al. A Retrospective Comparison of Three Patient-Controlled Analgesic Strategies: Intravenous Opioid Analgesia Plus Abdominal Wall Nerve Blocks versus Epidural Analgesia versus Intravenous Opioid Analgesia Alone in Open Liver Surgery. Biomedicines. 2022; 10(10):2411. https://doi.org/10.3390/biomedicines10102411
Chicago/Turabian StyleTsai, Hsin-I, Yu-Chieh Lu, Chih-Wen Zheng, Ming-Chin Yu, An-Hsun Chou, Cheng-Han Lee, Hao-Wei Kou, Jr-Rung Lin, Yu-Hua Lai, Li-Ling Chang, and et al. 2022. "A Retrospective Comparison of Three Patient-Controlled Analgesic Strategies: Intravenous Opioid Analgesia Plus Abdominal Wall Nerve Blocks versus Epidural Analgesia versus Intravenous Opioid Analgesia Alone in Open Liver Surgery" Biomedicines 10, no. 10: 2411. https://doi.org/10.3390/biomedicines10102411
APA StyleTsai, H.-I., Lu, Y.-C., Zheng, C.-W., Yu, M.-C., Chou, A.-H., Lee, C.-H., Kou, H.-W., Lin, J.-R., Lai, Y.-H., Chang, L.-L., & Lee, C.-W. (2022). A Retrospective Comparison of Three Patient-Controlled Analgesic Strategies: Intravenous Opioid Analgesia Plus Abdominal Wall Nerve Blocks versus Epidural Analgesia versus Intravenous Opioid Analgesia Alone in Open Liver Surgery. Biomedicines, 10(10), 2411. https://doi.org/10.3390/biomedicines10102411