
The Chinese Government’s Response to the Pandemic: Measures, Dynamic Changes, and Main Patterns


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Preprocessing
2.2. Data Analysis
3. Results
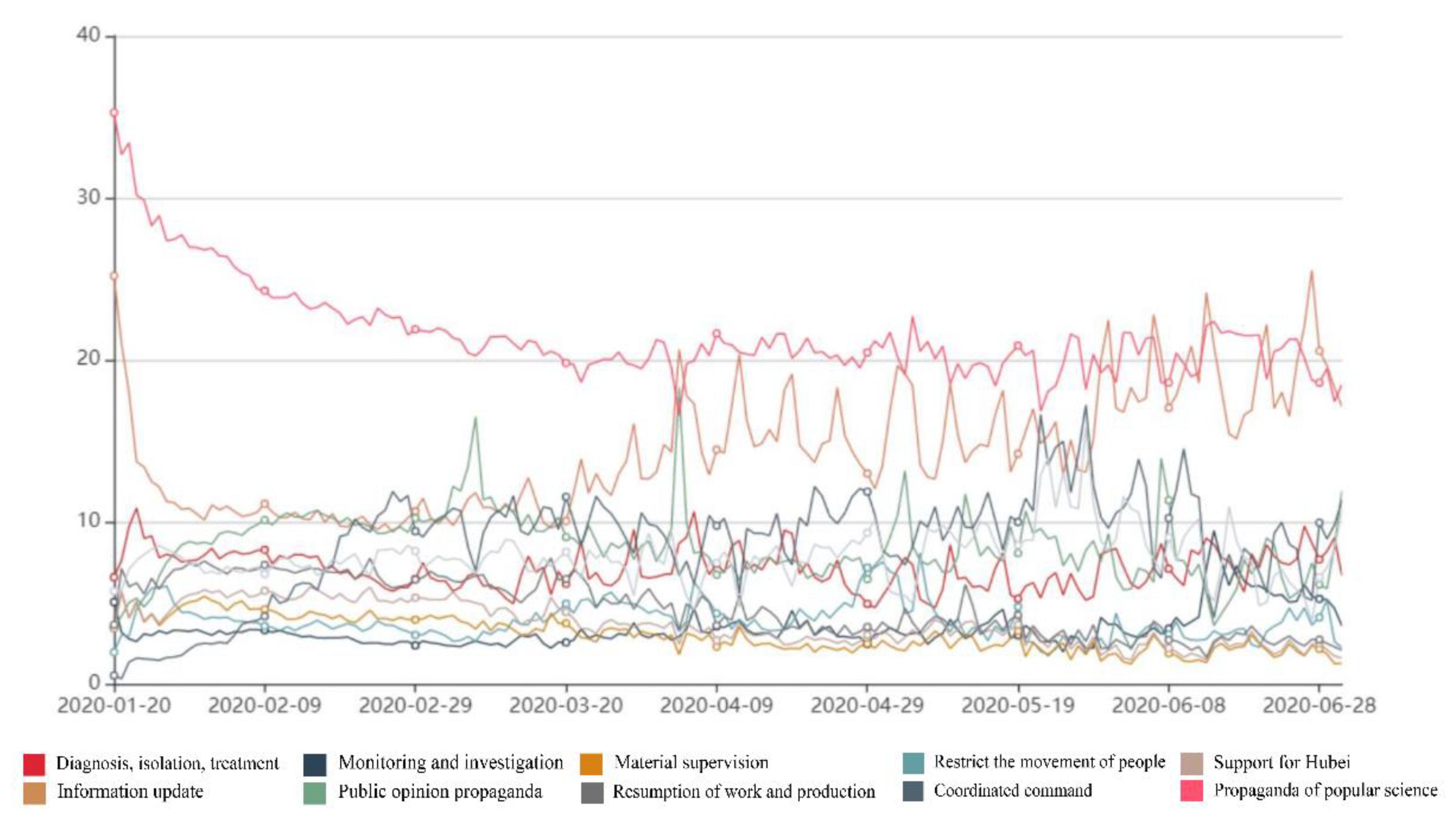
3.1. Overview of the Dynamic Evolution of Pandemic Governance Measures
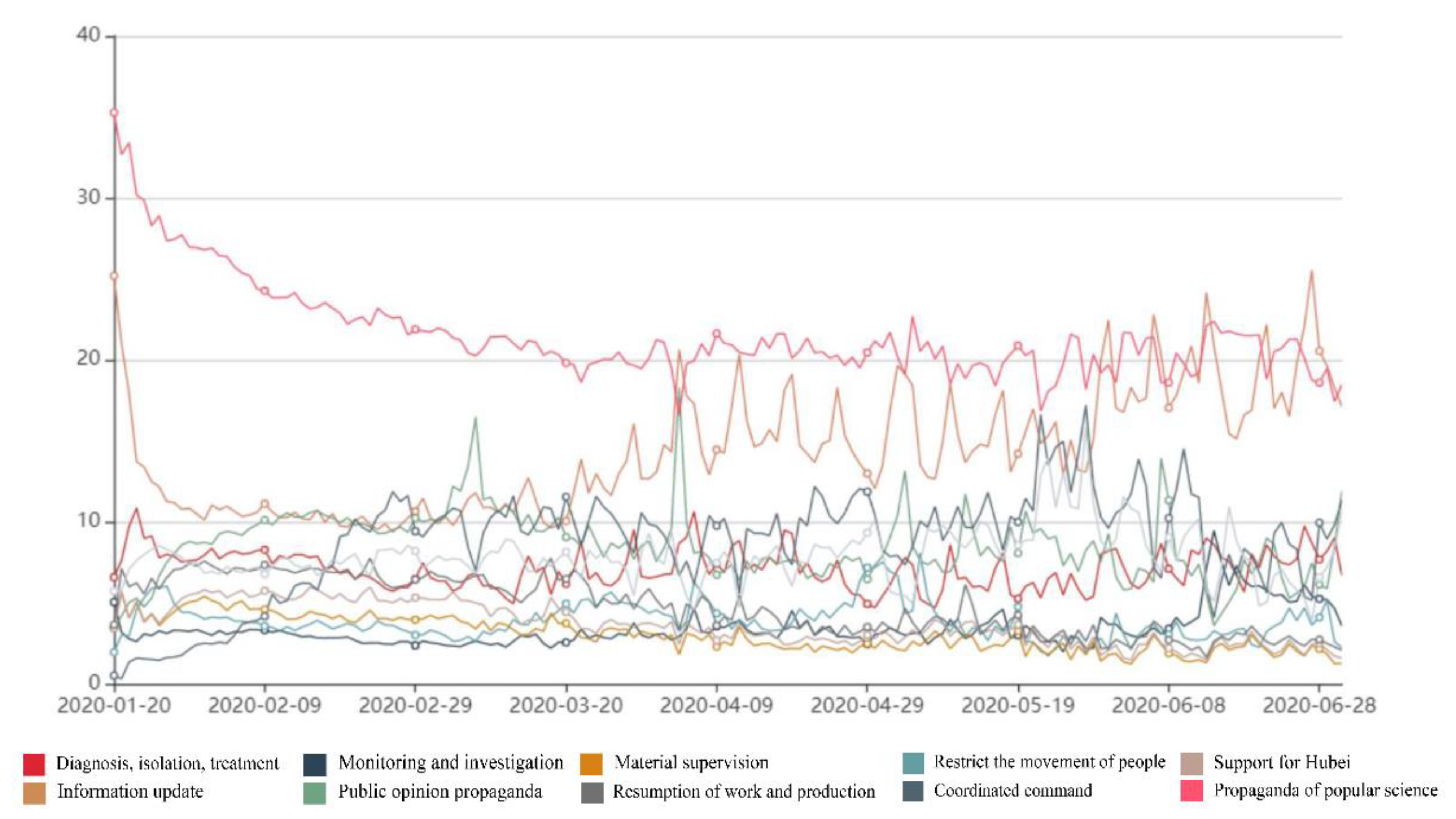
3.1.1. Comprehensive National Level
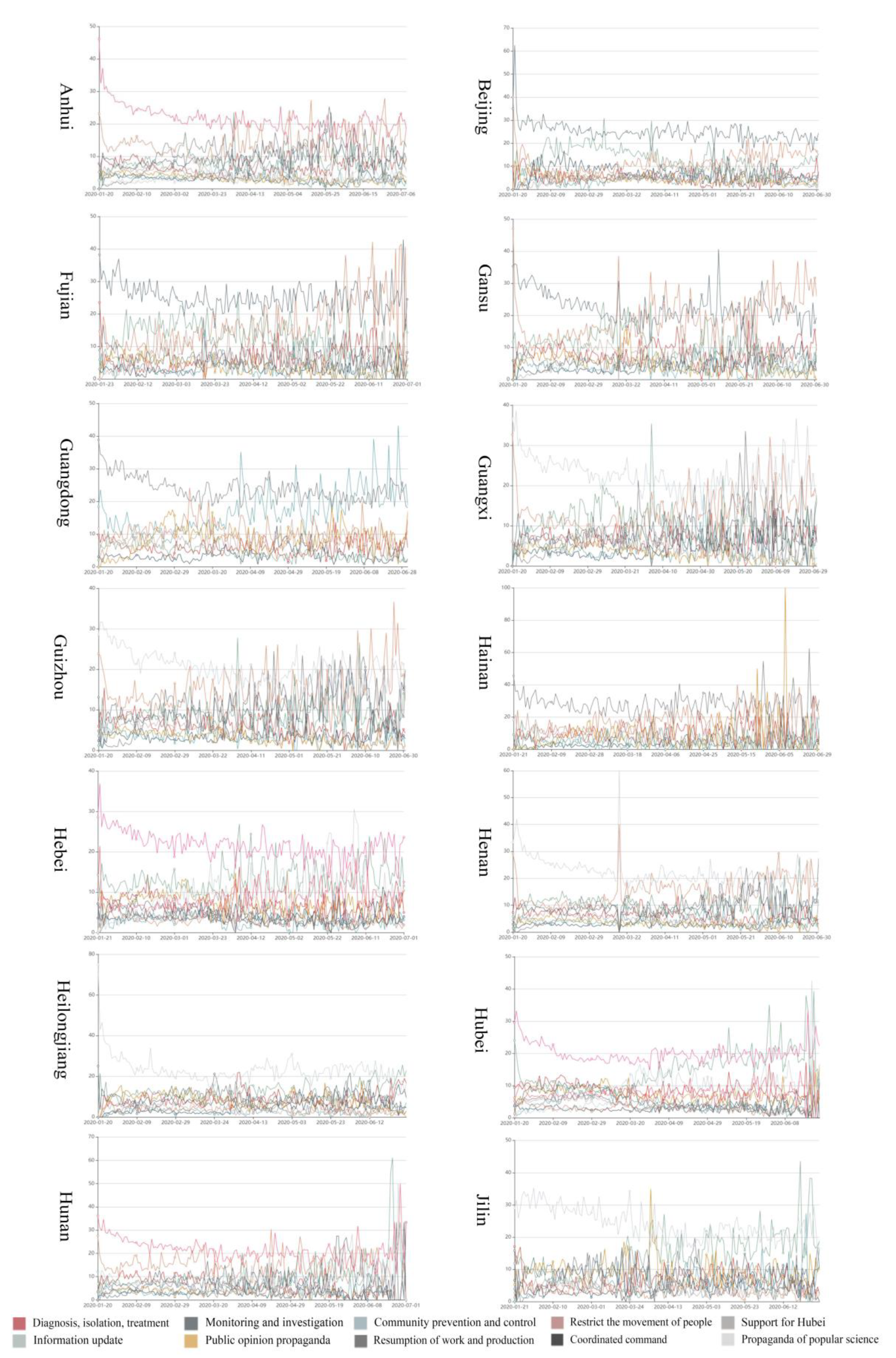
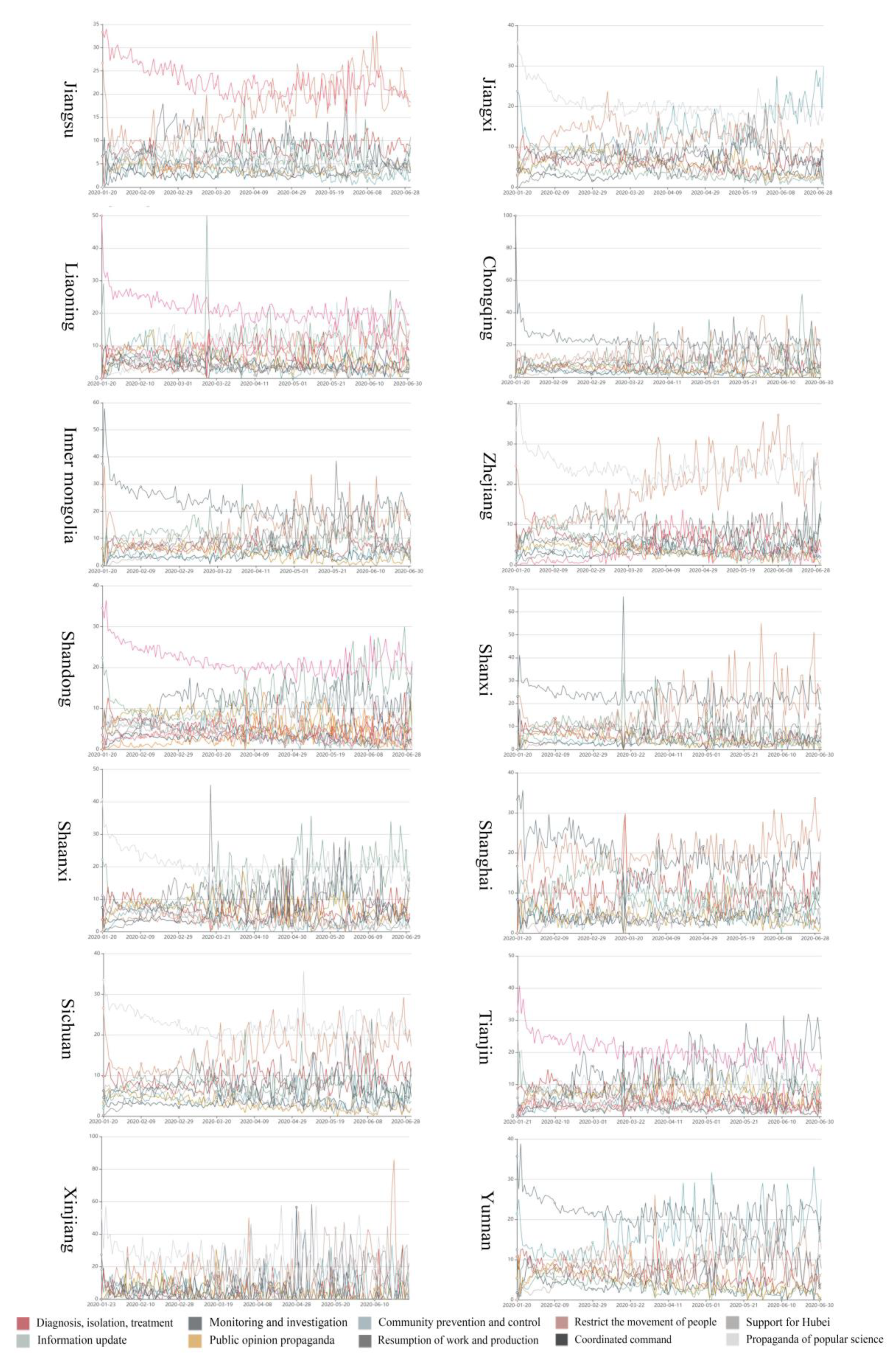
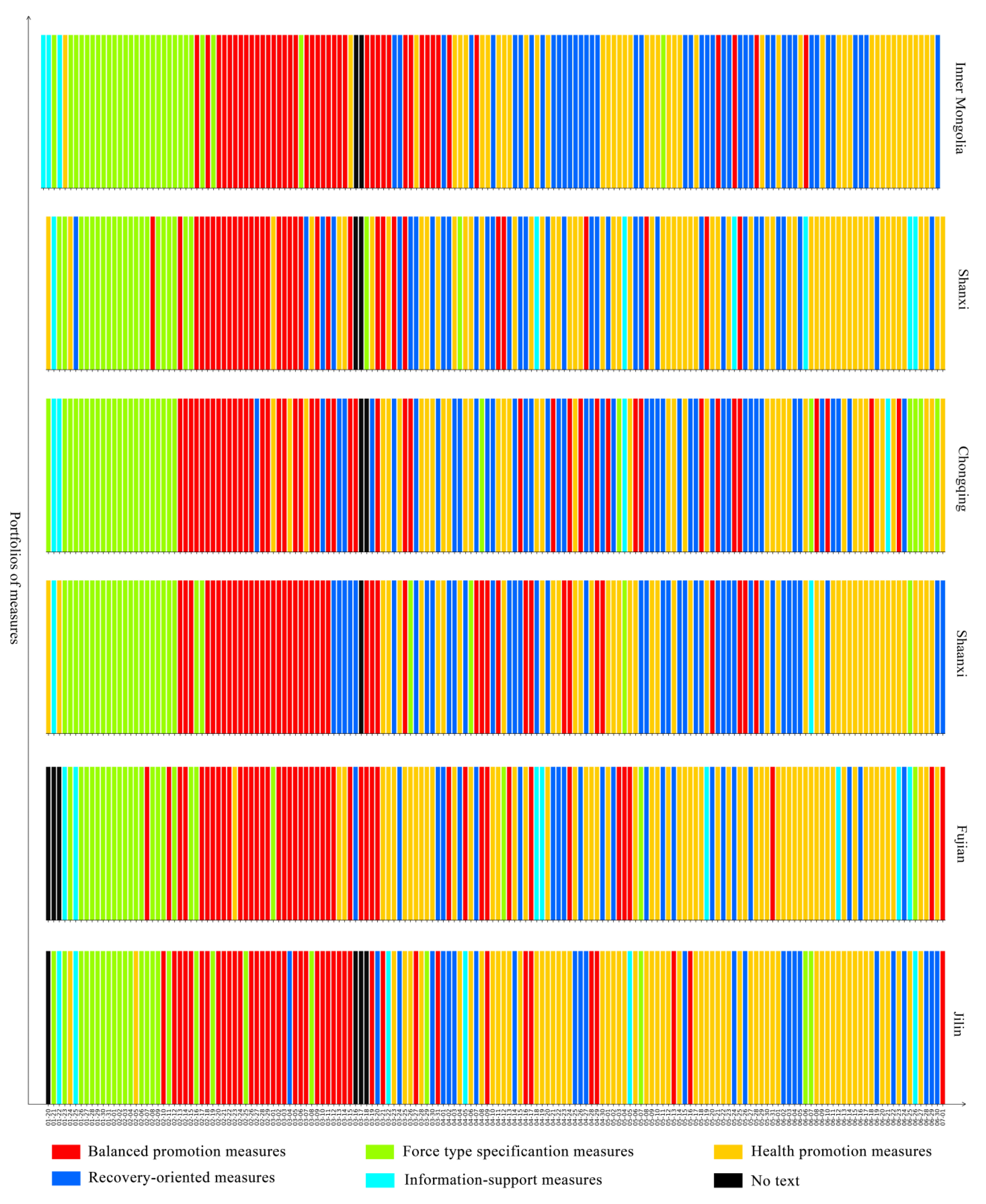
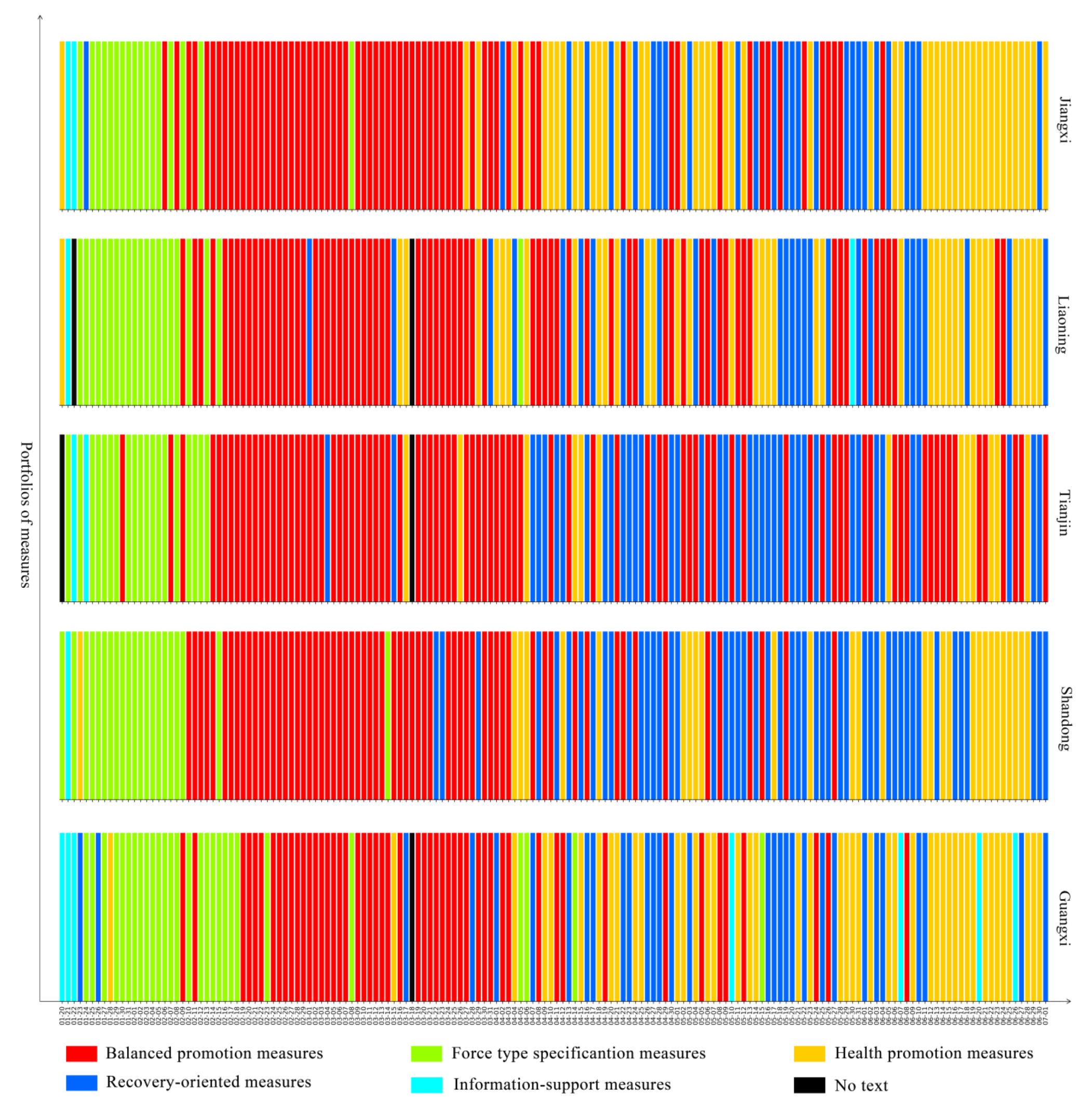
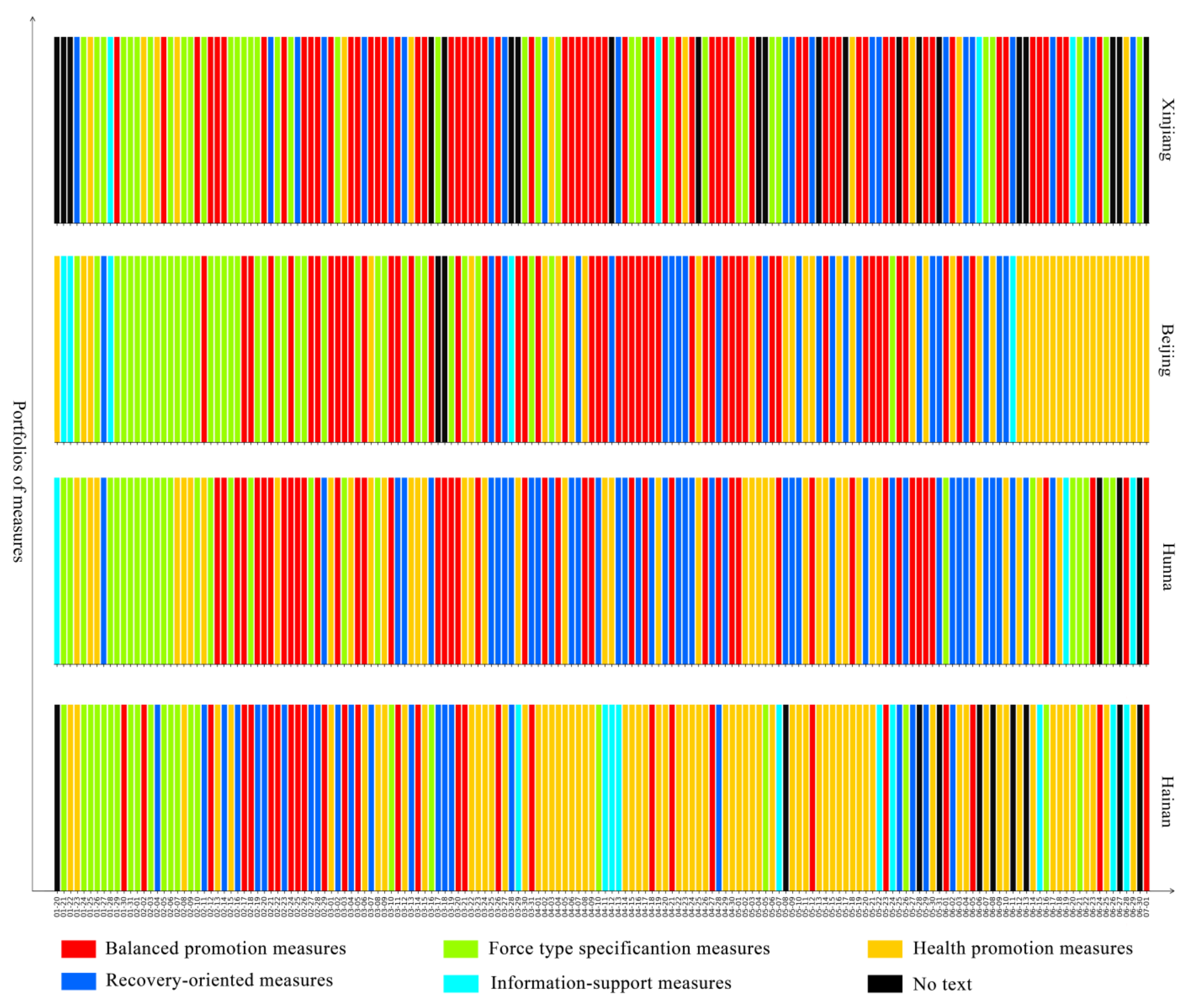
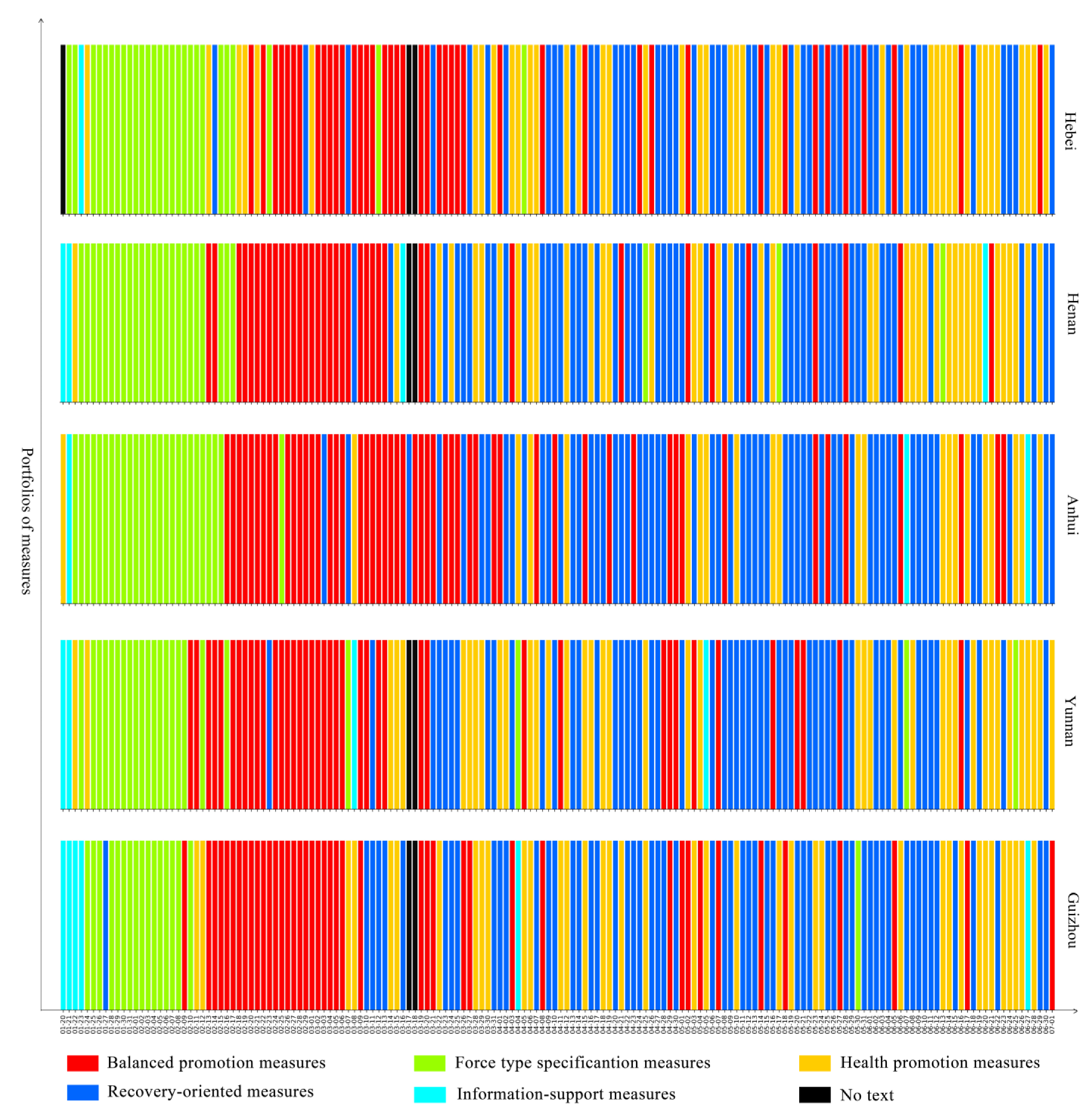
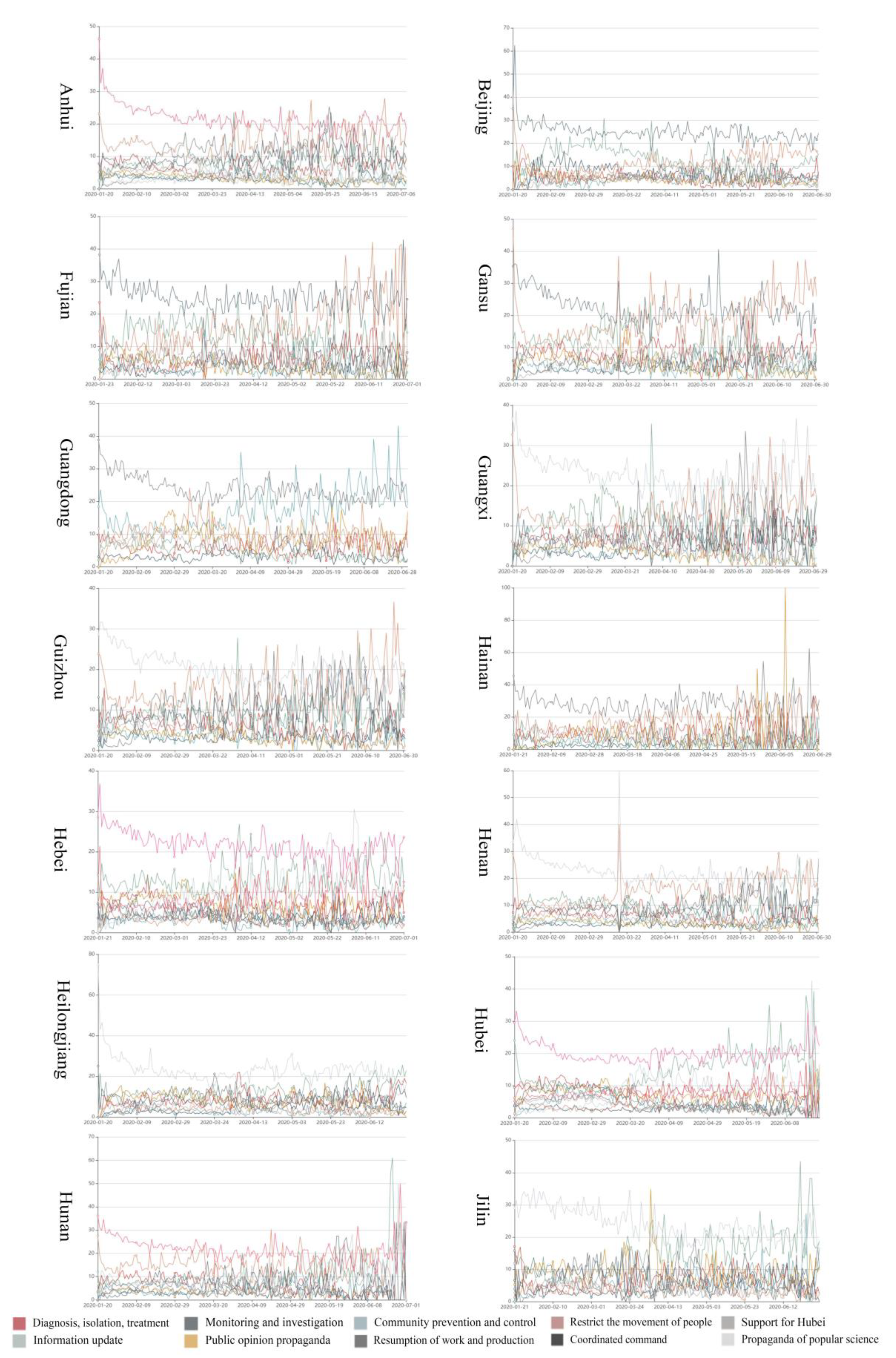
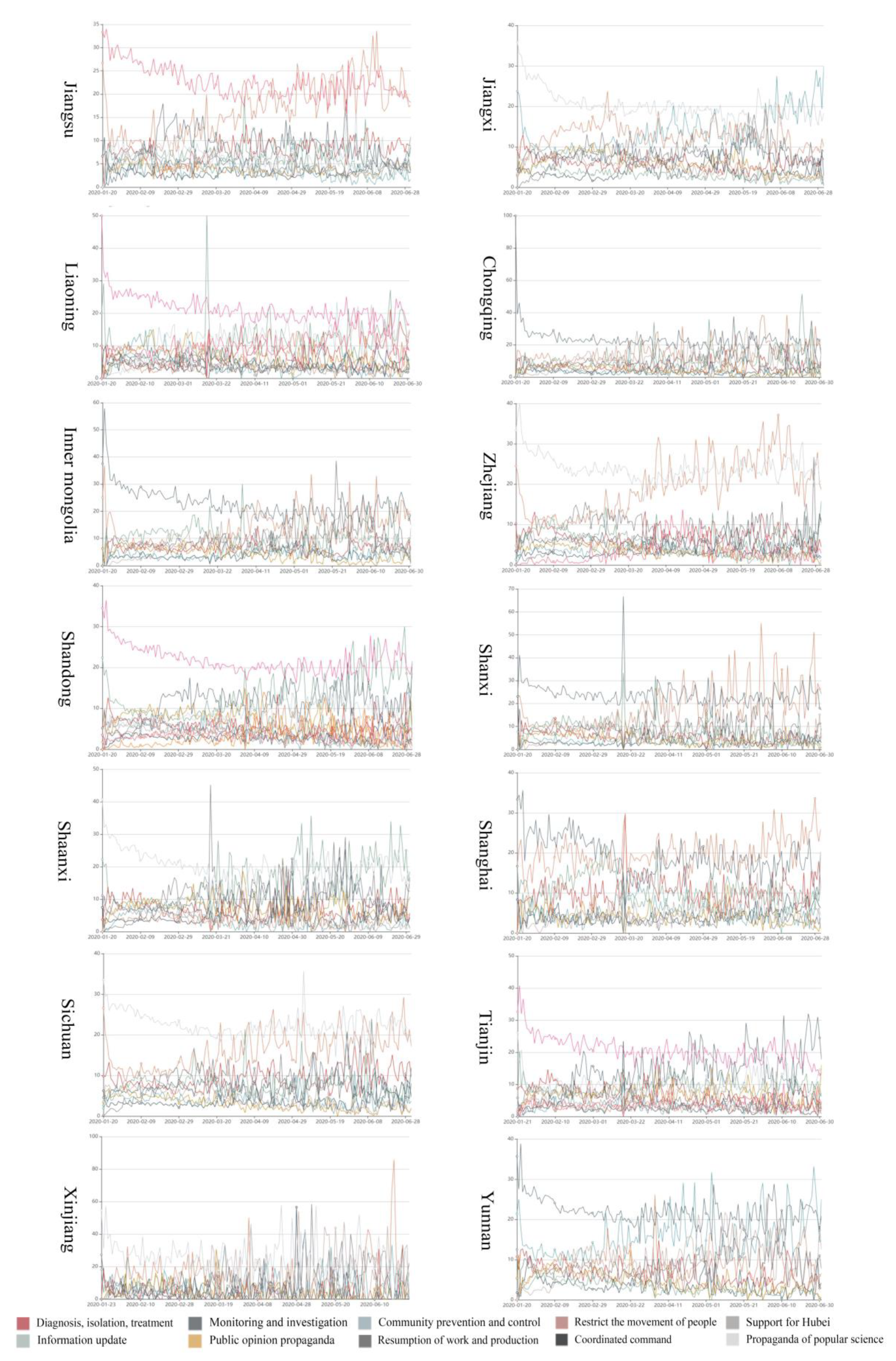
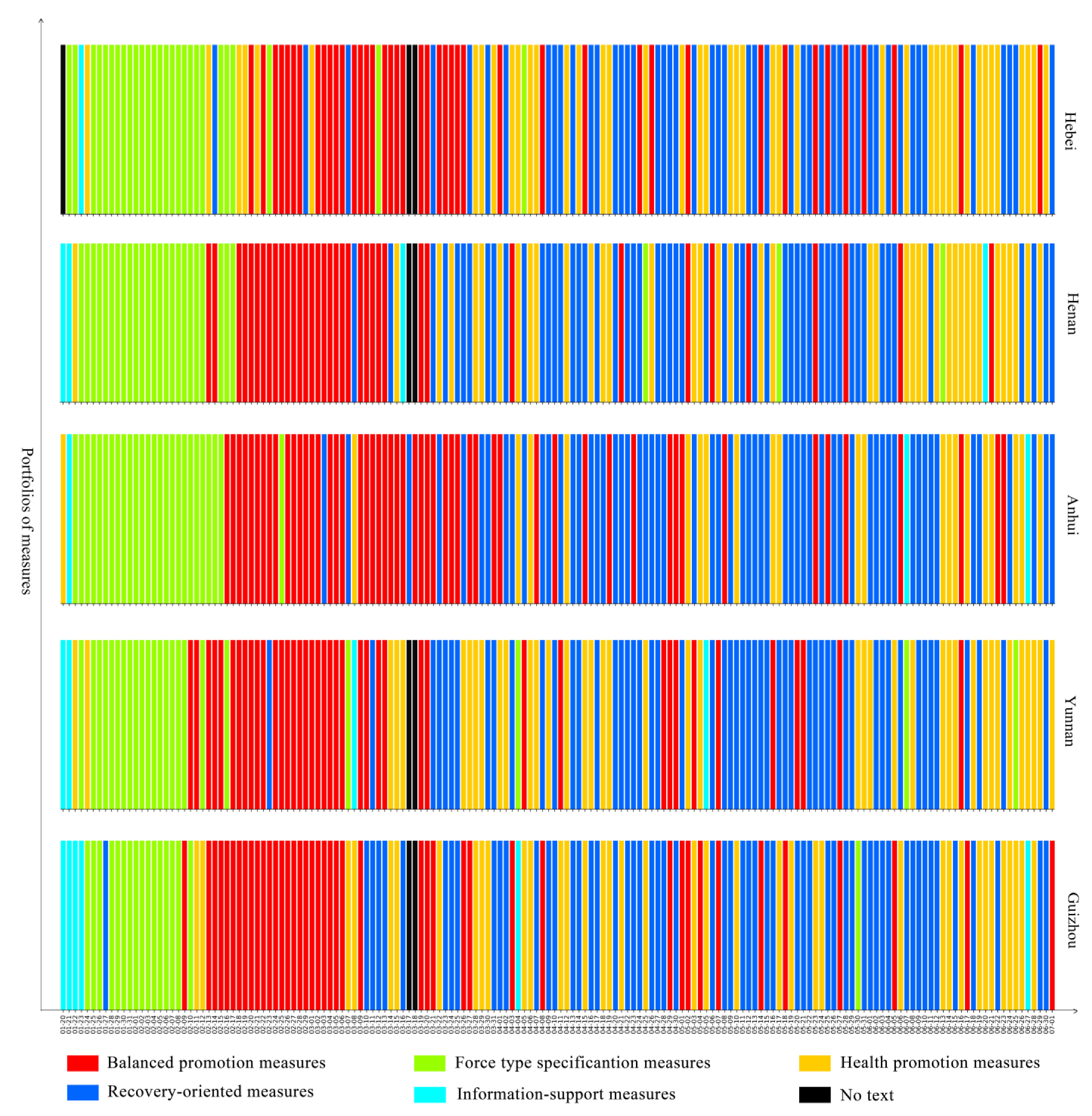
3.1.2. Provincial Level
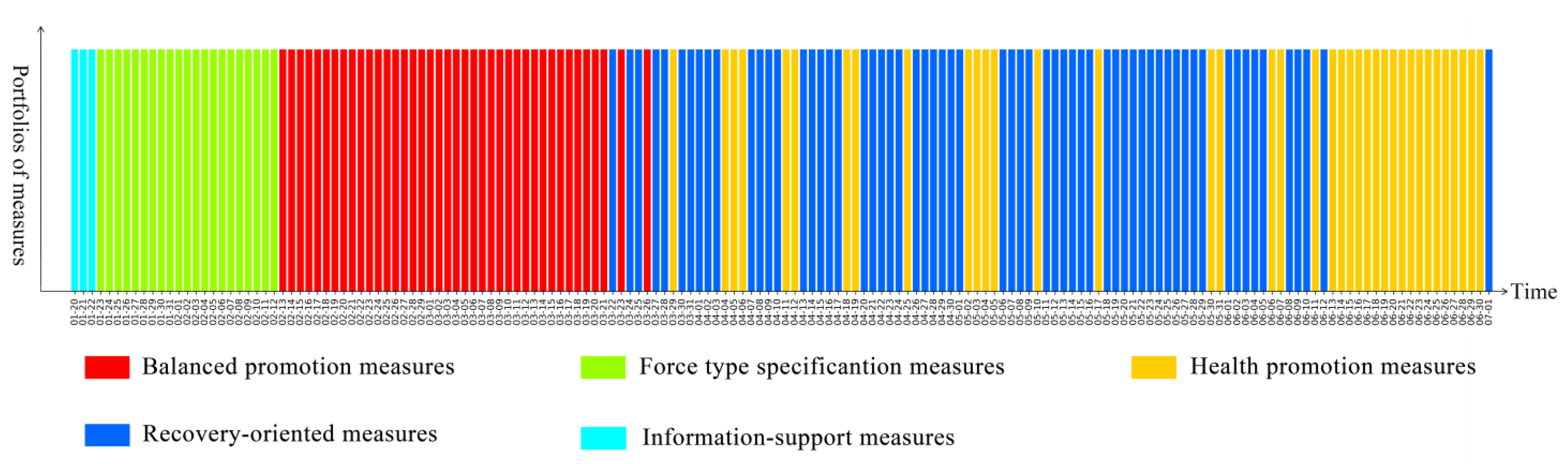
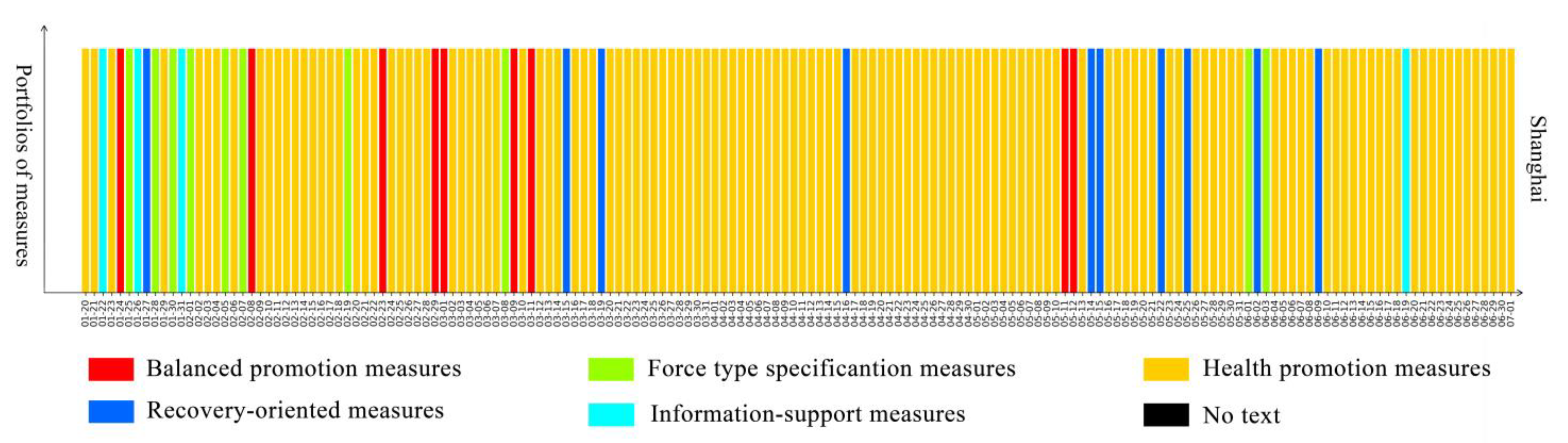
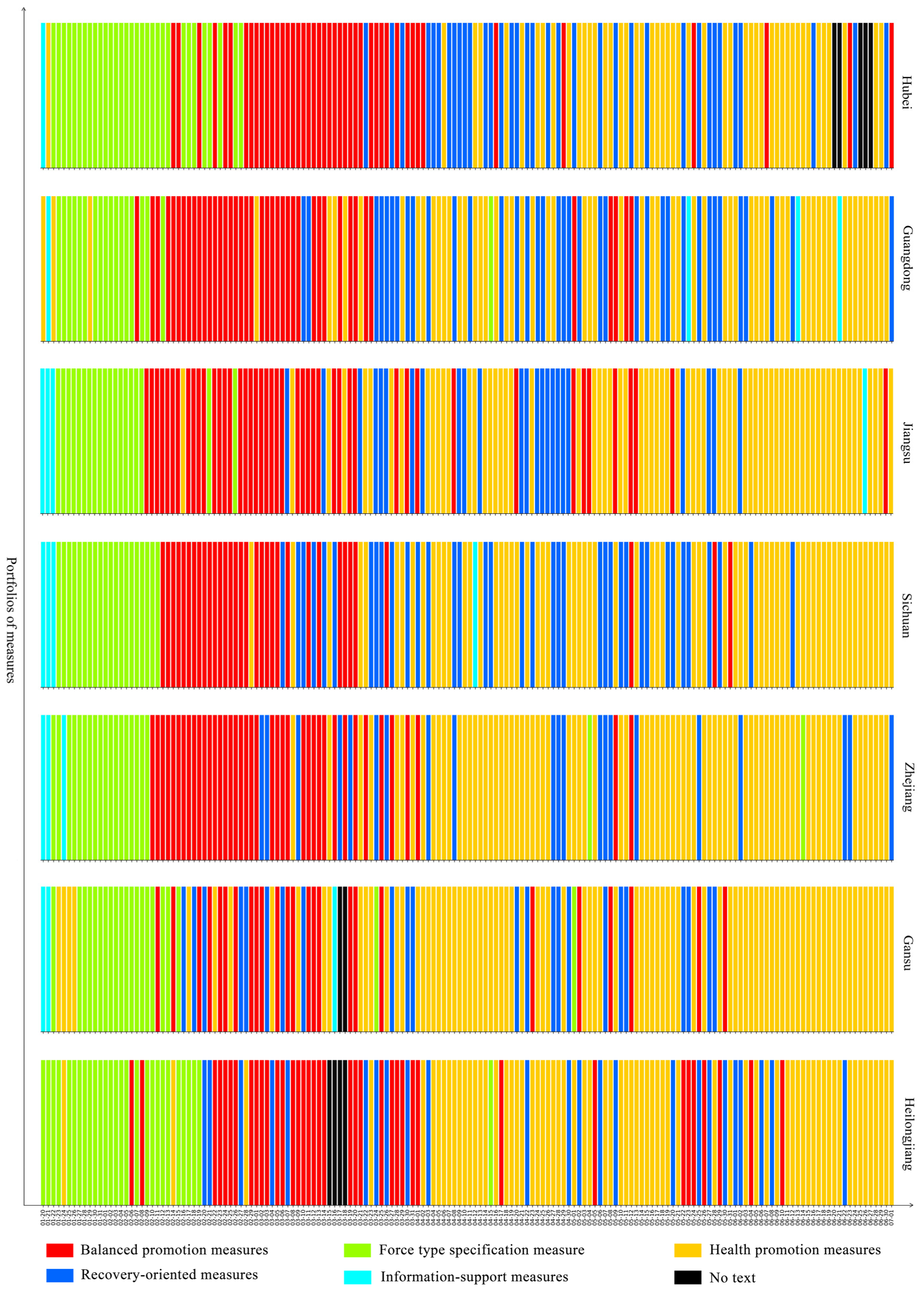
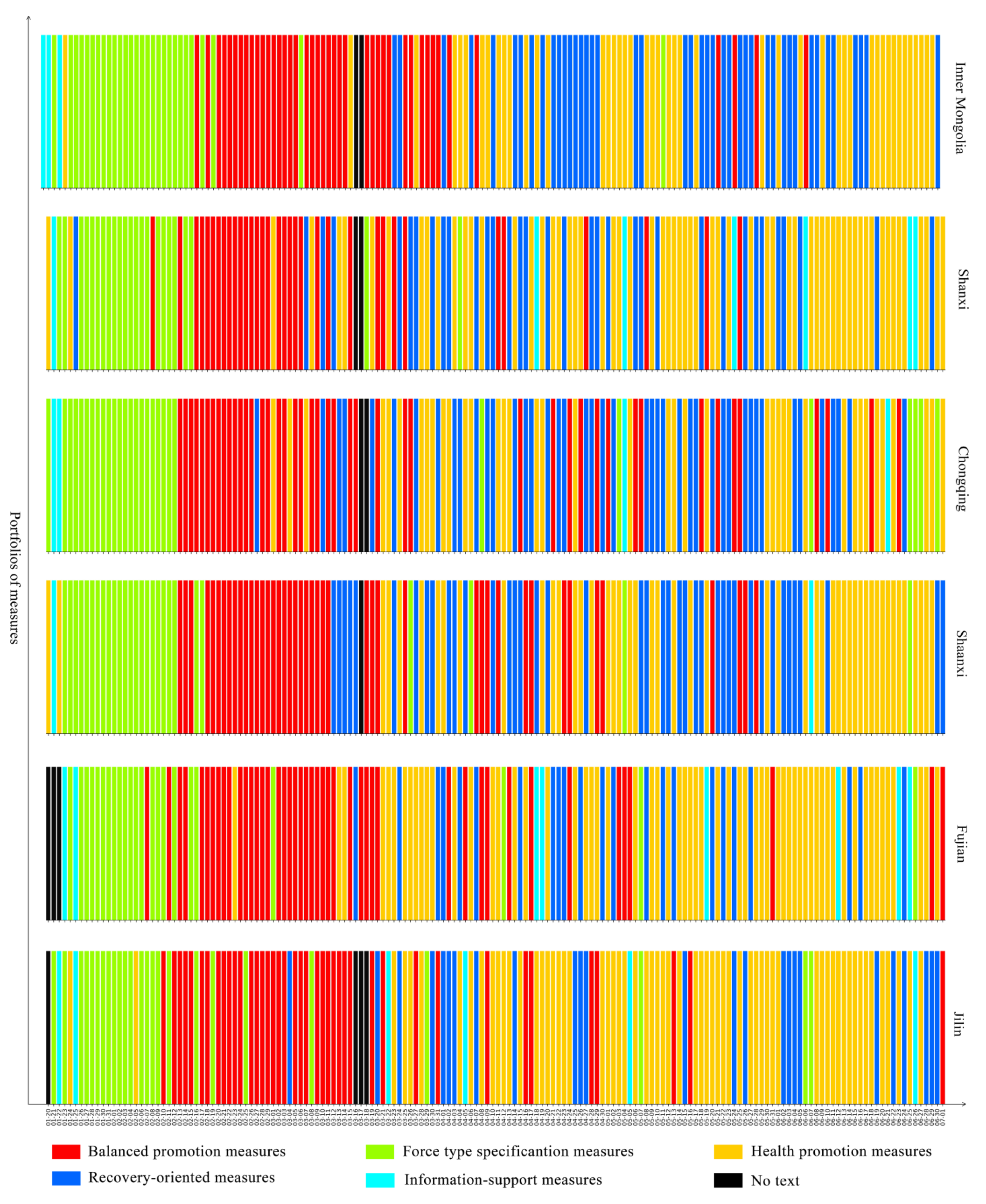
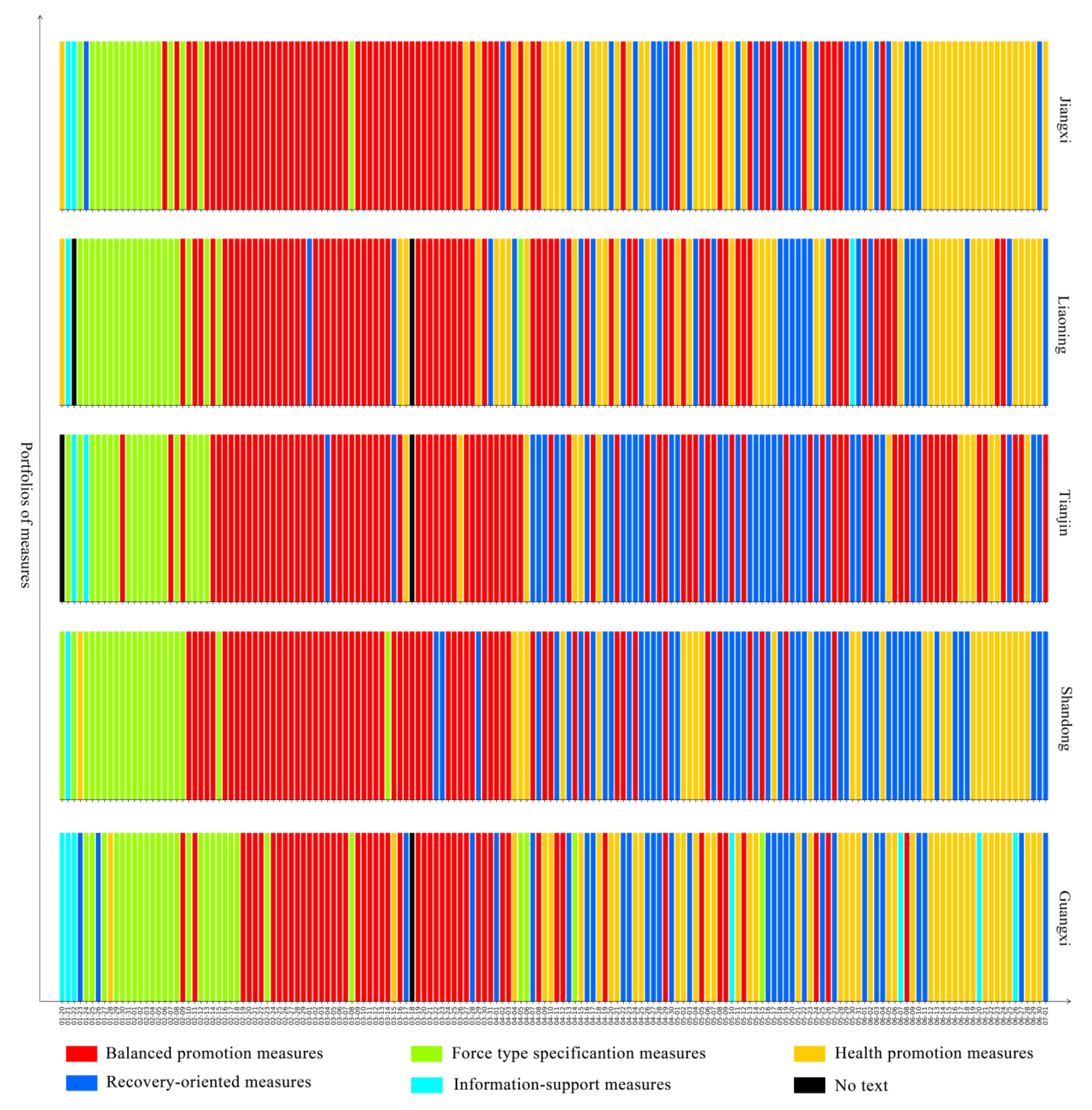
3.2. Pandemic Governance Patterns in Chinese Provincial Government
3.2.1. Pathogen-Control Pattern
3.2.2. Diagnosis and Treatment Consolidation Pattern
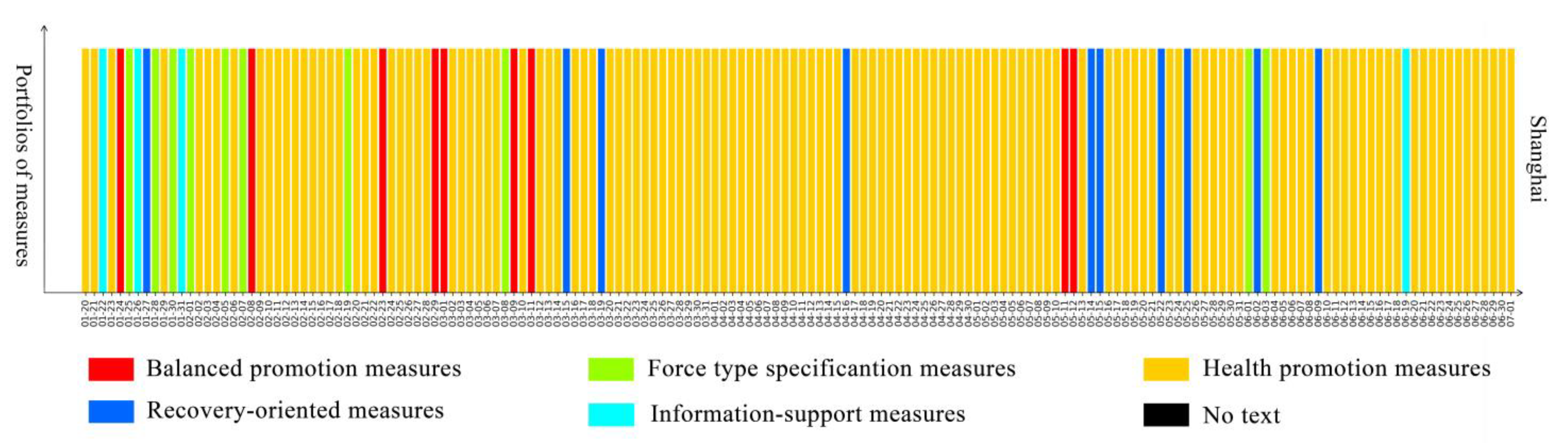
3.2.3. Balanced Promotion Pattern
3.2.4. Quick-Adjustment Response Pattern
3.2.5. Recovery-Oriented Pattern
4. Discussion
4.1. China’s Experience and Its Contribution to Pandemic Governance
4.2. Analysis on Factors Affecting the Pandemic Governance Measures
4.2.1. Factors Leading to Following a Controlling Pathogen Pattern
4.2.2. Factors Leading to Following a Diagnosis and Treatment Consolidation Pattern
4.2.3. Factors Leading to Following a Balanced Promotion Pattern
4.2.4. Factors Leading to Following a Quick-Adjustment Response Pattern
4.2.5. Factors Leading to Following a Recovery-Oriented Pattern
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Duan, J.; Jiao, F. Novel Case-Based Reasoning System for Public Health Emergencies. Risk Manag. Healthc. Policy 2021, 14, 541–553. [Google Scholar] [CrossRef]
- Bian, Q.; Zhang, X.; Mao, Q. The More Actions, the Higher the Performance Evaluation? Evidence from the Crisis Management of COVID-19 in China. Int. J. Disaster Risk Reduct. 2021, 60, 102281. [Google Scholar] [CrossRef]
- World Health Organization WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 8 July 2021).
- World Health Organization COVID-19 Global Risk Communication and Community Engagement Strategy—Interim Guidance. Available online: https://www.who.int/publications-detail-redirect/covid-19-global-risk-communication-and-community-engagement-strategy (accessed on 8 July 2021).
- World Health Organization COVID-19 Emergency Committee Highlights Need for Response Efforts over Long Term. Available online: https://www.who.int/news/item/01-08-2020-covid-19-emergency-committee-highlights-need-for-response-efforts-over-long-term (accessed on 25 June 2021).
- World Health Organization WHO Director-General Calls on G20 to Fight, Unite, and Ignite against COVID-19. Available online: https://www.who.int/news/item/26-03-2020-who-s-director-general-calls-on-g20-to-fight-unite-and-ignite-against-covid-19 (accessed on 25 June 2021).
- Siddik, M.N.A. Economic Stimulus for COVID-19 Pandemic and Its Determinants: Evidence from Cross-Country Analysis. Heliyon 2020, 6, e05634. [Google Scholar] [CrossRef] [PubMed]
- Hale, T.; Angrist, N.; Goldszmidt, R.; Kira, B.; Petherick, A.; Phillips, T.; Webster, S.; Cameron-Blake, E.; Hallas, L.; Majumdar, S.; et al. A Global Panel Database of Pandemic Policies (Oxford COVID-19 Government Response Tracker). Nat. Hum. Behav. 2021, 5, 529–538. [Google Scholar] [CrossRef]
- Berardi, C.; Antonini, M.; Genie, M.G.; Cotugno, G.; Lanteri, A.; Melia, A.; Paolucci, F. The COVID-19 Pandemic in Italy: Policy and Technology Impact on Health and Non-Health Outcomes. Health Policy Technol. 2020, 9, 454–487. [Google Scholar] [CrossRef] [PubMed]
- Toshkov, D.; Yesilkagit, K.; Carroll, B. Government Capacity, Societal Trust or Party Preferences? What Accounts for the Variety of National Policy Responses to the COVID-19 Pandemic in Europe? J. Eur. Public Policy 2021, 1–20. [Google Scholar] [CrossRef]
- Capano, G.; Howlett, M.; Jarvis, D.S.L.; Ramesh, M.; Goyal, N. Mobilizing Policy (In)Capacity to Fight COVID-19: Understanding Variations in State Responses. Policy Soc. 2020, 39, 285–308. [Google Scholar] [CrossRef]
- Gonzalez-Bustamante, B. Evolution and Early Government Responses to COVID-19 in South America. World Dev. 2021, 137, 105180. [Google Scholar] [CrossRef]
- Yin, Y.; Gao, J.; Jones, B.F.; Wang, D. Coevolution of Policy and Science during the Pandemic. Science 2021, 371, 128–130. [Google Scholar] [CrossRef]
- Seven, Ü.; Yılmaz, F. World Equity Markets and COVID-19: Immediate Response and Recovery Prospects. Res. Int. Bus. Financ. 2021, 56, 101349. [Google Scholar] [CrossRef]
- Zaremba, A.; Kizys, R.; Tzouvanas, P.; Aharon, D.Y.; Demir, E. The Quest for Multidimensional Financial Immunity to the COVID-19 Pandemic: Evidence from International Stock Markets. J. Int. Financ. Mark. Inst. Money 2021, 71, 101284. [Google Scholar] [CrossRef]
- Ashraf, B.N. Economic Impact of Government Interventions during the COVID-19 Pandemic: International Evidence from Financial Markets. J. Behav. Exp. Financ. 2020, 100371. [Google Scholar] [CrossRef] [PubMed]
- Koh, W.C.; Naing, L.; Wong, J. Estimating the Impact of Physical Distancing Measures in Containing COVID-19: An Empirical Analysis. Int. J. Infect. Dis. 2020, 100, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Siedner, M.J.; Harling, G.; Reynolds, Z.; Gilbert, R.F.; Haneuse, S.; Venkataramani, A.S.; Tsai, A.C. Social Distancing to Slow the US COVID-19 Epidemic: Longitudinal Pretest–Posttest Comparison Group Study. PLoS Med. 2020, 17, e1003244. [Google Scholar]
- Leffler, C.T.; Ing, E.; Lykins, J.D.; Hogan, M.C.; McKeown, C.A.; Grzybowski, A. Association of Country-Wide Coronavirus Mortality with Demographics, Testing, Lockdowns, and Public Wearing of Masks. Am. J. Trop. Med. Hyg. 2020, 103, 2400–2411. [Google Scholar] [CrossRef]
- Shiva, M.; Molana, H. The Luxury of Lockdown. Eur. J. Dev. Res. 2021, 1–21. [Google Scholar] [CrossRef]
- Galea, S.; Merchant, R.M.; Lurie, N. The Mental Health Consequences of COVID-19 and Physical Distancing: The Need for Prevention and Early Intervention. JAMA Intern. Med. 2020, 180, 817–818. [Google Scholar] [CrossRef] [Green Version]
- Ali, T.O.; Hassan, M.; Hossain, N. The Moral and Political Economy of the Pandemic in Bangladesh: Weak States and Strong Societies during COVID-19. World Dev. 2020, 137, 105216. [Google Scholar] [CrossRef]
- Tungen, B.; Zein, M.E.; Sulik, J.; Newson, M.; Deroy, O. Social Influence Matters: We Follow Pandemic Guidelines Most When Our Close Circle Does. Br. J. Psychol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Choutagunta, A.; Manish, G.P.; Rajagopalan, S. Battling COVID with Dysfunctional Federalism: Lessons from India. South. Econ. J. 2021, 87, 1267–1299. [Google Scholar] [CrossRef]
- Zhu, Y.; Fu, K.-W.; Grépin, K.A.; Liang, H.; Fung, I.C.-H. Limited Early Warnings and Public Attention to Coronavirus Disease 2019 in China, January–February, 2020: A Longitudinal Cohort of Randomly Sampled Weibo Users. Disaster Med. Public Health Prep. 2020, 14, e24–e27. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Negro, G. Weibo in China: Understanding Its Development through Communication Analysis and Cultural Studies. Commun. Politics Cult. 2013, 46, 199–216. [Google Scholar]
- Hale, T.; Petherick, A.; Phillips, T.; Webster, S. Variation in Government Responses to COVID-19. Blavatnik Sch. Gov. Work. Pap. 2020, 31, 2020-11. [Google Scholar]
- Cheng, C.; Barceló, J.; Hartnett, A.S.; Kubinec, R.; Messerschmidt, L. COVID-19 Government Response Event Dataset (CoronaNet v.1.0). Nat. Hum. Behav. 2020, 4, 756–768. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Q.; Jones, F.K.; Leavitt, S.V.; Ung, L.; Labrique, A.B.; Peters, D.H.; Lee, E.C.; Azman, A.S. HIT-COVID, a Global Database Tracking Public Health Interventions to COVID-19. Sci. Data 2020, 7, 286. [Google Scholar] [CrossRef] [PubMed]
- Desvars-Larrive, A.; Dervic, E.; Haug, N.; Niederkrotenthaler, T.; Chen, J.; Di Natale, A.; Lasser, J.; Gliga, D.S.; Roux, A.; Sorger, J.; et al. A Structured Open Dataset of Government Interventions in Response to COVID-19. Sci. Data 2020, 7, 285. [Google Scholar] [CrossRef]
- Alsharif, D.S.A. The Challenges Associated with Women Career Development at the State Universities in Saudi Arabia: A Ground Theory Approach. Int. J. Gend. Women’s Stud. 2018, 6, 18–30. [Google Scholar] [CrossRef] [Green Version]
- Graesser, A.C.; Mcnamara, D.S.; Louwerse, M.M. Methods of Automated Text Analysis. In Handbook of Reading Research, Volume IV; Routledge: London, UK, 2010; ISBN 978-0-203-84041-2. [Google Scholar]
- Grimmer, J.; Stewart, B.M. Text as Data: The Promise and Pitfalls of Automatic Content Analysis Methods for Political Texts. Political Anal. 2013, 21, 267–297. [Google Scholar] [CrossRef]
- Corbin, J.; Strauss, A. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory, 4th ed.; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2019. [Google Scholar]
- Blei, D.M.; Ng, A.Y.; Jordan, M.I. Latent Dirichlet Allocation. J. Mach. Learn. Res. 2003, 3, 993–1022. [Google Scholar]
- Charmaz, K. Constructing Grounded Theory: A Practical Guide through Qualitative Analysis; SAGE: Newcastle upon Tyne, UK, 2006; ISBN 978-1-4462-0040-7. [Google Scholar]
- Lam, S.K.K.; Kwong, E.W.Y.; Hung, M.S.Y.; Chien, W. Investigating the Strategies Adopted by Emergency Nurses to Address Uncertainty and Change in the Event of Emerging Infectious Diseases: A Grounded Theory Study. Int. J. Environ. Res. Public Health 2020, 17, 2490. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Selective Coding Index | Axial Coding Index (Measures) | Open Coding Index (Keywords) |
|---|---|---|
| Information | Information update | CCTV; Prevention; Diagnosis; Human transmission; Personal protection |
| Popular science dissemination | Publicity; Popular science; Authoritative experts; Guidance; Give a cue | |
| Public opinion propaganda | CCTV; Rumour; Come on; Win; Spread rumours | |
| Supervision | Market supervision | Price increase; Price; Product supply; Market supply; Price of medical commodity |
| Supervision of popular behaviour | Cooperate; Prevention of obstruction; Conceal facts; Deliberate concealment; Conceal illness | |
| Supervision of official performance | Perform duties; Inadequate prevention and control; Responsibility implementation is not in place; Dereliction of duty; Underreport | |
| Material supervision | Material supervision; Mask; Medical use; Materials; the Red Cross Society | |
| Diagnosis and treatment | Diagnosis; isolation; treatment | Isolation; Clinical symptoms; Medical observation; Designated hospitals; Treat and cure |
| Improve diagnosis and treatment | Nucleic acid detection; Chinese medicine; Hospital of traditional Chinese medicine; Virus strain; test kit | |
| Improve prevention | Vaccine research; Vaccination; Scientific research; Vaccine; Laboratory | |
| Support of Information-based diagnosis and treatment | AI diagnosis; Teleconsultation; Green channel for medical consultation; Online medical treatment | |
| Recovery | Resumption of school | Students; Term begins; Colleges and universities; Teaching; Online teaching |
| Resumption of work and production | Resumption of work; Production; Resumption of production; Economy; (of laid-off employees) return to the original job | |
| Security | Financial guarantee | Funds; Medical insurance; Guarantee; Financial bottom; Capital |
| Self-material support | Mask; Medical use; Materials; Protective clothing; Donation | |
| Command and coordination | Command and coordination | Research deployment; Instructions; Deploy; Leading group; Inspection and guidance |
| Support for Hubei Province | Mobilisation; Medical team; Expedition; Protective clothing; Donation | |
| Movement of people | Restrict the movement of people | Go out; Home; Outage; Return home |
| Control of gathering activities/places | Public places; Cancellation of aggregated activities; Suspension of opening to the outside world; Start closing; Scenic spot | |
| Community prevention and control | Community; Community residents; Housing estate; Streets; Residents’ committee | |
| Monitoring and investigation | Close contact; Nucleic acid detection; Check; Epidemiological investigation; Traffic quarantine; Virus detection | |
| Support of information-based prevention and control | Green code; Gan code; Health code; Five-colour map of pandemic situation; Pandemic information collection |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
He, Y.; Li, M.; Zhong, Q.; Li, Q.; Yang, R.; Lin, J.; Zhang, X. The Chinese Government’s Response to the Pandemic: Measures, Dynamic Changes, and Main Patterns. Healthcare 2021, 9, 1020. https://doi.org/10.3390/healthcare9081020
He Y, Li M, Zhong Q, Li Q, Yang R, Lin J, Zhang X. The Chinese Government’s Response to the Pandemic: Measures, Dynamic Changes, and Main Patterns. Healthcare. 2021; 9(8):1020. https://doi.org/10.3390/healthcare9081020
Chicago/Turabian StyleHe, Yuxi, Maorui Li, Qixi Zhong, Qi Li, Ruishi Yang, Jing Lin, and Xiaojun Zhang. 2021. "The Chinese Government’s Response to the Pandemic: Measures, Dynamic Changes, and Main Patterns" Healthcare 9, no. 8: 1020. https://doi.org/10.3390/healthcare9081020
APA StyleHe, Y., Li, M., Zhong, Q., Li, Q., Yang, R., Lin, J., & Zhang, X. (2021). The Chinese Government’s Response to the Pandemic: Measures, Dynamic Changes, and Main Patterns. Healthcare, 9(8), 1020. https://doi.org/10.3390/healthcare9081020