
The Evaluation of Preference and Perceived Quality of Health Communication Icons Associated with COVID-19 Prevention Measures

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Material and Methods
2.1. Participants
2.2. Icon Collection
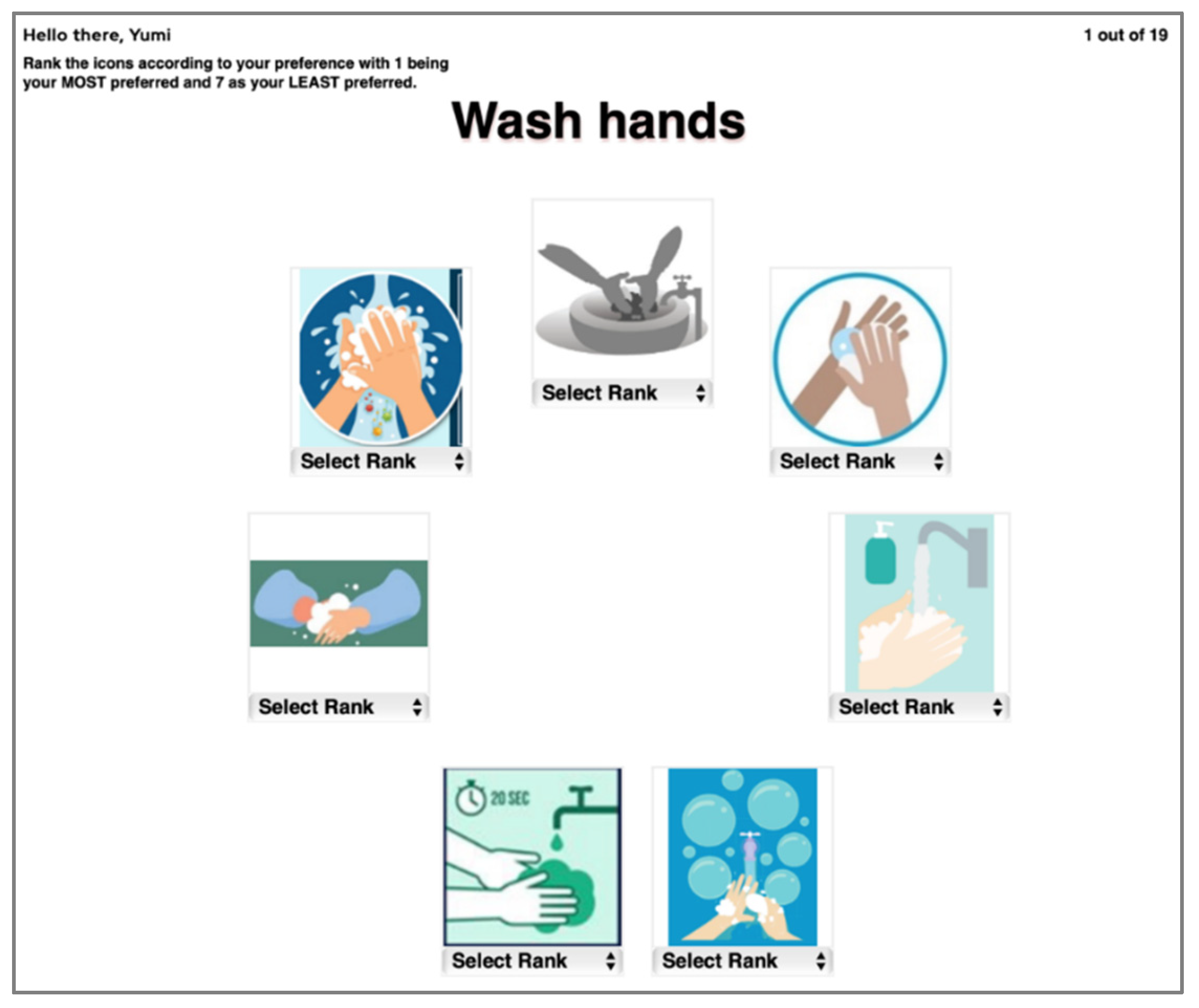
2.3. Ranking Test
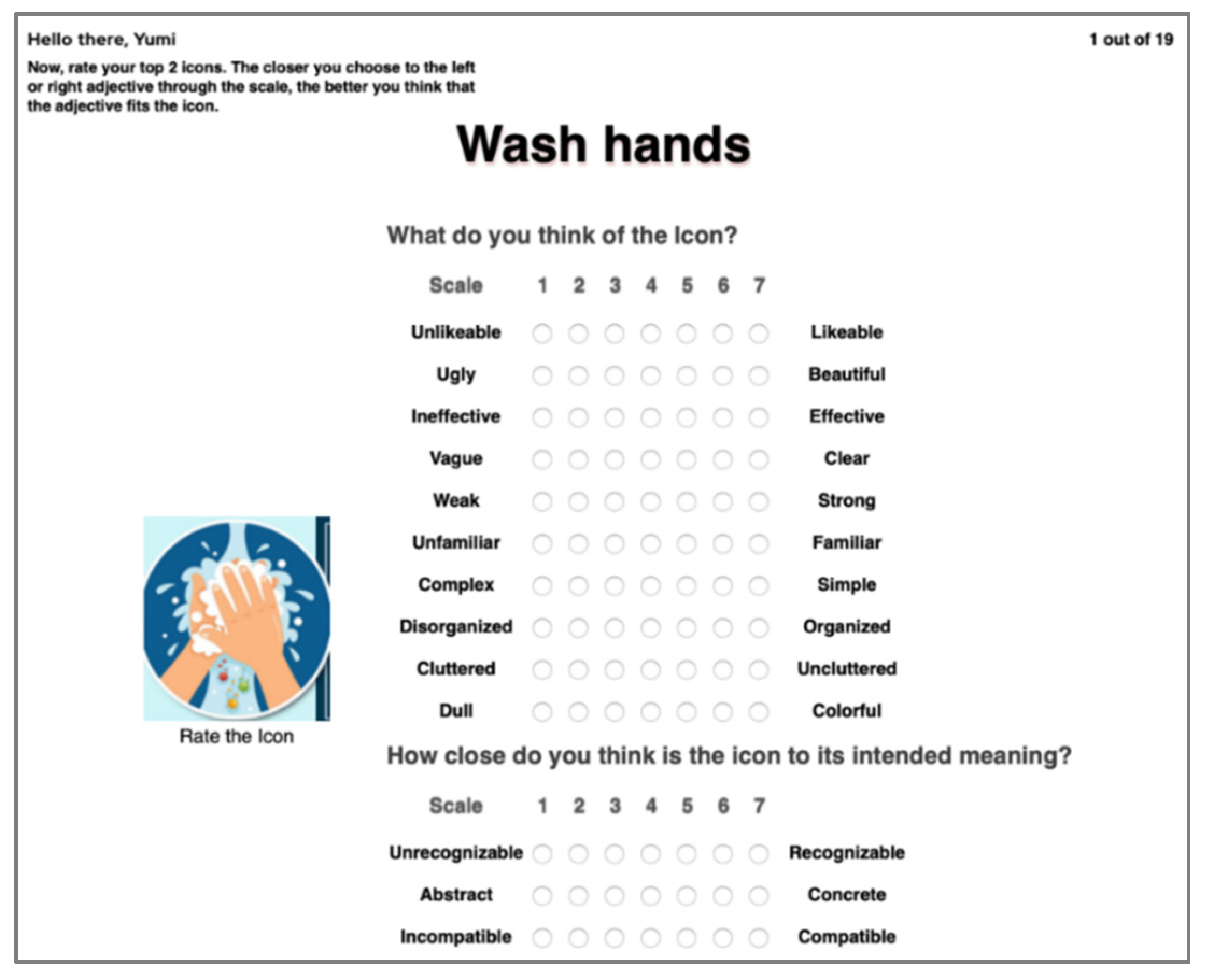
2.4. Subjective Rating Test
2.5. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vigoroso, L.; Caffaro, F.; Cavallo, E. Occupational safety and visual communication: User-centred design of safety training material for migrant farmworkers in Italy. Saf. Sci. 2020, 121, 562–572. [Google Scholar] [CrossRef]
- Horton, W. The Icon Book: Visual Symbols for Computer Systems and Documentation, 1st ed.; Wiley: New York, NY, USA, 1994. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. How to Protect Yourself & Others. 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/prevention.html (accessed on 12 August 2020).
- Chi, C.-F.; Dewi, R.S. Matching performance of vehicle icons in graphical and textual formats. Appl. Ergon. 2014, 45, 904–916. [Google Scholar] [CrossRef]
- Chi, C.-F.; Dewi, R.S.; Samali, P.; Hsieh, D.-Y. Preference ranking test for different icon design formats for smart living room and bathroom functions. Appl. Ergon. 2019, 81, 102891. [Google Scholar] [CrossRef] [PubMed]
- Lodding, K. Iconic Interfacing. IEEE Comput. Graph. Appl. 1983, 3, 11–20. [Google Scholar] [CrossRef]
- Goonetilleke, R.; Shih, H.M.; On, H.K.; Fritsch, J. Effects of training and representational characteristics in icon design. Int. J. Hum. Comput. Stud. 2001, 55, 741–760. [Google Scholar] [CrossRef] [Green Version]
- Blattner, M.; Sumikawa, D.; Greenberg, R. Earcons and Icons: Their Structure and Common Design Principles. Hum. Comput. Interact. 1989, 4, 11–44. [Google Scholar] [CrossRef]
- Reder, P.J.; Mccallum, C.A. Flexible Mouse-Driven Method of User Interface. U.S. Patent 6,727,919, 27 April 2004. Available online: https://patents.google.com/patent/US6727919B1/en (accessed on 12 August 2020).
- Wiedenbeck, S. The use of icons and labels in an end user application program: An empirical study of learning and retention. Behav. Inf. Technol. 1999, 18, 68–82. [Google Scholar] [CrossRef]
- Blankenberger, S.; Hahn, K. Effects of icon design on human-computer interaction. Int. J. Man-Mach. Stud. 1991, 35, 363–377. [Google Scholar] [CrossRef]
- Stotts, D.B. The Usefulness of Icons on the Computer Interface: Effect of Graphical Abstraction and Functional Representation on Experienced and Novice Users. Proc. Hum. Factors Ergon. Soc. Annu. Meet. 1998, 42, 453–457. [Google Scholar] [CrossRef]
- Dewar, R.E.; Ells, J.G.; Mundy, G. Reaction Time as an Index of Traffic Sign Perception. Hum. Factors J. Hum. Factors Ergon. Soc. 1976, 18, 381–391. [Google Scholar] [CrossRef]
- Lindberg, T.; Näsänen, R. The effect of icon spacing and size on the speed of icon processing in the human visual system. Displays 2003, 24, 111–120. [Google Scholar] [CrossRef]
- Ojanpää, H.; Näsänen, R. Effects of luminance and colour contrast on the search of information on display devices. Displays 2003, 24, 167–178. [Google Scholar] [CrossRef]
- Huang, K.-C.; Chang, W.-T.; Wei, W.-L. Effects of visual field, exposure time, and set size on icon search with varied delays using an LCD monitor. J. Soc. Inf. Disp. 2010, 18, 1. [Google Scholar] [CrossRef]
- Shen, Z.; Zhang, L.; Li, R.; Liang, R. The effects of icon internal characteristics on complex cognition. Int. J. Ind. Ergon. 2020, 79, 102990. [Google Scholar] [CrossRef]
- Ng, A.W.; Chan, A.H. The guessability of traffic signs: Effects of prospective-user factors and sign design features. Accid. Anal. Prev. 2007, 39, 1245–1257. [Google Scholar] [CrossRef]
- Ng, A.; Chan, A. Visual and Cognitive Features on Icon Effectiveness. In Proceedings of the International Multiconference of Engineers and Computer Scientists, Hong Kong, China, 19–21 March 2008; Volume 2, pp. 19–21. [Google Scholar]
- McDougall, S.J.P.; Curry, M.B.; De Bruijn, O. Measuring symbol and icon characteristics: Norms for concreteness, complexity, meaningfulness, familiarity, and semantic distance for 239 symbols. Behav. Res. Methods Instrum. Comput. 1999, 31, 487–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, S.-M.; Shieh, K.-K.; Chi, C.-F. Factors affecting the design of computer icons. Int. J. Ind. Ergon. 2002, 29, 211–218. [Google Scholar] [CrossRef]
- Isherwood, S.J.; McDougall, S.; Curry, M.B. Icon Identification in Context: The Changing Role of Icon Characteristics With User Experience. Hum. Factors J. Hum. Factors Ergon. Soc. 2007, 49, 465–476. [Google Scholar] [CrossRef]
- Silvennoinen, J.M.; Kujala, T.; Jokinen, J.P. Semantic distance as a critical factor in icon design for in-car infotainment systems. Appl. Ergon. 2017, 65, 369–381. [Google Scholar] [CrossRef] [Green Version]
- Tsai, C.-Y. Effect of graphic simplification and graphic metaphor on the memory and identification of travel map. Int. J. Ind. Ergon. 2017, 61, 29–36. [Google Scholar] [CrossRef]
- Gittins, D. Icon-based human-computer interaction. Int. J. Man-Mach. Stud. 1986, 24, 519–543. [Google Scholar] [CrossRef]
- García, M.; Badre, A.N.; Stasko, J.T. Development and validation of icons varying in their abstractness. Interact. Comput. 1994, 6, 191–211. [Google Scholar] [CrossRef]
- McDougall, S.J.P.; de Bruijn, O.; Curry, M.B. Exploring the effects of icon characteristics on user performance: The role of icon concreteness, complexity, and distinctiveness. J. Exp. Psychol. Appl. 2000, 6, 291–306. [Google Scholar] [CrossRef]
- Stammers, R.; Hoffman, J. Transfer between Icon Sets and Ratings of Icon Concreteness and Appropriateness. Proc. Hum. Factors Soc. Annu. Meet. 1991, 35, 354–358. [Google Scholar] [CrossRef]
- International Standards Organization. Graphical Symbols—Creation and Design of Public Information Symbols—Requirements; ISO Standard 22727; International Standards Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Gingold, M.; Shteingart, S.; Green, P. Truck Drivers’ Suggestions and Preferences for Instrument Panel Symbols; Techinical Report UM-HSRI-81-30; The University of Michigan Transportation Research Institute: Ann Arbor, MI, USA, 1981; Available online: https://deepblue.lib.umich.edu/bitstream/handle/2027.42/368/47110.0001.001.pdf;sequence=2 (accessed on 12 August 2020).
- Chi, C.-F.; Drury, C. A further note on psychophysical testing of handles. Appl. Ergon. 1988, 19, 315–318. [Google Scholar] [CrossRef]
- Chi, C.-F.; Dewi, R.S.; Huang, M.-H. Psychophysical evaluation of auditory signals in passenger vehicles. Appl. Ergon. 2016, 59, 153–164. [Google Scholar] [CrossRef] [PubMed]
- Hoekstra, E.; Williams, M.; Green, P. Development and Driver Understanding of Hazard Warning and Location Symbols for IVSAWS; Techinical Report UMTRI-93-16; The University of Michigan Transportation Research Institute: Ann Arbor, MI, USA, 1993; Available online: https://deepblue.lib.umich.edu/bitstream/handle/2027.42/1011/86543.0001.001.pdf?sequence=2 (accessed on 12 August 2020).
- Wolff, J.S.; Wogalter, M.S. Comprehension of Pictorial Symbols: Effects of Context and Test Method. Hum. Factors J. Hum. Factors Ergon. Soc. 1998, 40, 173–186. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.-C.; Ho, C.-H. The effects of age on symbol comprehension in central rail hubs in Taiwan. Appl. Ergon. 2012, 43, 1016–1025. [Google Scholar] [CrossRef] [PubMed]
- Chi, C.-F.; Lin, F.-T. A Comparison of Seven Visual Fatigue Assessment Techniques In Three Data-Acquisition VDT Tasks. Hum. Factors J. Hum. Factors Ergon. Soc. 1998, 40, 577–590. [Google Scholar] [CrossRef] [PubMed]
- Chi, C.-F.; Dewi, R.S.; Surbakti, Y.Y.; Hsieh, D.-Y. The perceived quality of in-vehicle auditory signals: A structural equation modelling approach. Ergonomics 2017, 60, 1471–1484. [Google Scholar] [CrossRef] [PubMed]
- Stylidis, K.; Wickman, C.; Söderberg, R. Perceived quality of products: A framework and attributes ranking method. J. Eng. Des. 2020, 31, 37–67. [Google Scholar] [CrossRef] [Green Version]
- Bovea, M.D.; Quemades-Beltrán, P.; Pérez-Belis, V.; Juan, P.; Braulio-Gonzalo, M.; Ibáñez-Forés, V. Options for labelling circular products: Icon design and consumer preferences. J. Clean. Prod. 2018, 202, 1253–1263. [Google Scholar] [CrossRef]
- Choi, J.H.; Lee, H.-J. Facets of simplicity for the smartphone interface: A structural model. Int. J. Hum. Comput. Stud. 2012, 70, 129–142. [Google Scholar] [CrossRef]
- Campbell, J.L.; Hoffmeister, D.H.; Kiefer, R.J.; Selke, D.J.; Green, P.; Richman, J.B. Comprehension Testing of Active Safety Symbols. J. Passeng. Cars Mech. Syst. J. 2004, 113, 197–203. [Google Scholar]
- Rogers, Y. Icons at the interface: Their usefulness. Interact. Comput. 1989, 1, 105–117. [Google Scholar] [CrossRef]
- Liu, W.; Cao, Y.; Proctor, R.W. How do app icon color and border shape influence visual search efficiency and user experi-ence? Evidence from an eye-tracking study. Int. J. Ind. Ergon. 2021, 84, 103160. [Google Scholar] [CrossRef]
- Cahigas, M.M.; Prasetyo, Y.T. Matching-Based Comprehension of Emergency Safety Symbols Among Filipinos: Us-er-Centered Quality Measure. In Proceedings of the 21st Congress of the International Ergonomics Association (IEA 2021), online, 13–18 June 2021; pp. 384–392. [Google Scholar]
- Madel, L.; Cahigas, M.; Tri Prasetyo, Y. Kansei Engineering-based Model and Online Content Assessment in Evaluating Ser-vice Design of Lazada Express. In Proceedings of the 2020 The 6th International Conference on Industrial and Business Engineerin, Macau, China, 27–29 September 2020. [Google Scholar]
- McDougall, S.; Reppa, I.; Kulik, J.; Taylor, A. What makes icons appealing? The role of processing fluency in predicting icon appeal in different task contexts. Appl. Ergon. 2016, 55, 156–172. [Google Scholar] [CrossRef]
- Huang, H.; Yang, M.; Yang, C.; Lv, T. User performance effects with graphical icons and training for elderly novice users: A case study on automatic teller machines. Appl. Ergon. 2019, 78, 62–69. [Google Scholar] [CrossRef]
- Prasetyo, Y.T.; Castillo, A.M.; Salonga, L.J.; Sia, J.A.; Seneta, J.A. Factors affecting perceived effectiveness of COVID-19 prevention measures among Filipinos during Enhanced Community Quarantine in Luzon, Philippines: Integrating Protection Motivation Theory and extended Theory of Planned Behavior. Int. J. Infect. Dis. 2020, 99, 312–323. [Google Scholar] [CrossRef] [PubMed]
- Salman, Y.B.; Cheng, H.-I.; Patterson, P.E. Icon and user interface design for emergency medical information systems: A case study. Int. J. Med. Inform. 2012, 81, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Lamy, J.-B.; Soualmia, L.F.; Kerdelhué, G.; Venot, A.; Duclos, C. Validating the semantics of a medical iconic language using ontological reasoning. J. Biomed. Inform. 2012, 46, 56–67. [Google Scholar] [CrossRef]
- Lindell, M.K.; Bostrom, A.; Goltz, J.D.; Prater, C.S. Evaluating hazard awareness brochures: Assessing the textual, graphical, and numerical features of tsunami evacuation products. Int. J. Disaster Risk Reduct. 2021, 61, 102361. [Google Scholar] [CrossRef]
- Payre, W.; Diels, C. Designing in-vehicle signs for connected vehicle features: Does appropriateness guarantee comprehension? Appl. Ergon. 2019, 80, 102–110. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.; Park, J.; Park, J.; Choe, M.; Kim, T.; Choi, M.; Lee, S. Effect of touch button interface on in-vehicle information systems usability. Int. J. Hum. Comput. Interac. 2021, 1–19. [Google Scholar] [CrossRef]
- Jylhä, H.; Hamari, J. Development of measurement instrument for visual qualities of graphical user interface elements (VISQUAL): A test in the context of mobile game icons. User Model. User-Adapted Interact. 2020, 30, 949–982. [Google Scholar] [CrossRef]
- Jylhä, H.; Hamari, J. Demographic factors have little effect on aesthetic perceptions of icons: A study of mobile game icons. Internet Res. 2021. ahead-of-print. [Google Scholar] [CrossRef]
- Cao, Y.; Zhang, Y.; Ding, Y.; Duffy, V.G.; Zhang, X. Is an anthropomorphic app icon more attractive? Evidence from neu-roergonomomics. Appl. Ergon. 2021, 97, 103545. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Huang, J.; Zhou, J. Skeuomorphic or flat icons for an efficient visual search by younger and older adults? Appl. Ergon. 2020, 85, 103073. [Google Scholar] [CrossRef]
- Chen, M.-S.; Lin, M.-C.; Wang, C.-C.; Chang, C.A. Using HCA and TOPSIS approaches in personal digital assistant menu–icon interface design. Int. J. Ind. Ergon. 2009, 39, 689–702. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Category | N | % |
|---|---|---|---|
| Gender | Male | 25 | 43.9 |
| Female | 32 | 56.1 | |
| Age | 18–25 | 48 | 84.2 |
| 26–33 | 3 | 5.3 | |
| 34–40 | 6 | 10.5 | |
| Educational Background | High School Graduate | 18 | 31.6 |
| College Graduate | 36 | 63.2 | |
| Master Graduate | 3 | 5.3 |
| Functions |
|---|
| 1. Shortness of Breath |
| 2. Fever |
| 3. Cough or Cold |
| 4. Difficulty in Breathing |
| 5. Wash Hands |
| 6. Consult Doctor/Seek Medical Help |
| 7. Avoid People with Flu-Like Symptoms |
| 8. Cover Face when Coughing/Sneezing |
| 9. Get Information from Trusted Sources |
| 10. Wear Face Mask |
| 11. Avoid Crowded Places/Limit Social Gatherings |
| 12. Dispose Tissue and Face Mask in Waste Can |
| 13. Use Alcohol-Based Hand Sanitizers if Soap and Water are Not Available. |
| 14. Avoid Travelling to Places with Known Cases |
| 15. Avoid Touching your Face |
| 16. Wash Clothes Properly |
| 17. De-Contaminate/Disinfect |
| 18. Home Quarantine/Stay at Home |
| 19. Social Distancing |
| Function | Rank 1 | Rank 2 | Rank 3 | Rank 4 | Rank 5 | Rank 6 | Rank 7 |
|---|---|---|---|---|---|---|---|
| Shortness of Breath (1) |  (mean: 2.807; SD 1.652) |  (mean: 3.175; SD: 1.843) |  (mean: 3.351; SD: 1.747) |  (mean: 4.351; SD: 1.986) |  (mean: 4.386; SD: 2.042) |  (mean: 4.93; SD: 1.981) |  (mean: 5.000; SD: 1.592) |
| Source | (k) | (j) | (c) | (e) | (e) | (l) | (a) |
| Fever (2) |  (mean: 2.772; SD: 1.604) |  (mean: 2.807; SD: 1.903) |  (mean: 3.509; SD: 1.774) |  (mean: 3.719; SD: 1.556) |  (mean: 3.737; SD: 1.395) |  (mean: 5.509; SD: 1.692) |  (mean: 5.947; SD:1.54) |
| Source | (m) | (a) | (e) | (e) | (c) | (e) | (e) |
| Cough or Cold (3) |  (mean: 2.789; SD: 1.75) |  (mean: 2.86; SD: 1.575) |  (mean: 3.158; SD: 1.601) |  (mean: 3.298; SD: 1.669) |  (mean: 4.93; SD: 1.438) |  (mean: 5.263; SD: 1.685) |  (mean: 5.702; SD: 1.792) |
| Source | (a) | (n) | (e) | (a) | (a) | (d) | (a) |
| Difficulty in Breathing (4) |  (mean: 2.772; SD: 1.991) |  (mean: 3.333; SD: 1.786) |  (mean: 3.86; SD: 1.652) |  (mean: 3.86; SD: 1.726) |  (mean: 4.07; SD: 2.017) |  (mean: 4.105; SD: 1.961) |  (mean: 6.000; SD: 1.268) |
| Source | (e) | (a) | (n) | (a) | (b) | (m) | (a) |
| Wash Hands (5) |  (mean: 2.526; SD: 1.91) |  (mean: 2.895; SD: 1.622) |  (mean: 3.544; SD: 1.477) |  (mean: 3.544; SD: 1.753) |  (mean: 4.579; SD: 1.569) |  (mean: 4.614; SD: 1.556) |  (mean: 6.298; SD: 1.451) |
| Source | (o) | (d) | (e) | (b) | (d) | (d) | (h) |
| Consult Doctor/Seek Medical Help (6) |  (mean: 1.789; SD: 1.176) |  (mean: 2.965; SD: 1.488) |  (mean: 3.439; SD: 1.604) |  (mean: 3.807; SD: 1.563) |  (mean: 3.965; SD: 1.5) |  (mean: 5.386; SD: 0.94) |  (mean: 6.649; SD: 1.11) |
| Source | (d) | (b) | (d) | (e) | (a) | (d) | (d) |
| Avoid People with Flu-Like Symptoms (7) |  (mean: 2.439; SD: 1.239) |  (mean: 2.491; SD: 1.571) |  (mean: 2.702; SD: 1.792) |  (mean: 4.228; SD: 1.268) |  (mean: 4.807; SD: 1.608) |  (mean: 5.298; SD: 1.488) |  (mean: 6.035; SD: 1.309) |
| Source | (d) | (d) | (d) | (a) | (a) | (d) | (g) |
| Cover when Coughing or Sneezing (8) |  (mean: 2.667; SD: 2.003) |  (mean: 3.000; SD: 1.5) |  (mean: 3.404; SD: 1.811) |  (mean: 4.246; SD: 1.735) |  (mean: 4.316; SD: 1.649) |  (mean: 4.614; SD: 1.634) |  (mean: 5.754; SD: 1.921) |
| Source | (a) | (d) | (d) | (e) | (a) | (a) | (d) |
| Get Information from Trusted Sources (9) |  (mean: 1.614; SD: 1.013) |  (mean: 3.158; SD: 1.544) |  (mean: 3.316; SD: 1.844) |  (mean: 4.316; SD: 1.919) |  (mean: 4.895; SD: 1.41) |  (mean: 5.018; SD: 1.458) |  (mean: 5.684; SD: 1.429) |
| Source | (d) | (h) | (e) | (e) | (a) | (a) | (a) |
| Wear Face Mask (10) |  (mean: 2.877; SD: 1.722) |  (mean: 2.982; SD: 1.685) |  (mean: 3.158; SD: 1.177) |  (mean: 3.579; SD: 1.625) |  (mean: 3.579; SD: 1.658) |  (mean: 5.702; SD: 2.009) |  (mean: 6.123; SD: 0.965) |
| Source | (p) | (n) | (g) | (e) | (e) | (a) | (d) |
| Avoid Crowded Places/Limit Social Gatherings (11) |  (mean: 1.754; SD: 1.023) |  (mean: 2.211; SD: 1.333) |  (mean: 3.754; SD: 1.418) |  (mean: 3.947; SD: 1.231) |  (mean: 4.193; SD: 1.381) |  (mean: 5.439; SD: 1.35) |  (mean: 6.702; SD: 0.626) |
| Source | (d) | (d) | (h) | (e) | (d) | (d) | (d) |
| Dispose Tissue and Face Mask in Waste Can (12) |  (mean: 1.86; SD: 1.025) |  (mean: 2.404; SD: 1.237) |  (mean: 2.456; SD: 1.351) |  (mean: 4.579; SD: 1.535) |  (mean: 5.158; SD: 0.996) |  (mean: 5.439; SD: 1.165) |  (mean: 6.105; SD: 1.175) |
| Source | (e) | (q) | (d) | (f) | (d) | (d) | (a) |
| Use Hand Sanitizers (13) |  (mean: 1.386; SD: 0.861) |  (mean: 3.228; SD: 1.402) |  (mean: 3.649; SD: 1.395) |  (mean: 4.351; SD: 1.631) |  (mean: 4.772; SD: 1.722 |  (mean: 5.298; SD: 1.812) |  (mean: 5.316; SD: 1.744) |
| Source | (e) | (r) | (d) | (i) | (d) | (a) | (i) |
| Avoid Traveling to Places with Known Cases (14) |  (mean: 1.807; SD: 1.302) |  (mean: 2.702; SD: 1.721) |  (mean: 3.702; SD: 1.463) |  (mean: 3.86; SD: 1.505 |  (mean: 4.14; SD: 1.302) |  (mean: 5.877; SD: 1.001) |  (mean: 5.912; SD: 1.64) |
| Source | (d) | (a) | (s) | (d) | (d) | (d) | (d) |
| Avoid Touching Face (15) |  (mean: 2.193; SD: 1.517) |  (mean: 2.93; SD: 1.689) |  (mean: 3.281; SD: 1.77 |  (mean: 3.404; SD: 1.438) |  (mean: 5.105; SD: 1.372) |  (mean: 5.14; SD: 1.381) |  (mean: 5.947; SD: 1.597) |
| Source | (d) | (e) | (d) | (d) | (d) | (f) | (d) |
| Wash Clothes Properly (16) |  (mean: 2.667; SD: 1.704) |  (mean: 2.579; SD: 1.569) |  (mean: 2.825; SD: 1.627) |  (mean: 3.842; SD: 1.556 |  (mean: 4.684; SD: 1.416) |  (mean: 4.912; SD: 1.455 |  (mean: 6.491; SD: 1.002) |
| Source | (i) | (d) | (d) | (i) | (i) | (i) | (i) |
| De-Contaminate (17) |  (mean: 2.526; SD: 1.477) |  (mean: 3.263; SD: 1.904) |  (mean: 3.86; SD: 1.807) |  (mean: 4.035; SD: 2.026) |  (mean: 4.07; SD: 2.17) |  (mean: 4.947; SD: 1.807) |  (mean: 5.298; SD: 1.388 |
| Source | (e) | (d) | (d) | (d) | (d) | (d) | (q) |
| Home Quarantine/Stay at Home (18) |  (mean: 1.439; SD: 0.982) |  (mean: 2.614; SD: 1.221) |  (mean: 3.368; SD: 1.588) |  (mean: 4.596; SD: 1.545) |  (mean: 5.035; SD: 1.752) |  (mean: 5.263; SD: 1.232) |  (mean: 5.684; SD: 1.242) |
| Source | (d) | (d) | (d) | (e) | (e) | (q) | (f) |
| Social Distancing (19) |  (mean: 2.158; SD: 1.192) |  (mean: 2.281; SD: 1.485 |  (mean: 3.526 SD: 1.67) |  (mean: 4.684; SD: 1.774) |  (mean: 4.737; SD: 1.653) |  (mean: 5.263; SD: 1.446) |  (mean: 5.351; SD: 1.706) |
| Source | (e) | (d) | (d) | (d) | (h) | (b) | (a) |
| Subjective Design Features | Definition |
|---|---|
| Perceived Icon Quality | One of the most critical aspects of icon development that defines the successful design [38] |
| Communicativeness | Refers to how the icon expresses its intended meaning [21]. |
| Complexity | Pertains to how complex the details intricated on the icon are [19]. |
| Layout | How carefully the features of an icon are arranged [21]. |
| Semantic Distance | The measure of the closeness of what is illustrated in the icon to its true intended meaning [20]. |
| Subjective Design Features | Semantic Scales |
|---|---|
| Perceived Icon Quality | 1. Unlikable—Likable 2. Ugly—Beautiful [39] 3. Ineffective—Effective |
| Communicativeness | 4. Vague—Clear 5. Weak—Strong [39] 6. Unfamiliar—Familiar [4,21,39] |
| Complexity | 7. Complex—Simple [4,7,40] |
| Layout | 8. Disorganized—Organized 9. Cluttered—Uncluttered 10. Dull—Colorful [39] |
| Semantic Distance | 11. Unrecognizable—Recognizable [21] 12. Abstract—Concrete [4,39] 13. Incompatible—Compatible |
| Variable | Mean | SD |
|---|---|---|
| 1. unlikeable–likeable | 6.0651 | 1.2062 |
| 2. ugly–beautiful | 5.8347 | 1.2821 |
| 3. ineffective–effective | 6.0803 | 1.2331 |
| 4. vague–clear | 6.0416 | 1.278 |
| 5. weak–strong | 5.9861 | 1.2754 |
| 6. unfamiliar–familiar | 6.0974 | 1.2317 |
| 7. complex–simple | 6.1053 | 1.2513 |
| 8. disorganized–organized | 6.1283 | 1.1324 |
| 9. cluttered–uncluttered | 5.9908 | 1.27 |
| 10. dull–colorful | 5.7664 | 1.4093 |
| 11. unrecognizable–recognizable | 6.1768 | 1.1496 |
| 12. abstract–concrete | 6.0794 | 1.1405 |
| 13. incompatible–compatible | 6.1491 | 1.1313 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Unlikable–Likable | 1 | 1 | ||||||||||||
| Ugly–Beautiful | 2 | 0.749 ** | 1 | |||||||||||
| Ineffective–Effective | 3 | 0.645 ** | 0.610 ** | 1 | ||||||||||
| Vague–Clear | 4 | 0.584 ** | 0.567 ** | 0.786 ** | 1 | |||||||||
| Weak–Strong | 5 | 0.609 ** | 0.607 ** | 0.787 ** | 0.796 ** | 1 | ||||||||
| Unfamiliar–Familiar | 6 | 0.560 ** | 0.553 ** | 0.709 ** | 0.722 ** | 0.749 ** | 1 | |||||||
| Complex–Simple | 7 | 0.494 ** | 0.489 ** | 0.661 ** | 0.666 ** | 0.689 ** | 0.727 ** | 1 | ||||||
| Disorganized–Organized | 8 | 0.579 ** | 0.569 ** | 0.684 ** | 0.681 ** | 0.685 ** | 0.709 ** | 0.774 ** | 1 | |||||
| Cluttered–Uncluttered | 9 | 0.548 ** | 0.560 ** | 0.637 ** | 0.621 ** | 0.635 ** | 0.655 ** | 0.731 ** | 0.819 ** | 1 | ||||
| Dull–Colorful | 10 | 0.552 ** | 0.619 ** | 0.454 ** | 0.448 ** | 0.471 ** | 0.442 ** | 0.362 ** | 0.460 ** | 0.448 ** | 1 | |||
| Unrecognizable–Recognizable | 11 | 0.586 ** | 0.526 ** | 0.706 ** | 0.701 ** | 0.682 ** | 0.661 ** | 0.627 ** | 0.639 ** | 0.604 ** | 0.428 ** | 1 | ||
| Abstract–Concrete | 12 | 0.575 ** | 0.547 ** | 0.703 ** | 0.700 ** | 0.706 ** | 0.653 ** | 0.634 ** | 0.656 ** | 0.632 ** | 0.459 ** | 0.752 ** | 1 | |
| Incompatible–Compatible | 13 | 0.587 ** | 0.542 ** | 0.707 ** | 0.681 ** | 0.693 ** | 0.653 ** | 0.613 ** | 0.650 ** | 0.622 ** | 0.453 ** | 0.784 ** | 0.816 ** | 1 |
| Rank | −0.195 ** | −0.134 ** | −0.199 ** | −0.206 ** | −0.205 ** | −0.169 ** | −0.162 ** | −0.176 ** | −0.152 ** | −0.145 ** | −0.194 ** | −0.195 ** | −0.200 ** | |
| Ranks | |
|---|---|
| Mean Rank | |
| Unlikable–Likable Rank 1 | 1.7 |
| Unlikable–Likable Rank 2 | 1.3 |
| Test Statistics | |
| N | 57 |
| Chi-Square | 14.297 |
| df | 1 |
| Asymptotic significance | 0.000 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Function 1 | 0.024 | 0.9 | 0.947 | 0.1 | 0.021 | 1.884 | 0 | 2.273 | 0.364 | 1.089 | 3.27 | 0.1 | 1.256 |
| Function 2 | 7.049 ** | 6.149 ** | 1.882 | 6.721 ** | 6.422 ** | 2.5 | 4 * | 4.667 * | 3.13 | 4.787 ** | 6.081 ** | 7.811 ** | 6.4 ** |
| Function 3 | 5.818 ** | 1.256 | 5.488 ** | 13.714 ** | 8.100 ** | 4.667 * | 0.676 | 1.778 | 3.457 | 3.13 | 11.765 ** | 12.6 ** | 9.323 ** |
| Function 4 | 4.667 ** | 1.6 | 4.568 ** | 7.714 ** | 5.818 ** | 1.195 | 0 | 0.857 | 0.1 | 2.273 | 3.789 | 1.524 | 4.122 * |
| Function 5 | 2 | 1.4 | 1.195 | 2.814 | 2.951 | 0.818 | 0.22 | 2.189 | 1.256 | 0.037 | 2.5 | 1.524 | 0.857 |
| Function 6 | 1.976 | 1.976 | 4.122 * | 1.524 | 0.61 | 0.231 | 2.077 | 2.632 | 1.195 | 0 | 4.333* | 1.524 | 5.233 ** |
| Function 7 | 2.077 | 1.976 | 2.314 | 0.9 | 2.778 | 1.778 | 0.947 | 1.195 | 0.22 | 6.721 ** | 0.421 | 2.077 | 2.5 |
| Function 8 | 14.297 ** | 5.444 ** | 7.111 ** | 10.314 ** | 9.757 ** | 7.258 ** | 6.818 ** | 3.457 | 6.429 ** | 11.308 ** | 13.333 ** | 14.235 ** | 15.125 ** |
| Function 9 | 4.333 ** | 1.195 | 5.488 ** | 2.381 | 6.721 ** | 5.233 ** | 7.049 ** | 2.189 | 3.27 | 1.391 | 1.684 | 3.596 | 2.381 |
| Function 10 | 6.081 ** | 1.524 | 3.333 | 7.529 ** | 6.125 ** | 2.133 | 6.737 ** | 9 ** | 7.346 ** | 5.444 ** | 5.121 ** | 4.235 ** | 10.125 ** |
| Function 11 | 0.15 | 1.4 | 2 | 1.778 | 5.765 ** | 4.235 ** | 2 | 5.143 ** | 1.2 | 2.814 | 2.455 | 6.533 | 3.457 |
| Function 12 | 2.814 | 0.243 | 8.805 ** | 4.333 ** | 5.333 ** | 0.857 | 1.524 | 2.814 | 0.206 | 4.122 ** | 2.189 | 3.756 | 5.769 ** |
| Function 13 | 6.429 ** | 1.256 | 0.4 | 2.189 | 3.27 | 1.485 | 5.121 ** | 1.778 | 3.6 | 6.081 ** | 3.103 | 4.235 ** | 1.485 |
| Function 14 | 3.125 | 0.105 | 10.526 ** | 10.314 ** | 7.111 ** | 6.737 ** | 5.121 ** | 9.757 ** | 7.111 ** | 0.231 | 11.111 ** | 9 ** | 4.568 ** |
| Function 15 | 1.485 | 1.4 | 4 ** | 10.756 ** | 6.081 ** | 4.333 ** | 12.6 ** | 9 ** | 4 ** | 2.778 | 7.41 ** | 3.457 | 6.081 ** |
| Function 16 | 0.118 | 0.4 | 0.111 | 0.027 | 0.118 | 0.758 | 1.125 | 0.105 | 0.22 | 0.9 | 3.457 | 1.324 | 3.27 |
| Function 17 | 10.800 ** | 7.410 ** | 2.778 | 1.778 | 1.6 | 1.125 | 1.385 | 2.286 | 7.529 ** | 6.422 ** | 2.286 | 5.452 ** | 5.765 * |
| Function 18 | 4.235 * | 2.635 | 8.395 ** | 7.078 ** | 5.488 * | 4.900* | 6.095 * | 8.395 ** | 5.488 * | 1.976 | 1.884 | 3.130 | 5.000 * |
| Function 19 | 4.333 * | 2.951 | 7.111 ** | 3.333 | 2.778 | 6.818 ** | 5.765 * | 2.793 | 4.235 * | 0.243 | 1.581 | 4.568 * | 1.690 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prasetyo, Y.T.; Dewi, R.S.; Balatbat, N.M.; Antonio, M.L.B.; Chuenyindee, T.; Perwira Redi, A.A.N.; Young, M.N.; Diaz, J.F.T.; Kurata, Y.B. The Evaluation of Preference and Perceived Quality of Health Communication Icons Associated with COVID-19 Prevention Measures. Healthcare 2021, 9, 1115. https://doi.org/10.3390/healthcare9091115
Prasetyo YT, Dewi RS, Balatbat NM, Antonio MLB, Chuenyindee T, Perwira Redi AAN, Young MN, Diaz JFT, Kurata YB. The Evaluation of Preference and Perceived Quality of Health Communication Icons Associated with COVID-19 Prevention Measures. Healthcare. 2021; 9(9):1115. https://doi.org/10.3390/healthcare9091115
Chicago/Turabian StylePrasetyo, Yogi Tri, Ratna Sari Dewi, Naiomi M. Balatbat, Michael Lancelot B. Antonio, Thanatorn Chuenyindee, Anak Agung Ngurah Perwira Redi, Michael Nayat Young, John Francis T. Diaz, and Yoshiki B. Kurata. 2021. "The Evaluation of Preference and Perceived Quality of Health Communication Icons Associated with COVID-19 Prevention Measures" Healthcare 9, no. 9: 1115. https://doi.org/10.3390/healthcare9091115
APA StylePrasetyo, Y. T., Dewi, R. S., Balatbat, N. M., Antonio, M. L. B., Chuenyindee, T., Perwira Redi, A. A. N., Young, M. N., Diaz, J. F. T., & Kurata, Y. B. (2021). The Evaluation of Preference and Perceived Quality of Health Communication Icons Associated with COVID-19 Prevention Measures. Healthcare, 9(9), 1115. https://doi.org/10.3390/healthcare9091115