
Treatment Pattern of Antithrombotic Therapy over Time after Percutaneous Coronary Intervention in Patients with Atrial Fibrillation in Real-World Practice in Korea

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
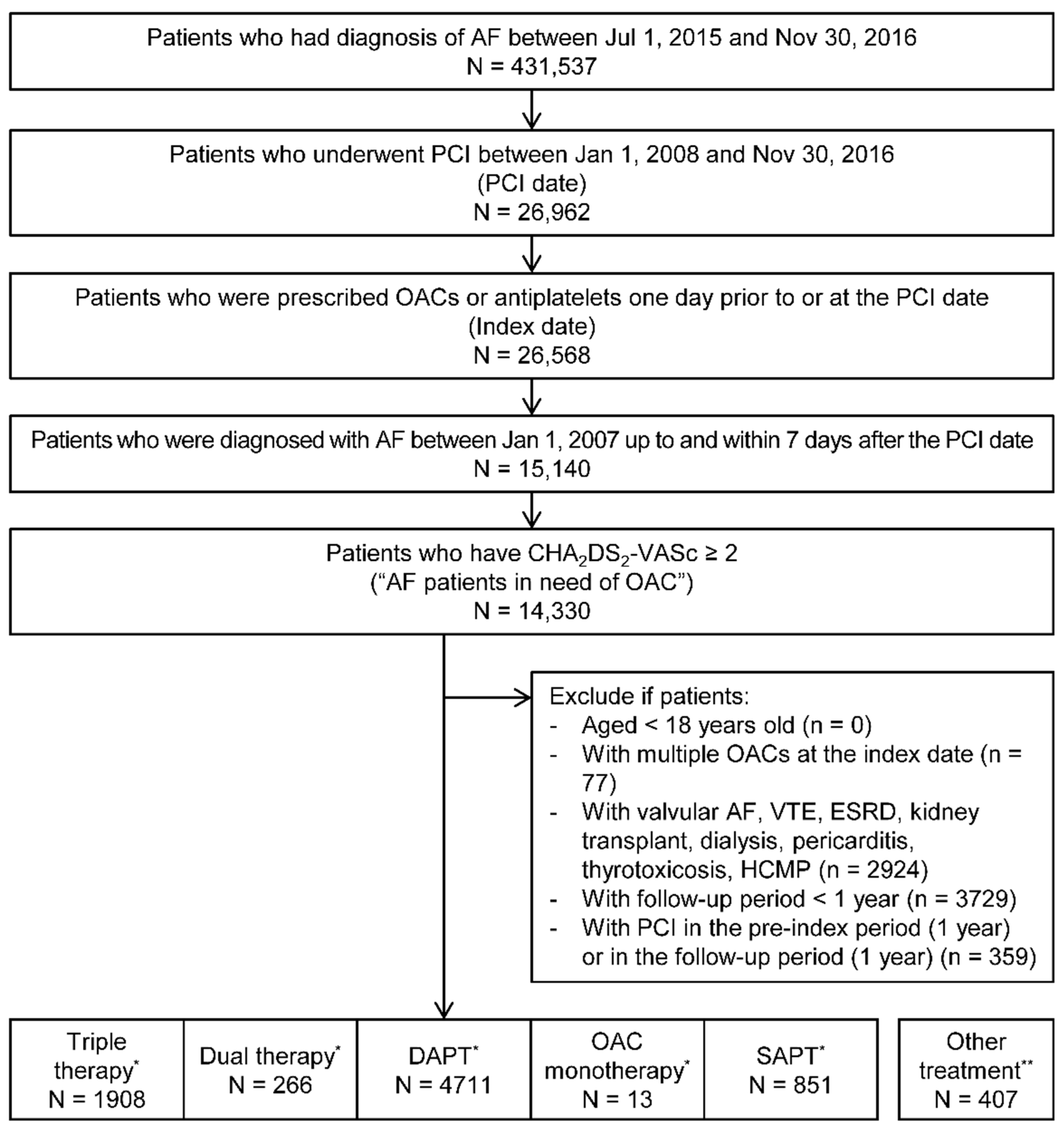
2.2. Study Population
2.3. Temporal Trends and Treatment Patterns
2.4. Treatment Duration
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
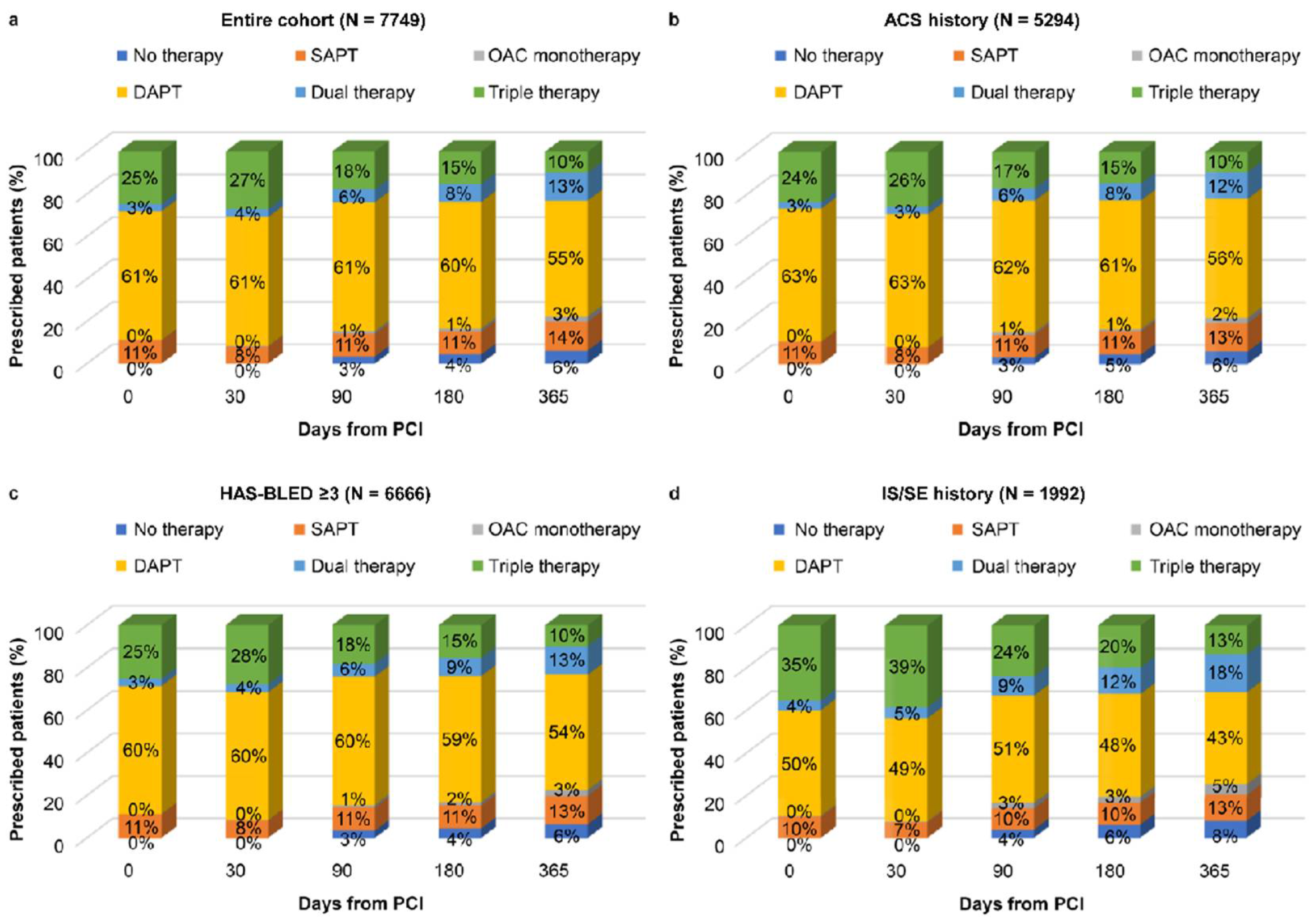
3.2. Treatment Patterns and Temporal Trends
3.3. Treatment Duration
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Caturano, A.; Galiero, R.; Pafundi, P.C. Atrial fibrillation and stroke. A review on the use of vitamin K antagonists and novel oral anticoagulants. Medicina 2019, 55, 617. [Google Scholar] [CrossRef] [Green Version]
- Benjamin, E.J.; Virani, S.S.; Callaway, C.W.; Chamberlain, A.M.; Chang, A.; Cheng, S.; Chiuve, S.E.; Cushman, M.; Delling, F.N.; Deo, R.; et al. Heart disease and stroke statistics—2018 update: A report from the American Heart Association. Circulation 2018, 137, e67–e492. [Google Scholar] [CrossRef] [PubMed]
- Kirchhof, P.; Benussi, S.; Kotecha, D.; Ahlsson, A.; Atar, D.; Casadei, B.; Castella, M.; Diener, H.-C.; Heidbuchel, H.; Hendriks, J.; et al. 2016 ESC guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur. Heart J. 2016, 37, 2893–2962. [Google Scholar] [CrossRef] [Green Version]
- Lip, G.Y.H.; Banerjee, A.; Boriani, G.; Chiang, C.E.; Fargo, R.; Freedman, B.; Lane, D.A.; Ruff, C.T.; Turakhia, M.; Werring, D.; et al. Antithrombotic therapy for atrial fibrillation: CHEST guideline and expert panel report. Chest 2018, 154, 1121–1201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michniewicz, E.; Mlodawska, E.; Lopatowska, P.; Tomaszuk-Kazberuk, A.; Malyszko, J. Patients with atrial fibrillation and coronary artery disease—Double trouble. Adv. Med. Sci. 2018, 63, 30–35. [Google Scholar] [CrossRef]
- Valgimigli, M.; Bueno, H.; Byrne, R.A.; Collet, J.P.; Costa, F.; Jeppsson, A.; Jüni, P.; Kastrati, A.; Kolh, P.; Mauri, L.; et al. ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS: The task force for dual antiplatelet therapy in coronary artery disease of the European Society of Cardiology (ESC) and of the European As-sociation for Cardio-Thoracic Surgery (EACTS). Kardiol. Pol. 2018, 39, 213–260. [Google Scholar]
- ACTIVE Writing Group on behalf of the ACTIVE Investigators. Clopidogrel plus aspirin versus oral anticoagulation for atrial fibrillation in the atrial fibrillation clopidogrel trial with irbesartan for prevention of vascular events (ACTIVE W): A ran-domized controlled trial. Lancet 2006, 367, 1903–1912. [Google Scholar] [CrossRef]
- Dewilde, W.J.; Oirbans, T.; Verheugt, F.W.; Kelder, J.C.; De Smet, B.J.; Herrman, J.-P.; Adriaenssens, T.; Vrolix, M.; Heestermans, A.A.; Vis, M.M.; et al. Use of clopidogrel with or without aspirin in patients taking oral anticoagulant therapy and undergoing percutaneous coronary intervention: An open-label, randomised, controlled trial. Lancet 2013, 381, 1107–1115. [Google Scholar] [CrossRef]
- Gibson, C.M.; Mehran, R.; Bode, C.; Halperin, J.; Verheugt, F.W.; Wildgoose, P.; Birmingham, M.; Ianus, J.; Burton, P.; Van Eickels, M.; et al. Prevention of bleeding in patients with atrial fibrillation undergoing PCI. N. Engl. J. Med. 2016, 375, 2423–2434. [Google Scholar] [CrossRef] [Green Version]
- Cannon, C.P.; Bhatt, D.L.; Oldgren, J.; Lip, G.Y.; Ellis, S.G.; Kimura, T.; Maeng, M.; Merkely, B.; Zeymer, U.; Gropper, S.; et al. Dual antithrombotic therapy with dabigatran after PCI in atrial fibrillation. N. Engl. J. Med. 2017, 377, 1513–1524. [Google Scholar] [CrossRef]
- Lopes, R.D.; Heizer, G.; Aronson, R.; Vora, A.N.; Massaro, T.; Mehran, R.; Goodman, S.G.; Windecker, S.; Darius, H.; Li, J.; et al. Antithrombotic therapy after acute coronary syndrome or PCI in atrial fibrillation. N. Engl. J. Med. 2019, 380, 1509–1524. [Google Scholar] [CrossRef] [Green Version]
- January, C.T.; Wann, L.S.; Calkins, H.; Chen, L.Y.; Cigarroa, J.E.; Cleveland, J.C., Jr.; Ellinor, P.T.; Ezekowitz, M.D.; Field, M.E.; Furie, K.L.; et al. 2019 AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: A report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines and the Heart Rhythm Society in collaboration with the Society of Thoracic Surgeons. Circulation 2019, 140, e125–e151. [Google Scholar] [PubMed]
- Angiolillo, D.J.; Goodman, S.G.; Bhatt, D.L.; Eikelboom, J.W.; Price, M.J.; Moliterno, D.J.; Cannon, C.P.; Tanguay, J.F.; Granger, C.B.; Mauri, L.; et al. Antithrombotic therapy in patients with atrial fibrillation treated with oral anticoagulation undergoing percutaneous coronary intervention: A north American perspective—2018 Update. Circulation 2018, 138, 527–536. [Google Scholar] [CrossRef] [Green Version]
- Neumann, F.-J.; Uva, M.S.; Ahlsson, A.; Alfonso, F.; Banning, A.; Benedetto, U.; Byrne, R.A.; Collet, J.-P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS guidelines on myocardial revascularization. Eur. Heart J. 2018, 40, 87–165. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-A.; Yoon, S.; Kim, L.-Y.; Kim, D.-S. Towards actualizing the value potential of Korea health insurance review and assessment (HIRA) data as a resource for health research: Strengths, limitations, applications, and strategies for optimal use of HIRA data. J. Korean Med. Sci. 2017, 32, 718–728. [Google Scholar] [CrossRef]
- Valgimigli, M.; Bueno, H.; Byrne, R.; Collet, J.-P.; Costa, F.; Jeppsson, A.; Jüni, P.; Kastrati, A.; Kolh, P.; Mauri, L.; et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS. Eur. J. Cardio-Thorac. Surg. 2017, 53, 34–78. [Google Scholar] [CrossRef] [Green Version]
- Palmerini, T.; Biondi-Zoccai, G.; Della Riva, D.; Stettler, C.; Sangiorgi, D.; D’Ascenzo, F.; Kimura, T.; Briguori, C.; Sabatè, M.; Kim, H.S.; et al. Stent thrombosis with drug-eluting and bare-metal stents: Evidence from a comprehensive network meta-analysis. Lancet 2012, 379, 1393–1402. [Google Scholar] [CrossRef]
- El-Hayek, G.; Bangalore, S.; Casso Dominguez, A.; Devireddy, C.; Jaber, W.; Kumar, G.; Mavromatis, K.; Tamis-Holland, J.; Samady, H. Meta-analysis of randomized clinical trials comparing biodegradable polymer drug-eluting stent to second-generation durable polymer drug-eluting stents. JACC Cardiovasc. Interv. 2017, 10, 462–473. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.; Koh, Y.-S.; Kim, P.-J.; Kim, H.-Y.; Park, C.S.; Lee, J.M.; Kim, D.-B.; Yoo, K.-D.; Jeon, D.S.; Her, S.-H.; et al. Incidence, implications, and predictors of stent thrombosis in acute myocardial infarction. Am. J. Cardiol. 2016, 117, 1562–1568. [Google Scholar] [CrossRef] [PubMed]
- Bartorelli, A.L.; Versaci, F.; Briguori, C.; Tomai, F.; Aprigliano, G.; Poli, A.; Vigna, C.; Marinucci, L.; My, L.; Masi, F.; et al. The BIOFLOW-III Italian satellite registry: 18-month results of the Orsiro stent in an all-comer high-risk population. J. Cardiovasc. Med. 2019, 20, 464–470. [Google Scholar] [CrossRef]
- Secemsky, E.A.; Matteau, A.; Yeh, R.W.; Steg, P.G.; Camenzind, E.; Wijns, W.; McFadden, E.; Mauri, L.; PROTECT Trial Investigators. Comparison of short- and long-term cardiac mortality in early versus late stent thrombosis (from Pooled PROTECT Trials). Am. J. Cardiol. 2015, 115, 1678–1684. [Google Scholar]
- Camm, A.J.; Kirchhof, P.; Lip, G.Y.; Schotten, U.; Savelieva, I.; Ernst, S.; Van Gelder, I.C.; Al-Attar, N.; Hindricks, G.; European Heart Rhythm Association (EHRA); et al. Guidelines for the management of atrial fibrillation: The task force for the management of atrial fibrillation of the European Society of Cardiology (ESC). Eur. Heart J. 2010, 31, 2369–2429. [Google Scholar] [CrossRef]
- Dulli, D.A.; Stanko, H.; Levine, R.L. Atrial fibrillation is associated with severe acute ischemic stroke. Neuroepidemiology 2003, 22, 118–123. [Google Scholar] [CrossRef]
- Park, J.; Choi, E.-K.; Han, K.-D.; Choi, Y.-J.; Lee, S.-R.; Cha, M.-J.; Kang, J.; Park, K.W.; Oh, S.; Lip, G.Y. Antithrombotic therapy in patients with atrial fibrillation after percutaneous coronary intervention during 2-year follow-up, from a nationwide population study. Am. J. Cardiol. 2019, 123, 1921–1926. [Google Scholar] [CrossRef] [PubMed]
- Vranckx, P.; Valgimigli, M.; Eckardt, L.; Tijssen, J.; Lewalter, T.; Gargiulo, G.; Batushkin, V.; Campo, G.; Lysak, Z.; Vakaliuk, I.; et al. Edoxaban-based versus vitamin K antagonist-based antithrombotic regimen after successful coronary stenting in patients with atrial fibrillation (ENTRUST-AF PCI): A randomized, open-label, phase 3b trial. Lancet 2019, 394, 1335–1343. [Google Scholar] [CrossRef]
- Park, J.; Choi, E.K.; Han, K.D.; Choi, Y.J.; Lee, E.; Choe, W.; Lee, S.R.; Cha, M.J.; Lim, W.H.; Kang, J.; et al. Temporal trends in prevalence and antithrombotic treatment among Asians with atrial fibrillation undergoing percutaneous coronary intervention: A nationwide Korean population-based study. PLoS ONE 2019, 14, e0209593. [Google Scholar] [CrossRef]
- Park, B.J.; Sung, J.; Park, K.; Seo, S.W.; Kim, S.H. Studying on Diagnosis Accuracy for Health Insurance Claims Data in Korea; Seoul National University: Seoul, Korea, 2003; pp. 17–29. (In Korean) [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Triple Therapy a (N = 1908) | Dual Therapy a (N = 266) | DAPT a (N = 4711) | OAC Monotherapy a (N = 13) | SAPT a (N = 851) | p-Value b | |
|---|---|---|---|---|---|---|
| Index treatment, % | ||||||
| Warfarin | 94.5 | 97.7 | 0 | 92.3 | 0 | NA |
| NOAC | 5.5 | 2.3 | 0 | 7.7 | 0 | NA |
| Apixaban | 0.8 | 0.8 | 0 | 0 | 0 | NA |
| Dabigatran | 2.3 | 0.8 | 0 | 7.7 | 0 | NA |
| Rivaroxaban | 2.4 | 0.8 | 0 | 0 | 0 | NA |
| Aspirin–clopidogrel | 97.2 | 0 | 94.1 | 0 | 0 | NA |
| Aspirin–prasugrel | 0.5 | 0 | 1.0 | 0 | 0 | NA |
| Aspirin–ticagrelor | 2.4 | 0 | 4.9 | 0 | 0 | NA |
| Aspirin | 0 | 6.0 | 0 | 0 | 6.3 | NA |
| Clopidogrel | 0 | 92.9 | 0 | 0 | 91.2 | NA |
| Prasugrel | 0 | 0.4 | 0 | 0 | 0.6 | NA |
| Ticagrelor | 0 | 0.8 | 0 | 0 | 1.9 | NA |
| Age (years), mean | 70.7 | 69.0 | 70.3 | 68.9 | 69.7 | 0.0097 |
| Female, % | 33.1 | 28.2 | 34.5 | 30.8 | 36.0 | 0.1525 |
| Insurance, % | ||||||
| NHI | 92.7 | 94.0 | 92.6 | 100.0 | 92.9 | 0.7763 |
| Medical aid | 7.3 | 6.0 | 7.4 | 0.0 | 7.1 | |
| CHA2DS2-VASc, mean | 4.6 | 4.1 | 4.2 | 4.6 | 4.1 | <0.0001 |
| HAS-BLED, mean | 3.7 | 3.4 | 3.5 | 3.9 | 3.5 | <0.0001 |
| CCI, mean | 4.1 | 3.6 | 3.7 | 3.8 | 3.5 | <0.0001 |
| Medical history, % | ||||||
| ACS | 65.6 | 58.3 | 70.5 | 38.5 | 65.9 | <0.0001 |
| CHF | 44.9 | 33.1 | 36.1 | 46.2 | 26.8 | <0.0001 |
| Hypertension | 91.6 | 92.5 | 92.2 | 92.3 | 92.7 | 0.8604 |
| Diabetes | 64.4 | 66.2 | 60.8 | 53.8 | 63.8 | 0.027 |
| Ischemic stroke | 34.1 | 29.3 | 19.2 | 53.8 | 20.6 | <0.0001 |
| Systemic embolism | 4.4 | 5.3 | 2.9 | 7.7 | 3.8 | 0.0125 |
| Vascular disease | 42.1 | 31.6 | 46.6 | 38.5 | 38.9 | <0.0001 |
| Renal disease (CKD3/4) | 1.5 | 0.0 | 0.9 | 0.0 | 0.1 | 0.0053 |
| Bleeding | 27.1 | 16.5 | 26.3 | 38.5 | 23.3 | 0.0012 |
| Medication history, % | ||||||
| NOACs | 3.6 | 1.1 | 1.4 | 0.0 | 0.8 | <0.0001 |
| Warfarin | 49.8 | 53.8 | 9.4 | 69.2 | 12.0 | <0.0001 |
| NSAIDs | 81.4 | 80.1 | 83.3 | 76.9 | 83.4 | 0.2617 |
| Antiplatelets | 63.9 | 64.3 | 72.5 | 84.6 | 70.9 | <0.0001 |
| Antiarrhythmics | 61.4 | 56.8 | 59.4 | 76.9 | 61.6 | 0.1971 |
| Statins | 88.7 | 78.2 | 88.4 | 92.3 | 82.0 | <0.0001 |
| Proton pump inhibitors | 44.3 | 30.1 | 42.6 | 38.5 | 28.4 | <0.0001 |
| H2-receptor antagonists | 74.6 | 69.2 | 76.7 | 53.8 | 76.0 | 0.0095 |
| Digoxin | 39.8 | 38.7 | 29.8 | 38.5 | 29.6 | <0.0001 |
| N | % | Treatment Patterns | |
|---|---|---|---|
| Triple therapy group | 1908 | ||
| 1st | 440 | 23.1 | Triple therapy 12 months |
| 2nd | 218 | 11.4 | Triple therapy 1 month ⇒ DAPT 11 months |
| 3rd | 86 | 4.5 | Triple therapy 1 month ⇒ Dual therapy 11 months |
| Triple therapy group ⇒ Dual therapy switcher | 611 | ||
| 1st | 86 | 14.1 | Triple therapy 1 month ⇒ Dual therapy 11 months |
| 2nd | 44 | 7.2 | Triple therapy 8 months ⇒ Dual therapy 4 months |
| 3rd | 41 | 6.7 | Triple therapy 7 months ⇒ Dual therapy 5 months |
| DAPT group | 4711 | ||
| 1st | 2951 | 62.6 | DAPT 12 months |
| 2nd | 119 | 2.5 | DAPT 1 month ⇒ SAPT 11 months |
| 3rd | 55 | 1.2 | DAPT 11 months ⇒ SAPT 1 month |
| Treatment Durations (Days) | ||||
|---|---|---|---|---|
| N | % | Mean (SE) | Median | |
| Triple therapy group | 1908 | Treatment duration of triple therapy a | ||
| Entire b | 1907 | 99.9 | 138.18 (3.17) | 81 |
| ACS history b | 1251 | 65.6 | 141.39 (3.94) | 87 |
| HAS-BLED ≥ 3 b | 1675 | 87.8 | 134.56 (3.37) | 75 |
| IS/SE history | 703 | 36.8 | 122.93 (5.09) | 55 |
| Female | 694 | 36.4 | 120.71 (5.09) | 47 |
| Age ≥ 75 | 632 | 33.1 | 122.32 (5.3) | 56.5 |
| Triple therapy group ⇒ Dual therapy switcher | 611 | Treatment duration of dual therapy a | ||
| Entire | 611 | 100.0 | 162.57 (4.17) | 155 |
| ACS history | 400 | 65.5 | 164.17 (5.21) | 149 |
| HAS-BLED ≥ 3 | 541 | 88.5 | 162.53 (4.47) | 155 |
| IS/SE history | 238 | 39.0 | 157.52 (6.99) | 131 |
| Female | 230 | 37.6 | 160.49 (6.81) | 150.5 |
| Age ≥ 75 | 205 | 33.6 | 157.49 (7.09) | 142 |
| DAPT group | 4711 | Treatment duration of DAPT a | ||
| Entire | 4711 | 100.0 | 261.75 (1.99) | 344 |
| ACS history | 3321 | 70.5 | 262.37 (2.38) | 345 |
| HAS-BLED ≥ 3 | 4015 | 85.2 | 258.21 (2.19) | 343 |
| IS/SE history | 994 | 21.1 | 236.71 (4.63) | 324 |
| Female | 1677 | 35.6 | 245.93 (3.49) | 334 |
| Age ≥ 75 | 1627 | 34.5 | 256.58 (3.44) | 341 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, S.; Han, S.; Jang, S.-W.; Lee, M.-Y.; On, Y.-K.; Bang, O.Y.; Lee, J.-M.; Park, Y.-J.; Shin, J.-S.; Kang, S.; et al. Treatment Pattern of Antithrombotic Therapy over Time after Percutaneous Coronary Intervention in Patients with Atrial Fibrillation in Real-World Practice in Korea. Healthcare 2021, 9, 1185. https://doi.org/10.3390/healthcare9091185
Han S, Han S, Jang S-W, Lee M-Y, On Y-K, Bang OY, Lee J-M, Park Y-J, Shin J-S, Kang S, et al. Treatment Pattern of Antithrombotic Therapy over Time after Percutaneous Coronary Intervention in Patients with Atrial Fibrillation in Real-World Practice in Korea. Healthcare. 2021; 9(9):1185. https://doi.org/10.3390/healthcare9091185
Chicago/Turabian StyleHan, Seongwook, Sola Han, Sung-Won Jang, Myung-Yong Lee, Young-Keun On, Oh Young Bang, Ji-Min Lee, Yoo-Jung Park, Ji-Soo Shin, Seongsik Kang, and et al. 2021. "Treatment Pattern of Antithrombotic Therapy over Time after Percutaneous Coronary Intervention in Patients with Atrial Fibrillation in Real-World Practice in Korea" Healthcare 9, no. 9: 1185. https://doi.org/10.3390/healthcare9091185
APA StyleHan, S., Han, S., Jang, S.-W., Lee, M.-Y., On, Y.-K., Bang, O. Y., Lee, J.-M., Park, Y.-J., Shin, J.-S., Kang, S., Suh, H. S., & Kim, Y.-H. (2021). Treatment Pattern of Antithrombotic Therapy over Time after Percutaneous Coronary Intervention in Patients with Atrial Fibrillation in Real-World Practice in Korea. Healthcare, 9(9), 1185. https://doi.org/10.3390/healthcare9091185