
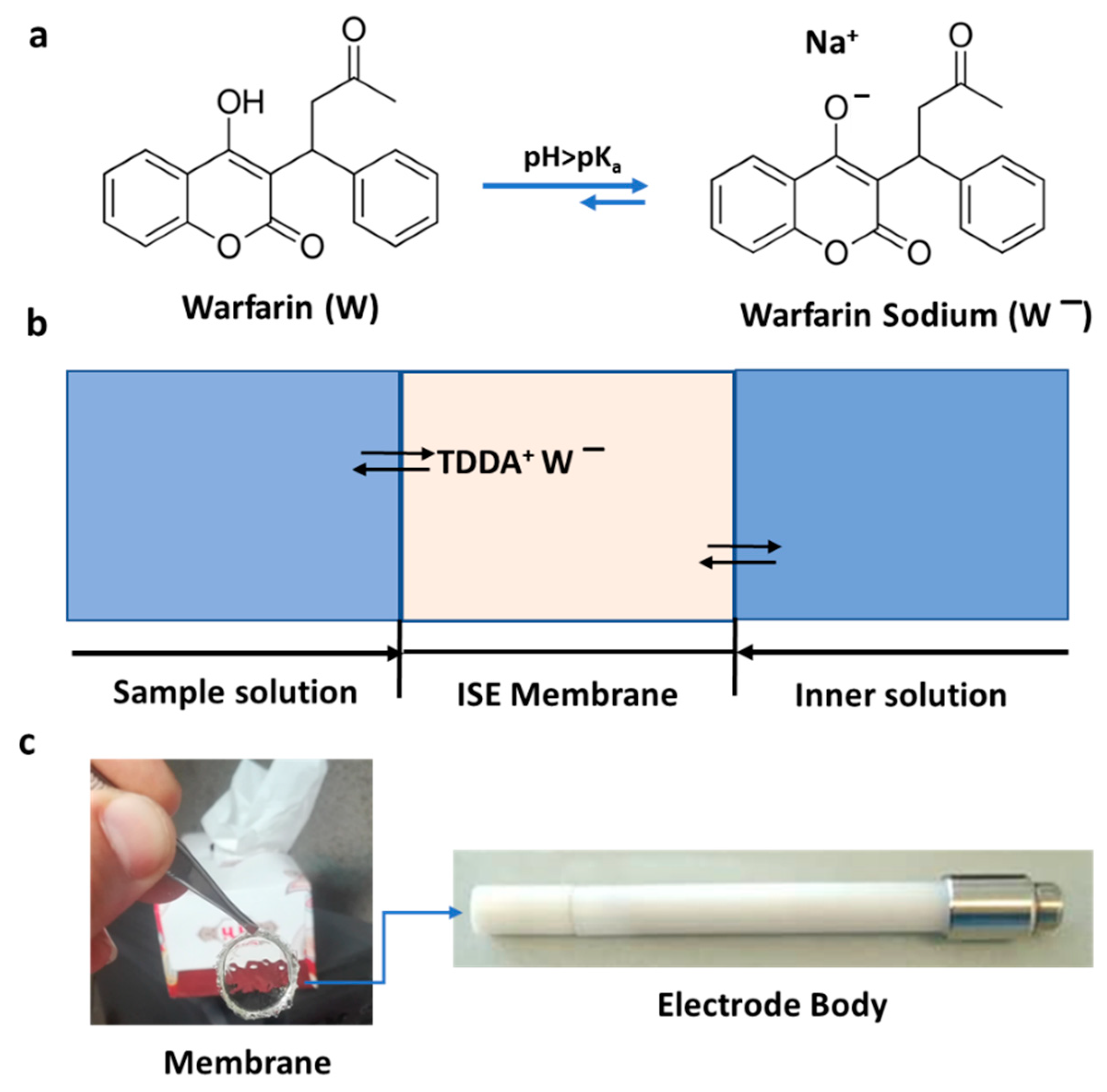
Electrochemical Sensor for the Direct Determination of Warfarin in Blood





Abstract
:1. Introduction
2. Materials and Methods
2.1. Reagents
2.2. Instrumentation
2.3. Preparation of PVC Membrane
3. Results and Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kaur, N.; Pandey, A.; Shafiq, N.; Gupta, A.; Das, R.; Singh, H.; Ahluwalia, J.; Malhotra, S. Genetic and Nongenetic Determinants of Variable Warfarin Dose Requirements: A Report from North India. Public Health Genom. 2022, 25, 52–60. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. International Drug Monitoring: The Role of the Hospital, Report of a WHO Meeting [Held in Geneva from 18 to 23 November 1968]; World Health Organization: Geneva, Switzerland, 1969; Available online: https://apps.who.int/iris/handle/10665/40747 (accessed on 7 December 2021).
- Adumitrăchioaie, A.; Tertiș, M.; Cernat, A.; Săndulescu, R.; Cristea, C. Electrochemical methods based on molecularly imprinted polymers for drug detection. Int. J. Electrochem. Sci. 2018, 13, 2556–2576. [Google Scholar] [CrossRef]
- Li, W.; Luo, W.; Li, M.; Chen, L.; Chen, L.; Guan, H.; Yu, M. The impact of recent developments in electrochemical POC sensor for blood sugar care: A mini review. Front. Chem. 2021, 9, 723186. [Google Scholar] [CrossRef] [PubMed]
- Sugarman, D.T. Patient Page, Blood Thinners. JAMA 2013, 310, 2579. [Google Scholar] [CrossRef] [Green Version]
- Chen, A.; Stecker, E.; Warden, B.A. Direct oral anticoagulant use: A practical guide to common clinical challenges. J. Am. Heart Assoc. 2020, 9, e017559. [Google Scholar] [CrossRef]
- Vats, A. Estimation of Warfarin Dosage with reinforcement learning. arXiv Prepr. 2021, arXiv:2109.07564. [Google Scholar]
- Kamuren, Z.; Kigen, G.; Keter, A.; Maritim, A. Characteristics of patients with thromboembolic disorders on warfarin therapy in resource limited settings. BMC Health Serv. Res. 2018, 18, 723. [Google Scholar] [CrossRef]
- Kimura, R.; Miyashita, K.; Kokubo, Y.; Akaiwa, Y.; Otsubo, R.; Nagatsuka, K.; Otsuki, T.; Okayama, A.; Minematsu, K.; Naritomi, H.; et al. Genotypes of vitamin K epoxide reductase, γ-glutamyl carboxylase, and cytochrome P450 2C9 as determinants of daily warfarin dose in Japanese patients. Thromb. Res. 2007, 120, 181. [Google Scholar] [CrossRef]
- Huang, Q.; Cao, L.; Luo, N.; Qian, H.; Wei, M.; Xue, L.; Zhou, Q.; Zou, B.; Tan, L.; Chu, Y.; et al. Predicting Range of Initial Warfarin Dose Based on Pharmacometabolomic and Genetic Inputs. Clin. Pharmacol. Ther. 2021, 110, 1585. [Google Scholar] [CrossRef]
- Ng, S.S.; Lai, N.M.; Nathisuwan, S.; Jahan, N.K.; Dilokthornsakul, P.; Kongpakwattana, K.; Hollingworth, W.; Chaiyakunapruk, N. Comparative efficacy and safety of warfarin care bundles and novel oral anticoagulants in patients with atrial fibrillation: A systematic review and network meta-analysis. Sci. Rep. 2020, 10, 662. [Google Scholar] [CrossRef] [Green Version]
- Connolly, S.J.; Pogue, J.; Eikelboom, J.; Flaker, G.; Commerford, P.; Franzosi, M.G.; Healey, J.S.; Yusuf, S. Benefit of oral anticoagulant over antiplatelet therapy in atrial fibrillation depends on the quality of international normalized ratio control achieved by centers and countries as measured by time in therapeutic range. Circulation 2008, 118, 2029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, R.H.; McKittrick, V.; Hutchinson, R.; Twitchell, J. Temporary discontinuation of warfarin therapy: Changes in the international normalized ratio. Ann. Intern. Med. 1995, 122, 40. [Google Scholar] [CrossRef] [PubMed]
- Gage, B.; Eby, C.; Johnson, J.; Deych, E.; Rieder, M.; Ridker, P.; Milligan, P.; Grice, G.; Lenzini, P.; Rettie, A. Use of pharmacogenetic and clinical factors to predict the therapeutic dose of warfarin. Clin. Pharmacol. Ther. 2008, 84, 326. [Google Scholar] [CrossRef] [PubMed]
- Ghimenti, S.; Lomonaco, T.; Biagini, D.; Bellagambi, F.G.; Onor, M.; Trivella, M.G.; Ruocco, L.; Pellegrini, G.; Di Francesco, F.; Fuoco, R. Determination of warfarin and warfarin alcohols in dried blood spots by ultra-high performance liquid chromatography coupled to electrospray ionization-tandem mass spectrometry (UHPLC-ESI-MS/MS). Microchem. J. 2018, 136, 247. [Google Scholar] [CrossRef]
- Nooraee Nia, N.; Hadjmohammadi, M.R. Nanofluid of magnetic-activated charcoal and hydrophobic deep eutectic solvent: Application in dispersive magnetic solid-phase extraction for the determination and preconcentration of warfarin in biological samples by high-performance liquid chromatography. Biomed. Chromatogr. 2021, 35, e5113. [Google Scholar] [CrossRef] [PubMed]
- Pan, T.-Y.; Tsai, W.-C.; Tan, C.-H.; Cheng, C.-M.; Chen, W.; Soundappan, T.; Arasu, M.V.; Al-Dhabi, N.A.; Wu, C.-F.; Ponnusamy, V.K. Rapid simultaneous clinical monitoring of five oral anti-coagulant drugs in human urine using green microextraction technique coupled with LC–MS/MS. J. King Saudi Univ. Sci. 2021, 33, 101602. [Google Scholar] [CrossRef]
- Nowak, P.; Olechowska, P.; Mitoraj, M.; Woźniakiewicz, M.; Kościelniak, P. Determination of acid dissociation constants of warfarin and hydroxywarfarins by capillary electrophoresis. J. Pharm. Biomed. Anal. 2015, 112, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Tzanavaras, P.D.; Themelis, D.G. Review of recent applications of flow injection spectrophotometry to pharmaceutical analysis. Anal. Chim. Acta 2007, 588, 1–9. [Google Scholar] [CrossRef]
- Sultan, M.A.; Abou El-Alamin, M.M.; Wark, A.W.; Azab, M.M. Detection and quantification of warfarin in pharmaceutical dosage form and in spiked human plasma using surface enhanced Raman scattering. Spectrochim. Acta Part A Mol. Biomol. Spectrosc. 2020, 228, 117533. [Google Scholar] [CrossRef]
- Gouda, A.A.; El-Sayed, M.I.K.; Amin, A.S.; El Sheikh, R. Spectrophotometric and spectrofluorometric methods for the determination of non-steroidal anti-inflammatory drugs: A review. Arab. J. Chem. 2013, 6, 145. [Google Scholar] [CrossRef] [Green Version]
- Bertucci, C.; Cimitan, S. Rapid screening of small ligand affinity to human serum albumin by an optical biosensor. J. Pharm. Med. Anal. 2003, 32, 707. [Google Scholar] [CrossRef]
- Fitzpatrick, B.; O’Kennedy, R.J. The development and application of a surface plasmon resonance-based inhibition immunoassay for the determination of warfarin in plasma ultrafiltrate. J. Immunol. Methods 2004, 19, 11. [Google Scholar] [CrossRef] [PubMed]
- Yawari, I.; Kaykhaii, M. Determination of (S)-warfarin using an activated screen-printed gold electrode modified with gold nanoparticles and an enantioselective molecularly imprinted polymer. Anal. Methods 2017, 9, 6583. [Google Scholar] [CrossRef]
- Gholivand, M.B.; Torkashvand, M. Electrooxidation behavior of warfarin in Fe3O4 nanoparticles modified carbon paste electrode and its determination in real samples. Mater. Sci. Eng. C 2015, 48, 235–242. [Google Scholar] [CrossRef]
- Hassan, S.S.; Mahmoud, W.H.; Elmosallamy, M.A.; Almarzooqi, M.H. Iron (II)-phthalocyanine as a novel recognition sensor for selective potentiometric determination of diclofenac and warfarin drugs. J. Pharm. Biomed. Anal. 2005, 39, 315. [Google Scholar] [CrossRef]
- Edelbroek, P.M.; van der Heijden, J.; Stolk, L.M. Dried blood spot methods in therapeutic drug monitoring: Methods, assays, and pitfalls. Ther. Drug Monit. 2009, 31, 327. [Google Scholar] [CrossRef]
- Shayesteh, O.H.; Mahjub, R.; Ranjbar, A.; Derankhshandeh, K.; Jamshidi, M. Nano optical and electrochemical sensors and biosensors for detection narrow therapeutic index drugs. Microchim. Acta 2021, 188, 411. [Google Scholar] [CrossRef]
- Hassan, S.S.; Mahmoud, W.H.; Abdel-Samad, M.S. Direct potentiometry and potentiotitrimetry of warfarin and ibuprofen in pharmaceutical preparations using PVC ferroin-based membrane sensors. Microchim. Acta 1998, 129, 251. [Google Scholar] [CrossRef]
- Gholivand, M.R.; Mohamadi-Behzad, L. An electrochemical sensor for warfarin based on covalent immobilization of quantum dots onto carboxylated multiwalled carbon nanotubes and chitosan-modified electrodes. Mat. Sci. Eng. 2015, 57, 77. [Google Scholar] [CrossRef]
- Dimitrokalli, E.; Fertaki, S.; Lykouras, M.; Kokkinos, P.; Orkoula, M.; Kontoyannis, C. Warfarin Sodium Stability in Oral Formulations. Molecules 2021, 26, 6631. [Google Scholar] [CrossRef]
- Hylek, E.M.; Regan, S.; Go, A.S.; Hughes, R.A.; Singer, D.E.; Skates, S.J. Clinical predictors of prolonged delay in return of the international normalized ratio to within the therapeutic range after excessive anticoagulation with warfarin. Ann. Intern. Med. 2001, 135, 393. [Google Scholar] [CrossRef] [PubMed]
- D’Andrea, G.; D’Ambrosio, R.L.; Di Perna, P.; Chetta, M.; Santacroce, R.; Brancaccio, V.; Grandone, E.; Margaglione, M. A polymorphism in the VKORC1 gene is associated with an interindividual variability in the dose-anticoagulant effect of warfarin. Blood 2005, 105, 645. [Google Scholar] [CrossRef] [PubMed]
- Gage, B.F.; Lesko, L.J. Pharmacogenetics of warfarin: Regulatory, scientific, and clinical issues. J. Thromb. Thrombolysis 2008, 25, 45. [Google Scholar] [CrossRef] [PubMed]
- Consortium, I.W.P. Estimation of the warfarin dose with clinical and pharmacogenetic data. N. Engl. J. Med. 2009, 360, 753. [Google Scholar]
- Johnson, J.A.; Gong, L.; Whirl-Carrillo, M.; Gage, B.F.; Scott, S.A.; Stein, C.; Anderson, J.; Kimmel, S.E.; Lee, M.T.M.; Pirmohamed, M. Clinical Pharmacogenetics Implementation Consortium Guidelines for CYP2C9 and VKORC1 genotypes and warfarin dosing. Clin. Pharmacol. Ther. 2011, 90, 625. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| M1 | M2 | M3 | M4 | M5 | M6 | M7 | M8 | |
|---|---|---|---|---|---|---|---|---|
| TDDA (mmol/kg) | 1 | 2 | 5 | 10 | 25 | 50 | 75 | 100 |
| Slope (mV) | −54.2 | −56.3 | −58.8 | −57.9 | −58.2 | −58.4 | −58.9 | −59.1 |
| LOD (logax−) | −7.2 | −7 | −6.9 | −6.5 | −6.4 | −5.8 | −5.3 | −4.9 |
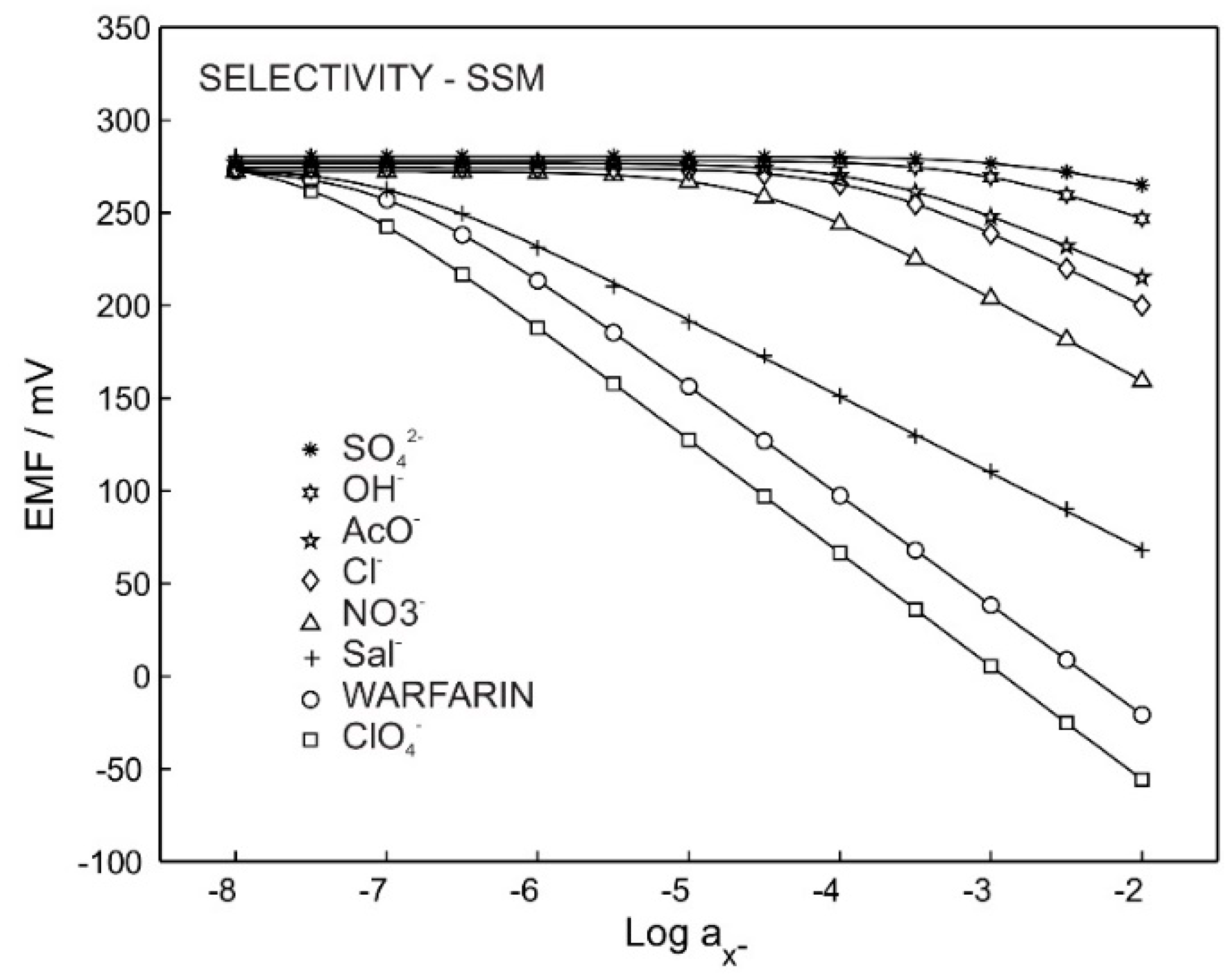
| SO42− | OH− | AcO− | Cl− | NO3− | Sal− | ClO4− | Warfarin | |
|---|---|---|---|---|---|---|---|---|
| Slope (mV/dec) | −18.4 | −30.1 | −35.2 | −41.1 | −45.4 | −60.2 | −61.3 | −59.1 |
| Intercept | 230.2 | 188.1 | 145.3 | 118.5 | 69.7 | −35.3 | −178.2 | −139.1 |
| LOD | −2.8 | −3.0 | −3.7 | −3.8 | −4.5 | −6.2 | −7.4 | −6.9 |
| Log Kijpot. | −6.2 | −5.5 | −4.8 | −4.1 | −3.5 | −1.9 | 0.6 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saeedi, I.; Ahmadi, S.; Thompson, M.; Hashemi, P.; Ramezani, Z. Electrochemical Sensor for the Direct Determination of Warfarin in Blood. Chemosensors 2022, 10, 44. https://doi.org/10.3390/chemosensors10020044
Saeedi I, Ahmadi S, Thompson M, Hashemi P, Ramezani Z. Electrochemical Sensor for the Direct Determination of Warfarin in Blood. Chemosensors. 2022; 10(2):44. https://doi.org/10.3390/chemosensors10020044
Chicago/Turabian StyleSaeedi, Iman, Soha Ahmadi, Michael Thompson, Payman Hashemi, and Zahra Ramezani. 2022. "Electrochemical Sensor for the Direct Determination of Warfarin in Blood" Chemosensors 10, no. 2: 44. https://doi.org/10.3390/chemosensors10020044
APA StyleSaeedi, I., Ahmadi, S., Thompson, M., Hashemi, P., & Ramezani, Z. (2022). Electrochemical Sensor for the Direct Determination of Warfarin in Blood. Chemosensors, 10(2), 44. https://doi.org/10.3390/chemosensors10020044